Introduction
Hyperbilirubinemia is a common phenomenon and occurs
in ~60% of full-term newborns (1).
Although the majority of cases of neonatal hyperbilirubinemia are
physiological, excessive unconjugated bilirubin is a potential
neurotoxin and infants should be monitored, to identify those who
may develop severe hyperbilirubinemia, and in rare cases, acute
bilirubin encephalopathy or kernicterus (2,3).
To prevent the potential toxicity of bilirubin,
phototherapy has been suggested for the treatment of neonatal
hyperbilirubinemia. In addition, intravenous immunoglobulin (IVIG)
and albumin (IVALB) are administrated to neonates with hemolytic
hyperbilirubinemia (4,5). IVALB may be effective for preventing the
occurrence of complications associated with hyperbilirubinemia,
including neuronal developmental abnormalities and blood
transfusions (6–9). However, there have been a number of
previous studies indicating that neonatal hyperbilirubinemia and/or
phototherapy may be associated with infant immune disorders
including asthma, thrombocytopenia and arthritis (10–12), or
septic shock (13,14). Administration of IVALB serves a key
role in preventing neonatal encephalopathy or kernicterus by
binding to bilirubin and accelerating its supersession in plasma
(7). Conversely, albumin (ALB)
peptides may exhibit a cross-linking interaction with the neonatal
Fc receptor (FcRn) and promote IgG catabolism by saturating FcRn to
decrease sustained high serum IgG level (15).
To evaluate the occurrence of humoral immunity
injury associated with the administration of phototherapy or IVALB
in neonatal hyperbilirubinemia, a retrospective study was
conducted, and it was identified that phototherapy and IVALB were
risk factors in the decrease of globin (GLB) levels in neonatal
hyperbilirubinemia.
Patients and methods
Patients
The present study was conducted in the neonatal
intensive care unit (NICU) in Zhongnan Hospital of Wuhan University
(Wuhan, China) between January 2011 and December 2015. A total of
465 full-term infants were diagnosed with neonatal
hyperbilirubinemia, ages ranging from 1 to 28 days, and 430 cases
were enrolled in the study cohort according to modified criteria
based on the American Academy of Pediatrics Subcommittee on
Hyperbilirubinemia, for the management of hyperbilirubinemia in
newborn infants ≥37 weeks gestation age (1): i) Newborns had total serum bilirubin
≥100 µmol/l at first day of birth or ≥257 µmol/l at 2–28 days
following birth; ii) patients exhibited blood group incompatibility
(ABO), maternal Rhesus group negative hemolysis or G-6-PD
deficiency hemolytic anemia and polycythemia; iii) idiopathic
hyperbilirubinemia without cholestasis, and cranial hematoma; iv)
confirmed bacterial infection following birth with positive blood
culture and increased C-reactive protein. Cases of
hyperbilirubinemia lasting >1 week due to blood group
incompatibility or physiological delay were also included in this
study. A total of 25 cases were excluded as they exhibited
congenital abnormalities, including subtle dysmorphism of unknown
significance or a major anomaly of a single organ, inborn errors of
metabolism and congenital viral infections. The present study was
registered as a clinical study in the Chinese Clinical Trial
Registry (ChiCTR-ORC-16008872) and the Institutional Review Board
of Zhongnan Hospital of Wuhan University approved the study
(approval no. 2015019), and all guardians signed informed
consents.
