Introduction
Atherosclerosis is characterized by a complex
multi-factorial pathophysiology that is the major cause of coronary
artery disease (CAD) (1). Conventional
risk factors have been proposed to cause this condition; however,
the genetic effect remains unexplained (1). Gene-environment interactions may be
particularly important. Certain studies have investigated the
associations between polymorphic variants in candidate genes and
atherosclerosis. A potential suspected gene system is the matrix
metalloproteinase (MMP) family that consists of N20 proteases,
which functions to degrade collagens and other extracellular matrix
proteins to maintain vascular homeostasis (2).
Macrophages, the primary cells of the
atherosclerotic lesions, express MMPs as proteolytic enzymes that
may influence rates of atherogenesis and the stability of
atherosclerotic plaques (3). The rate
of extracellular matrix breakdown and accumulation is predominantly
regulated by the interaction between MMPs and their endogenous
antagonists.
MMP-3 and MMP-9 are affected at
transcription levels by two specific polymorphisms, 5A/6A
and C/T, respectively, with their gene promoters (3,4). A common
variant in the promoter region of the human MMP-3 gene with
one allele having a run of five adenines (5A) and the other
having six adenines (6A) has been reported as an important
genetic risk factor for premature myocardial infarction (5), carotid stenosis (6) and in-stent restenosis (7). Another MMP is gelatinase B (MMP-9), which
is characterized by a broad substrate specificity and high
expression in the disruption-prone regions of atherosclerotic
plaques (8). It has been reported that
the T allele of the −1562C/T promoter polymorphism
was associated with an approximate 2-fold higher promoter activity
(4).
In the current study, whether the 5A/6A
polymorphism in the MMP-3 gene and the C/T
polymorphism in the MMP-9 gene, as well as other sequence
variants influenced the presence of CAD was investigated.
Materials and methods
Study population
The study group consisted of 200 consecutive
patients with angiographically diagnosed CAD and 200 consecutive
patients with angiographically normal coronary arteries, and the
two groups were recruited from the Department of Cardiology,
Cumhuriyet University Hospital (Sivas, Turkey). All patients
exhibited stable symptoms. The study was conducted in accordance
with the Declaration of Helsinki. The study protocol was approved
by the Ethics Committee of the Medical Faculty of Cumhuriyet
University (approval no. 2011–02/04) and each participant provided
written informed consent.
