Introduction
In the framework of cataract surgery, a comfortable
postoperative uncorrected distance visual acuity (UDVA) may be
successfully achieved due to the development of modern biometric
methods and calculation formulas. However, patients also require to
be able to see a normal reading text without further correction,
which has led to the development of multifocal or accommodation
intraocular lenses (IOLs). The challenge of these models is the
number of contraindications, risk of asthenopic problems caused by
higher-order aberrations, as well as the additional required
payment by the patient.
For pseudophakic eyes, in addition to the optimal
UDVA, the optimal uncorrected near visual acuity (UNVA) may also be
seen, although a monofocal IOL has been implanted. In a previous
study (1) it was proven that optimal
near visual acuity may be achieved even without targeted
postoperative myopisation in eyes with a short axial length (AL).
For 30.33% of eyes with a UNVA of ≥0.6, the AL was ≤23.5 mm,
whereas even for a UNVA of 0.8, the AL was up to 22.5 mm.
Theoretically, a significant role of the postoperative
pseudo-accommodation amplitude in such eyes may be expected,
particularly the effect of an axial shift of the IOL causing a
reduction of the anterior chamber depth (ACD), which occurs even
when the direction of view of the eye is changed. It was proven
that a change in the position of the eye affects the ACD, albeit to
a lesser extent than predicted (2).
The hydrodynamic status in the eye is practically indefinable with
regard to several influencing factors. However, the validity of
Pascal's law is hypothesised, and due to the hydrostatic pressure
under the influence of a small gravitational force, the shift of
the IOL causes a slight myopisation that likely confers an increase
in near visual acuity.
The subject of the present study was a statistical
evaluation of a change in the UNVA depending on the position of the
text or a change of the direction of the eye, including an analysis
of a mutual correlation of the individual eye parameters.
Materials and methods
Study parameters
In total, 121 eyes were evaluated following surgery
in 65 patients. Patients who underwent cataract surgery with
implantation of a monofocal IOL were included in the study. The
patient selection was performed randomly, depending on the time the
patients came for the check-up examinations between January and
March 2017. The surgery was performed by a single surgeon using an
identical technique (phacoemulsification using the initial incision
of 2.2 mm), and the relation SRK/T was used to calculate the
optical power of the IOL for emmetropy; the evaluation period was
at least 1 month post-surgery. The following models of IOL were
implanted: MA50BM (58.68% of eyes), SA60AT (23.14%), SN60WF
(13.22%) and SN6ATx (4.96%). Only the postoperatively emmetropic
eyes among the eyes examined were included, with 97.52% of the eyes
achieving a vision of 1.0 or better (the remaining 2.48% of the
eyes achieved a vision of 0.8, whereas no correction improved the
vision). Input data for the study are summarised in Table I.
 | Table IInput values and parameters of the
study. |
Table I
Input values and parameters of the
study.