Intervention protocol in
hyperbilirubinemia
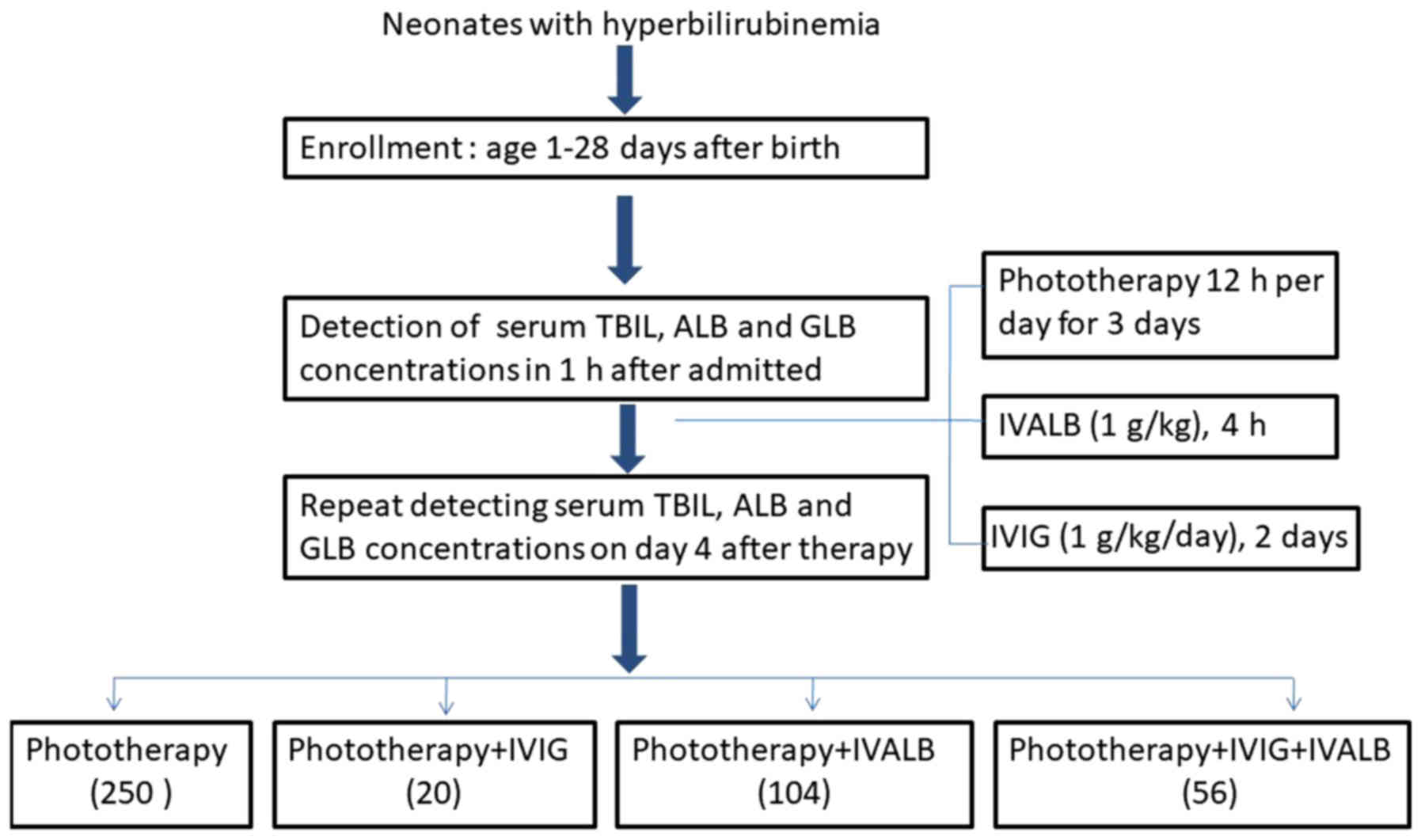
The intervention was conducted according to the time
of neonatal jaundice onset, the causes of hyperbilirubinemia and
the serum bilirubin levels. Neonates with hyperbilirubinemia were
divided into four groups: conventional intensive single-side
phototherapy (halogen lamps) alone (used in all jaundice neonates);
phototherapy combined with IVALB (used for unidentified
pathological hyperbilirubinemia with total serum bilirubin (TSB)
>300 µmol/l]: phototherapy combined with IVIG (used for
jaundiced patients with blood group incompatibility with TSB
<300 µmol/l); and phototherapy combined with IVIG+IVALB (for
blood group incompatibility with TSB >300 µmol/l). The
interference protocols were performed as follows: Phototherapy for
12 h/day, for 3 days; IVIG 1 g/kg/day for 2 days; and IVALB 1 g/kg
(Fig. 1). A total of 31 of 178
neonates with TSB >300 µmol/l did not receive IVALB or IVIG due
to refusal of blood products by parents.
Data were recorded from the clinical database of
infants admitted to the NICU. Clinical characteristics were
documented at the time of enrollment, including sex, age (in days
after birth), gestation age at delivery, delivery manner and birth
weight. Blood samples were collected, and concentrations of serum
GLB, ALB, TSB and direct serum bilirubin (DSB) were examined twice,
at the first day of hospitalization and the fourth day following
phototherapy with or without IVIG and/or IVALB treatment. In the
phototherapy-alone group, patients received an equal amount of a 5%
glucose intravenous infusion. The human IVIG (pH 4, 5%, 50 ml, 4°C)
and IVALB (20%, 50 ml, room temperature) products used in the
present study were provided by Wuhan Institute of Biological
Products Co., Ltd. (Wuhan, China). The IVIG treatment contained 95%
monomeric IgG and no aggregates when applied according to the
manufacturer's protocol.
