Introduction
Pulmonary fibrosis (PF) is a type of diffuse
parenchymal lung disease characterized by chronic inflammation and
progressive parenchymal fibrosis (1).
PF with unclear etiology is known as idiopathic PF (IPF). The
incidence of IPF increases worldwide and is similar to that of
certain types of cancer, including stomach and liver cancer
(2–4).
IPF results in deteriorated lung function and ultimately leads to
respiratory failure. Patients with IPF have a poor prognosis, with
a median survival of 3 years, which is worse than certain types of
cancer (5). The diagnosis of IPF is
established after excluding specific known causes of PF and a
pattern so-called usual interstitial pneumonia (6).
Numerous drugs, such as bleomycin, are known to
contribute to lung injury and PF. Bleomycin is a chemotherapeutic
drug, with lung injury and dose-independent PF observed in 10% of
bleomycin users. Bleomycin is commonly used to establish an animal
model of PF (7,8). Microscopically, lung injury is followed
by inflammation, excessive accumulation and deposition of
extracellular matrix (ECM) resulting in the thickening of alveolar
interval. Matrix metalloproteinases (MMPs) and tissue matrix
metalloproteinase inhibitors (TIMPs) are the main proteases
involved in the degradation and remolding of the ECM (9). As a non-selective dual endothelin-1
receptor antagonist, bosentan protects against acute lung injury
resulting from PF by reducing inflammation factor release (10). Bosentan also improves PF induced by
bleomycin and reduces the expression levels of MMP-2 gene (11). Although both MMP-2 and MMP-9 are
gelatinases, only MMP-9 has been shown to be correlated with the
degree of bleomycin-induced PF, while its serum levels decrease in
patients with pulmonary arterial hypertension and increase
following treatment with bosentan (12). However, the roles of MMP-9 and TIMP1 in
bosentan treatment for PF have not been studied. Therefore, the aim
of the present study was to investigate the effects of bosentan on
MMP-9 and TIMP1 expression in a model of bleomycin-induced PF in
rats.
Materials and methods
Ethical approval
All animal studies and procedures were approved by
the Institutional Animal Use and Care Committee of Sun Yat-sen
University (Guangzhou, China; animal welfare assurance no. SCXK
2011-0029; experiment welfare assurance no. SYXK 2012-0081). All
rats were maintained according to institutional guidelines. Animal
procedures were performed in compliance with the Institutional
Standards for Humane Care and Use of Laboratory Animals.
Animals
A total of 48 specific pathogen-free, healthy young
rats, aged 7 weeks (weight range, 182–248 g) were obtained from the
Center of Experimental Animal of Sun Yat-sen University, and raised
in a room with windows (temperature at 22±20°C, humidity 55±5%,
natural light/dark, food and water no limited). All rats were
randomly assigned to the following groups: Saline (control; C
groups), bleomycin-induced PF (F groups) and bleomycin-induced PF
followed by bosentan treatment (B groups). The C, F and B groups
were also randomly treated for two different time durations prior
to sacrifice, including rats treated for 2 weeks (namely groups C1,
F1 and B1) and for 4 weeks (namely groups C2, F2 and B2). All rats
were housed in a specific pathogen-free facility and screened
regularly for pathogens. Bleomycin-induced PF rats were
anesthetized by isoflurane inhalation prior to treating with
intranasal injection of 50 ml sterile saline solution containing 6
U/kg body weight (7.5 mg/kg body weight) bleomycin (Nippon Kayaku,
Tokyo, Japan) (13). Rats in the B
groups were then treated with bosentan on the next day (B1) or 15th
day (B2) after bleomycin treatment. Control rats (C1 and C2)
received a single intratracheal dose of sterile saline alone. The
rats were monitored and weighed daily for the duration of the
experiment. Animals were euthanized by CO2 asphyxiation
at the indicated time-points.