| A, AL <22.5
mm |
|---|
| Eye no. | AL (mm) | IOL | UDVA | ACD (mm) | KC
(D) | KVA
(D) | UNVAH | UNVAV |
|---|
| 1 | 21.16 | 27.5 SA | 0.80 | 3.90 | 44.68 | 44.95 | 0.40 | 0.50 |
| 2 | 21.28 | 26.5 SA | 1.00 | 3.90 | 43.77 | 42.65 | 0.80 | 0.80 |
| 3 | 21.28 | 27.0 SA | 1.00 | 4.00 | 46.05 | 45.33 | 0.50 | 0.60 |
| 4 | 21.43 | 23.0 SA | 1.20 | 4.10 | 46.50 | 46.71 | 0.60 | 0.60 |
| 5 | 21.46 | 30.5 SA | 1.00 | 3.40 | 42.15 | 41.68 | 0.80 | 0.80 |
| 6 | 21.47 | 23.0 SA | 1.20 | 4.10 | 46.50 | 46.74 | 0.60 | 0.60 |
| 7 | 21.54 | 25.5 SA | 1.20 | 3.80 | 44.86 | 45.46 | 1.00 | 1.00 |
| 8 | 21.64 | 24.5 SA | 1.20 | 3.80 | 46.10 | 45.77 | 0.80 | 0.80 |
| 9 | 21.68 | 24.0 SA | 1.20 | 3.80 | 46.10 | 45.84 | 0.80 | 0.80 |
| 10 | 21.75 | 26.0 SA | 1.00 | 3.80 | 43.12 | 44.14 | 0.40 | 0.60 |
| 11 | 21.75 | 25.5 SA | 1.00 | 3.80 | 42.00 | 43.00 | 0.40 | 0.60 |
| 12 | 21.80 | 24.5 SA | 1.00 | 4.19 | 45.57 | 45.45 | 0.80 | 0.80 |
| 13 | 21.80 | 25.0 SA | 1.00 | 4.19 | 44.67 | 45.06 | 0.80 | 0.80 |
| 14 | 21.80 | 27.0 SA | 1.20 | 3.80 | 47.16 | 45.55 | 1.00 | 1.00 |
| 15 | 21.87 | 24.0 SA | 1.20 | 3.50 | 45.20 | 45.67 | 0.50 | 0.50 |
| 16 | 21.87 | 24.5 SA | 1.00 | 3.70 | 44.78 | 44.45 | 0.50 | 0.60 |
| 17 | 21.94 | 24.5 MA | 1.00 | 3.30 | 45.91 | 44.76 | 0.30 | 0.40 |
| 18 | 21.95 | 24.0 SA | 1.50 | 3.80 | 45.81 | 45.19 | 0.20 | 0.30 |
| 19 | 21.95 | 24.5 SA | 1.00 | 3.50 | 45.00 | 44.81 | 0.40 | 0.40 |
| 20 | 21.96 | 24.0 SA | 1.20 | 3.50 | 45.58 | 45.54 | 0.50 | 0.50 |
| 21 | 21.96 | 23.5 SA | 1.50 | 3.90 | 45.64 | 45.93 | 0.20 | 0.30 |
| 22 | 21.99 | 25.0 SA | 1.00 | 3.50 | 45.07 | 44.36 | 0.40 | 0.40 |
| 23 | 21.99 | 24.5 MA | 1.00 | 3.50 | 45.70 | 44.47 | 0.30 | 0.40 |
| 24 | 22.12 | 26.5 SA | 1.00 | 4.00 | 46.06 | 45.54 | 0.50 | 0.60 |
| 25 | 22.13 | 24.5 SA | 1.00 | 3.50 | 44.84 | 44.53 | 0.50 | 0.60 |
| 26 | 22.14 | 22.0 SA | 1.20 | 3.60 | 46.35 | 45.79 | 0.40 | 0.40 |
| 27 | 22.16 | 24.0 IQ | 1.00 | 2.00 | 45.64 | 45.66 | 0.60 | 0.60 |
| 28 | 22.20 | 22.5 SA | 1.20 | 3.80 | 45.93 | 46.25 | 0.50 | 0.60 |
| 29 | 22.22 | 25.0 IQ | 1.20 | 4.20 | 44.00 | 44.01 | 0.30 | 0.30 |
| 30 | 22.28 | 22.0 SA | 1.20 | 3.80 | 46.26 | 46.48 | 0.50 | 0.60 |
| 31 | 22.32 | 23.5 IQ | 1.00 | 2.00 | 45.61 | 44.80 | 0.50 | 0.60 |
| 32 | 22.35 | 22.0 SA | 1.00 | 3.60 | 45.94 | 46.52 | 0.60 | 0.60 |
| 33 | 22.38 | 24.5 SA | 1.00 | 3.70 | 43.94 | 43.30 | 0.50 | 0.50 |
| 34 | 22.40 | 22.0 SA | 1.00 | 3.70 | 45.28 | 45.11 | 0.60 | 0.60 |
| 35 | 22.42 | 24.5 IQ | 1.20 | 3.60 | 44.27 | 44.38 | 0.30 | 0.30 |
| 36 | 22.46 | 24.0 SA | 1.00 | 3.70 | 42.72 | 42.65 | 0.50 | 0.50 |
| 37 | 22.47 | 23.0 SA | 1.20 | 4.20 | 44.45 | 44.80 | 0.30 | 0.40 |
The evaluated postoperative parameters included the
typography values (Anterior Segment Analyser Orbscan II) for
optical power in the central part of the cornea (KC), as well as in
the visual axis (KVA), anterior chamber depth (ACD; OcuScan
biometer) and eye axial length (AL; OcuScan biometer).