Laboratory examination
The serum was separated from blood samples in the
dark and centrifuged (1,509 × g for 10 min at room temperature).
Serum TSB, DSB, ALB and GLB were measured in all hyperbilirubinemia
neonates at 1 h after admission and the fourth day after the
initiation of treatment using a Beckman AU5800 biochemistry
analyzer (Beckman Coulter, Inc., Brea, CA, USA).
Statistical analysis
Data are presented as mean ± standard deviation or
number (%). Pearson correlation analysis was performed between the
variances of infant age with ALB and GLB levels. Continuous
variables were compared between the groups using the two-tailed
Student's t-test and one-way analysis of variance with the
Student-Newman-Keuls method. Statistical analysis was performed
using GraphPad Prism 5 (GraphPad Software, Inc., La Jolla, CA,
USA). P<0.05 was considered to indicate a statistically
significant difference.
Results
Characteristics of neonatal
hyperbilirubinemia
A total number of 430 Chinese full-term newborns
were enrolled in the present study. Patient clinical
characteristics are summarized in Table
I. A total of 302 cases were admitted at 1–6 days after birth,
42 cases at 7–10 days, 43 cases at 11–15 days and 43 cases at 16–28
days. The primary cause of hyperbilirubinemia was idiopathic
(84.4%), followed by blood group incompatibility (11.6%) and
bacterial infection, identified as sepsis (2.6%). Median of TSB and
DSB levels prior to interference were 281.3 (100.7–536.1) µmol/l
and 20.6 (1.5–87.2) µmol/l, respectively.
 | Table I.Characteristics of neonatal
hyperbilirubinemia. |
Table I.
Characteristics of neonatal
hyperbilirubinemia.
| Characteristics | Median (range) or n
(%) |
|---|
| Sex |
|
| Male | 240 (55.8) |
|
Female | 190 (44.2) |
| Age at enrollment,
days | 4 (1–28) |
| Delivery |
|
| Natural
labor | 183 (42.6) |
|
Cesarean | 247 (57.4) |
| Gestational age,
weeks | 38 (37–42) |
| Body weight, g | 3,200
(900–4,800) |
| Serum TSB at
enrollment, µmol/l | 281.3
(100.7–536.1) |
| DSB at enrollment,
µmol/l | 20.6 (1.5–87.2) |
| Pathological cause of
hyperbilirubinemia |
|
|
