Introduction
Urolithiasis is one of the most prevalent urological
diseases in the nineteenth century population in Europe is quite
similar to that of the twentieth century in Asia (1). The incidence of urolithiasis in Japan
has steadily increased between 1965 and 2005(2). Urolithiasis has been reported to
increase the number of patients of various dietary habits. It has
been reported that 12% of people globally suffer from urolithiasis
(3). The increase in urolithiasis
prevalence is thought to associated with changes in dietary habits,
but may be particularly associated with a higher intake of animal
protein (4,5).
Urolithiasis is a metabolic syndrome that presents
symptoms including hypertension, lipid metabolism disorders,
diabetes, obesity, atherosclerosis, ischemic heart disease and
other associated problems that have a common pathology of visceral
fat accumulation and insulin resistance (6-10).
This common pathology means urolithiasis is considered to be a
lifestyle disease. Various studies have reported cases of
urolithiasis associated with hyperlipidemia, obesity, fatty liver,
hyperuricemia, diabetes, hypertension and aortic calcification
(9,10).
Although urolithiasis is considered to be strongly
associated with lifestyle habits, there are numerous cases in which
urolithiasis develops despite a non-obese body type or healthy
lifestyle habits (6-10).
However, in clinical practice, diet therapy and lifestyle changes
instructed for the prevention of recurrence of urolithiasis are
almost identical in numerous different cases.
Therefore, the present study examined the effect of
body mass index (BMI) on urolithiasis and its surrounding
environment in patients, by analyzing the number of normal- and
high-BMI (healthy and overweight) patients with urolithiasis. Based
on their BMI, patients with urolithiasis were categorized into a
standard-type patient group and an obese-type patient group, and
differences in clinical factors were assessed.
Materials and methods
The present study analyzed a total of 63 patients
with urolithiasis for whom height and weight were measured at our
hospital (Tokyo Medical University Ibaraki Medical Center, Ibaraki,
Japan) between July 2013 and June 2015. The mean age of the
patients was 55.6 years (range, 59-78 years). Of the total 63
patients, 49 were male and 14 were female (Table I). Written informed consent was
obtained from all patients and all procedures used in the present
study were ethically approved by the Ethical Committee of our
hospital (Tokyo Medical University Ibaraki Medical Center). For
each patient, BMI was calculated initially. According to World
Health Organization guidelines, BMI <25 is of healthy body types
and BMI ≥25 represents overweight body types (11). Thus, patients were then grouped by
BMI-defined body type using a threshold value of 25 accordingly
(11).
 | Table IClinical features of the 63 patients
with urolithiasis. |
Table I
Clinical features of the 63 patients
with urolithiasis.
| Characteristics | Value |
|---|
| Age, mean
(range) | 55.6 years (range,
59-78 years) |
| Sex, n | Male 49, female
14 |
| Body Mass Index, mean
(range) | 24.4 (17.6-41.0) |
| Size of urolithiasis,
mean (range) | 9.5 mm (4-35) |
| Number of
urolithiasis, n | Single 36, double 5,
more than triple 22 |
| Value of uric acid,
mean (range) | 5.86 mg/dl
(2.3-10.1) |
| Value of urine pH,
mean (range) | 6.63 (5.5-7.5) |
| Value of liver
computed tomography, mean (range) | 56.2 Hounsfield Unit
(30-70) |
The measurement of the computed tomography (CT)
value was determined using the Hounsfield Unit (HU). The liver CT
value was defined as the mean value of three CT values selected
randomly. Two CT model types, the Brilliance iCT SP 64-Slice
configuration (Philips Healthcare, Amsterdam, The Netherlands) and
the SOMATOM Sensation 64-Slice configuration (Siemens AG, Munich,
Germany) were used.
Statistical analysis
All statistical analyses were performed using Stat
View (ver. 5.0; SAS Institute, Inc., Cary, NC, USA). Continuous
variables were presented as the mean ± standard deviation. A
χ2 test was used to evaluate comparisons between the
differences in sex between the BMI≥25 and BMI<25 groups
(Table II). A Student's t-test was
used to evaluate the comparisons between the clinical features,
including BMI, calculus size, serum uric acid value, urinary pH
value and liver CT value (Fig. 1).
