Introduction
The prevalence of metabolic syndrome (Mets), which
is defined as obesity with hypertension or glucose intolerance, has
been increasing worldwide and varies from 12-41% (1). Several studies demonstrated that
moderate alcohol consumption reduces the risk of Mets-related
diseases and mortality (2-8).
Light or moderate alcohol consumption is reported to enhance
insulin sensitivity, increase high-density lipoprotein cholesterol
(HDL-C) and reduce the risk of type 2 diabetes mellitus (9). Moreover, non-alcoholic fatty liver
disease (NAFLD) is considered a phenotype of Mets in the liver
(10-12).
According to previous studies in Japan, the prevalence of NAFLD in
the general population ranges from 24.6-29.7% (13,14) and
light or moderate alcohol consumption is negatively associated with
fatty liver (15-19).
Previously, chronic kidney disease (CKD) has been considered a
renal phenotype of Mets (20).
Previous studies reported that light or moderate alcohol
consumption reduced the risk of CKD (21,22).
Elevated serum uric acid has been proposed as a risk factor for not
only CKD (23) but also diabetes
(24) and hypertension (25). While alcohol consumption has been
recognized as an important risk factor for gout and hyperuricemia,
moderate alcohol consumption does not increase the risk of
hyperuricemia (26,27). However, certain studies reported that
even light alcohol consumption (LAC) could increase blood pressure
in Japanese men (28-30).
Recently, liver dysfunction and hypercholesterolemia
have been reported as the most common abnormal findings associated
with Mets among individuals who underwent a regular health check-up
in Japan. The main reason for the increase in liver dysfunction is
associated with the increasing incidence of NAFLD (31). Although there have been some reports
on the effect of LAC on Mets-related diseases in individuals with
NAFLD, the association between LAC and each Mets-related disease
among those with or without fatty liver is unclear. Therefore, this
study investigated the effect of LAC on Mets-related diseases, such
as obesity, dyslipidemia, impaired glucose tolerance (IGT),
hyperuricemia and CKD, in individuals with and without fatty
liver.
Patients and methods
Subjects
In this cross-sectional study, 2,096 men who
underwent regular health check-up, including physical and
physiological examinations, abdominal ultrasound, and blood
screening examination, between January 2017 and December 2017 at
Fukuchiyama City Hospital (Fukuchiyama City, Japan) were enrolled.
Subjects were included if they fulfilled the following criteria:
Absence of markers of hepatitis B surface antigen and hepatitis C
antibody, alcohol consumption ≥20 g/day, and chronic liver
diseases, including autoimmune hepatitis, primary biliary
cholangitis, and drug-induced liver disease. Patients judged to be
inappropriate for this study were excluded (n=906). A total of
1,190 eligible subjects were analyzed. Patient characteristics are
shown in Table I. All patients
provided written informed consent prior to participation and the
study was conducted in accordance with the Declaration of Helsinki
and was approved by the institutional review board of Fukuchiyama
City Hospital.
 | Table IComparison of clinical
characteristics between non-drinkers and light drinkers. |
Table I
Comparison of clinical
characteristics between non-drinkers and light drinkers.
|
Characteristics | Non-drinker
(n=505) | Light drinker
(n=685) | P-value |
|---|
| Age (years) | 56 (28-83) | 56 (24-78) | 0.920 |
| BMI
(kg/m2) | 23.6
(15.2-52.9) | 23.3
(16.0-41.4) | 0.150 |
| WC (cm) | 85.5
(61.0-143.0) | 85.0
(63.0-127.0) | 0.080 |
| Obesity | 174 (34.4) | 195 (28.3) | 0.020 |
| SBP (mmHg) | 126 (93-196) | 128 (94-190) | 0.212 |
| DBP (mmHg) | 79 (48-122) | 81 (54-112) | 0.028 |
| Hypertension | 200 (39.6) | 298 (43.3) | 0.194 |
| T-CHO (mg/dl) | 197 (86-330) | 195 (106-312) | 0.769 |
| TG (mg/dl) | 104 (18-772) | 93 (28-648) | 0.009 |
| HDL (mg/dl) | 50 (26-93) | 54 (27-100) | <0.001 |
| LDL (mg/dl) | 123 (33-228) | 119 (47-229) | 0.007 |
| Dyslipidemia | 296 (58.6) | 329 (47.8) | <0.001 |
| FPG (mg/dl) | 98 (74-284) | 98 (76-291) | 0.149 |
| HbA1c (NGSP)
(%) | 5.9 (4.6-12.0) | 5.8 (4.9-11.1) | 0.016 |
| IGT | 119 (23.5) | 117 (17.0) | 0.006 |
| UA (mg/dl) | 5.8 (0.9-11.1) | 6.0 (0.9-9.6) | 0.076 |
| Hyperuricemia | 106 (20.9) | 148 (21.6) | 0.798 |
| AST (IU/l) | 21 (12-64) | 22 (12-124) | 0.094 |
| ALT (IU/l) | 22 (6-108) | 21 (9-148) | 0.314 |
| GGT (IU/l) | 26 (9-202) | 30 (9-737) | 0.001 |
| Fib-4 index | 1.07
(0.29-3.96) | 1.16
(0.35-3.86) | 0.027 |
| Fatty liver | 269 (53.7) | 292 (42.8) | <0.001 |
| eGFR (ml/min/1.73
m2) | 75.7
(12.2-151.5) | 75.8
(40.9-136.1) | 0.644 |
| Proteinuria | 41 (8.1) | 32 (4.6) | 0.014 |
| CKD | 91 (18.0) | 89 (12.9) | 0.017 |
| Mets by Japanese
criteria | 145 (28.7) | 144 (20.9) | 0.002 |
| Regular
exercises | 109 (21.5) | 192 (28.0) | 0.011 |
| Current
smoking | 99 (19.6) | 124 (18.1) | 0.512 |
Physical examination and serum
biochemistry
The subjects were divided into two groups: Fatty
liver group and non-fatty liver group. Body weight and height were
obtained for both groups, and body mass index (BMI) was calculated.