Idiopathic | 363 (84.4) |
| Blood
group incompatibility | 50 (11.6) |
|
Infection | 11 (2.6) |
|
Polycythemia | 2 (0.5) |
|
Extravascular bleeding | 4 (1.0) |
| Therapy |
|
|
Phototherapy alone | 250 (58.1) |
|
Phototherapy+IVIG | 20 (4.7) |
|
Phototherapy+IVALB | 104 (24.2) |
|
Phototherapy+IVIG+IVALB | 56 (13) |
Associations between ALB, GLB and TSB
levels in neonatal hyperbilirubinemia
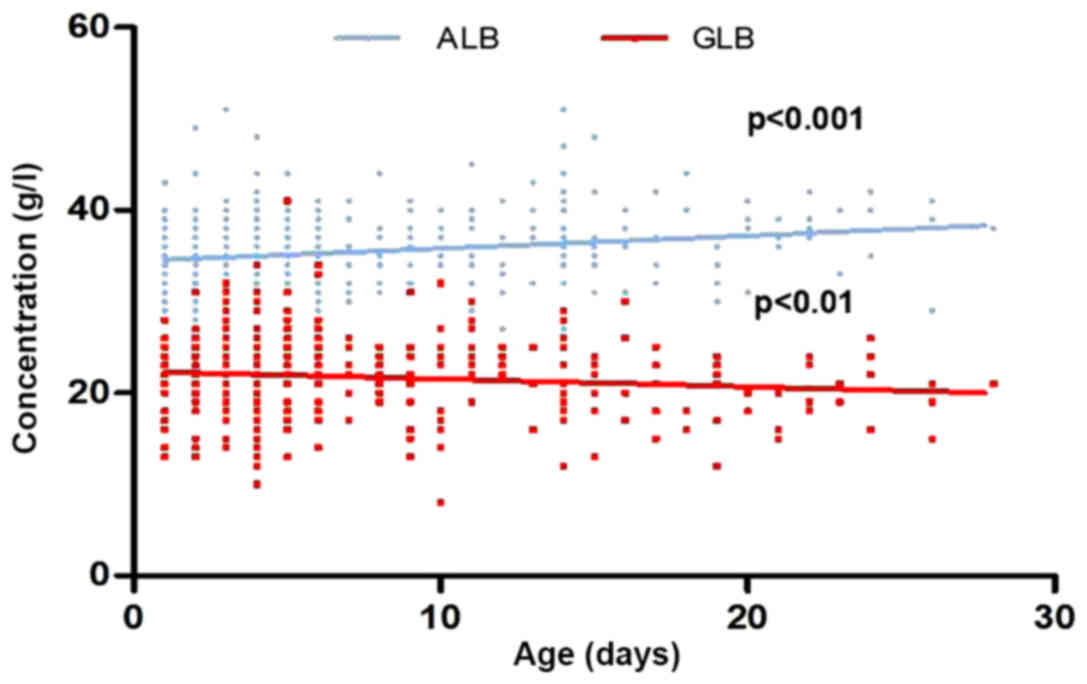
Prior to the intervention, the association between
neonatal hyperbilirubinemia baseline ALB, GLB and TSB levels was
evaluated. Pearson correlation analysis indicated no correlation
between ALB and TSB levels (r=0.072; P=0.134). Conversely, GLB and
TSB levels were significantly positively correlated (r=0.249;
P<0.01). The linear regression analyses indicated that the ALB
concentrations increased along with the age [95% confidence
interval (CI); 0.073, 0.205; P<0.001], and GLB concentration
gradually decreased with age from day 1 to day 28 after birth (95%
CI; −0.152, −0.0159; Fig. 2).
Following 3 days of treatment, TSB concentrations decreased from
299.6±83.9 to 163.6±57.6 µmol/l (P<0.001). These data imply that
neonatal hyperbilirubinemia incurs a decrease in GLB levels during
the perinatal period.
When compared with the effect of different methods
of intervention on serum ALB and GLB levels, as indicated in
Table IIA, there was no significant
difference of the serum ALB concentration in the phototherapy-alone
and phototherapy combined with IVIG treatment (P>0.05), and ALB
levels increased in groups who received additional IVALB. By
contrast, the GLB levels decreased significantly from 21.3±4.1 to
18.5±4.2 g/l in the phototherapy group (Table IIB), and 23.0±3.9 to 16.6±4.5 g/l in
the group of phototherapy combined with IVALB (P<0.001). There
was no significant difference in GLB levels in groups receiving
IVIG. All infants exhibited marked decreases in TSB concentration
compared with their baseline levels (Table IIC).
| Table II.ALB, GLB and TSB levels in each
treatment group. |
Table II.
ALB, GLB and TSB levels in each
treatment group.