Blood collection
Blood was collected by inferior vena cava puncture
following euthanasia. After standing at room temperature for 30
mins, the blood was centrifuged for 5 min at 1,358.37 × g at 4°C.
The supernatants were collected and stored at −20°C until further
use.
Histopathological analysis of lung
tissue
The lungs of rats were perfused with 10 ml cold
phosphate-buffered saline before sacrifice (C1, F1, B1 group rats
after 2 weeks of treatment, and C2, F2, B2 group rats after 4 weeks
of treatment) and then harvested. The right lung lobes were placed
in 10% formalin and embedded in paraffin for sectioning (25×25 mm).
Following deparaffinization, rehydration and washing in deionized
water, the slides containing serial sections were stained with
H&E or Masson's trichrome according to routine procedures
(14).
Alveolitis and fibrosis were individually assessed
by lung histology using the semiquantitative grading system
described by Szapiel et al (15): 0, no alveolitis/fibrosis was observed;
1 (mild), focal lesions occupying <25% or <20% (for
alveolitis and fibrosis, respectively) of the lung were detected in
the alveolar septum; 2 (moderate), widespread alveolitis or
fibrosis involving 25–50% or 20–50%, respectively, of the lung was
observed; and 3 (severe), a diffused alveolitis or fibrosis
spanning >50% of the lung was observed, with occasional
consolidation of air spaces and patches of hemorrhagic areas within
the interstitium. The entire lung section was reviewed under a
lower power field (Olympus, BX-51; magnification, ×100). In total,
20 random microscopic fields per section were examined, and a score
ranging between 0 and 3 was assigned. All assessments were
performed in double-blind manner.
MMP-9 and TIMP-1 concentrations
determined by ELISA
The concentrations of MMP-9 (e02m0329) and TIMP-1
(e02t0047) in the plasma of rats in the various groups were
measured by ELISA kits (Shanghai BlueGene Biotech Co., Ltd.,
Shanghai, China) according to the manufacturer's instructions.
Statistical analysis
Evaluation of statistically significant differences
between the groups was performed using Student's t-test and
analysis of variance. Data are expressed as the mean ± standard
deviation, as indicated. All analyses of data were performed using
SPSS software for Windows (version 13.0; SPSS, Inc., Chicago, IL,
USA) and a P<0.05 was considered to indicate a statistically
significant difference.
Results
Changes in body weight
Table I shows the
effect of bosentan on the body weight of bleomycin-administered
groups of rats. Compared with the normal control rats (C1 and C2),
rats administered bleomycin alone (F1 and F2) or along with
bosentan treatment after 15 days (B2) had a lower increase in body
weight between the beginning of the experiments and sacrifice (C1
vs. F2 and B2; P=0.001, others P<0.0001). By contrast, the group
treated with bosentan on the day following bleomycin administration
(B1) demonstrated a similar increase in body weight to the control
groups (C1 and C2), and a significantly higher body weight increase
when compared with the F1, F2 and B2 groups (B1 vs. C1, P=0.706; B1
vs. C2, P=0.858; B1 vs. F1, P<0.0001; B1 vs. F2, P=0.003; and B1
vs. B2, P=0.002). However, the body weight of B2 rats showed no
significant change compared with the bleomycin-administrated groups
without bosentan treatment (F2; P=0.682).
 | Table I.Efficacy of bosentan on body weight of
bleomycin-induced fibrosis rats. |
Table I.
