Introduction
Orthognathic surgery has become a standard procedure
in the field of oral and maxillofacial surgery. For mandibular
orthognathic surgery, a sagittal split ramus osteotomy (SSRO) is a
popular procedure that can be performed on an intraoral basis
(1), while a Le Fort I osteotomy is
widely applied for removal and accurate repositioning of the
maxilla (2). However, despite advances
in surgical techniques used for orthognathic surgery, various
complications that occur following surgery, including hypoesthesia,
bleeding, respiratory difficulty, temporomandibular joint
dysfunction and infection, have been documented (3,4). Among
those, surgical site infection is an important problem, as it
delays wound repair and prolongs hospital stay. In order to prevent
wound infection, use of antibiotics as well as application of oral
health care procedures, such as professional teeth cleaning and
self-care instructions, are considered as important factors for
patients undergoing oral surgery, as they are associated with
reduced numbers of oral bacteria, resulting in inhibition of
surgical site infection in oral surgery cases.
However, few studies have shown a significant
association between preoperative oral health care and postoperative
complications in patients who underwent orthognathic surgery. In
the present study, the influence of preoperative oral health care
on postoperative inflammatory response, infection and length of
hospital stay was investigated in patients undergoing orthognathic
surgery.
Patients and methods
Patient characteristics
The records of 58 patients (17 males, 41 females;
mean age, 25.8 years; range, 16–49 years) with jaw bone deformity
who underwent surgical treatment in the surgical room under general
anesthesia at the Department of Oral and Maxillofacial
Reconstructive Surgery, Hiroshima University Hospital (Hiroshima,
Japan), between January 2010 and March 2015 were reviewed. Subjects
included in the study were those who underwent an orthognathic
surgery procedure, including SSRO (n=42), SSRO and Le Fort I
osteotomy (n=13), genioplasty (n=2), and anterior maxillary
alveolar osteotomy (n=1). All the surgeries were performed
intraorally without abnormal bone fracture or blood transfusion.
Clinical data obtained included patient age, gender, medical
history, blood loss volume and surgical duration. Patients with a
past history of diabetes, respiratory disorders, cardiovascular
disorders, hyperlipidemia, hypoalbuminemia or others were not
included in order to exclude the effects of those diseases on
postoperative conditions. Cephem antibiotics (cefdinir or
cefmetazole) were administered in all patients for 3–5 days after
the surgery.
Treatment
Patients in the oral care group received
professional teeth cleaning or scaling by a dental hygienist within
2 days prior to surgery, while those in the non-oral care group did
not receive special treatment from a dental hygienist prior to
surgery. Following surgery, regular oral care was performed for all
patients in the two groups by a doctor at least once a day.
Markers and statistical analysis
Markers, such as white blood cell (WBC) count and
C-reactive protein (CRP) level, were examined on the day before and
at 1, 3–5, and 7–9 days after surgery to evaluate the inflammatory
response following the surgery. Occurrences of complications such
as anastomotic leak and surgical site infection were investigated
within 14 days after surgery, with the latter determined according
to the method of Johnson et al (5). The length of hospital stay for each
patient was also examined. Welch's t-test, a one-way analysis of
variance test, and Fisher's exact test were used for statistical
analysis. P<0.05 was considered to indicate a statistically
significant difference. This retrospective study was approved by
the ethics committee of Hiroshima University.
Results
Correlation between postoperative
complications and clinical features
The associaton between preoperative oral care and
postoperative infectious complications (surgical site infection,
aspiration pneumonia, anastomotic leak) was investigated. One case
of surgical site infection was observed in the non-oral care group,
while an anastomotic leak was identified in 4 (13.8%) in the
non-oral care and 3 (10.3%) in the oral care group. No aspiration
pneumonia was reported in any of the patients. The correlation
between postoperative complications and clinical features, such as
gender, age, surgical duration, blood loss and pre-operative oral
health care (Fisher's exact test), was subsequently examined
(Table I). Although there was no
statistical association identified between them, the rate of
occurrence of complications was decreased in patients who received
preoperative oral health care (10.3%) as compared to those who did
not (17.2%).
 | Table I.Correlation between postoperative
complications and clinical factors. |
Table I.