Waist circumference (WC) was measured at the level of the umbilicus
according to the definition in the Japanese Committee for the
Diagnostic Criteria of Metabolic Syndrome (32). Venous blood samples (10 ml) were
obtained from all subjects following a 12-h overnight fast.
Aspartate aminotransferase, alanine aminotransferase, γ-glutamyl
transpeptidase (GGT), total cholesterol, HDL-C, triglycerides (TG),
low-density lipoprotein cholesterol (LDL-C), uric acid (UA),
fasting plasma glucose (FPG), hemoglobin A1c (HbA1c; National
Glycohemoglobin Standardization Program) and estimated glomerular
filtration rate (eGFR) were measured using standard clinical
chemistry laboratory techniques.
Assessment of fatty liver
All the subjects received an abdominal ultrasound to
assess fatty liver. Experienced technicians performed real-time
ultrasonography to detect vascular blurring, deep attenuation and
increased liver echotexture in comparison to the kidneys
(liver-kidney contrast) to assess fatty infiltration (33). Each certificated gastroenterologist
independently reviewed the images and judged that the presence of
one or more findings was indicative of a fatty liver.
Evaluation of alcohol consumption
Lifestyle-related information, such as medical
history, smoking status and alcohol consumption, was obtained using
a common standardized self-response questionnaire. The amount of
alcohol consumption per day was calculated in grams using the
representative percentage of alcohol by volume of each type of
alcohol beverage. Subjects were classified into two groups
according to drinking information: Non-drinkers and light drinkers;
the latter is defined as those who consumed >0 to <20 g of
alcohol per day.
Variables
Obesity was defined as BMI ≥25 kg/m2,
which is the commonly used definition of obesity in the Japanese
population (34). Hypertension was
defined as systolic blood pressure (SBP) ≥140 mmHg, diastolic blood
pressure (DBP) ≥90 mmHg, or the use of medications for
hypertension. Dyslipidemia was defined as TG ≥150 mg/dl, HDL-C
<40 mg/dl and LDL-C ≥140 mg/dl or the use of medications for
dyslipidemia. IGT was defined as FPG ≥110 mg/dl or the use of
medications for diabetes mellitus. Hyperuricemia was defined as UA
>7.0 mg/dl or the use of medications for hyperuricemia. CKD was
defined as eGFR <60 ml/min/1.73 m2 and/or overt
proteinuria (35). According to the
Japanese criteria, Mets is defined as WC ≥85 cm and the presence of
two or more of the following risk factors: SBP ≥130 mmHg or DBP ≥85
mmHg; reduced HDL-C (HDL-C <40 mg/dl) and/or increased TG (TG
≥150 mg/dl); and FPG ≥110 mg/dl.
Statistical analysis
Baseline data were expressed as median with
interquartile range and subject number (%) for categorical
variables. P-values were calculated using a Mann-Whitney U test for
continuous variables and Fisher's exact probability test or the Chi
square test for categorical variables. Factors with a significant
influence on the prevalence of hypertension in the non-fatty liver
group were determined by univariate analysis. Age, obesity,
dyslipidemia, IGT, hyperuricemia, CKD, smoking and LAC were