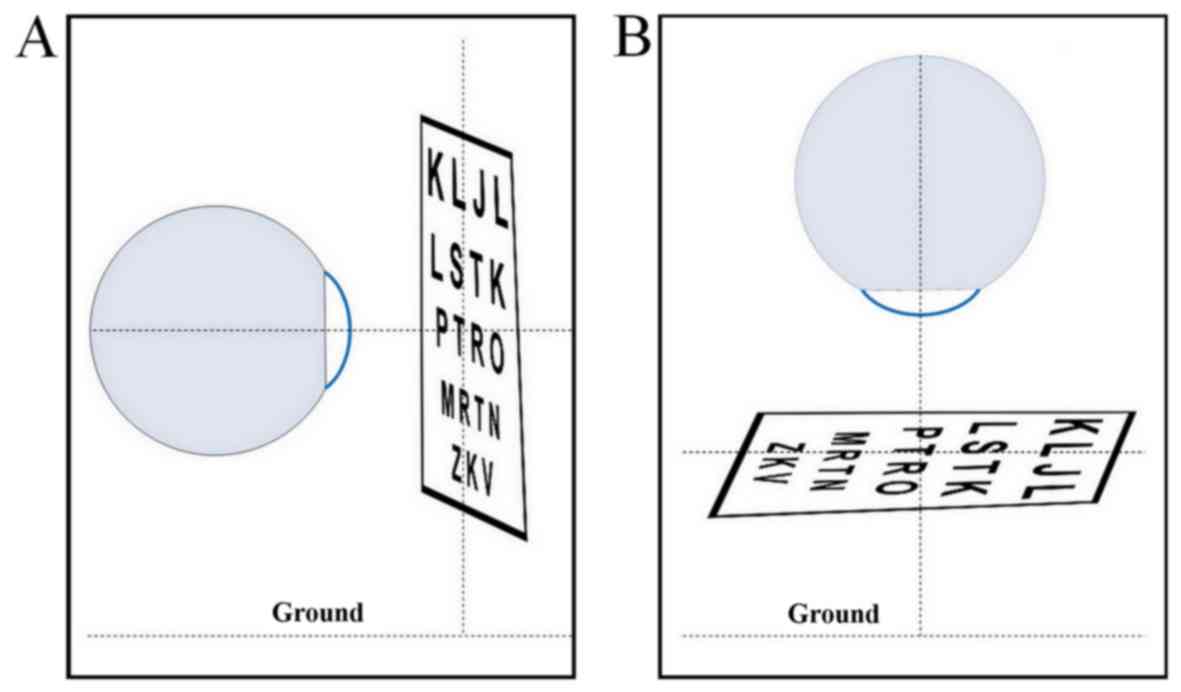
To determine the near vision values, each eye was
examined separately using the Jäeger table ZEISS at a distance of
40 cm and its perpendicular position relative to the eye viewing
axis. First, the value of the least read text was recorded at the
horizontal position of the eye (UNVAH, viewing axis of
the eye parallel with the floor) and subsequently at the vertical
position (UNVAV, viewing axis of the eye perpendicular
to the floor). Demonstration of the position of the mutual axes is
shown on Fig. 1. The observed
parameters were evaluated for the whole group of patients, but also
following categorisation of the group into three cohorts according
to the AL: The group of short eyes (AL<22.5) included
eyes up to 22.5 mm, AL 22.5-23.5 mm was identified as the group of
normal eyes (AL22.5-23.5) and the cohort of long eyes
had an AL >23.5 mm (AL>23.5).