Efficacy of bosentan on body weight of
bleomycin-induced fibrosis rats.
| Group | Body weight increase,
g |
|---|
| C1 |
110.38±28.32a |
| C2 |
100.50±16.02b |
| F1 |
22.75±5.82c |
| F2 |
61.25±18.68d |
| B1 |
99.63±22.15e |
| B2 |
57.25±19.61 |
Bosentan attenuates bleomycin-induced
alveolitis and lung fibrosis
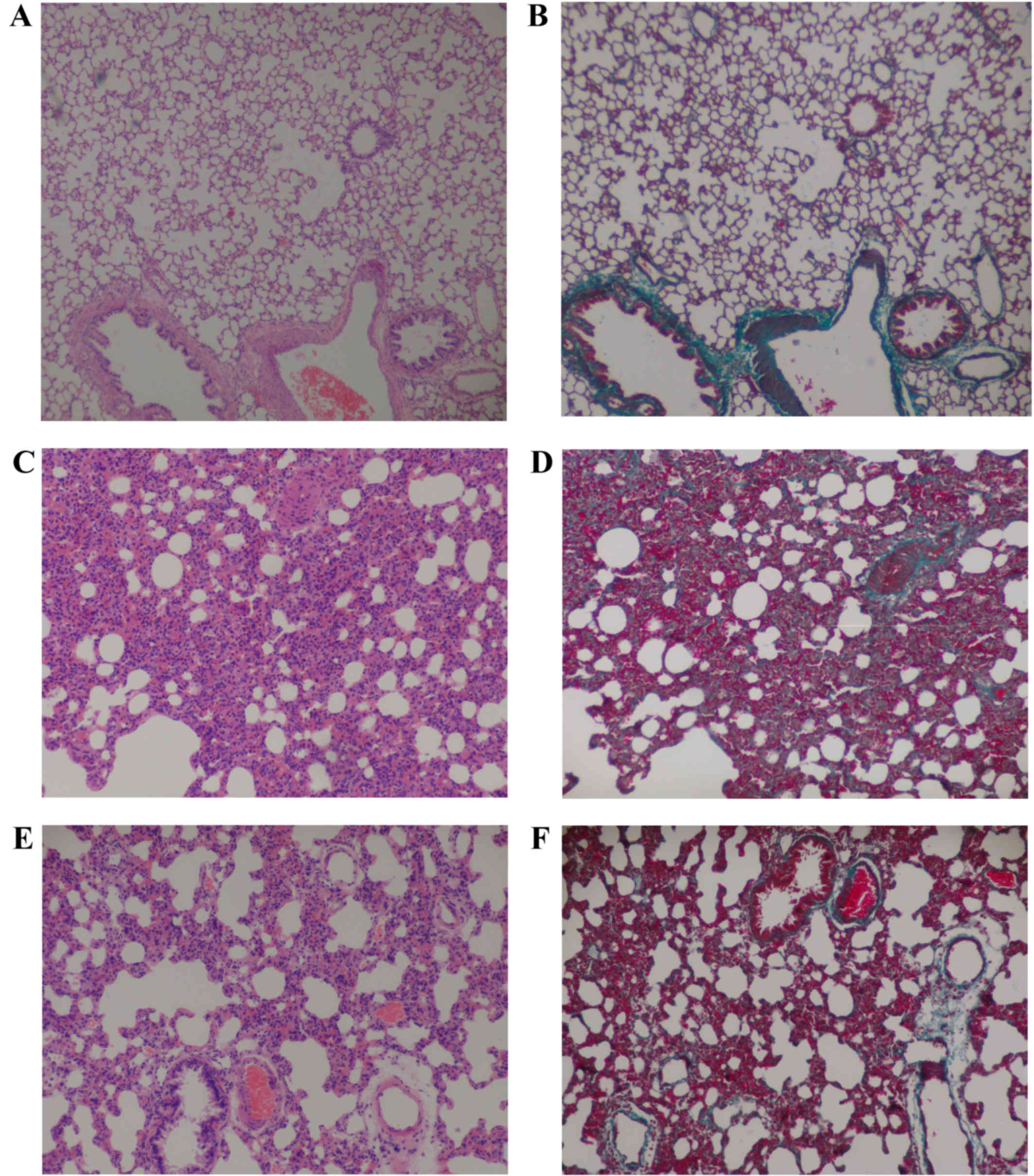
Microscopically, the histopathological changes in
the lung tissues between the control (C groups), bleomycin-induced
PF (F groups) and bleomycin-induced PF treated with bosentan (B
groups) rats were evaluated. The results demonstrated that
bleomycin-induced alveolitis and PF were inhibited by bosentan
treatment on the next day after bleomycin (Table II). Sections of the control groups had
a normal structure without alveolitis and PF (Fig. 1A and B). The most severe alveolitis was
identified in group F1, with the lung sections showing infiltration
of numerous inflammatory cells, including neutrophilic
granulocytes, lymphocytes and macrophages, in the interstitial lung
and alveoli. Interstitial edema, diffuse hemorrhage and thickened
alveolus interstitium were also observed in the F1 group tissues.