subsequently subjected to multivariable logistic regression
analyses. P<0.05 was considered to indicate a statistically
significant difference. IBM SPSS version 16.0 for Windows (SPSS,
Inc.) was used in the statistical analyses.
Results
Clinical characteristics of
non-drinkers and light drinkers
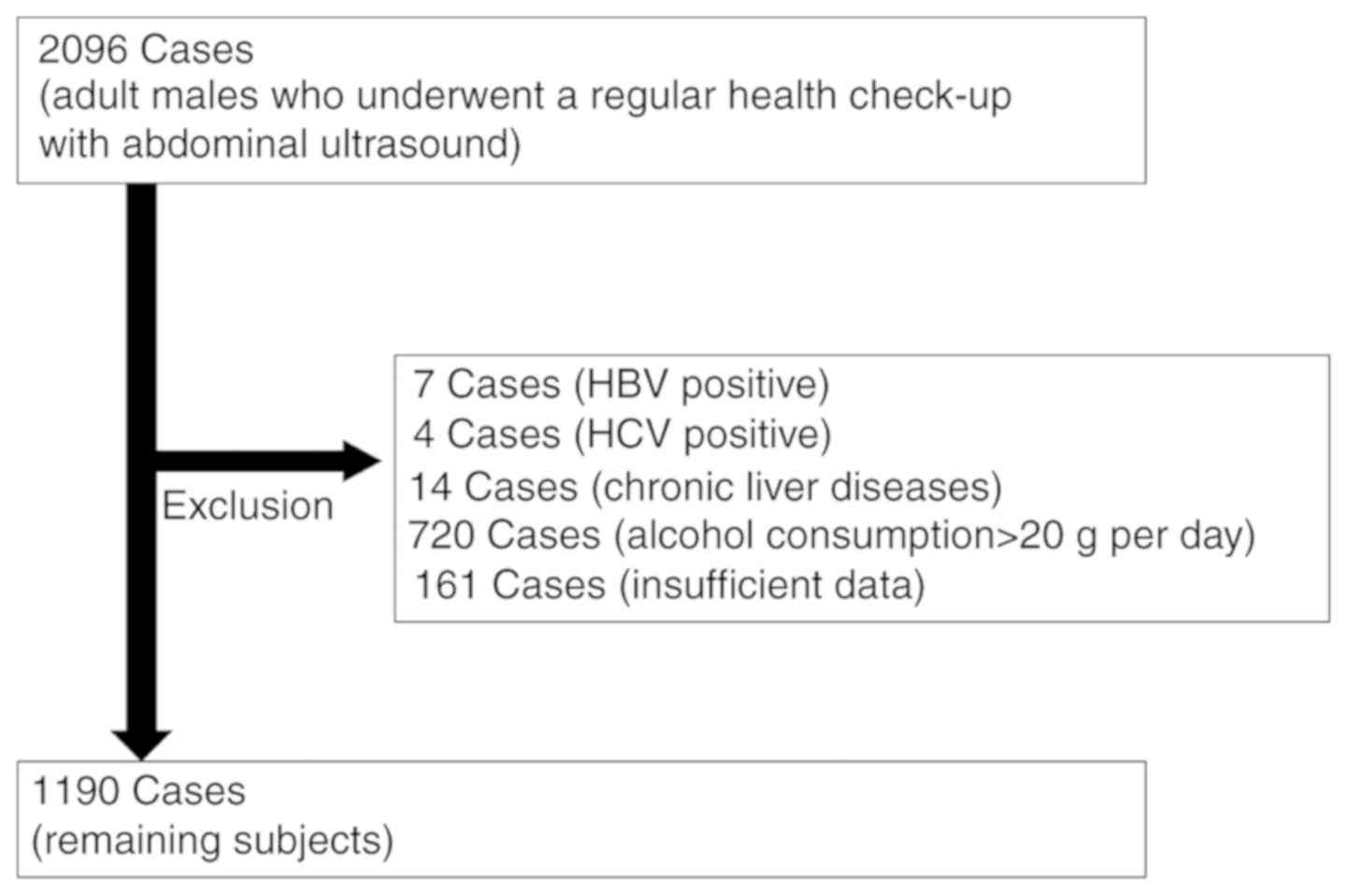
The protocol followed for participant selection and
enrollment is shown in Fig. 1. Of the
2,096 participants, 906 were excluded. Of the 1,190 participants
included in the analysis, 505 (42.4%) were non-drinkers and 685
(57.6%) were light drinkers. Table I
shows the comparison of the clinical characteristics between
non-drinkers and light drinkers. No significant difference was
noted between non-drinkers and light drinkers in terms of age and
BMI. TG, LDL, HbA1c and the prevalence of proteinuria were
significantly decreased in light drinkers compared with in
non-drinkers (P<0.01). DBP, HDL, GGT, and Fib-4 index were
significantly increased in light drinkers compared with in
non-drinkers (P<0.05). No significant difference was observed
between non-drinkers and light drinkers in the prevalence of
hypertension and hyperuricemia. The prevalence of obesity,
dyslipidemia, IGT, fatty liver, CKD and Mets, according to the
Japanese criteria, was significantly decreased in light drinkers
compared with in non-drinkers (P<0.05); in fact, this prevalence
was lowest in light drinkers among the 4 groups of participants
(non-drinkers; light drinkers, alcohol use/day <20 g; moderate
drinkers, alcohol use/day 20-59 g; heavy drinkers, alcohol use/day
≥60 g; Table SI). Among the
lifestyle parameters, regular exercise habit was significantly more
prevalent in light drinkers than in non-drinkers (P<0.05), but
no significant difference was noted between non-drinkers and light
drinkers in terms of current smoking.
Treatment for each Mets-related
diseases in non-drinkers and light drinkers
A comparison of the treatment for each Mets-related
disease between non-drinkers and light drinkers is shown in
Table II. No significant difference
in the treatment for hypertension was observed between non-drinkers
and light drinkers. DBP in those without treatment for hypertension
was significantly increased in light drinkers compared with in
non-drinkers (P<0.01). No significant difference in the
treatment for dyslipidemia was noted between non-drinkers and light
drinkers. Regardless of treatment for dyslipidemia, HDL was
significantly increased in light drinkers compared with in
non-drinkers (P<0.001). TG and HDL levels in those without
treatment for dyslipidemia were significantly decreased in light
drinkers compared with those in non-drinkers. The number of
subjects receiving treatment for IGT was significantly decreased
among light drinkers compared with among non-drinkers (P<0.05).
No significant difference was found in the treatment for
hyperuricemia between non-drinkers and light drinkers.
| Table IIComparison between non- and light
drinkers receiving treatment for Mets-associated diseases. |
Table II
Comparison between non- and light
drinkers receiving treatment for Mets-associated diseases.