Results
Mean parameters of the input group
following categorization
The mean age of the group was 71 years. The mean
parameter values of the eyes included in the study are presented in
Table II.
| Table IIMean parameters of the input group
following categorization into the groups. |
Table II
Mean parameters of the input group
following categorization into the groups.
| Values based on the
AL groups |
|---|
| Parameters | Values of the whole
group | <22.5 | ≤22.5-23.5≥ | >23.5 |
|---|
| Count (eyes) | 121 | 37 | 52 | 32 |
| AL (mm) | 22.96±0.85 | 21.93±0.36 | 23.09±0.31 | 23.96±0.43 |
| ACD (mm) | 3.83±0.37 | 3.68±0.47 | 3.84±0.35 | 3.68±0.47 |
| KC
(D) | 44.19±1.73 | 45.11±1.21 | 44.04±1.65 | 43.36±1.91 |
| KVA
(D) | 44.21±1.58 | 44.96±1.17 | 44.10±1.55 | 43.53±1.73 |
Mean values of UNVAH and
UNVAV
The paired t-test was used to compare visual acuity
at the horizontal and vertical position of the eye for the whole
group of patients. The results revealed that, in the case of
UNVAH for the horizontal position of the eye, the values
were lower compared with UNVAV for the vertical position
of the eye (mean 0.51 vs. 0.56, respectively; P<0.001). A higher
or identical UNVAV value compared with UNVAH
was always achieved in all groups based on the AL. Visual
improvement in UNVAV was observed in 40.2% of the eyes.
The lowest mean value for the UNVAH was recorded in eyes
with an AL >23.5 mm. The highest mean value for the
UNVAV was achieved in short eyes (mean 0.58;
P<0.001). The complete values are summarised in Table III.
| Table IIIMean values of UNVAH and
UNVAV. |
Table III
Mean values of UNVAH and
UNVAV.
| Category | Mean (mm) | SD | t | P-value |
|---|
| All AL |
|
UNVAH | 0.51 | 0.15 | -8.18 | <0.001 |
|
UNVAV | 0.56 | 0.15 | | |
|
AL<22.5 |
|
UNVAH | 0.53 | 0.20 | -4.62 | <0.001 |
|
UNVAV | 0.58 | 0.18 | | |
|
AL22.5-23.5 |
|
UNVAH | 0.52 | 0.12 | -5.25 | <0.001 |
|
UNVAV | 0.56 | 0.12 | | |
|
AL>23.5 |
|
UNVAH | 0.47 | 0.13 | -4.19 | <0.001 |
|
UNVAV | 0.52 | 0.16 | | |
Correlation coefficients
Evaluation of the association of the eye parameters
for UNVAH and UNVAH was performed using
correlation coefficients (Table IV).
We did not identify a more significant than weak correlation value
for the whole group. For the AL<22.5 group, we
observed a weak negative correlation of the UNVAH with
AL (-0.39), but a moderate negative correlation was observed for AL
and UNVAV (-0.45). In the AL22.5-23.5 group
of eyes, the positive correlation of the UNVAH with
KC (0.45) and KVA (0.34), and of
UNVAV with KC (0.42) and KVA
(0.33), was found to be more significant. For eyes with an AL
>23.5 mm there was only a weak negative correlation of
UNVAV with ACD (-0.28).
| Table IVCorrelation coefficients for the
whole group and different ALs. |
Table IV
Correlation coefficients for the
whole group and different ALs.
| | Variables |
|---|
| AL (mm) | ACD | KC | KVA | AL |
|---|
| Whole group |
|
UNVAH | -0.06 | 0.24 | 0.18 | -0.21 |
|
UNVAV | -0.04 | 0.22 | 0.17 | -0.22 |
| <22.5 |
|
UNVAH | 0.06 | 0.11 | 0.06 | -0.39 |
|
UNVAV | 0.07 | 0.06 | 0.04 | -0.45 |
| 22.5-23.5 |
|
UNVAH | -0.09 | 0.45 | 0.34 | -0.21 |
|
UNVAV | 0.01 | 0.42 | 0.33 | -0.29 |
| >23.5 |
|
UNVAH | -0.11 | 0.03 | -0.01 | 0.12 |
|
UNVAV | -0.28 | 0.07 | 0.02 | 0.05 |
Discussion
During the postoperative evaluation of patients with
implanted monofocal IOL following standard cataract surgery, an
unexpectedly high postoperative near visual acuity was observed. To
predict this effect, scientific studies have gradually attempted to
identify a correlation between eye parameters and this phenomenon.