Coronary angiography and quantitative
analysis
Coronary angiography and interventional procedures
were performed using standard techniques via transfemoral or
transradial approaches. All imaging analyses were performed by two
experienced interventional cardiologists. The diagnosis of CAD was
established angiographically in the presence of >50% stenosis in
≥1 of the three major coronary arteries or their major branches,
and all the patients had stable CAD. Routine intracoronary
injections of nitroglycerin were administered to avoid artery
spasm.
Blood samples and genotyping
All venous blood samples (2 ml) were obtained upon
patient presentation. After an overnight fast, antecubital venous
blood samples (2 ml) were collected in vacuum tubes between 08:00
and 10:00 a.m. Blood samples were brought to the Genetic Laboratory
(Cumhuriyet University Hospital) within 10 min. The DNA was
extracted from the whole blood of the patient and control groups
using a standard phenol-chloroform method according to Sambrook and
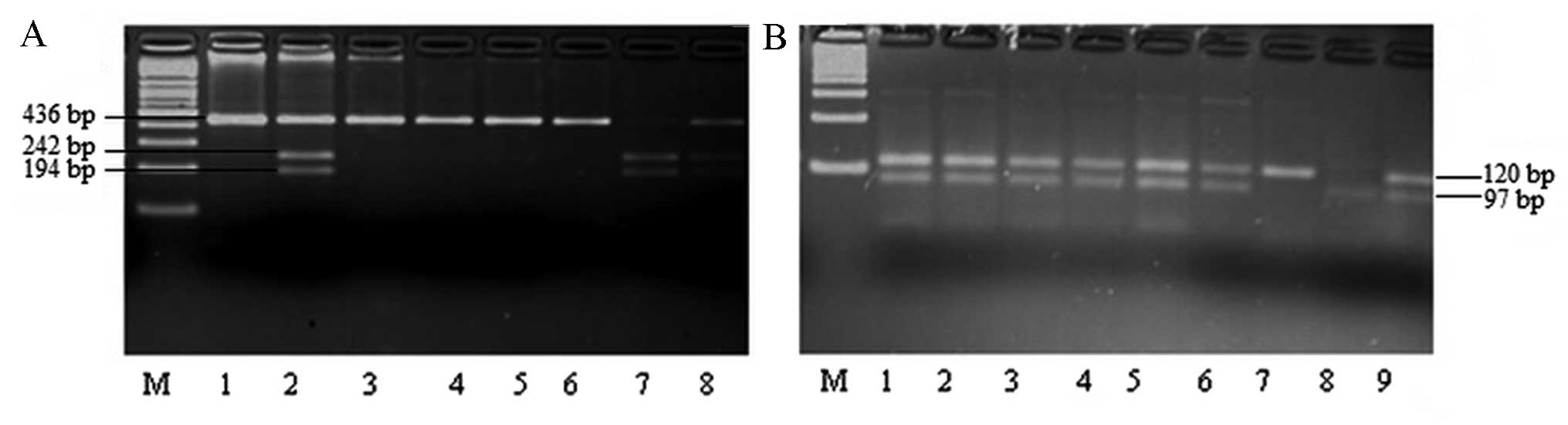
Russell (9). The MMP-3 and
MMP-9 genotypes were determined using polymerase chain
reaction (PCR)-based restriction fragment length polymorphism
(RFLP). The PCR reaction was performed in a total volume of 25 µl
containing ~100 ng genomic DNA, 200 mM deoxynucleotide
triphosphates (dNTPs), 0.2 mM of each of the synthesized primers
(Iontek Biotechnology, Istanbul, Turkey; Table I), 1X reaction buffer (MBI Fermentas,
St. Leon-Rot, Germany), 1.5 mM MgCl2, and 2-unit Taq
polymerase (MBI Fermentas). The temperature profile for the
35-cycle amplification reaction using a Techne TC-4000 thermal
cycler (Techne; Bibby Scientific Ltd., Staffordshire, UK) was as
follows: Initial denaturation at 94°C for 5 min, denaturation at
94°C for 30 sec, annealing according to the temperatures in
Table I and extension at 72°C for 1
min, with a final extension at 72°C for 5 min. Amplification
products (5 µl) were resolved in 2% agarose gel (Sigma-Aldrich, St.
Louis, MO, USA). MMP-3 and MMP-9 PCR products (10 µl)
were digested with 10 units of restriction enzymes, SphI and
XmnI (MBI Fermentas; Table I).
The fragments and uncut products were separated using 4% agarose
gel electrophoresis (45 min, 100 mA and 50 V) and visualized on a
Safe Imager™ 2.0 Blue Light Transilluminator (Thermo Fisher
Scientific, Inc., Waltham, MA, USA) after staining with ethidium
bromide (Fig. 1).
 | Table I.Primer sequences, annealing
temperatures and restriction enzymes of two polymorphisms. |
Table I.
Primer sequences, annealing
temperatures and restriction enzymes of two polymorphisms.