| A,
Hypertension |
|---|
|
Characteristics | Non-drinker
(n=505) | Light drinker
(n=685) | P-value |
|---|
| Treatment | 119 (23.6) | 159 (23.2) | 0.887 |
|
SBP
(mmHg) | 132 (101-179) | 132 (94-170) | 0.383 |
|
DBP
(mmHg) | 83 (54-111) | 83 (54-109) | 0.404 |
| Treatment (-) | 386 (76.4) | 526 (76.8) | |
|
SBP
(mmHg) | 123 (96-196) | 126 (94-190) | 0.068 |
|
DBP
(mmHg) | 78 (48-122) | 81 (56-112) | 0.003 |
| B,
Dyslipidemia |
|
Characteristics | Non-drinker
(n=505) | Light drinker
(n=685) | P-value |
| Treatment (+) | 101 (20.0) | 108 (15.7) | 0.058 |
|
T-CHO
(mg/dl) | 185 (114-330) | 181 (128-293) | 0.894 |
|
TG
(mg/dl) | 113 (42-772) | 100 (42-304) | 0.310 |
|
HDL
(mg/dl) | 49 (26-77) | 54 (31-93) | 0.004 |
|
LDL
(mg/dl) | 110 (46-228) | 105 (61-203) | 0.105 |
| Treatment (-) | 404 (80.0) | 577 (74.3) | |
|
T-CHO
(mg/dl) | 202 (86-300) | 198 (106-312) | 0.484 |
|
TG
(mg/dl) | 101 (18-687) | 91 (28-648) | 0.028 |
|
HDL
(mg/dl) | 51 (27-93) | 54 (27-100) | <0.001 |
|
LDL
(mg/dl) | 126 (33-202) | 121 (47-229) | 0.006 |
| C, IGT |
|
Characteristics | Non-drinker
(n=505) | Light drinker
(n=685) | P-value |
| Treatment (+) | 44 (8.7) | 38 (5.5) | 0.033 |
|
FPG
(mg/dl) | 130 (83-84) | 134 (87-220) | 0.649 |
|
HbA1c (NGSP)
(%) | 7.0 (5.0-12.0) | 6.8 (6.1-10.8) | 0.666 |
| Treatment (-), n
(%) | 461 (91.3) | 647 (94.5) | |
|
FPG
(mg/dl) | 98 (74-156) | 97 (76-291) | 0.360 |
|
HbA1c (NGSP)
(%) | 5.8 (4.6-8.4) | 5.7 (4.9-11.1) | 0.051 |
| D,
Hyperuricemia |
|
Characteristics | Non-drinker
(n=505) | Light drinker
(n=685) | P-value |
| Treatment (+) | 30 (5.9) | 52 (7.6) | 0.229 |
|
UA
(mg/dl) | 6.2 (4.3-7.9) | 6.5 (3.6-8.7) | 0.296 |
| Treatment (-), n
(%) | 475 (94.1) | 632 (92.4) | |
|
UA
(mg/dl) | 5.8 (0.9-11.1) | 6.0 (0.6-9.6) | 0.148 |
Prevalence of Mets-related diseases
and risk factors between non-drinkers and light drinkers
A comparison of the prevalence of each risk factor
for Mets-related diseases between non-drinkers and light drinkers
in the non-fatty liver and fatty liver groups are shown in Table III. In the non-fatty liver group, no
significant difference was found in age and BMI between
non-drinkers and light drinkers. The prevalence of hypertension was
significantly increased in light drinkers compared with in
non-drinkers (P<0.05; Table
III). In the fatty liver group, no significant difference was
observed in age and BMI between non-drinkers and light drinkers.
The prevalence of dyslipidemia, IGT and Mets by the Japanese
criteria was significantly decreased in light drinkers than in
non-drinkers (P<0.05; Table
III).
| Table IIIComparison of the prevalence of
Mets-associated diseases and risk factors between non-drinkers and
light drinkers. |
Table III
Comparison of the prevalence of
Mets-associated diseases and risk factors between non-drinkers and
light drinkers.
| A, Prevalence of
Mets-associated diseases and risk factors in the non-fatty liver
group |
|---|
| Characteristic | Non-drinker
(n=236) | Light drinker
(n=393) | P-value |
|---|
| Age (years) | 56 (28-83) | 56 (24-78) | 0.610 |
| BMI
(kg/m2) | 21.8
(15.2-31.4) | 22.1
(16.1-33.1) | 0.060 |
| Obesity | 28 (11.8) | 53 (13.4) | 0.557 |
| Hypertension | 63 (26.6) | 139 (35.3) | 0.024 |
| Dyslipidemia | 106 (44.9) | 148 (37.6) | 0.073 |
| IGT | 27 (11.4) | 53 (13.4) | 0.456 |
| Hyperuricemia | 31 (13.1) | 61 (15.5) | 0.413 |
| CKD | 38 (16.1) | 49 (12.4) | 0.202 |
| Mets by Japanese
criteria | 25 (20.5) | 45 (11.4) | 0.741 |
| Regular
exercises | 66 (27.9) | 128 (32.5) | 0.336 |
| Current
smoking | 58 (24.5) | 71 (18.0) | 0.050 |
| B, Prevalence of