The pupil size and AL were not conclusively found to be correlated
with near vision in 84 patients. However, a pupil diameter <2.6
mm along with AL <23 mm demonstrated better near visual acuity
(3). Our previous study partially
supports these conclusions, as our data revealed a moderate
negative correlation of the postoperative UNVA with a decreasing AL
(<22.5 mm) (1).
Association of age with UNVA was not proven in the
present study, whereas Hayashi et al (4) confirmed that patient age is a negative
factor affecting the postoperative amplitude of
pseudo-accommodation (correlation coefficient of -0.49); however,
that study also included patients aged <40 years, while only 3
patients were <60 years of age in the present study. A relevant
assessment of the dependence on age would require a higher age
range. According to Nanavatyet al (5), corneal astigmatism (against the rule) is
a significant factor that increases the possibility of
pseudo-accommodation up to 10-fold.
A more statistically significant dependence on
preoperative ACD, KC or KVA for the whole
group of patients was not observed. When comparing different
positions of the read text and the position of the eyes, there was
a probability of increasing the value of the near vision for the
vertical position (UNVAV). The mean values show an
increase of near visual acuity in all patients, particularly those
with an AL <22.5 mm. It is believed that, in short eyes with an
implanted IOL of higher optical power, the same value of its
displacement towards the cornea will cause a higher myopia compared
with an IOL that of lower optical power.
Acknowledgements
The authors would like to thank the entire staff of
the Eye Clinic JL FBMI CTU in Prague for their cooperation in this
study.
Funding
No funding was received.
Availability of data and materials
The input data for the study are summarised in
Table I and do not include any direct
or indirect identifiers. The datasets generated and analysed in the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
MZ conceived, designed and performed the data
analysis of this study. MF and JL coordinated preoperative and
postoperative examinations of the eyes and made general revisions.
SP performed cataract surgery in all the patients and made general
revisions of study. All the authors have read and approved the
final version of this manuscript for publication.
Ethics approval and consent to
participate
All patients included in the present study provided
written informed to participate, and the study protocol conformed
to the principles outlined in the Declaration of Helsinki under
approval from the ethic committee of JL Clinic FBME CTU in
Prague.
Patient consent to publication
All patients consented to disclose their
postoperative condition, visual acuity and eye parameters to be
published in the present study.
Competing interests
The authors state that there are no conflicts of
interest regarding the publication of this article.
References
|
1
|
Lešták J, Pitrová Š, Fůs M and Žáková M:
The Uncorrected Near Visual Acuity after the Monofocal Intraocular
Lens Implantation. Cesk Slov Oftalmol. 73:127–133. 2017.(In Czech).
PubMed/NCBI
|
|
2
|
Lister LJ, Suheimat M, Verkicharla PK,
Mallen EA and Atchison DA: Influence of Gravity on Ocular Lens
Position. Invest Ophthalmol Vis Sci. 57:1885–1891. 2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lim DH, Han JC, Kim MH, Chung ES and Chung
TY: Factors affecting near vision after monofocal intraocular lens
implantation. J Refract Surg. 29:200–204. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Hayashi K, Hayashi H, Nakao F and Hayashi
F: Aging changes in apparent accommodation in eyes with a monofocal
intraocular lens. Am J Ophthalmol. 135:432–436. 2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nanavaty MA, Vasavada AR, Patel AS, Raj SM
and Desai TH: Analysis of patients with good uncorrected distance
and near vision after monofocal intraocular lens implantation. J
Cataract Refract Surg. 32:1091–1097. 2006.PubMed/NCBI View Article : Google Scholar
|