Introduction
Escherichia coli (E. coli) is a common
opportunistic pathogen for nosocomial infection (1). The National Antimicrobial Resistance
Monitoring Network (www.carss.cn)
has previously shown that the E. coli isolation rate ranked
first as a gram-negative bacterium. This constitutes the reason for
β lactam antibiotic resistance producing the AmpC enzyme (2). The AmpC enzyme gene is transferred to
other bacteria through conjugation and transformation, and is
mediated by the plasmid. The AmpC enzyme-producing strains show
broader resistance, making it challenging for clinicians to treat
associated infections (3).
In the present study, clinical isolates of E.
coli-producing AmpC enzyme-mediated plasmid were examined in
the local tertiary hospitals (Xuzhou City Hospital Affiliated to
Xuzhou Medical College, Xuzhou No.1 People's Hospital and Xuzhou
Central Hospital) between August and October 2012.
Materials and methods
Materials
In total, 96 strains of E. coli with no
duplication of clinical specimens were collected from patients at
the Xuzhou First People's Hospital, Affiliated Hospital of Xuzhou
Medical College, Xuzhou Central Hospital (Jiangsu, China) between
August and October 2012.
The standard AmpC-producing negative control strains
were E. coli ATCC 25922. The positive control strains were
Enterobacter cloacae 029M.
Instruments and reagents used to conduct the
experiment were: Vitek-32 automatic microbiological analyzer
(bioMerieux, Marcy l'Etoile, France), gel imaging system (Bio
Canon, Shanghai, China), polymerase chain reaction (PCR)
amplification instrument (Biometra GmbH, Goettingen, Germany),
electrophoresis apparatus (Beijing Liuyi Instrument Factory,
Beijing, China), cefoxitin (FOX, 30 µg), and drug-sensitive slips.
Mueller-Hinton agar was purchased from the British Opioid company
(www.oxoid.com). Ex Taq enzyme, dNTPs, and DNA
marker 100 were purchased from Tiangen Biotech Co., Ltd., Beijing,
China. Agarose, and ethidium bromide were purchased from Sigma, St.
Louis, MO, USA.
Method
Clinical specimens were cultured in blood agar
medium at 35°C for 18–24 h and identified for bacteria and drug
sensitivity analysis using the Microscan microbial identification
system (Microscan, Siemens Healthcare Diagnostics, Deerfield, IL,
USA). Primary screening of the AmpC enzyme-producing strains was
conducted using the Kirby-Bauer disk diffusion method. Bacteria
were detected using FOX (30 µg) drug-sensitive slips according to
the standards of USA National Committee for Clinical Laboratory
Standards in 2009 (www.biomedresearch.com). A bacteriostatic circle
diameter of ≤18 mm indicated strains producing AmpC enzyme.
The DNA of the positive clinical strains in the AmpC
enzyme primary screening test was extracted using a bacterial DNA
extraction kit, and this DNA served as a PCR template. The
procedure was carried out according to the manufacturer's protocol.
The multiplex PCR primer sequences were carried out as previously
described (1). Six pairs of primers
were synthesized by Shanghai Saigon Biological Engineering
Technology Co., Ltd. (Shanghai, China) (Table I).
 | Table I.Polymerase chain reaction primer
sequences and target gene. |
Table I.
Polymerase chain reaction primer
sequences and target gene.
| Primers | Primer sequences
(5′→3′) | Expected product
length (bp) |
|---|
|
BlaMOX | P1:
GCTGCTCAAGGAGCACAGGAT | 520 |
|
| P2:
CACATTGACATAGGTGTGC |
|
|
BlaCIT | P1:
TGGCCAGAACTGACAGGCAAA | 462 |
|
| P2:
TTTCTCCTGAACGTGGCTGGC |
|
|
BlaDHA | P1:
AACTTTCACAGGTGTGCTGGGT | 405 |
|
| P2:
CCGTACGCTTACTGGCTTTGC |
|
|
BlaACC | P1:
AACAGCCTCAGCCGGTTA | 346 |
|
| P2:
TTCGCCGCAATCCCTAGC |
|
|
BlaEBC | P1:
TCGGTAAAGCCGATGTTGCGG | 302 |
|
| P2:
CTTCCACTGCGGCTGCCAGTT |
|
|
BlaFOX | P1:
AACATGGGGTATCAGGGAGATG | 190 |
|
| P2:
CAAAGCGCGTAACCGGATTGG |
|
The total volume of the reaction system was 50 µl.