The correlations amongst the liver CT value, calculus size and BMI
were determined using a Spearman's rank correlation test (Fig. 2). P<0.05 was considered to indicate
a statistically significant difference. The difference between the
mean values of the two groups was analyzed using a Student's
t-test, and the difference between the two variables was analyzed
using a χ2 test. Regression analysis was used to
identify correlations between variables.
| Table IIComparison of BMI between male and
female patients with urolithiasis. |
Table II
Comparison of BMI between male and
female patients with urolithiasis.
| Gender | BMI <25 | BMI ≥25 | Rate of high BMI
(%) |
|---|
| Male (n=49) | 26 | 23 | 46.9 |
| Female (n=14) | 10 | 4 | 28.6 |
| Total (n=63) | 36 | 27 | 42.9 |
Results
The clinical features of the 63 patients with
urolithiasis are listed in Table I.
The mean age of the patients was 55.6 years (range, 59-78 years).
Of the total 63 patients, 49 were male and 14 were female. The mean
BMI was 24.4 (range, 17.6-41.0). The mean value of the urine PH was
6.63 (range, 5.5-7.5). The mean value of the calculus size was 9.5
mm (range, 4-35). The mean value of the uric acid was 5.86 mg/dl
(range, 2.3-10.1). The mean value of the liver CT was 56.2 (range,
30-70).
The comparison of the BMI between males and females
revealed that the male patients with urolithiasis had a higher BMI
compared with the female patients with urolithiasis. It was
observed that there was a higher percentage of obesity amongst
males compared with females, however this difference was not
significant (P=0.2207; Table
II).
Association amongst clinical
characteristics and BMI in patients with urolithiasis
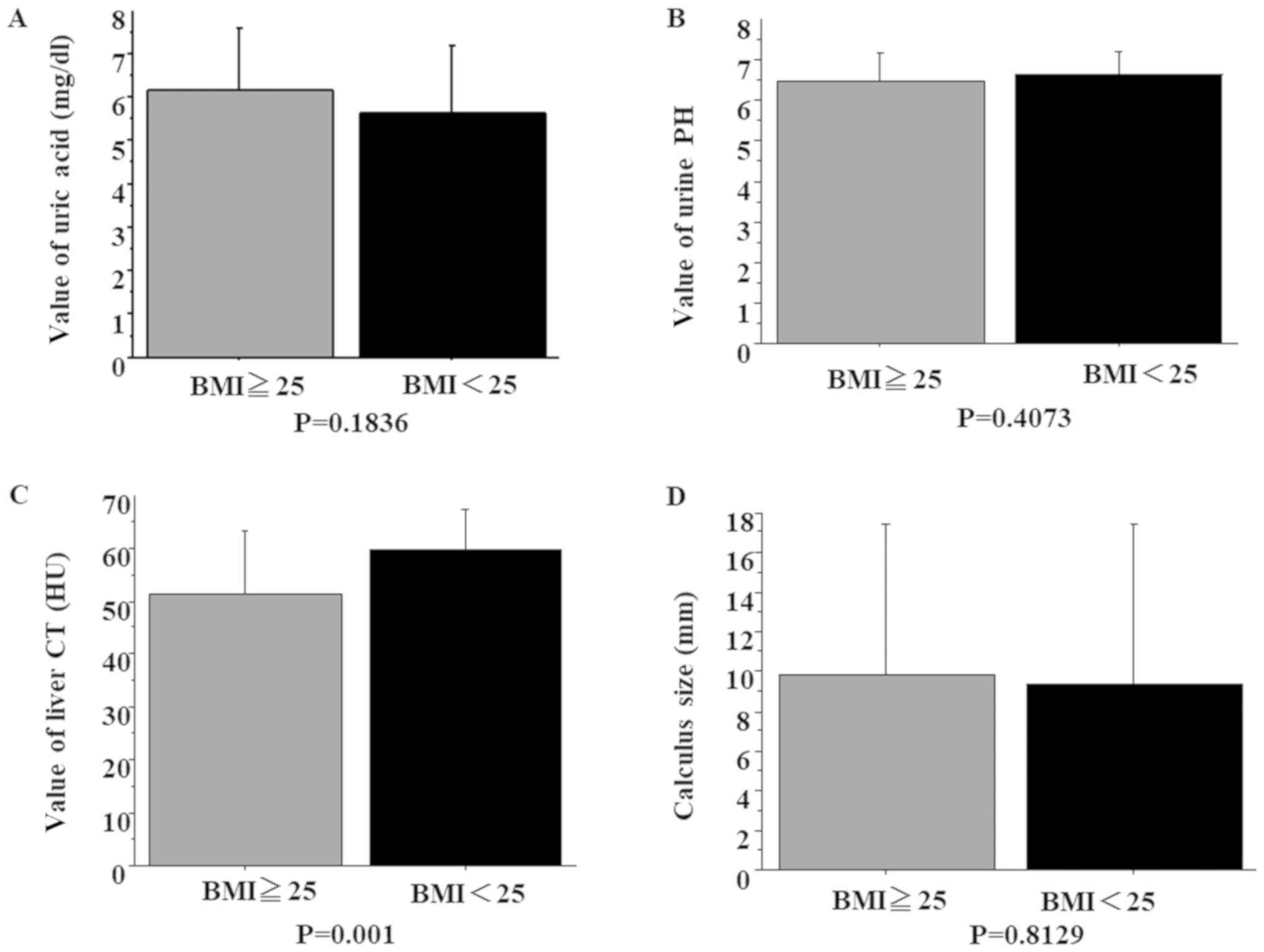
Upon comparing the normal- and high-BMI groups, no
significant differences were observed in uric acid level (P=0.1836;
Fig. 1A), urine PH (P=0.4073;
Fig. 1B) or calculus size (P=0.8129;
Fig. 1D) between the two groups.