| Polymorphism | Primer
sequence | Annealing
temperature (°C) | Restriction
enzyme |
|---|
| MMP-9 | F:
5′-GCCTGGCACATAGTAGGCCC-3′ | 56 | SphI |
| −1562 C>T | R:
5′-CTTCCTAGCCAGCCGGCATC-3′ |
|
|
| MMP-3 | F: 5′-GAT TACAGACAT
GGG TCACA-3′ | 53 | XmnI |
| −1612 5A/6A | R:
5′-TTTCAATCAGGACAAGACGAAGTTT-3′ |
|
|
Statistical analysis
Statistical analysis was performed using SPSS 16.0
(SPSS, Inc., Chicago, IL, USA). The variables were investigated
using the One Sample Kolmogorov-Smirnov test to establish whether
there was normal distribution. Continuous variables were expressed
as means ± standard deviation or medians (minimum-maximum) in the
presence of abnormal distribution, and the categorical variables
were presented as percentages. Comparisons between groups of
patients were made using a Pearson χ2 test for
categorical variables, Student's t-test for normally distributed
continuous variables and the Mann-Whitney U test when the
distribution was skewed. Odds ratio (OR) and 95% confidence
intervals (CIs) were calculated for each variable to compare the
two groups. Analysis of haplotype frequencies was performed using
the EH program (www.jurgott.org/linkage/eh.htm; Rockefeller
University, New York, NY, USA), which assesses and estimates
linkage disequilibrium between different markers or between a
disease locus and markers (10). The
EH program estimates allele frequencies for each marker and
haplotype frequencies are estimated via allelic association. In all
cases, P<0.05 was considered to indicate a statistically
significant difference.
Results
Clinical and demographic
parameters
The clinical and demographic parameters of patients
in the CAD and control groups are presented in Table II. The distribution of age, gender,
smoking status, diabetes and hypercholesterolemia status between
the CAD and control groups were not significantly different, except
for hypertension (Table II). The
presence of hypertension was significantly higher in the CAD group
when compared with the control group (63.5 vs. 27.5%;
P<0.001).
| Table II.Demographic and clinical parameters
of patients with CAD and control subjects. |
Table II.
Demographic and clinical parameters
of patients with CAD and control subjects.
| Variable | CAD group
(n=200) | Control group
(n=200) | Odds ratio (95%
CI) | P-value |
|---|
| Age, years | 60.2±7.4 | 58.3±7.7 |
|
0.059 |
| Gender |
|
|
|
|
| Female,
n (%) | 65
(32.5) | 83
(41.5) |
|
|
| Male, n
(%) | 135 (67.5) | 117 (58.5) | 1.67
(0.98–2.87) |
0.058 |
| Smoking status |
|
|
|
|
|
Non-smoker, n (%) | 98
(49.0) | 113 (56.5) |
|
|
| Smoker,
n (%) | 102 (51.0) | 87
(43.5) | 1.35
(0.91–2.00) |
0.133 |
| Hypertension |
|
|
|
|
| Absent,
n (%) | 73
(36.5) | 145 (72.5) |
|
|
|
Present, n (%) | 127 (63.5) | 55
(27.5) | 4.58
(3.00–7.00) | <0.001 |
| Diabetes
mellitus |
|
|
|
|
| Absent,
n (%) | 121 (60.5) | 131 (65.5) |
|
|
|
Present, n (%) | 79
(39.5) | 69
(34.5) | 1.24
(0.82–1.86) |
0.300 |
|
Hypercholesterolemia |
|
|
|
|
| Absent,
n (%) | 128 (64.0) | 145 (72.5) |
|
|
|
Present, n (%) | 72
(36.0) | 55
(27.5) | 1.48
(0.97–2.26) |
0.068 |
Allelic and genotype frequencies
The allele and genotype distributions of
MMP-3 and MMP-9 genes in the CAD and control groups
are presented in Table III. The
distribution of the MMP-3 allelic frequency differed
significantly between the CAD and control groups (P<0.001; OR=
2.18). Comparison of the 5A/5A genotype with the wild-type
6A/6A genotype of the MMP-3 gene revealed that the
variation between CAD patients and control subjects was
statistically significant (P=0.005; OR=2.92). Distribution of the
MMP-9 gene allelic and genotype frequency was similar
between the CAD and control groups (Table III).
| Table III.Risk estimates of alleles and
genotypes for MMP polymorphisms in the two study populations. |
Table III.