| A, ALB concentrations
in different intervention groups |
|---|
|
|---|
| Intervention
group | N | ALB-0 (g/l) | ALB-1 (g/l) | P-value |
|---|
| Phototherapy
alone | 250 | 35.4±3.9 | 35.2±3.6 |
0.582 |
|
Phototherapy+IVIG | 20 | 34.3±4.3 | 32.4±5.3 |
0.586 |
|
Phototherapy+IVALB | 104 | 35.7±4.8 | 39.3±3.6 | <0.010 |
|
Phototherapy+IVIG+IVALB | 56 | 34.8±4.3 | 36.5±3.3 |
0.009 |
|
| B, GLB
concentrations in different intervention groups |
|
| Intervention
group | N | GLB-0
(g/l) | GLB-1
(g/l) | P-value |
|
| Phototherapy
alone | 250 | 21.3±4.1 | 18.5±4.2 | <0.010 |
|
Phototherapy+IVIG | 20 | 22.4±3.5 | 23.8±5.6 |
0.499 |
|
Phototherapy+IVALB | 104 | 23.0±3.9 | 16.6±4.5 | <0.010 |
|
Phototherapy+IVIG+IVALB | 56 | 22.9±4.7 | 22.6±4.3 |
0.451 |
|
| C, TSB
concentrations in different intervention groups |
|
| Intervention
group | N | TSB-0
(µmol/l) | TSB-1
(µmol/l) | P-value |
|
| Phototherapy
alone | 250 |
230.9±54.0a |
149.4±60.6b | – |
|
Phototherapy+IVIG | 20 |
222.3±57.8a |
144.1±27.3b | – |
|
Phototherapy+IVALB | 104 | 353.1±44.5 |
182.0±34.6b | – |
|
Phototherapy+IVIG+IVALB | 56 | 325.7±71.8 |
172.5±46.2b | – |
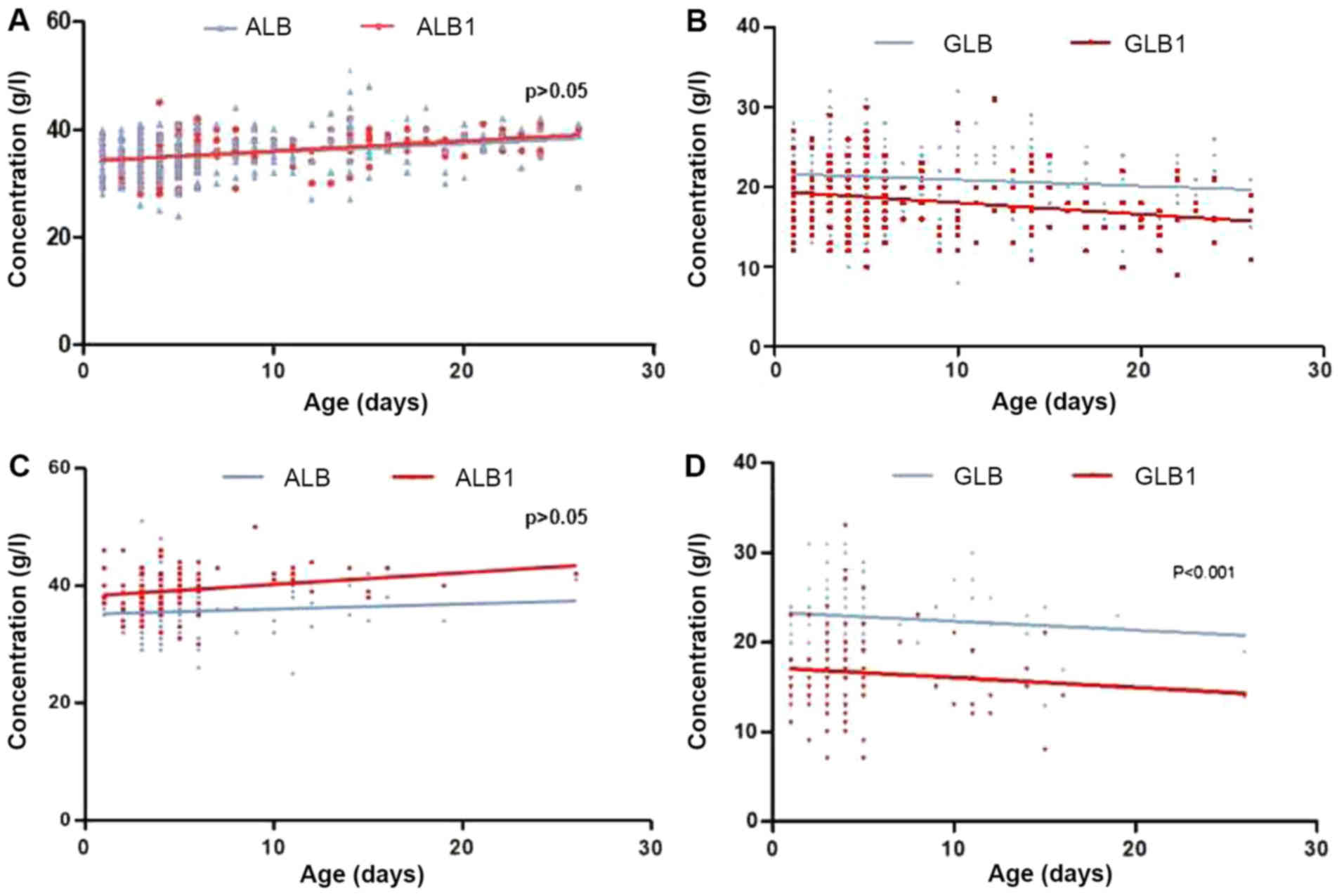
Phototherapy promotes the decrease in
GLB levels in neonatal hyperbilirubinemia
To exclude the effect of IVIG and ALB infusion on
serum GLB levels, the effect of phototherapy with and without IVALB
intervention on serum GLB concentration along with neonatal age was
evaluated. As demonstrated in Fig.
3A, 250 patients received phototherapy only, and the ALB levels
indicated no change following the intervention (P>0.05).
However, the GLB level decreased significantly (Fig. 3B) following the treatment, and the
degree of decrease in concentration increased with age
(P<0.001). Among these cases, 4 neonates admitted were
identified as having a bacterial infection, with severe sepsis on
the fifth day following phototherapy, requiring the administration
of antibiotics. The maximum decrease in GLB levels occurred in age
range of 16–28 days, which exhibited a 4.7 g/l decrease (22%) in
comparison with the first day of admission.