However, liver CT values were significantly lower in the high-BMI
group compared with the normal-BMI group. (P=0.001; Fig. 1C).
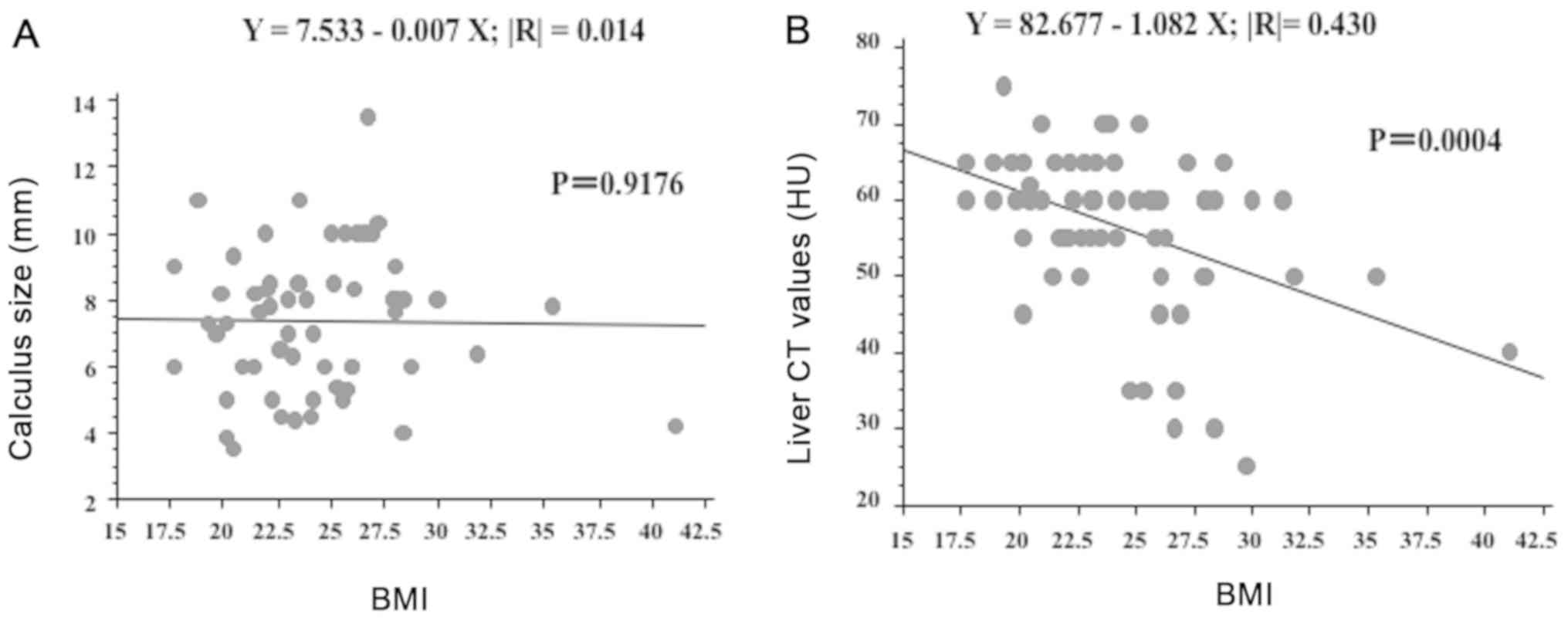
Correlation between liver CT value,
calculus size counts and BMI in patients with urolithiasis
There was no significant correlation between
calculus size counts and BMI (P=0.9176; Fig. 2A). However, a significant negative
correlation was observed between BMI and liver CT value (P=0.0004;
Fig. 2B).