Risk estimates of alleles and
genotypes for MMP polymorphisms in the two study populations.
| Gene | CAD group, n
(%) | Control group, n
(%) | OR (95% CI) | P-value |
|---|
| MMP-3 |
|
| 6A | 269 (67.3) | 327 (81.8) |
Referencea | – |
| 5A | 131 (32.8) | 73
(18.3) | 2.18
(1.57–3.03) | <0.001 |
|
6A/6A | 90
(45.0) | 138 (69.0) |
Referencea | – |
|
6A/5A | 89
(44.5) | 51
(25.5) | 0.97
(0.55–1.72) |
0.929 |
|
5A/5A | 21
(10.5) | 11
(5.5) | 2.92
(1.34–6.36) |
0.005 |
| 6A/5A
+5A/5A | 110 (55.0) | 62
(3.1) | 2.72
(1.80–4.09) | <0.001 |
| MMP-9 |
|
| C | 354 (88.5) | 351 (87.8) |
Referencea | – |
| T | 46
(11.5) | 49
(12.3) | 0.93
(0.60–1.42) |
0.743 |
| CC | 158 (79.0) | 154 (77.0) |
Referencea | – |
| CT | 38
(19.0) | 43
(21.5) | 0.86
(0.52–1.40) |
0.550 |
| TT | 4
(2.0) | 3
(1.5) | 1.30
(0.28–5.90) |
0.517 |
|
CT+TT | 42
(21.0) | 46
(23.0) | 0.89
(0.55–1.42) |
0.629 |
Haplotype analysis
Haplotype analysis was conducted for all the
possible haplotypes, and all four haplotypes determined by the two
single nucleotide polymorphisms, were observed in the study
samples. Haplotype frequencies of the MMP-3 and MMP-9
genes in the study population are presented in Table III. Distribution of the 5A-C
haplotype frequency between the CAD and control groups was
statistically significant (P=0.001). The distributions of
6A-C and 5A-T haplotype frequencies were similar
between the CAD and control groups (P=0.896 and P=0.152,
respectively; Table IV).
| Table IV.Frequencies of alleles and genotypes
for MMP polymorphisms in the two study populations. |
Table IV.
Frequencies of alleles and genotypes
for MMP polymorphisms in the two study populations.
| Frequency of
haplotypes |
|
|---|
|
|
|---|
| MMP-3 | MMP-9 | CAD group, n
(%) | Control group, n
(%) | OR (95% CI) | P-value |
|---|
| 6A | C | 117 (29.3) | 144 (36.0) |
Referencea | – |
| 6A | T | 17 (4.3) | 20 (5.0) | 1.04
(0.52–2.08) | 0.896 |
| 5A | C | 58
(14.5) | 32 (8.0) | 2.23
(1.35–3.66) | 0.001 |
| 5A | T | 8
(2.0) | 4
(1.0) | 2.46
(0.72–8.37) | 0.152 |
Risk estimates with regards to the
demographic and clinical parameters
The risk estimates of the MMP-3 polymorphisms
were calculated for the demographic and clinical parameters, and
are presented in Table V. As the
allele and genotype frequencies of MMP-9 were not
statistically significant, the same calculations for risk
estimation were not performed for the MMP-9 polymorphisms.
Female patients in the CAD group exhibited significantly higher
frequencies of the 6A/5A genotype compared with the female
patients in the control group (P<0.001; OR=4.59). The male
patients in the CAD group demonstrated statistically higher
frequencies of 6A/5A and 5A/5A genotypes compared
with the male patients in the control group [P=0.001 (OR=1.98) and
P=0.035 (OR=2.51), respectively]. Current smokers in the CAD group
demonstrated a higher frequency of the 6A/5A genotype
compared with current smokers in the control group (P=0.001;
OR=2.81). When compared with the control subjects, CAD patients
with hypertension had significantly higher frequencies of the
6A/5A and 5A/A genotypes [P=0.003 (OR=2.78) and
P=0.006 (OR=10.23), respectively]. Patients with
hypercholesterolemia in the CAD group had statistically different
frequencies of 6A/5A and 5A/5A genotypes compared
with the control subjects with hypercholesterolemia [P=0.016
(OR=2.48) and P=0.025 (OR=8.69), respectively; Table V].
| Table V.Risk estimates for MMP-3
polymorphisms in demographic and clinical parameters. |
Table V.