Correlation between postoperative
complications and clinical factors.
|
|
| Postoperative
complications, n (%) |
|
|---|
|
|
|
|
|
|---|
| Clinical factors | Cases, n | (−) | (+) | P-value |
|---|
| Gender |
|
|
|
|
| Male | 17 | 15 (88.2) | 2 (11.8) | 1.00 |
|
Female | 41 | 35 (85.4) | 6 (14.6) |
|
| Age, years |
|
|
|
|
|
16–19 | 17 | 14 (85.7) | 3 (14.3) | 0.65 |
|
20–29 | 23 | 19 (82.6) | 4 (17.4) |
|
|
30–39 | 12 | 11 (91.7) | 1 (8.3) |
|
|
40–49 | 6 | 0 (0.0) | 1 (100) |
|
| Surgical
procedure |
|
|
|
|
| SSRO | 42 | 38 (90.5) | 4 (9.5) | 0.060 |
| SSRO
& Lefort I | 13 | 11 (84.6) | 2
(15.4) |
|
|
Genioplasty | 2 | 1
(50.0) | 1
(50.0) |
|
| Maxillary alveolar
osteotomy | 1 | 0 (0.0) | 1 (100) |
|
| Oral care |
|
|
|
|
| (−) | 29 | 24 (82.8) | 5
(17.2) | 0.71 |
| (+) | 29 | 26 (89.7) | 3
(10.3) |
|
| Blood loss, ml |
|
|
|
|
|
<300 | 18 | 16 (88.9) | 2
(11.1) | 0.64 |
| ≥300 | 40 | 34 (85.0) | 6
(15.0) |
|
| Surgical time,
min |
|
|
|
|
|
<180 | 11 | 9
(81.8) | 2
(18.2) | 1.00 |
| ≥180 | 47 | 41 (87.2) | 6
(12.8) |
|
Comparison of inflammatory response
between oral care and non-oral care groups
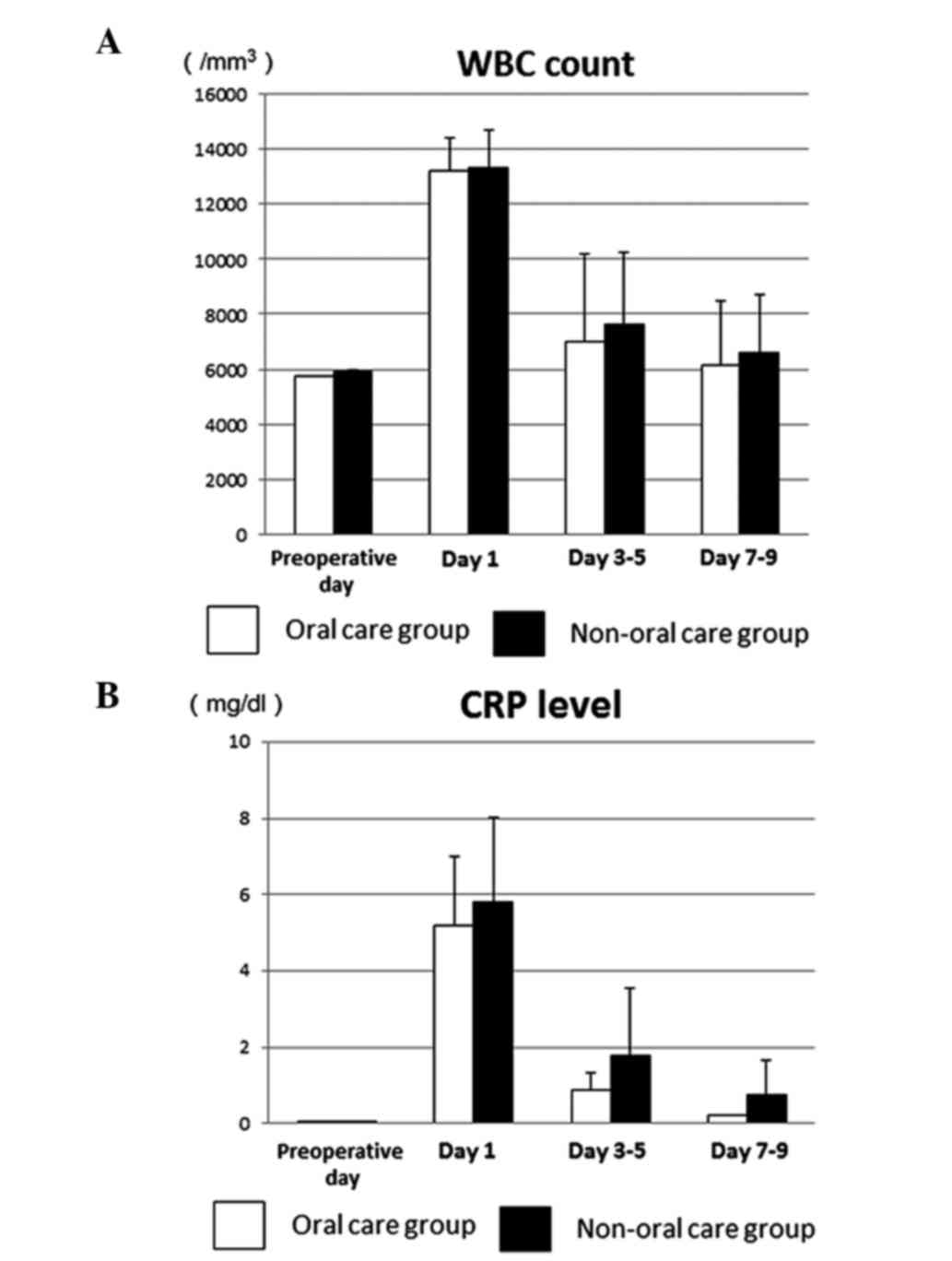
The preoperative WBC count in the oral care and
non-oral care groups was 5,941/mm3 and
5,746/mm3, respectively, both of which were within a
normal range. On day 1 after surgery, the counts increased to a
maximum of 13,344/mm3 and 13,230/mm3,
subsequently decreased to 7,607/mm3 and
6,973/mm3 on days 3–5, and returned to
6,132/mm3 and 6,155/mm3 on days 7–9,
respectively (Fig. 1A). The mean WBC
count in the oral care group was lower compared to the non-oral
care group at days 3–5 and 7–9 after surgery, but was not
significant.
The preoperative CRP level was within a normal range
in all the patients in the two groups. The mean postoperative CRP
in the non-oral care group increased to a maximum of 5.82 mg/dl on