In addition, the most significant inhibition of alveolitis was
demonstrated when bosentan was administered on the day after
bleomycin (B1), which suggested that early administration of
bosentan had a better effect than later administration (as in B2).
The most severe fibrosis was observed in group F2; those sections
showed a thickened alveolus interstitium, and accumulation of
collagen and fibrosis, with reduced number of inflammatory cells.
Therefore, bosentan treatment for PF on the following day from
bleomycin administration in rats may assist in preventing certain
pathological changes induced by bleomycin. Furthermore, reduced
inflammatory cell infiltration and collagen deposition was detected
in B1 group. However, no significant reduction in alveolitis, lung
fibrosis and collagen fibers were observed in group B2, which
suggested that bosentan was less effective if administered at a
later stage after bleomycin (Fig. 1;
Table II).
| Table II.Efficacy of bosentan on
bleomycin-induced alveolitis and fibrosis rats. |
Table II.
Efficacy of bosentan on
bleomycin-induced alveolitis and fibrosis rats.
| Group | Grading of
alveolitis | Grading of
fibrosis |
|---|
| C1a |
0.1±0.4 |
0.0±0.0 |
| C2b |
0.0±0.0 |
0.0±0.0 |
| F1c |
2.6±0.5 |
1.4±0.5 |
| F2d |
2.3±0.7 |
2.8±0.5 |
| B1e |
1.5±0.8 |
1.8±0.7 |
| B2 |
2.0±0.8 |
2.6±0.5 |
Effect of bosentan treatment on
expression levels of MMP-9 and TIMP-1 in PF lung tissues
The control groups demonstrated the highest
concentration of MMP-9 and MMP-9/TIMP-1 ratio, and the lowest
concentration of TIMP-1 in the blood serum of rats. However, the
concentration of MMP-9 was significantly reduced in all the
bleomycin-induced PF groups treated with or without bosentan
compared with the control rats (P<0.05; Table III). In addition, the concentration
of TIMP-1 in all the bleomycin-induced PF groups treated with or
without bosentan was significantly increased compared with that in
the control rats (Table III). And
the ratio of MMP-9/TIMP-1 of longer survival (F2, B2) was
significantly lower than that of shorter survival (F1).
| Table III.Efficacy of bosentan on
bleomycin-induced MMP-9 and TIMP-1 of rats. |
Table III.
Efficacy of bosentan on
bleomycin-induced MMP-9 and TIMP-1 of rats.
| Group | MMP-9 (µg/l) | TIMP-1 (µg/l) | MMP-9/TIMP-1 |
|---|
| C1a |
4.14±0.86 |
0.35±0.16 |
14.34±8.67 |
| C2b |
4.39±0.75 |
0.32±0.10 |
14.72±4.02 |
| F1c |
1.57±0.85 |
0.70±0.08 |
2.29±1.29 |
| F2d |
0.29±0.08 |
1.18±0.51 |
0.28±0.12 |
| B1e |
1.35±0.55 |
0.48±0.16 |
3.11±1.58 |
| B2 |
0.60±0.20 |
0.75±0.18 |
0.88±0.42 |
Between the bleomycin-induced PF groups, F2 showed a
significantly lower MMP-9 concentration and MMP-9/TIMP-1 ratio, and
a higher concentration of TIMP-1 compared with the F1 group
(P<0.05). Also, B2 showed a lower MMP-9 and higher MMP-9/TIMP-1
ratio compared with B1 (P<0.05).