Mets-associated diseases and risk factors in the fatty liver
group |
| Characteristic | Non-drinker
(n=269) | Light drinker
(n=292) | P-value |
| Age (years) | 56 (30-75) | 56 (31-76) | 0.479 |
| BMI
(kg/m2) | 25.2
(19.3-52.9) | 24.8
(18.6-41.4) | 0.133 |
| Obesity | 146 (54.2) | 140 (47.9) | 0.134 |
| Hypertension | 137 (50.9) | 158 (54.1) | 0.451 |
| Dyslipidemia | 189 (70.2) | 179 (61.3) | 0.026 |
| IGT | 92 (34.2) | 64 (21.9) | 0.001 |
| Hyperuricemia | 75 (27.8) | 87 (29.2) | 0.617 |
| CKD | 53 (19.7) | 40 (13.6) | 0.057 |
| Mets by Japanese
criteria | 120 (44.6) | 98 (33.5) | 0.007 |
| Regular
exercises | 43 (15.9) | 64 (21.9) | 0.074 |
| Current
smoking | 41 (15.2) | 53 (18.1) | 0.357 |
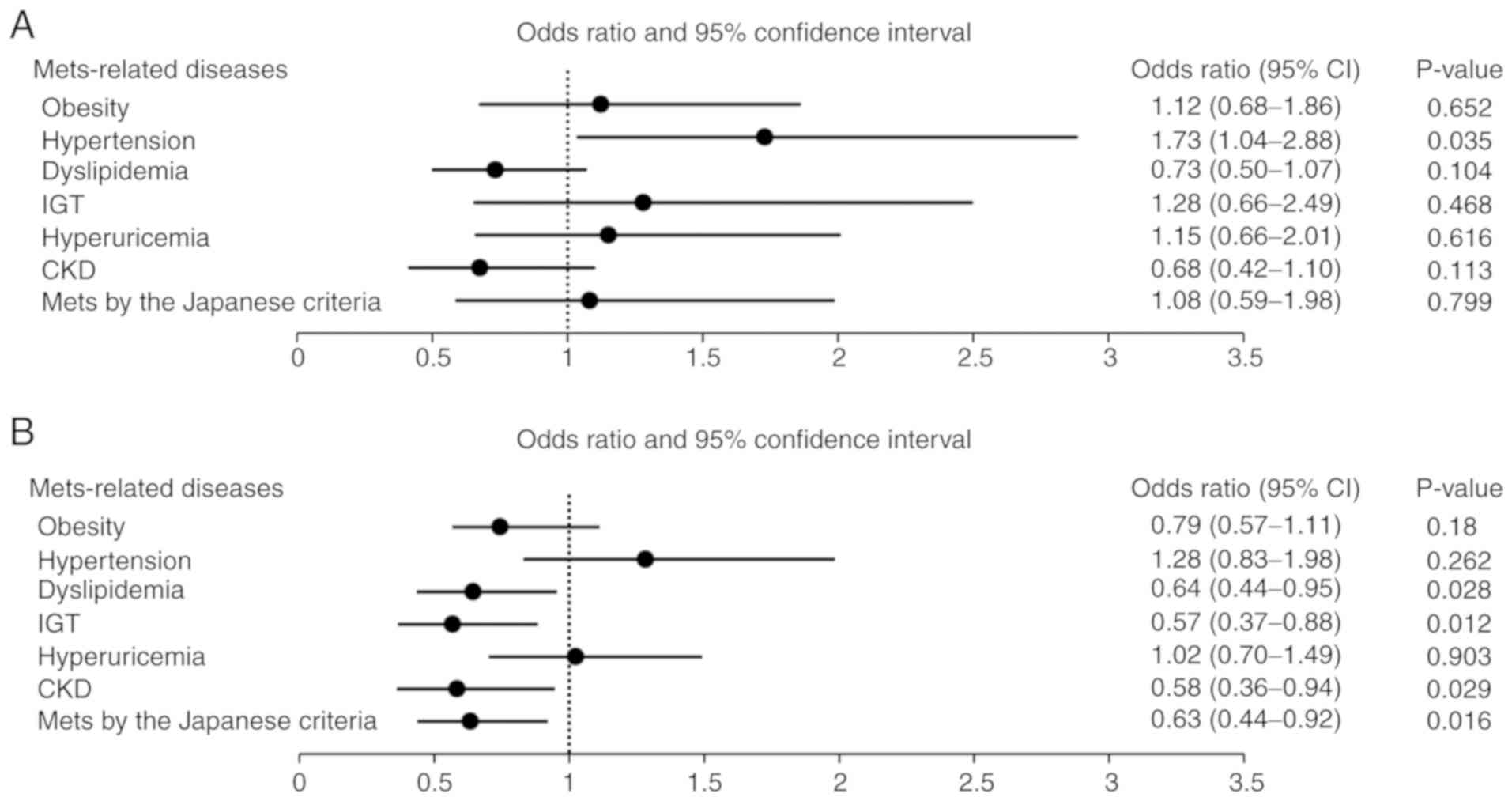
Odds ratio for each Mets-related
diseases comparing light drinkers to non-drinkers
The odds ratio [OR; 95% confidence interval (CI),
P-value] for each Mets-related disease in light drinkers and
non-drinkers is shown in Fig. 2. In
the non-fatty liver group, the OR for hypertension among light
drinkers was 1.73 (1.04-2.88, P=0.035). In the fatty liver group,
the OR for each Mets-related disease among light drinkers were as
follows: Dyslipidemia, 0.64 (0.44-0.95, P=0.028); IGT, 0.57
(0.37-0.88, P=0.012); CKD, 0.58 (0.36-0.94, P=0.029) and Mets by
the Japanese criteria, 0.63 (0.44-0.92, P=0.016).
Discussion
In this cross-sectional study, the results indicated
that the effect of LAC was different between individuals with and
those without fatty liver. In the non-fatty liver group, the
prevalence of hypertension in light drinkers was 35.3%, which was
increased compared with in non-drinkers (26.6%). In the fatty liver
group, the prevalence of dyslipidemia, IGT, CKD and Mets by the
Japanese criteria was lower in light drinkers than that in
non-drinkers.
Fatty liver among non-drinkers and light drinkers
was diagnosed as NAFLD, which is considered a phenotype of Mets in
the liver (10-12).
Previous studies reported that light or moderate alcohol
consumption is negatively associated with fatty liver (15-19).
The mechanism of inverse association of alcohol consumption with
fatty liver has been previously elucidated. Moderate alcohol
consumption has been shown to reduce fasting serum insulin and TG
levels and is associated with a lower incidence of diabetes, all of
which are important risk factors for the development of NAFLD
(2,36). In addition, certain studies revealed
that the level of adiponectin, which is a hormone involved in lipid
and glucose homeostasis and is reduced in patients with NAFLD, is
upregulated in people who consume alcohol (37-39).
Antioxidant agents in alcoholic beverages, mostly in wine (15), may also exert a protective effect in
NAFLD. In this study, the serum levels of TG, LDL and HbA1c were
lower, and the prevalence of IGT and fatty liver was decreased in
light drinkers compared with in non-drinkers.
The relationship between alcohol consumption and
all-cause mortality has been reported to have J- or U-shaped curve
(8). This effect is thought to be
mainly because of reduction in cardiovascular disease (40,41), which
can be attributed to the beneficial effect of alcohol on plasma
lipids levels, hemostatic factors (2,41) and
insulin sensitivity (36). Several
studies have shown the influence of lifestyle factors on better
mortality in moderate drinkers. Moderate alcohol users tend to have
higher socioeconomic status, high level of education, increased
physical activity and less obesity (42,43). The
prevalence of subjects with regular exercise habit was greater in
light drinkers in the present study.