Risk estimates for MMP-3
polymorphisms in demographic and clinical parameters.
| Variable | CAD group, n
(%) | Control group, n
(%) | Odds ratio (95%
CI) | P-value |
|---|
| Female |
|
|
6A/6A | 36 (55.4) | 70 (84.3) |
Referencea | – |
|
6A/5A | 26 (40.0) | 11 (13.3) | 4.59
(2.04–10.34) | <0.001 |
|
5A/5A | 3 (4.6) | 2 (2.4) | 2.91
(0.46–18.25) |
0.342 |
| Male |
|
|
6A/6A | 54 (40.0) | 68 (58.1) |
Referencea | – |
|
6A/5A | 63 (46.7) | 40 (34.2) | 1.98
(1.16–3.38) |
0.011 |
|
5A/5A | 18 (13.3) | 9 (7.7) | 2.51
(1.04–6.04) |
0.035 |
| Smoker |
|
|
6A/6A | 44 (43.1) | 58 (66.7) |
Referencea | – |
|
6A/5A | 47 (46.1) | 22 (25.3) | 2.81
(1.48–5.34) |
0.001 |
|
5A/5A | 11 (10.8) | 7 (8.0) | 2.07
(0.74–5.77) |
0.158 |
| Hypertension |
|
|
6A/6A | 52 (41.0) | 38 (69.1) |
Referencea | – |
|
6A/5A | 61 (48.0) | 16 (29.1) | 2.78
(1.39–5.56) |
0.003 |
|
5A/5A | 14 (11.0) | 1 (1.8) | 10.23
(1.28–81.19) |
0.006 |
| Diabetes
mellitus |
|
|
6A/6A | 40 (50.6) | 44 (63.8) |
Referencea | – |
|
6A/5A | 32 (40.5) | 20 (29.0) | 1.76
(0.87–3.55) |
0.114 |
|
5A/5A | 7 (8.9) | 5 (7.2) | 1.54
(0.45–5.24) |
0.487 |
|
Hypercholesterolemia |
|
|
6A/6A | 29 (40.3) | 36 (65.5) |
Referencea | – |
|
6A/5A | 36 (50.0) | 18 (32.7) | 2.48
(1.17–5.24) |
0.016 |
|
5A/5A | 7 (9.7) | 1 (1.8) | 8.69
(1.01–74.71) |
0.025 |
Discussion
In the present study, the associations between CAD
and MMP-3 and MMP-9 polymorphisms were investigated.
The patients with CAD exhibited a higher frequency of the 5A
allele, 5A/5A genotype and 6A/5A+5A/5A
genotype of the MMP-3 gene compared with the patients with
normal coronary arteries. The distribution of allele and genotype
frequencies of the MMP-9 gene was similar between the CAD
and control groups. However, there was a strong link between the
CAD groups as compared to patients with normal coronary arteries in
terms of 5A-C haplotype of the MMP-3 and MMP-9
genes.
Stromelysin-1, also termed MMP-3, catalyses the
breakdown of extracellular matrix macromolecules, including
proteoglycans, different types of collagen, fibronectin, and
laminin, and facilitates the conversion of other MMPs, such as
collagenase-1 (MMP-1), collagenase-2 (MMP-8), matrilysin (MMP-7),
and 92-kDa gelatinase (MMP-9), from their inactive to their
proteolytically active forms (11).
The human stromelysin-1 gene contains a common promoter
polymorphism, characterized by runs of five or six adenosines,
located at nucleotide positions 1171–1175 or 1171–1176,
respectively, upstream from the start site of transcription
(11). Its expression is primarily
regulated at the level of transcription 5. Due to its important
function in extracellular matrix turnover, stromelysin-1
polymorphism 5A/6A was extensively investigated in patients with
CAD (12).
An association between the MMP-3 5A/6A
promoter polymorphism and atherosclerosis was first described in
1995, and the 6A/6A genotype was associated with greater
progression of coronary atherosclerosis (13). It was shown that the 6A/6A
genotype was associated with a greater progression of CAD following
angioplasty (14). Regarding MMP-3,
certain studies have linked the 6A allele to a higher risk
of rapid progression of the atherosclerotic process (15,16). Three
independent studies have found that the patients carrying the 6A/6A
genotype exhibited more progression of angiographically detectable
lesions in documented CAD (13,15).