The PCR reaction conditions were: Pre-degeneration at 94°C for 3
min, degeneration at 94°C for 30 sec, annealing at 56°C for 30 sec,
extension at 72°C for 60 sec, for 28 cycles, and a final extension
at 72°C for 7 min. The PCR product underwent electrophoresis in
1.5% agarose gel containing 0.5 µg/ml ethidium bromide for gel
imaging system observation and image recording.
The PCR products were analyzed by gene sequencing
using bidirectional sequencing by Shanghai Saigon Biological
Engineering Technology Co., Ltd. The results were assessed in BLAST
to determine the genotype.
Results
The primary screening results identified that 43 of
96 strains tested for E. coli were resistant or intermediate
to cefoxitin. The strains were AmpC enzyme-producing-positive
strains in the primary screening. The positive rate was 44.8%
(43/96).
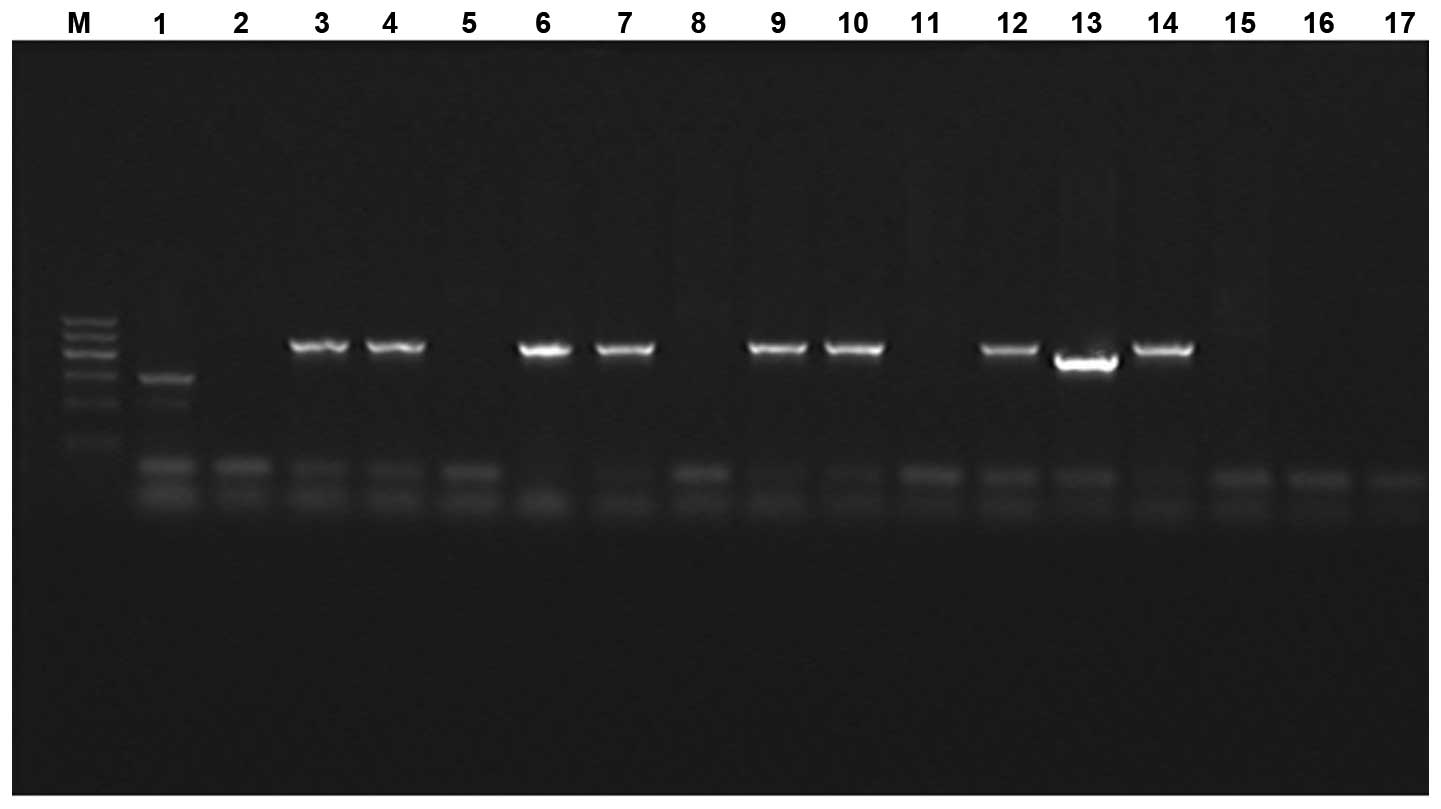
The multiplex PCR results identified 12 cases that
were positive, including 11 strains with an amplified fragment size
of ~405 bp. The strains were determined as type DHA according to
the amplified fragment size. The amplified fragment size of the one
strain was ~346 bp and was determined to be of type ACC. The total
positive rate was 12.5% (12/96). The electrophoresis results are
shown in Fig. 1. The purified PCR
product sequencing results were crossed with GenBank database to
determine the genotype of E. coli. Eleven strains of E.