Discussion
Bleomycin, as an anticancer drug for a number of
human malignancies, is commonly used as a lung fibrosis inducer in
bleomycin-rodent animal model (16).
In the present study, a Wistar rat model of PF was established by
administration a single dose of bleomycin sulfate by intratracheal
instillation. A lower body weight increase was observed in the
bleomycin-administrated groups without bosentan and the group
bosentan treated on the 15th day compared with that of control
rats. This change in the body weight maybe attributed to the
progression of the fibrosis (17).
When treated with bosentan on the day after bleomycin
administration, the rats showed a higher body weight increase
compared with the bleomycin induced groups without bosentan
treatment, the group with bosentan treated on the 15th day, and a
similar body weight increase to the control groups. In addition, no
significant difference was detected between the rats treated with
bosentanon the 15th day after bleomycin administration and the rats
without bosentan treatment after bleomycin administration. Although
bosentan was found to inhibit the effect of the bleomycin-induced
PF on the body weight of rats, treatment with bosentan at a later
time-point resulted in reduced effect. Thus, timely use of bosentan
is important to improve the body weight of bleomycin-administrated
rats.
Bosentan has been demonstrated to be as effective as
dexamethasone for treating lung injury (18). PF is the main side effect of bleomycin
treatment in cancer patients, and the initial damage in the lung
leads to inflammatory cell infiltration into the lung parenchyma.
The local tissue response to bleomycin-induced lung injury in the
present study was evaluated by histopathological examination to
confirm the progression of lung fibrosis in bleomycin-administrated
rats, as well as to demonstrate the possible protective effect of
bosentan against the bleomycin-induced PF. PF is characterized by
fibrous hyperplasia and uncontrolled deposition of ECM substances,
resulting in destruction of the lung tissue structure (19). It was observed that inflammatory cell
infiltration and PF initiation after bleomycin administration in
present study. Similar structural changes have been reported in
other bleomycin-induced lung fibrosis rat models, thus
consolidating the credence of the present experimental model
(17,20–22). The
results of the current study identified that bleomycin-induced
alveolitis and PF were inhibited by bosentan. However, no
significant reductions in alveolitis, lung fibrosis and collagen
fibers were observed in the group treated with bosentan 15 days
after bleomycin administration, which suggested that bosentan was
less effective when administered later. Therefore, early treatment
with bosentan may reduce alveolitis induced by bleomycin.
It has been reported that fibrosis is a consequence
of fibrous hyperplasia subsequent to tissue injury and is known to
be closely associated with remodeling of ECM tissue (23,24). PF is
characterized by inflammatory cell infiltration, fibroblast
differentiation, ECM remodeling and collagen deposition. In
addition, MMPs can be produced and released by the epithelium,
fibroblasts, myofibroblasts and macrophages, while TIMPs are the
inhibitors of MMPs. The activity of MMPs and TIMPs changes with the
tissue condition, being low under normal conditions and increasing
during certain pathological processes, including repair or tumor
development (25). MMP-9, a kind of
gelatinases, plays an important role in human and experimental lung
fibrosis (26). MMP-9 and TIMPs
increase in IPF patients (27,28). Furthermore, it has been reported that
MMP-7 serves a critical role in the induction of PF by bleomycin
(29). In the present study,
bleomycin-treated rats showed reduced levels of MMP-9 and elevated
levels of TIMP-1 when compared with the normal control rats. Thus,
the bleomycin-treated rats also showed a reduction in the
MMP-9/TIMP-1 ratio. These results suggested that the lung injury
induced by bleomycin resulted in reduction of MMP-9, elevation of
TIMP-1, and the imbalance of MMPs and TIMPs, which are known to
promote lung fibrosis and result in increased collagen deposition
and decreased ECM degradation. Although bosentan failed to affect
MMP-9 and TIMP-1 quickly, it decreased the reduction of MMP-9
levels and elevation of TIMP-1 levels. Therefore, timely use of
bosentan may help to protect lung tissues against alveolitis and
fibrosis induced by bleomycin. As the histopathology of
experimental animal models is similarity to PF in humans, bosentan
may be suitable as a new drug for the management of PF.