However, this association was not supported by clinical studies
investigating stent restenosis subsequent to angioplasty and
MMP-3 gene polymorphisms (11).
Among the MMPs that are expressed in atheroma is
MMP-3, which has a broad substrate specificity and activates
other enzymes in the MMP family (5).
In various cross-sectional studies investigating patients with
angiographically documented CAD, it was demonstrated that patients
with the 6A/6A genotype have more coronary arteries with
significant stenosis when compared with those of the 5A/5A
or 5A/6A genotype (5,17,18).
However, in the present study, 5A/5A and 6A/5A+5A/5A
genotypes were demonstrated to be strongly associated with CAD.
The expression of MMP-9 is regulated
primarily at the transcription level, and it was investigated in
studies associated with CAD. Zhang et al (4) reported a functional 21562C/T
polymorphism in the promoter region of MMP-9. The T
allele was found to be associated with complicated coronary
lesions, and carriers of the T allele demonstrated greater
levels of the MMP-9 mRNA protein, as well as stiffer, large
arteries (1). Consistent with the
result reported by Blankenberg et al (19), the present study found that the
MMP-9 C/T polymorphism is not associated with an increased
risk of CAD.
A previous study suggested that haplotype analysis
is frequently more powerful than analysis using single
polymorphisms (20). In the current
study, an association between the 5A-C haplotype and an
increased risk of CAD was identified.
There were certain limitations of the present study.
The serum levels of MMP-3 and MMP-9 were not measured. In addition,
although the study subjects were recruited prospectively, this
study was a case-control study and selection bias was not excluded.
Furthermore, clinical outcomes of the present findings were not
investigated. Therefore, large-scale, multicenter randomized
clinical studies are required to assess the effect of the
MMP-3 polymorphism on clinical cardiovascular outcomes. In
conclusion, the present study demonstrated that the 5A/5A
and 6A/5A+5A/5A alleles and the 5A-C haplotype of the
MMP-3/MMP-9 genes were associated with an increased
risk of CAD.
Acknowledgements
The present study was supported by the Research
Council of Cumhuriyet University (Sivas, Turkey; CUBAP project no.
F-340).
Glossary
Abbreviations
Abbreviations:
|
CAD
|
coronary artery disease
|
|
CI
|
confidence interval
|
|
MMP
|
matrix metalloproteinase
|
|
OR
|
odds ratio
|
|
PCR
|
polymerase chain reaction
|
|
RFLP
|
restriction fragment length
polymorphism
|
References
|
1
|
Abilleira S, Bevan S and Markus HS: The
role of genetic variants of matrix metalloproteinases in coronary
and carotid atherosclerosis. J Med Genet. 43:897–901. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen QJ, Lu L, Peng WH, Hu J, Yan XX, Wang
LJ, Zhang Q, Zhang RY and Shen WF: Polymorphisms of MMP-3 and
TIMP-4 genes affect angiographic coronary plaque progression in
non-diabetic and type 2 diabetic patients. Clin Chim Acta.
405:97–103. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ye S, Gale CR and Martyn CN: Variation in
the matrix metalloproteinase-1 gene and risk of coronary heart
disease. Eur Heart J. 24:1668–1671. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang B, Ye S, Herrmann SM, Eriksson P, de
Maat M, Evans A, Arveiler D, Luc G, Cambien F, Hamsten A, et al:
Functional polymorphism in the regulatory region of gelatinase B
gene in relation to severity of coronary atherosclerosis.
Circulation. 99:1788–1794. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Beyzade S, Zhang S, Wong YK, Day IN,
Eriksson P and Ye S: Influences of matrix metalloproteinase-3 gene
variation on extent of coronary atherosclerosis and risk of
myocardial infarction. J Am Coll Cardiol. 41:2130–2137. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rauramaa R, Väisänen SB, Luong LA,
Schmidt-Trücksäss A, Penttilä IM, Bouchard C, Töyry J and Humphries
SE: Stromelysin-1 and interleukin-6 gene promoter polymorphisms are
determinants of asymptomatic carotid artery atherosclerosis.