Moreover, the present study indicated that in all
subjects, the prevalence of obesity, dyslipidemia, IGT, fatty
liver, CKD and Mets by the Japanese criteria was decreased among
light drinkers compared with among non-drinkers. These results
agreed with those of previous reports (2-9,15-22,36,37,40-45).
In the non-fatty liver group, because the prevalence of
Mets-related diseases was low, no significant relationship between
LAC and the prevalence of Mets-related diseases without
hypertension was observed. In the fatty liver group, a relationship
between LAC and lower prevalence of dyslipidemia, IGT, CKD and Mets
by the Japanese criteria was observed. The inverse association
between LAC and the prevalence of dyslipidemia, IGT, CKD, and Mets
by the Japanese criteria may be explained by an improvement in
insulin sensitivity and other metabolic parameters, including
improved cytokine profiles and decreased oxidative stress, as has
been described in the general population (8,12,30,44,45). NAFLD
is considered a phenotype of Mets in the liver (10-12)
and in the fatty liver group, the prevalence of each Mets-related
disease was actually increased compared with in the non-fatty liver
group in this study. Thus, the effect of LAC to suppress
Mets-related diseases has been shown more clearly in the fatty
liver group.
Nonetheless, numerous studies have shown that
alcohol consumption is associated with increased blood pressure.
Furthermore, increased alcohol consumption affects endothelial
function (40,46). Oda et al (30) reported that light to moderate alcohol
consumption impairs endothelial function. Endothelial dysfunction
is the initial stage in the pathogenesis of atherosclerosis and
plays an important role in the development of atherosclerosis and
hypertension. The present study indicated that the prevalence of
hypertension is increased in light drinkers compared with in
non-drinkers, especially in the non-fatty liver group. While it may
suppress fatty liver, LAC may promote hypertension. Increased
caloric intake through consuming alcoholic beverages and elevated
salt intake associated with drinking may also be involved in
alcohol-related hypertension (47).
Taking into consideration that liver dysfunction is the most common
abnormal finding associated with Mets in a regular health check-up
(31), hypertension could occur in
Mets-related diseases first. Moreover, in the fatty liver group, no
significant relationship between LAC and hypertension was found.
VanWagner et al (48) reported
that alcohol use may not reduce the risk of cardiovascular disease
in patients with NAFLD. A previous study also demonstrated that
alcohol use is not associated with a significant difference in
markers of subclinical atherosclerosis, such as coronary artery
calcium, which is a well-established risk marker for future
cardiovascular events (49).
This study has some limitations. Eating habits,
which may have an influence on Mets-related diseases and the types
of beverages consumed were not evaluated. Selection bias was also
possible. Most of the participants were healthy and willing to
undergo medical check-up. Further studies are needed to address
these limitations.
In conclusion, the present study found that the
effect of LAC was different between individuals with and those
without fatty liver. In the non-fatty liver group, LAC may increase
the risk of hypertension, whereas in the fatty liver group, LAC may
decrease the prevalence of dyslipidemia, IGT, CKD and Mets by the
Japanese criteria. The effect of LAC to suppress Mets-related
diseases has been shown more clearly in the fatty liver group,
because of the higher prevalence of each Mets-related disease. On
the other hand, it may suppress fatty liver and LAC may promote
hypertension.
Supplementary Material
Comparison of prevalence of
Mets-associated diseases among participants.
Acknowledgements
The authors thank all the members of the Department
of Gastroenterology and Hepatology, Fukuchiyama City Hospital. The
authors would also like to thank Noriko for assistance with data
collection.
Funding
No funding was received.
Availability of data and materials
The datasets of the present study are available from
the corresponding author on reasonable request.
Authors' contributions
The study was conducted and designed by TH. TH, NI,
YIn, TT, TO, TK and KK collected and interpreted clinical data. The
results were analyzed and interpreted by TH, YS and YIt. TH wrote
the first draft of the manuscript and YS and YIt contributed to the
writing of the manuscript. All authors have read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
This study was conducted in accordance with the
Declaration of Helsinki and approved by the institutional review
board of Fukuchiyama City Hospital (Fukuchiyama City, Japan). All
patients provided written informed consent prior to
participation.
Patient consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing
interests.
References
|
1
|
Deepa M, Farooq S, Datta M, Deepa R and
Mohan V: Prevalence of metabolic syndrome using WHO, ATPIII and IDF
definitions in Asian Indians: The chennai urban rural epidemiology
study (CURES-34). Diabetes Metab Res Rev. 23:127–134.
2007.PubMed/NCBI View
Article : Google Scholar
|
|
2
|
Gaziano JM, Buring JE, Breslow JL,
Goldhaber SZ, Rosner B, VanDenburgh M, Willett W and Hennekens CH:
Moderate alcohol intake, increased levels of high-density
lipoprotein and its subfractions, and decreased risk of myocardial
infarction. N Engl J Med. 329:1829–1834. 1993.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Conigrave KM, Hu BF, Camargo CA Jr,
Stampfer MJ, Willett WC and Rimm EB: A prospective study of
drinking patterns in relation to risk of type 2 diabetes among men.
Diabetes. 50:2390–2395. 2001.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mukamal KJ, Conigrave KM, Mittleman MA,
Camargo CA Jr, Stampfer MJ, Willett WC and Rimm EB: Roles of
drinking pattern and type of alcohol consumed in coronary heart
disease in men. N Engl J Med. 348:109–118. 2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Tolstrup J, Jensen MK, Tjonnald A, Overvad
K, Mukamal KJ and Grønbaek M: Prospective study of alcohol drinking
patterns and coronary heart diseases in women and men. BMJ.
332:1244–1248. 2006. View Article : Google Scholar
|
|
6
|
Gaziano JM, Gaziano TA, Glynn RJ, Sesso
HD, Ajani UA, Stampfer MJ, Manson JE, Hennekens CH and Buring JE:
Light-to-moderate alcohol consumption and mortality in the
Physicians' Health Study enrollment cohort. J Am Coll Cardiol.