In conclusion, the bleomycin-induced fibrosis model
investigated in the present study displayed fibrotic hyperplasia in
the lung tissue, as well as reduced MMP-9 and increased TIMP-1
expression. However, bosentan treatment appeared to have a
pneumoprotective effect by decreasing in the level of inflammation
and fibrous hyperplasia, increasing of MMP-9 expression and
reducing TIMP-1 expression. Therefore, bosentan may be used to
effectively inhibit PF.
Acknowledgements
The present study was funded by the Science and
Technology Project of Guangdong Province (grant no.
2013B021800045).
References
|
1
|
Selman M, Buendía-Roldán I and Pardo A:
Aging and pulmonary fibrosis. Rev Invest Clin. 68:75–83.
2016.PubMed/NCBI
|
|
2
|
Hutchinson J, Fogarty A, Hubbard R and
McKeever T: Global incidence and mortality of idiopathic pulmonary
fibrosis: A systematic review. Eur Respir J. 46:795–806. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Antoniou KM, Wuyts W, Wijsenbeek M and
Wells AU: Medical Therapy in Idiopathic Pulmonary Fibrosis. Semin
Respir Crit Care Med. 37:368–377. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lynch JP III, Huynh RH, Fishbein MC,
Saggar R, Belperio JA and Weigt SS: Idiopathic Pulmonary Fibrosis:
Epidemiology, Clinical Features, Prognosis, and Management. Semin
Respir Crit Care Med. 37:331–357. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vancheri C, Failla M, Crimi N and Raghu G:
Idiopathic pulmonary fibrosis: A disease with similarities and
links to cancer biology. Eur Respir J. 35:496–504. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Raghu G, Collard HR, Egan JJ, Martinez FJ,
Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, et
al: ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis: An
official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis:
evidence-based guidelines for diagnosis and management. Am J Respir
Crit Care Med. 183:788–824. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Turgut NH, Kara H, Elagoz S, Deveci K,
Gungor H and Arslanbas E: The Protective effect of naringin against
bleomycin-induced pulmonary fibrosis in Wistar rats. Pulm Med.
2016:76013932016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moore BB and Hogaboam CM: Murine models of
pulmonary fibrosis. Am J Physiol Lung Cell Mol Physiol.
294:L152–L160. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bonnans C, Chou J and Werb Z: Remodelling
the extracellular matrix in development and disease. Nat Rev Mol
Cell Biol. 15:786–801. 2014. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang Z, Jian X, Zhang W, Wang J and Zhou
Q: Using bosentan to treat paraquat poisoning-induced acute lung
injury in rats. PLoS One. 8:e759432013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Koo HS, Kim KC and Hong YM: Gene
expressions of nitric oxide synthase and matrix metalloproteinase-2
in monocrotaline-induced pulmonary hypertension in rats after
bosentan treatment. Korean Circ J. 41:83–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Giannelli G, Iannone F, Marinosci F,
Lapadula G and Antonaci S: The effect of bosentan on matrix
metalloproteinase-9 levels in patients with systemic
sclerosis-induced pulmonary hypertension. Curr Med Res Opin.
21:327–332. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang HD, Yamaya M, Okinaga S, Jia YX,
Kamanaka M, Takahashi H, Guo LY, Ohrui T and Sasaki H: Bilirubin
ameliorates bleomycin-induced pulmonary fibrosis in rats. Am J
Respir Crit Care Med. 165:406–411. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bancroft JD and Gamble M: Connective
tissue stainsTheory and practice of histological techniques. 6th.