day 1 and decreased to 1.77 mg/dl on days 3–5 (Fig. 1B). In the oral care group, the mean
post-operative CRP increased to a maximum of 5.21 mg/dl on day 1,
decreased to 0.87 mg/dl on days 3–5 and returned to 0.22 mg/dl on
days 7–9 (Fig. 1B). The mean CRP in
the oral care group was lower compared to the non-oral care group
at each time point following surgery, but was not significant.
These results suggest that preoperative oral care may aid in
inhibiting inflammation in the early postoperative period.
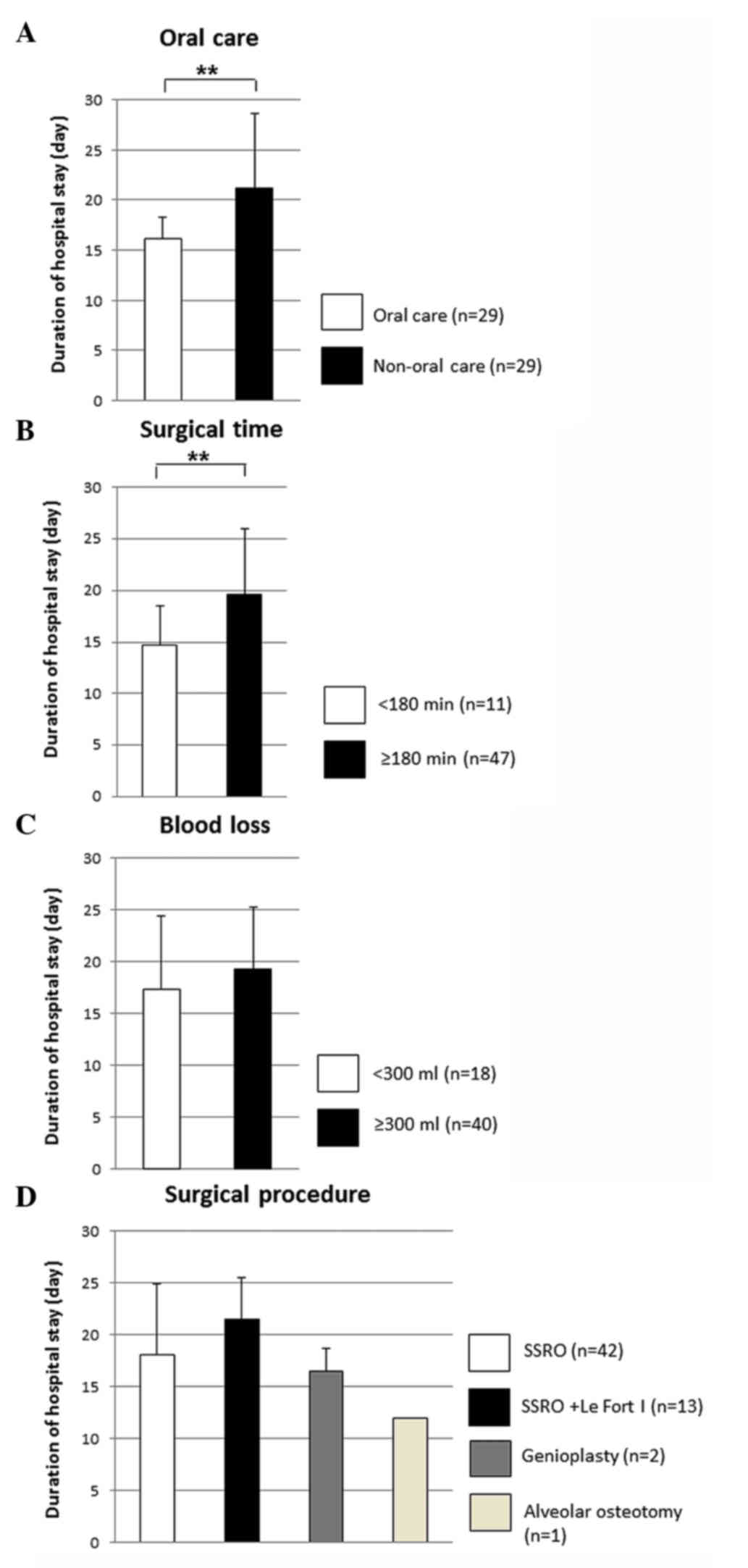
Hospitalization duration
To investigate the effect of preoperative oral
health care on postoperative recovery, the length of hospital stay
was examined. In the oral care and non-oral care groups, the mean
hospital stay was 16.2±3.8 and 21.2±7.4 days, respectively
(Fig. 2A), which was significantly
shorter for the patients who received preoperative oral care. In
addition, this was significantly shorter in cases with a surgical
time <180 min as compared to those with a longer surgical time
(14.7±3.8 vs. 19.6±6.4 days) (Fig.
2B). By contrast, the length of hospital stay was not
significantly associated with blood loss (Fig. 2C). As for the surgical method, patients
who underwent SSRO and Le Fort I osteotomy procedures in
combination showed the longest hospital stay duration (21.5±4.1
days) due to the severity of the procedure (Fig. 2D). However, no significant difference
was identified among the surgical procedures employed. These
results indicate that preoperative oral health care and surgical
time may be associated with recovery of the wound area in the oral
cavity in patients who underwent orthognathic surgery.
Discussion
Patients who undergo oral surgery often have
difficulties with elimination of dental plaque due to
surgery-related swelling, bleeding and pain following the surgery.
Without regular removal, dental plaque undergoes a process of