Discussion
The present study examined whether there exist
differences in a number of variables, including body type and BMI,
amongst patients with urolithiasis. The present study examined
patients with urolithiasis, identified the differences between
obese-type patients with urolithiasis and normal-type patients, and
deduced that the CT value of the liver in obese-type patients with
urolithiasis is significantly lower compared with that in
standard-type patients with urolithiasis, and that obese-type
urolithiasis is more common in males compared with in females.
However, these were no significant differences between obese-type
patients with urolithiasis and standard-type patients with
urolithiasis in other factors other than liver CT values. The
present study revealed that obese-type patients with urolithiasis
were more common amongst males, and standard-type patients with
urolithiasis were more common amongst females; and these results
suggest that lifestyle-associated disease factors may not be
involved in the formation of urolithiasis in females. Furthermore,
these results suggest that the prevention of recurrence in females
with urolithiasis may be less useful compared with that in
males.
The present data indicated that liver CT values were
significantly lower in obese patients (high-BMI) with urolithiasis.
In abdominal CT examination, the liver CT value decreases with fat
deposition in such a manner that CT value has been noted to be
associated with fatty liver (12). In
fact, fatty liver may be diagnosed using the CT value of the liver
(13). The results of the present
study suggest that only fatty liver, amongst all the symptoms of
metabolic syndrome, was significantly different between normal- and
high-BMI groups.
Fatty liver affects not only the liver, but also
other aspects of metabolism. ‘Fatty liver is a phenotype in the
liver of metabolic syndrome’ (14)
and is closely associated with insulin resistance (15). Furthermore, it has been reported to be
a predictor of coronary artery disease independent of other risk
factors (16).
An increase in urolithiasis has been associated with
an increase in metabolic syndrome (6-10).
In particular, associations with type 2 diabetes, a high BMI,
hypertension, hyperlipidemia (6) and
cardiovascular diseases have been noted (7). It has been reported that the decrease in
urine pH resulting from metabolic syndrome is the mechanism for the
increase in urolithiasis (10).
Increased acid excretion through urine and ammonium excretion
disorder are considered to be responsible for decreased urinary pH;
in patients with diabetes, the main cause of uric acid calculus, a
common complication, is low urine pH (10). One study suggests that an increased
intake of fructose causes metabolic syndrome, and the low urinary
pH in turn results in an increase in urolithiasis (17). In particular, urine pH is persistently
low (usually there is a diurnal variation with a transient rise in
urine pH during the daytime). The diurnal variation of urine pH
disappears in urolithiasis, uric acid becomes insoluble and is
precipitated, and uric acid stones are formed (18).
A report on urolithiasis and metabolic
syndrome-associated factors from Japan noted that fatty liver in
male patients is a notable risk factor, an observation that the
present study supports (19).
However, in a large-scale cohort study in the United States it was
observed that weight and BMI are associated with the onset of
calculus in males and females, and that this association is
stronger in females (20). In Japan,
detailed cross-sectional studies on the presence or absence of
insulin resistance were performed, and they determined that female
patients with kidney stones had high insulin resistance and insulin
values, supporting the link between obesity and urolithiasis
(21). Furthermore, one study reports
that urolithiasis formation (calcium phosphate) is observed in the
kidney when rats receive a high cholesterol diet (22).
It has been reported that urolithiasis is similar to
arteriosclerotic lesions, one of the metabolic syndromes, in
cross-sectional studies and studies using mice models. In addition,
in this phenomenon, the number of macrophages (Mφ) of the renal
interstitium increased with the formation of calculus and an image
of Mφ phagocytizing the crystal was observed (23). From these results of this previous
study, the formation and disappearance of nephrolithiasis may be
mostly attributed to the adhesion of crystals to the renal tubule
cells, which are then transferred to the interstitial crystalline
mass, the expression of chemokines/cytokines and other associated
processes (23). Subsequent to
adhesion to vascular endothelial cells, Mφ mature, begin
phagocytosis, intracellular digestion, antigen presentation of Mφ
and finally digest the crystal (24).