Arterioscler Thromb Vasc Biol. 20:2657–2662. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liu PY, Li YH, Chan SH, Lin LJ, Wu HL, Shi
GY and Chen JH: Genotype-phenotype association of matrix
metalloproteinase-3 polymorphism and its synergistic effect with
smoking on the occurrence of acute coronary syndrome. Am J Cardiol.
98:1012–1017. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnson C and Galis ZS: Matrix
metalloproteinase-2 and −9 differentially regulate smooth muscle
cell migration and cell-mediated collagen organization.
Arterioscler Thromb Vasc Biol. 24:54–60. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sambrook J and Russell DW: Purification of
nucleic acids by extraction with phenol: chloroform. CSH Protoc.
2006(pii): pdb.prot4455. 2006.
|
|
10
|
Xie X and Ott J: Testing linkage
disequilibrium between a disease gene and marker loci. Am J Hum
Genet. 53:1107–1113. 1993.PubMed/NCBI
|
|
11
|
Hoppmann P, Koch W, Schömig A and Kastrati
A: The 5A/6A polymorphism of the stromelysin-1 gene and restenosis
after percutaneous coronary interventions. Eur Heart J. 25:335–341.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Koch W, de Waha A, Hoppmann P, Schömig A
and Kastrati A: Haplotypes and 5A/6A polymorphism of the matrix
metalloproteinase-3 gene in coronary disease: Case-control study
and a meta-analysis. Atherosclerosis. 208:171–176. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ye S, Watts GF, Mandalia S, Humphries SE
and Henney AM: Preliminary report: Genetic variation in the human
stromelysin promoter is associated with progression of coronary
atherosclerosis. Br Heart J. 73:209–215. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Humphries S, Bauters C, Meirhaeghe A,
Luong L, Bertrand M and Amouyel P: The 5A6A polymorphism in the
promoter of the stromelysin-1 (MMP3) gene as a risk factor for
restenosis. Eur Heart J. 23:721–725. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
de Maat MP, Jukema JW, Ye S, Zwinderman
AH, Moghaddam PH, Beekman M, Kastelein JJ, van Boven AJ, Bruschke
AV, Humphries SE, et al: Effect of the stromelysin-1 promoter on
efficacy of pravastatin in coronary atherosclerosis and restenosis.
Am J Cardiol. 83:852–856. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Humphries SE, Luong LA, Talmud PJ, Frick
MH, Kesäniemi YA, Pasternack A, Taskinen MR and Syvänne M: The
5A/6A polymorphism in the promoter of the stromelysin-1 (MMP-3)
gene predicts progression of angiographically determined coronary
artery disease in men in the LOCAT gemfibrozil study. Lopid
Coronary Angiography Trial. Atherosclerosis. 139:49–56. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hirashiki A, Yamada Y, Murase Y, Suzuki Y,
Kataoka H, Morimoto Y, Tajika T, Murohara T and Yokota M:
Association of gene polymorphisms with coronary artery disease in
low- or high-risk subjects defined by conventional risk factors. J
Am Coll Cardiol. 42:1429–1437. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Schwarz A, Haberbosch W, Tillmanns H and
Gardemann A: The stromelysin-1 5A/6A promoter polymorphism is a
disease marker for the extent of coronary heart disease. Dis
Markers. 18:121–128. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Blankenberg S, Rupprecht HJ, Poirier O,
Bickel C, Smieja M, Hafner G, Meyer J, Cambien F and Tiret L:
AtheroGene Investigators: Plasma concentrations and genetic
variation of matrix metalloproteinase 9 and prognosis of patients
with cardiovascular disease. Circulation. 107:1579–1585. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Johnson GC, Esposito L, Barratt BJ, Smith
AN, Heward J, Di Genova G, Ueda H, Cordell HJ, Eaves IA, Dudbridge
F, et al: Haplotype tagging for the identification of common
disease genes. Nat Genet. 29:233–237. 2001. View Article : Google Scholar : PubMed/NCBI
|