coli were type DHA with one strain of type ACC.
The results of E. coli producing AmpC enzyme
mediated by plasmid were completely sensitive to imipenem with a
high sensitivity to cefepime (66.7%), amikacin (66.7%) and a low
sensitivity (33.3%) to piperacillin and tazobactam.
The drug resistance rates to aztreonam,
ciprofloxacin, and second- or third-generation cephalosporin were
high (Table II).
| Table II.Twelve strains of AmpC enzyme
producing Escherichia coli drug susceptibility results. |
Table II.
Twelve strains of AmpC enzyme
producing Escherichia coli drug susceptibility results.
|
| Sensitive | Intermediate | Resistance |
|---|
|
|
|
|
|
|---|
| Antibiotics | No. of sensitive
strains | The sensitive rate
(%) | No. of intermediate
strains | The intermediate rate
(%) | No. of resistance
strains | The resistance rate
(%) |
|---|
| FOX | 0 |
0.0 | 1 | 8.3 | 11 | 91.7 |
| CRO | 3 | 25.0 | 1 | 8.3 | 8 | 66.7 |
| CAZ | 1 |
8.3 | 1 | 8.3 | 10 | 83.3 |
| FEP | 8 | 66.7 | 1 | 8.3 | 3 | 25.0 |
| ATM | 1 |
8.3 | 1 | 8.3 | 10 | 83.3 |
| TZP | 6 | 50.0 | 2 | 16.7 | 4 | 33.3 |
| AMK | 8 | 66.7 | 1 | 8.3 | 3 | 25.0 |
| CIP | 1 |
8.3 | 0 | 0.0 | 11 | 91.7 |
| IVX | 1 |
8.3 | 0 | 0.0 | 11 | 91.7 |
| IMP | 12 | 100.0 | 0 | 0.0 | 0 | 0.0 |
Discussion
E. coli is an important pathogen in
nosocomial infection (4). With the
extensive application of broad-spectrum antibiotics, drug-resistant
strains have been on the increase. AmpC enzyme production is the
main mechanism for drug resistance. Although the AmpC structural
gene exists in E. coli chromosome, it can only be produced
from low levels of AmpC enzyme, due to a lack of the AmpR
gene. However, when E. coli obtains an exogenous AmpC
gene or the mutations lead to a high expression of AmpC structural
gene, the result is resistance to many antibiotics. The AmpC
enzyme-producing E. coli was recently identified (5). Thus, detection of the AmpC enzyme in
E. coli in the tertiary hospital in the local region was
useful in gaining a better understanding of the enzyme's prevalence
and drug resistance.
The USA Committee for Clinical and Laboratory
Standards Institute has not recommended use of a standard method
for the detection of AmpC (6). Thus,
the standard detection method for screening AmpC enzyme remains to
be determined (7). The AmpC enzyme can
hydrolyze cefoxitin whereas other β lactam enzymes do not have this
function. In the present study, 96 strains of E. coli were
screened using a cefoxitin susceptibility disk test, and 43 strains
were screened for producing AmpC enzyme. The positive E.