35:96–105. 2000.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Freiberg MS, Cabral HJ, Heeren TC, Vasan
RS and Curtis Ellison R: Third National Health and Nutrition
Examination Survey: Alcohol consumption and the prevalence of the
metabolic syndrome in the US: A cross-sectional analysis of data
from the Third National Health And Nutrition Examination Survey.
Diabetes Care. 27:2954–2959. 2004.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Thun MJ, Peto R, Lopez AD, Monaco JH,
Henley SJ, Heath CW Jr and Doll R: Alcohol consumption and
mortality among middle-aged and elderly U.S. adults. N Engl J Med.
337:1705–1714. 1997.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Wannamethee SG, Camargo CA Jr, Manson JE,
Willett WC and Rimm EB: Alcohol drinking patterns and risk of type
2 diabetes mellitus among younger women. Arch Intern Med.
163:1329–1336. 2003.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Neuschwander-Tetri BA: Nonalcoholic
steatohepatitis and the metabolic syndrome. Am J Med Sci.
330:326–335. 2005.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Marchesini G, Brizi M, Bianchi G,
Tomassetti S, Bugianesi E, Lenzi M, McCullough AJ, Natale S,
Forlani G and Melchionda N: Nonalcoholic fatty liver disease: A
feature of the metabolic syndrome. Diabetes. 50:1844–1850.
2001.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Eckel RH, Grundy SM and Zimmet PZ: The
metabolic syndrome. Lancet. 365:1415–1428. 2005.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Eguchi Y, Hyogo H, Ono M, Mizuta T, Ono N,
Fujimoto K, Chayama K and Saibara T: JSG-NAFLD: Prevalence and
associated metabolic factors of nonalcoholic fatty liver disease in
the general population from 2009 to 2010 in Japan: A multicenter
large retrospective study. J Gastroenterol. 47:586–595.
2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Nishioji K, Sumida Y, Kamaguchi M,
Mochizuki N, Kobayashi M, Nishimura T, Yamaguchi K and Itoh Y:
Prevalence of and risk factors for non-alcoholic fatty liver
diseases in a non-obese Japanese population, 2011-2012. J
Gastroenterol. 50:95–108. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Dunn W, Xu R and Schwimmer JB: Modest wine
drinking and decreased prevalence of suspected nonalcoholic fatty
liver disease. Hepatology. 47:1947–1954. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Gunji T, Matsuhashi N, Sato H, Fujibayashi
K, Okumura M, Sasabe N and Urabe A: Light and moderate alcohol
consumption significantly reduces the prevalence of fatty liver in
the Japanese male population. Am J Gastroenterol. 104:2189–2195.
2009.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Moriya A, Iwasaki Y, Ohguchi S, Kayashima
E, Mitsumune T, Taniguchi H, Ikeda F, Shiratori Y and Yamamoto K:
Alcohol consumption appears to protect against non-alcoholic fatty
liver disease. Aliment Pharmacol Ther. 33:378–388. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hamaguchi M, Kojima T, Ohbora A, Takeda N,
Fukui M and Kato T: Protective effect of alcohol consumption for
fatty liver but not metabolic syndrome. World J Gastroenterol.
18:156–167. 2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sogabe M, Okahisa T, Taniguchi T, Tomonari
T, Tanaka T, Tanaka H, Nakasono M and Takayama T: Light alcohol
consumption plays a protective role against non-alcoholic fatty
liver disease in Japanese men with metabolic syndrome. Liver Int.
35:1707–1714. 2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kang HT, Kim JK, Shim JY, Lee HR, Linton
JA and Lee YJ: Low grade inflammation, metabolic syndrome and the
risk of chronic kidney disease: The 2005 Korean national health and
nutrition examination survey. J Korean Med Sci. 27:630–635.
2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Yamagata K, Ishida K, Sairenchi T,
Takahashi H, Ohba S, Shiigai T, Narita M and Koyama A: Risk factors
for chronic kidney disease in a community-based population: A
10-year follow-up study. Kidney Int. 71:159–166. 2007.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Shankar A, Klein R and Klein BE: The
association among smoking, heavy drinking, and chronic kidney
disease. Am J Epidemiol. 164:263–271. 2006.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Jalal DI, Chonchol M, Chen W and Targher
G: Uric acid as a target of therapy in CKD. Am J Kidney Dis.
61:134–146. 2013.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kodama S, Saito K, Yachi Y, Asumi M,
Sugawara A, Totsuka K, Saito A and Sone H: Association between
serum uric acid and development of type 2 diabetes. Diabetes Care.
32:1737–1742. 2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Feig DI, Kang DH and Johnson RJ: Uric acid
and cardiovascular risk. N Engl J Med. 359:1811–1821.
2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Nakamura K, Sakurai M, Miura K, Morikawa
Y, Yoshita K, Ishizaki M, Kido T, Naruse Y, Suwazono Y and Nakagawa
H: Alcohol intake and the risk of hyperuricemia: A 6-year
prospective study in Japanese men. Nutr Metab Cardiovasc Dis.
22:989–996. 2012.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Li Z, Guo X, Liu Y, Chang Y, Sun Y, Zhu G
and Abraham MR: The relation of moderate alcohol consumption to
hyperuricemia in a rural general population. Int J Environ Res
Public Health. 13(E732)2016.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Nakamura K, Okamura T, Hayakawa T, Hozawa
A, Kadowaki T, Murakami Y, Kita Y, Okayama A and Ueshima H: NIPPON
DATA90 Research Group: The proportion of individuals with
alcohol-induced hypertension among total hypertensives in a general
Japanese population: NIPPON DATA90. Hypertens Res. 30:663–668.