However, M1 macrophages are pro-inflammatory, and M2
anti-inflammatory (25); M1s are
associated with adipocytes and metabolic syndrome, whereas M2s are
associated with organ restoration (26,27) and
carcinogenesis (28). When crystals
adhere to the renal tubular epithelium, M1-associated genes are
highly expressed and promoted by adipocytes (29); in mice in which M2 macrophages are
dysfunctional, M1 macrophages and kidney stone formation are
increased (30).
There may be a number of potential limitations in
the present study. Although the present study focused on BMI,
urolithiasis is a multifactorial disease. Additionally, although
using BMI as a marker is not the best method to measure obesity, it
has been focused on in this paper as limited other studies on
urolithiasis, to date, have focused on it.
Further studies, including studies with a larger
number of cases, a greater number of clinical factors included, and
the time course of treatment progress being taken into
consideration, are warranted to rigorously examine the
characteristics associated with urolithiasis formation.
Liver CT values correlated negatively with BMI, but
the present data indicate that other mechanisms unassociated with
fatty liver may be involved in urolithiasis in non-obese patients.
It may be suggested that physicians should consider the mechanism
involved in preventing the recurrence of urolithiasis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
HT designed the study, and wrote the initial draft
of the manuscript. HT contributed to analysis and interpretation of
data, and assisted in the preparation of the manuscript. HT
contributed to data collection and interpretation, and critically
reviewed the manuscript. All authors approved the final version of
the manuscript, and agree to be accountable for all aspects of the
work in ensuring that questions related to the accuracy or
integrity of any part of the work are appropriately investigated
and resolved.
Ethics approval and consent to
participate
All procedures used in this research were approved
by the Ethical Committee of Tokyo Medical University Ibaraki
Medical Center. Written informed consent was obtained from all
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Asper R: Epidemiology and socioeconomic
aspects of urolithiasis. Urol Res. 12:1–5. 1984.PubMed/NCBI
|
|
2
|
Yasui T, Iguchi M, Suzuki S and Kohri K:
Prevalence and epidemiological characteristics of urolithiasis in
Japan: National trends between 1965 and 2005. Urology. 71:209–213.
2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Pak CY: Kidney stones. Lancet.
351:1797–1801. 1998.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Breslau NA, Brinkley L, Hill KD and Pak
CY: Relationship of animal protein-rich diet to kidney stone
formation and calcium metabolism. J Clin Endocrinol Metab.
66:140–146. 1988.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Curhan GC, Willett WC, Rimm EB and
Stampfer MJ: A prospective study of dietary calcium and other
nutrients and the risk of symptomatic kidney stones. N Engl J Med.
328:833–838. 1993.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sakhaee K: Nephrolithiasis as a systemic
disorder. Curr Opin Nephrol Hypertens. 17:304–309. 2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sakhaee K and Maalouf NM: Metabolic
syndrome and uric acid nephrolithiasis. Semin Nephrol. 28:174–180.
2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Cameron MA, Maalouf NM, Adams-Huet B, Moe
OW and Sakhaee K: Urine composition in type 2 diabetes:
Predisposition to uric acid nephrolithiasis. J Am Soc Nephrol.
17:1422–1428. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Abate N, Chandalia M, Cab-Chan AV Jr, Moe
OW and Sakhaee K: The metabolic syndrome and uric acid
nephrolithiasis: Novel features of renal manifestation of insulin
resistance. Kidney Int. 65:386–392. 2004.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Maalouf NM, Cameron MA, Moe OW, Adams-Huet
B and Sakhaee K: Low urine pH: A novel feature of the metabolic
syndrome. Clin J Am Soc Nephrol. 2:883–888. 2007.PubMed/NCBI View Article : Google Scholar
|
|
11
|
WHO Expert Consultation: Appropriate
body-mass index for Asian populations and its implications for
policy and intervention strategies. Lancet 363: 157-163, 2004.
|
|
12
|
Bydder GM, Kreel L, Chapman RW, Harry D,
Sherlock S and Bassan L: Accuracy of computed tomography in
diagrosis of fatty liver. Br Med J. 281(1042)1980.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kan H, Kimura Y, Hyogo H, Fukuhara T,
Fujino H, Naeshiro N, Honda Y, Kawaoka T, Tsuge M, Chayama K, et
al: Non-invasive assessment of liver steatosis in non-alcoholic
fatty liver disease. Hepatol Res. 44:E420–E427. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Marchesini G, Brizi M, Bianchi G,
Tomassetti S, Bugianesi E, Lenzi M, McCullough AJ, Natale S,
Forlani G and Melchionda N: Nonalcoholic fatty liver disease: A
feature of the metabolic syndrome. Diabetes. 50:1844–1850.