Fig. 3C describes the
104 infants who received phototherapy combined with IVALB at the
various birth ages. The ALB levels increased in correspondence with
increases in age, while there was no significant change compared
with their original levels (P>0.05). Conversely, the decrease in
GLB level was significantly decreased at each age (Fig. 3D; P<0.001). The maximum decrease in
GLB levels occurred between the ages of 16–28 days, which exhibited
a 4.5 g/l decrease compared with their baseline level. These
results indicate that phototherapy may be the primary mechanism for
the decreasing neonatal serum GLB levels, particularly in infants
aged >16 days old, while additional IVALB promoted the decrease,
along with increasing birth ages. As a result, the effect of
phototherapy on GLB levels was correlated with patient age; older
infants (16–28 days old) exhibited a greater decrease in GLB levels
compared with younger patients (<16 days old).
Discussion
The present study summarized the observation that
serum GLB levels decrease in response to intensive phototherapy,
with or without IVALB infusion in full-term neonates with
hyperbilirubinemia. In addition, age may be an important factor in
the decrease of GLB levels.
Phototherapy is popular for the treatment of
neonatal hyperbilirubinemia, and occasionally in combination with
IVIG and IVALB infusion for severe cases (6,9,16). IVIG and/or IVALB are effective for
neonates with hemolytic hyperbilirubinemia and for preventing
neurodevelopmental abnormalities or kernicterus. The present study
adopted phototherapy+IVALB treatment strategy for certain
hyperbilirubinemia cases as these infants exhibited higher serum
bilirubin levels compared with normal physiological ranges; these
increased levels may be attributed to hyperhemoglobinemia, which
causes prolonged hyperbilirubinemia and increases the risk of
bilirubin encephalopathy. Therefore, the IVALB was used as a
preventive treatment. In the present study, although there was
different baseline TSB levels between the phototherapy-alone and
phototherapy+IVALB groups, there was no difference in their
baseline ALB and GLB levels. Phototherapy was conducted for each
infant, and IVIG was added if neonates presented with hemolytic
hyperbilirubinemia at first day of birth, or IVALB was added for
neonates with serum TSB levels >300 µmol/l at the time of
admission, and the combination of IVIG+IVALB was administered in
patients with hemolytic hyperbilirubinemia with TSB >300 µmol/l.
Using this protocol, no infant mortalities were recorded, and no
patients developed kernicterus or required blood transfusion.
However, four neonates who had a negative blood culture at their
initial admission were identified as having bacterial infection
with severe sepsis (Escherichia coli) on the fifth day
following phototherapy alone (3 cases) or combined with IVALB (1
case), requiring the administration of antibiotics. No side effects
were observed in groups who received IVIG.
The GLB proteins are usually classified into four
groups, defined as α-1, −2, β and γ globulins. The optimal range
for GLB is 21–23 g/l in neonates, which includes 75% γ globulin
(17,18). α and β globulins are synthesized in
the liver cells and γ globulin is produced by B lymphocytes. Among
the serum GLB in neonates, 75% are IgG, and a small number of IgM,
IgA and IgD molecules, which are predominantly active against
bacteria, and are responsible for the opsonization of microbes and
facilitation of their uptake and elimination by phagocytic cells in
the immune system. In the present study, the baseline ALB/GLB ratio
was 1.7, and increased to 2.3 g in the phototherapy-only group,
which implies that phototherapy is the primary reason for decreases
in GLB, while IVALB additionally promoted the decrease.
Infants acquire maternal IgG in utero, and then
begin to gradually produce IgG autonomously up to normal levels by
1 year after birth; IgG concentrations decrease progressively until
the third month, and then increase again until the sixth month
(19,20). However, phototherapy intervention may
accelerate the clearance of IgG, which may confer a potential risk
of developing humoral immune disorders (11,12).
Although it cannot be confirmed that the cases of sepsis were
directly associated with the phototherapy, the risks of severe
infection appeared to be unavoidable when the ALB/ALB ratio was
disrupted (21). It has been
demonstrated that phototherapy may cause an increased incidences of
infection in neonates by increasing the total number of peripheral
white blood cells, which may complicate any existing infections
(22,23). Previous study has demonstrated that
phototherapy may have harmful effects on the immune system of
neonates with hyperbilirubinemia (14). The potential mechanisms of
immunological disturbances subsequent to phototherapy treatment
involve affecting the Th2/Th1 switch disorder, ultimately causing
allergic diseases during childhood and later in life, which may
affect the immune system and lead to autoimmunity disorders
(13,24). From these studies, it may be inferred
that phototherapy is not only associated with cellular immunity,
but that it also attenuates humoral immunity.