2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Okubo Y, Sairenchi T, Irie F, Yamagishi K,
Iso H, Watanabe H, Muto T, Tanaka K and Ota H: Association of
alcohol consumption with incident hypertension among middle-aged
and older Japanese population: The Ibaraki Prefectural Hearth Study
(IPHS). Hypertension. 63:41–47. 2014.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Oda N, Kajikawa M, Maruhashi T, Iwamoto Y,
Kishimoto S, Matsui S, Hidaka T, Kihara Y, Chayama K, Goto C, et
al: Endothelial function is impaired in relation to alcohol intake
even in the case of light alcohol consumption in Asian men:
Flow-mediated Dilation Japan (FMD-J) Study. Int J Cardiol.
230:523–528. 2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Research Committee for the Mega Database
of Japan Society of Ningen Dock, May 2019 : Nationwide data
analysis of the Ningen Dock in 2016 (Part 1) (In Japanese).
https://www.ningen-dock.jp/wp/wp-content/uploads/2013/09/2016dockdata-No1.pdf.
Accessed May 31, 2019.
|
|
32
|
Matsuzawa Y: Metabolic syndrome-definition
and diagnostic criteria in Japan. J Atheroscler Thromb.
12(301)2005.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Hamaguchi M, Kojima T, Itoh Y, Harano Y,
Fujii K, Nakajima T, Kato T, Takeda N, Okuda J, Ida K, et al: The
severity of ultrasonographic findings in nonalcoholic fatty liver
disease reflects the metabolic syndrome and visceral fat
accumulation. Am J Gastroenterol. 102:2708–2715. 2007.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Examination Committee of Criteria for
‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity:
New criteria for ‘obesity disease’ in Japan. Circ J 66: 987-992,
2002.
|
|
35
|
Levey AS, Coresh J, Balk E, Kausz AT,
Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J and Eknoyan G:
National Kidney Foundation: National Kidney Foundation practice
guidelines for chronic kidney disease: Evaluation, classification,
and stratification. Ann Intern Med. 139:137–147. 2003.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Kiechl S, Willeit J, Poewe W, Egger G,
Oberhollenzer F, Muggeo M and Bonora E: Insulin sensitivity and
regular alcohol consumption: Large, prospective, cross sectional
population study (Bruneck study). BMJ. 313:1040–1044.
1996.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Sierksma A, Patel H, Ouchi N, Kihara S,
Funahashi T, Heine RJ, Grobbee DE, Kluft C and Hendriks HF: Effect
of moderate alcohol consumption on adiponectin, tumor necrosis
factor-alpha, and insulin sensitivity. Diabetes Care. 27:184–189.
2004.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Pischon T, Girman CJ, Rifai N,
Hotamisligil GS and Rimm EB: Association between dietary factors
and plasma adiponectin concentration in men. Am J Clin Nutr.
81:780–786. 2005.PubMed/NCBI View Article : Google Scholar
|
|
39
|
You M, Considine RV, Leone TC, Kelly DP
and Crabb DW: Role of adiponectin in the protective action of
dietary saturated fat against alcoholic fatty liver in mice.
Hepatology. 42:568–577. 2005.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Rimm EB, Giovannucci EL, Willett WC,
Colditz GA, Ascherio A, Rosner B and Stampfer MJ: Prospective study
of alcohol consumption and risk of coronary disease in men. Lancet.
338:464–468. 1991.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rimm EB, Williams P, Fosher K, Criqui M
and Stampfer MJ: Moderate alcohol intake and lower risk of coronary
heart disease: Meta-analysis of effects on lipids and haemostatic
factors. BMJ. 319:1523–1528. 1999.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Mukamal KJ, Ding EL and Djoussé L: Alcohol
consumption, physical activity, and chronic disease risk factors: A
population-based cross-sectional survey. BMC Public Health.
6(118)2006.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Fillmore KM, Golding JM, Graves KL, Kniep
S, Leino EV, Romelsjö A, Shoemaker C, Ager CR, Allebeck P and
Ferrer HP: Alcohol consumption and mortality. I. Characteristics of
drinking groups. Addiction. 93:183–203. 1998.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Goude D, Fagerberg B and Hulthe J: AIR
Study Group: Alcohol consumption, the metabolic syndrome and
insulin resistance in 58-year-old clinically healthy men (AIR
study). Clin Sci (Lond). 102:345–352. 2002.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Yoon YS, Oh SW, Baik HW, Park HS and Kim
WY: Alcohol consumption and the metabolic syndrome in Korean
adults: The 1998 Korean National Health and Nutrition Examination
Survey. Am J Clin Nutr. 80:217–224. 2004.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Rehm J, Mathers C, Popova S,
Thavorncharoensap M, Teerawattananon Y and Patra J: Global burden
of disease and injury and economic cost attribute to alcohol use
and alcohol-use disorders. Lancet. 373:2223–2233. 2009.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Kawano Y: Physio-pathological effects of
alcohol on the cardiovascular system: Its role in hypertension and
cardiovascular disease. Hypertens Res. 33:181–191. 2010.PubMed/NCBI View Article : Google Scholar
|
|
48
|
VanWagner LB, Ning H, Allen NB, Ajmera V,
Lewis CE, Carr JJ, Lloyd-Jones DM, Terrault NA and Siddique J:
Alcohol use and cardiovascular disease risk in patients with
nonalcoholic fatty liver disease. Gastroenterology. 153:1260–1272.
2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Yeboah J, McClelland RL, Polonsky TS,
Burke GL, Sibley CT, O'Leary D, Carr JJ, Goff DC, Greenland P and
Herrington DM: Comparison of novel risk markers for improvement in
cardiovascular risk assessment in intermediate-risk individuals.
JAMA. 308:788–795. 2012.PubMed/NCBI View Article : Google Scholar
|