maturation that results in development of pathogenic bacterial
flora. Therefore, proper oral health care during the perioperative
period is thought to be necessary to decrease the number of oral
pathogens. A previous study showed that oral care is essential to
decrease surgical site infection in oral cancer patients (6). In addition, preoperative oral care was
shown to reduce inflammation during the early postoperative stage
in oral cancer patients who underwent a combination of surgical
resection with neck dissection and free-flap transplantation, or
pectoralis major myocutaneous flap transplantation (7). Together, these results suggest that oral
health care is required for oral cancer patients to prevent wound
infection. As those patients have difficulties with cleaning their
oral cavity, professional oral hygiene procedures, such as
mechanical plaque removal from teeth, gingival and mucosal
surfaces, can help them maintain their oral health condition.
Furthermore, proper instructions for self-oral care may help the
affected patients to maintain good oral health in the postoperative
period.
By contrast, few studies have evaluated the effects
of preoperative oral health care on postoperative complications in
patients who undergo an oral surgery procedure, such as
orthognathic surgery. In the present study of the association
between preoperative oral care and inflammatory response
parameters, no significant difference was identified in regard to
the percentage of postoperative infectious complications between
the oral care (10.3%) and non-oral care (17.2%) groups, although a
declining tendency of postoperative complications following
preoperative oral care was noted. Professional oral health care
appears to have an important role in managing infectious
complications by reducing the number of oral pathogens present at
the time of surgery.