As demonstrated in the present study, the decrease
in neonate GLB levels was associated with phototherapy; the maximum
ratio decreased to 30% compared with baseline levels, particularly
in the group of neonates >16 days. The mechanism through which
phototherapy causes decreases in GLB remains unclear. Previous
studies have indicated that ALB may bind to the FcRn and alter the
serum half-life of GLB, while ALB may block the FcRn-IgG
interaction and increase IgG catabolism, as FcRn is responsible for
protecting IgG from degradation by trafficking IgG (15,25).
Neonates who received IVIG demonstrated an optimal concentration of
GLB following treatment (26).
However, this does not mean that the use of IVIG during
phototherapy should be encouraged; conversely, doctors must
carefully consider the use of phototherapy in those patients with
hyperbilirubinemia that are not high risk, and ensure that
sufficient access to breast feeding is available during
phototherapy (27–30).
There are certain limitations in the present study:
The IgG levels were not measured, and there was no long-term
follow-up strategy to define the subsequent immune status of the
children who underwent phototherapy during the neonatal period. The
final conclusions of the effects of phototherapy on the levels of
serum GLB later in childhood are not available at present, but will
be observed in future.
Taken together, the results of the present study
demonstrated that phototherapy accelerates serum GLB depletion,
which implies infants receiving phototherapy have an increased risk
of immunosuppression, particularly in newborns aged >16 days.
Additional IVALB treatment promoted this decrease, along with
increased age.
Acknowledgements
The present study was published as an abstract at
the 26th Annual Conference of the Asian Pacific Association for the
Study of the Liver conference proceedings.
Funding
The present study was supported by the National
Natural Scientific Fund of China, awarded to Dr Zhao (grant nos.
81170005 and 81670007).
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JZ performed the initial analysis and drafted the
initial manuscript. CW and MZ performed the statistical analysis.
DZ contributed to the conception of the study, interpreted the data
analysis and finalized the manuscript as submitted. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was registered as a clinical study
in the Chinese Clinical Trial Registry (ChiCTR-ORC-16008872), and
the Institutional Review Board of Zhongnan Hospital of Wuhan
University approved the study (approval no. 2015019). All guardians
provided informed consent.
Patient consent for publication
All guardians provided informed consent on behalf of
infants for the publication of associated data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
American Academy of Pediatrics
Subcommittee on Hyperbilirubinemia: Management of
hyperbilirubinemia in the newborn infant 35 or more weeks of
gestation. Pediatrics. 114:297–316. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rennie J, Burman-Roy S and Murphy MS:
Guideline Development Group: Neonatal jaundice: summary of NICE
guidance. BMJ. 340:c24092010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gamaleldin R, Iskander I, Seoud I, Aboraya
H, Aravkin A, Sampson PD and Wennberg RP: Risk factors for
neurotoxicity in newborns with severe neonatal hyperbilirubinemia.
Pediatrics. 128:e925–e931. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hosono S, Ohno T, Kimoto H, Nagoshi R,
Shimizu M and Nozawa M: Effects of albumin infusion therapy on
total and unbound bilirubin values in term infants with intensive
phototherapy. Pediatr Int. 43:8–11. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Huizing K, Røislien J and Hansen T:
Intravenous immune globulin reduces the need for exchange
transfusions in Rhesus and AB0 incompatibility. Acta Paediatr.
97:1362–1365. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hosono S, Ohno T, Kimoto H, Nagoshi R,
Shimizu M, Nozawa M and Harada K: Follow-up study of auditory
brainstem responses in infants with high unbound bilirubin levels
treated with albumin infusion therapy. Pediatr Int. 44:488–492.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ahlfors CE and Wennberg RP:
Bilirubin-albumin binding and neonatal jaundice. Semin Perinatol.
28:334–339. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yokota T, Morioka I, Kodera T, Morisawa T,
Sato I, Kawano S, Koda T, Matsuo K, Fujioka K, Morikawa S, et al:
Novel treatment strategy for Japanese newborns with high serum
unbound bilirubin. Pediatr Int. 55:54–59. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Xiong T, Chen H and Mu D: Effect of
pre-exchange albumin infusion on neonatal hyperbilirubinaemia and
long-term developmental outcomes. Cochrane Database of Systematic
Reviews. (2): Art. no. CD011001. 2014.
|
|
10
|
Khera S and Gupta R: Incidence of
thrombocytopenia following phototherapy in hyperbilirubinemic
neonates. Med J Armed Forces India. 67:329–332. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Huang L, Bao Y, Xu Z, Lei X, Chen Y, Zhang
Y and Zhang J: Neonatal bilirubin levels and childhood asthma in
the US Collaborative Perinatal Project, 1959–1965. Am J Epidemiol.