2001.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Maruhama Y, Ohneda A, Tadaki H, Ohtsuki M
and Yanbe A: Hepatic steatosis and the elevated plasma insulin
level in patients with endogenous hypertriglyceridemia. Metabolism.
24:653–664. 1975.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Targher G, Bertolini L, Rodella S, Tessari
R, Zenari L, Lippi G and Arcaro G: Nonalcoholic fatty liver disease
is independently associated with an increased incidence of
cardiovascular event in type 2 diabetic patients. Diabetes Care.
30:2119–2121. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Taylor EN and Curhan GC: Fructose
consumption and the risk of kidney stones. Kidney Int. 73:207–212.
2008.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Murayama T, Sakai N, Takano T and Yamada
T: Role of the diurnal variation of urinary pH and urinary calcium
in urolithiasis: A study in outpatients. Int J Urol. 8:525–532.
2001.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sakai N: Recent issues in urolithiasis. J
Analytical Bio Sci. 32:215–219. 2009.
|
|
20
|
Taylor EN, Stampfer MJ and Curhan GC:
Obesity, weight gain, and the risk of kidney stones. JAMA.
293:455–462. 2005.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Ando R, Suzuki S, Nagaya T, Yamada T,
Okada A, Yasui T, Tozawa K, Tokudome S and Kohri K: Impact of
insulin resistance, insulin and adiponectin on kidney stones in the
Japanese population. Int J Urol. 18:131–138. 2011.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Strohmaier WL, Witte B and Nelde HJ:
Influence of nifedipine on stone formation and renal function in
chlesterol-induced nephrolithiasis in rats. Urol Int. 52:87–92.
1994.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ando R, Nagaya T, Suzuki S, Takahashi H,
Kawai M, Okada A, Yasui T, Kubota Y, Umemoto Y, Tozawa K and Kohri
K: Kidney stone formation is positively associated with
conventional risk factors for coronary heart disease in Japanese
men. J Urol. 189:1340–1346. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Okada A, Yasui T, Hamamoto S, Hirose M,
Kubota Y, Itoh Y, Tozawa K, Hayashi Y and Kohri K: Genome-wide
analysis of genes related to kidney stone formation and elimination
in the calcium oxalate nephrolithiasis model mouse: Detection of
stone-preventive factors and involvement of macrophage activity. J
Bone Miner Res. 24:908–924. 2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Mantovani A, Sica A, Sozzani S, Allavena
P, Vecchi A and Locati M: The chemokine system in diverse forms of
macrophage activation and polarization. Trends Immunol. 25:677–686.
2004.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Zhang MZ, Yao B, Yang S, Jiang L, Wang S,
Fan X, Yin H, Wong K, Miyazawa T, Chen J, et al: CSF-1 signaling
mediates recovery from acute kidney injury. J Clin Invest.
122:4519–4532. 2012.PubMed/NCBI View
Article : Google Scholar
|
|
27
|
Lee S, Huen S, Nishio H, Nishio S, Lee HK,
Choi BS, Ruhrberg C and Cantley LG: Distinct macrophage phenotypes
contribute to kidney injury and repair. J Am Soc Nephrol.
22:317–326. 2011.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Takeuchi H, Tanaka M, Tanaka A, Tsunemi A
and Yamamoto H: Predominance of M2-polarized macrophages in bladder
cancer affects angiogenesis, tumor grade and invasiveness. Oncol
Lett. 11:3403–3408. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ichikawa J, Okada A, Taguchi K, Fujii Y,
Zuo L, Niimi K, Hamamoto S, Kubota Y, Umemoto Y, Kohri K, et al:
Increased crystal-cell interaction in vitro under co-culture of
renal tubular cells and adipocytes by in vitro co-culture paracrine
systems simulating metabolic syndrome. Urolithiasis. 42:17–28.
2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Taguchi K, Okada A, Kitamura H, Yasui T,
Naiki T, Hamamoto S, Ando R, Mizuno K, Kawai N, Kohri K, et al:
Colony-stimulating factor-1 signaling suppresses renal crystal
formation. J Am Soc Nephrol. 25:1680–1697. 2014.PubMed/NCBI View Article : Google Scholar
|