As the CRP level can rapidly increase during the
acute phase of inflammation (8), it is
considered to be a sensitive inflammatory marker and useful
indicator for detection of infection following surgery (9,10). Although
there were no significant differences in regards to WBC count and
CRP level between the present oral care and non-oral care groups,
CRP levels were clearly different between the groups on days 1,
3–5, and 7–9. One possible reason is that an inflammatory condition
in the early postoperative period may be affected by preoperative
professional oral health care, and that in the late postoperative
period it may be influenced by pre- and postoperative oral health
care.
As for the duration of hospital stay, the median
duration was significantly lower in the oral care group as compared
with the non-oral care group, suggesting that a shortened hospital
stay may be attributed to rapid recovery from postoperative
inflammation and proper wound healing. Therefore, the present
findings suggest that preoperative oral health care can shorten the
length of hospital stay by attenuating the occurrence of
inflammation and infectious complications during the postoperative
stage.
Previous studies have identified a significant
association between blood loss and frequency of surgical site
infection in patients who underwent head and neck surgery (6,11,12). In the present study, no significant
differences in regards to the occurrence of postoperative
infectious complications between patients with low blood loss
(11.1%) and those with high blood loss (15.0%) were observed,
although postoperative complications showed a declining tendency in
the former group. Therefore, blood loss may be a risk factor for
infection in patients undergoing orthognathic surgery.
In summary, the present findings indicate that
preoperative oral health care may help to reduce postoperative
inflammation and the frequency of postoperative complications in
patients undergoing orthognathic surgery, resulting in a shorter
hospital stay.
Acknowledgements
The present study was supported by a Grant-in-aid
(no. 23592963) from the Japanese Ministry of Education, Culture,
Sports, and Technology.
Glossary
Abbreviations
Abbreviations:
|
SSRO
|
sagittal split ramus osteotomy
|
|
WBC
|
white blood cell
|
|
CRP
|
C-reactive protein
|
References
|
1
|
Al-Moraissi EA and Ellis E III: Is there a
difference in stability or neurosensory function between bilateral
sagittal split ramus osteotomy and intraoral vertical ramus
osteotomy for mandibular setback? J Oral Maxillofac Surg.
73:1360–1371. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
de Mol van Otterloo JJ, Tuinzing DB,
Greebe RB and van der Kwast WA: Intra- and early postoperative
complications of the Le Fort I osteotomy: A retrospective study on
410 cases. J Craniomaxillofac Surg. 19:217–222. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Garg S and Kaur S: Evaluation of
post-operative complication rate of le fort I osteotomy: A
retrospective and prospective study. J Maxillofac Oral Surg.
13:120–127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mitsukawa N, Morishita T, Saiga A, Kubota
Y, Omori N, Akita S and Satoh K: Dislocation of temporomandibular
joint: Complication of sagittal split ramus osteotomy. J Craniofac
Surg. 24:1674–1675. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Johnson JT, Myers EN, Thearle PB, Sigler
BA and Schramm VL Jr: Antimicrobial prophylaxis for contaminated
head and neck surgery. Laryngoscope. 94:46–51. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sato J, Goto J, Harahashi A, Murata T,
Hata H, Yamazaki Y, Satoh A, Notani K and Kitagawa Y: Oral health
care reduces the risk of postoperative surgical site infection in
inpatients with oral squamous cell carcinoma. Support Care Cancer.
19:409–416. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shigeishi H, Ohta K, Fujimoto S, Nakagawa
T, Mizuta K, Ono S, et al: Preoperative oral health care reduces
postoperative inflammation and complications in oral cancer
patients. Exp Ther Med. (In press).
|
|
8
|
Pepys MB and Hirschfield GM: C-reactive
protein: A critical update. J Clin Invest. 111:1805–1812. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Iizuka T and Lindqvist C: Changes in
C-reactive protein associated with surgical treatment of mandibular
fractures. J Oral Maxillofac Surg. 49:464–467. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mustard RA Jr, Bohnen JM, Haseeb S and
Kasina R: C-reactive protein levels predict postoperative septic
complications. Arch Surg. 122:69–73. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu SA, Wong YK, Poon CK, Wang CC, Wang CP
and Tung KC: Risk factors for wound infection after surgery in
primary oral cavity cancer patients. Laryngoscope. 117:166–171.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ogihara H, Takeuchi K and Majima Y: Risk
factors of postoperative infection in head and neck surgery. Auris
Nasus Larynx. 36:457–460. 2009. View Article : Google Scholar : PubMed/NCBI
|