coli in the primary screening were detected the genotypes using
multiplex PCR technique (8). Twelve
strains of E. coli amplification were positive for the test,
including 11 strains of tested bacteria amplified bands of ~405 bp
in size that were identified as DHA type AmpC enzymes according to
the size of the fragments. One strain of tested bacterial amplified
bands of ~346 bp in size was determined to be the ACC type AmpC
enzyme according to the fragment size. The total positive rate of
the E. coli-producing AmpC enzyme mediated by plasmid in the
tertiary hospital in the Xuzhou region was 12.5%. Dong et al
(9) have reported that the enzyme may
be associated with the widely used third-generation antibiotics in
this region. The most common AmpC resistance gene is type DHA-1 and
type ACT. The present findings have shown that the E.
coli-producing AmpC enzyme mediated by plasmid is mainly the
DHA type in the tertiary Hospital of Xuzhou region, which is
consistent with previous studies (10). Thus, type DHA may be the main base of
domestic plasmid-mediated AmpC enzyme combined with the results of
the present study.
The findings have shown that the drug susceptibility
of AmpC enzyme-producing E. coli exhibited multiple drug
resistance to second- or third-generation cephalosporin including
cefoxitin, ceftazidime, and ceftriaxone. It also showed high
resistant to quinolone antibiotics such as ciprofloxacin and
levofloxacin. The Amikacin drug resistance rate was 25% with a
relatively low resistance rate of 25%. The fourth-generation
cephalosporin was recommended for the treatment infection of
strains producing AmpC as it rapidly passes through the outer
membrane barrier. The E. coli producing the AmpC enzyme in
the present study was sensitive to cefepime. Therefore, the
fourth-generation cephalosporin can be used for the treatment of
related infection. Additionally, E. coli resistance to
carbapenem antibiotic imipenem in the present study is due to the
high stability of carbapenem antibiotics to β-lactamase. Carbapenem
antibiotic imipenem is thus recommended for the clinical treatment
of AmpC enzyme-producing E. coli infection mediated by
plasmid. The application of the fourth-generation cephalosporins
and aminoglycosides for treatment may also be considered.
The present study has demonstrated that the
detection rate of the AmpC enzyme-producing E. coli was high
in the tertiary hospital of the Xuzhou area. Carbapenem antibiotics
are thus a suitable choice for treatment of related infection.
References
|
1
|
Weinstein RA: Nosocomial infection update.
Emerg Infect Dis. 4:416–420. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jacoby GA: AmpC beta-lactamases. Clin
Microbiol Rev. 22:161–182. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Markovska R, Schneider I, Marteva-Proevsk
Y, Mitov I, Bauernfeind A and Markova B: First detection of the
AmpC beta-lactamase ACC-1 in a Klebsiella pneumoniae isolate
in Bulgaria. J Chemother. 24:307–308. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ma XZ, Lv Y and Xue F: Ministry of health,
the nationalantimicrobial resistance monitoring report: Bacterial
drug resistance monitoring bloodstream infection for 2010. Chin J
Nosocomiol. 21:5147–5151. 2011.(In Chinese).
|
|
5
|
Ahmed SF, Ali MM, Mohamed ZK, Moussa TA
and Klena JD: Fecal carriage of extended-spectrum beta-lactamases
and AmpC-producing Escherichia coli in a Libyan community.
Ann Clin Microbiol Antimicrob. 13:22.2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Clinical and Laboratory Standards
Institute: Performance standards for antimicrobial susceptibility
testing. Sixteenth informational supplement. M100–S116. 2006.
|
|
7
|
Joseph NM and Mathias S: Challenges in
detection of AmpC β-lactamases among Enterobacteriaceae.
Indian J Med Res. 137:216–217. 2013.PubMed/NCBI
|
|
8
|
Yilmaz NO, Agus N, Bozcal E, Oner O and
Uzel A: Detection of plasmid-mediated AmpC β-lactamase in
Escherichia coli and Klebsiella pneumoniae. Indian J
Med Microbiol. 31:53–59. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dong F, Xu X and Song W: Study on AmpC
beta lactamases in clinical isolates of Escherichia coli and
Klebsiella plasmid mediated. Chin Med J (Engl).
90:2723–2725. 2010.
|
|
10
|
Ying Ye, Qian Wang, Yan Chen and Jiabin
Li: Identification of plasmid-mediated AmpC β-lactamase in
Escherichia coli. Chin J Lab Med. 30:662–665. 2007.
|