178:1691–1697. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sun HL, Lue KH and Ku MS: Neonatal
jaundice is a risk factor for childhood allergic rhinitis: A
retrospective cohort study. Am J Rhinol Allergy. 27:192–196. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Abourazzak S, Bouharrou A and Hida M:
Jaundice and urinary tract infection in neonates: Simple
coincidence or real consequence? Arch Pediatr. 20:974–978. 2013.(In
French). View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chang HY, Cheng KS, Liu YP, Hung HF and Fu
HW: Neonatal infected subgaleal hematoma: an unusual complication
of early-onset E. coli sepsis. Pediatr Neonatol. 56:126–128.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Andersen JT, Dalhus B, Cameron J, Daba MB,
Plumridge A, Evans L, Brennan SO, Gunnarsen KS, Bjørås M, Sleep D,
et al: Structure-based mutagenesis reveals the albumin-binding site
of the neonatal Fc receptor. Nat Commun. 3:610. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Maisels MJ and McDonagh AF: Phototherapy
for neonatal jaundice. N Engl J Med. 358:920–928. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hyvarinen M, Zeltzer P, Oh W and Stiehm
ER: Influence of gestational age on serum levels of alpha-1
fetoprotein, IgG globulin, and albumin in newborn infants. J
Pediatr. 82:430–437. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Salimonu LS, Ladipo OA, Adeniran SO and
Osukoya BO: Serum immunoglobulin levels in normal, premature and
postmature newborns and their mothers. Int J Gynaecol Obstet.
16:119–123. 1978–1979. View Article : Google Scholar
|
|
19
|
Ballow M, Cates KL, Rowe JC, Goetz C and
Desbonnet C: Development of the immune system in very low birth
weight (less than 1500 g) premature infants: Concentrations of
plasma immunoglobulins and patterns of infections. Pediatr Res.
20:899–904. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Drossou V, Kanakoudi F, Diamanti E,
Tzimouli V, Konstantinidis T, Germenis A, Kremenopoulos G and
Katsougiannopoulos V: Concentrations of main serum opsonins in
early infancy. Arch Dis Child Fetal Neonatal Ed. 72:F172–F175.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Keller MA and Stiehm ER: Passive immunity
in prevention and treatment of infectious diseases. Clin Microbiol
Rev. 13:602–614. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jafarzadeh M: mohammadzadeh A. Should
urine culture be considered in the hyperbilirubinemia workup of a
neonate. JCCM. 4:136–138. 2009.
|
|
23
|
Shahian M, Rashtian P and Kalani M:
Unexplained neonatal jaundice as an early diagnostic sign of
urinary tract infection. Int J Infect Dis. 16:e487–e490. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Apaydin K, Ermis B, Arasli M, Tekin I and
Ankarali H: Cytokines in human milk and late-onset breast milk
jaundice. Pediatr Int. 54:801–805. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Eyada IK, El Saie AL, Ibrahem GA and Riad
NM: Effect of phototherapy on B and T lymphocytes in Egyptian
infants suffering from neonatal jaundice. Allergol Immunopathol
(Madr). 45:290–296. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu P, Li L, Fan P, Zheng J and Zhao D:
High-dose of intravenous immunoglobulin modulates immune tolerance
in premature infants. BMC Pediatr. 18:742018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chang RJ, Chou HC, Chang YH, Chen MH, Chen
CY, Hsieh WS and Tsao PN: Weight loss percentage prediction of
subsequent neonatal hyperbilirubinemia in exclusively breastfed
neonates. Pediatr Neonatol. 53:41–44. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
El Sakka A, Imam SS, El Barbary M and
Ibrahium W: Does Type of Infant Feeding Affect Phototherapy for
Neonatal Hyperbilirubinemia? SAGE J. 4:334–339. 2012.
|
|
29
|
Cuperus FJ, Schreuder AB, van Imhoff DE,
Vitek L, Vanikova J, Konickova R, Ahlfors CE, Hulzebos CV and
Verkade HJ: Beyond plasma bilirubin: The effects of phototherapy
and albumin on brain bilirubin levels in Gunn rats. J Hepatol.
58:134–140. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cohen RS, Wong RJ and Stevenson DK:
Understanding neonatal jaundice: A perspective on causation.
Pediatr Neonatol. 51:143–148. 2010. View Article : Google Scholar : PubMed/NCBI
|