Elsevier Health Sciences; Churchill Livingstone: pp. 1502008
|
|
15
|
Szapiel SV, Elson NA, Fulmer JD,
Hunninghake GW and Crystal RG: Bleomycin-induced interstitial
pulmonary disease in the nude, athymic mouse. Am Rev Respir Dis.
120:893–899. 1979.PubMed/NCBI
|
|
16
|
Sleijfer S: Bleomycin-induced pneumonitis.
Chest. 120:617–624. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhou XM, Zhang GC, Li JX and Hou J:
Inhibitory effects of Hu-qi-yin on the bleomycin-induced pulmonary
fibrosis in rats. J Ethnopharmacol. 111:255–264. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Araz O, Demirci E, Ucar E Yilmazel, Calik
M, Pulur D, Karaman A, Yayla M, Altun E, Halici Z and Akgun M:
Comparison of reducing effect on lung injury of dexamethasone and
bosentan in acute lung injury: An experimental study. Multidiscip
Respir Med. 8:74–81. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Watson WH, Ritzenthaler JD and Roman J:
Lung extracellular matrix and redox regulation. Redox Biol.
8:305–315. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Teixeira KC, Soares FS, Rocha LG, Silveira
PC, Silva LA, Valença SS, Dal Pizzol F, Streck EL and Pinho RA:
Attenuation of bleomycin-induced lung injury and oxidative stress
by N-acetylcysteine plus deferoxamine. Pulm Pharmacol Ther.
21:309–316. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Liang X, Tian Q, Wei Z, Liu F, Chen J,
Zhao Y, Qu P, Huang X, Zhou X, Liu N, et al: Effect of Feining on
bleomycin-induced pulmonary injuries in rats. J Ethnopharmacol.
134:971–976. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Arafa HM, AbdelWahab MH, ElShafeey MF,
Badary OA and Hamada FM: Anti-fibrotic effect of meloxicam in a
murine lung fibrosis model. Eur J Pharmacol. 564:181–189. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yoon JS, Chae MK, Jang SY, Lee SY and Lee
EJ: Antifibrotic effects of quercetin in primary orbital
fibroblasts and orbital fat tissue cultures of Graves' orbitopathy.
Invest Ophthalmol Vis Sci. 53:5921–5929. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
King TE Jr, Pardo A and Selman M:
Idiopathic pulmonary fibrosis. Lancet. 378:1949–1961. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pardo A, Cabrera S, Maldonado M and Selman
M: Role of matrix metalloproteinases in the pathogenesis of
idiopathic pulmonary fibrosis. Respir Res. 17:232016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pardo A and Selman M: Matrix
metalloproteases in aberrant fibrotic tissue remodeling. Proc Am
Thorac Soc. 3:383–388. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Selman M, Ruiz V, Cabrera S, Segura L,
Ramírez R, Barrios R and Pardo A: TIMP-1, −2, −3, and −4 in
idiopathic pulmonary fibrosis. A prevailing nondegradative lung
microenvironment? Am J Physiol Lung Cell Mol Physiol.
279:L562–L574. 2000.PubMed/NCBI
|
|
28
|
Ramos C, Montaño M, García-Alvarez J, Ruiz
V, Uhal BD, Selman M and Pardo A: Fibroblasts from idiopathic
pulmonary fibrosis and normal lungs differ in growth rate,
apoptosis, and tissue inhibitor of metalloproteinases expression.
Am J Respir Cell Mol Biol. 24:591–598. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zuo F, Kaminski N, Eugui E, Allard J,
Yakhini Z, BenDor A, Lollini L, Morris D, Kim Y, DeLustro B, et al:
Gene expression analysis reveals matrilysin as a key regulator of
pulmonary fibrosis in mice and humans. Proc Natl Acad Sci USA.
99:6292–6297. 2002. View Article : Google Scholar : PubMed/NCBI
|