Introduction
Colorectal cancer (CRC) is the third type of cancer
that is commonly diagnosed in both men and women (1). Diet and life-style choices play a
significant role in the development and prognosis of colon cancer
(2). Colon cancer is a condition
which is medically complex (1). This
heterogeneity makes it difficult to assess which patients will most
benefit from adjuvant therapy and hinders the development of new
targeted agents. It is therefore important to gain more insight
into the biological diversity of colon cancers, particularly with
regard to clinical characteristics (3). Vitamin D is not really a vitamin but
the precursor to the potent calcitriol steroid hormone that has
widespread body-wide actions (4).
Calcitriol controls various cellular pathways that can be used to
assess the incidence and prognosis of cancer. Epidemiological
studies have found a correlation between low serum levels of
vitamin D with increased risk of colon cancer as well as
inflammatory diseases including inflammatory bowel disease
(4).
An individual's vitamin D status also depends on
both diet and lifestyle. Garland and Garland (5) first proposed the correlation between
vitamin D and colon cancer, finding that populations residing in
the northeastern US had an increased incidence of colon
cancer-related mortality relative to those residing in the southern
US (6). Since then, sufficient
levels of serum vitamin D have been associated with a lower
incidence of colon cancer and lower mortality in patients with
colon cancer (7). Adequate levels of
serum vitamin D were also found to be associated with a lower risk
of developing inflammatory diseases such as Crohn's disease, a
colon cancer risk factor (8). Across
different mouse models, vitamin D was found to have a protective
effect against colon cancer (9).
Yet, there is currently no awareness of the protective effect of
vitamin D on inflammatory colon cancer. A previous study reported
that a daily intake of 1,000 IU of vitamin D reduces the risk of
CRC (10).
Non-steroidal anti-inflammatory drugs (NSAIDs)
minimize colon cancer incidence and reduce mortality in patients
with colon cancer (11). NSAIDs are
a very important class of drugs with several therapeutic
applications in the treatment of osteoarthritis, some tumors and
rheumatoid arthritis (12).
Among the various NSAIDs, indomethacin a standard
cyclooxygenase (COX)-1 and -2 antagonist commonly used in the
clinic for its potent anti-inflammatory and analgesic properties,
has been shown to exert anti-CRC effects and is used to treat many
solid and hematological malignancies in humans (13). Nonetheless, the body of evidence that
indomethacin has anti-neoplastic efficacy in animal and in humans
is one of the strongest among the numerous NSAIDs (14,15).
Platelet-derived growth factor (PDGF) is a
multifunctional polypeptide growth factor with significant
biological effects ranging from mitogenic activity for mesenchymal
cells to control of matrix metabolism, chemotactic and vasoactive
properties, and regulation of immune or inflammatory reactions
(16). PDGF plays an important role
in several solid tumors. PDGF is a key target in cancer therapy, as
it is mainly involved in cell migration and proliferation of
stromal cells in cancers (16). PDGF
encourages the development of new blood vessels that are necessary
for tumor growth and metastasis (17).
The aim of the present study was to assess the
protective role of the combined treatment of vitamin D and
indomethacin in a 1,2-dimethylhydrazine (1,2-DMH)-induced CRC model
in animals, and also to evaluate the combination of vitamin D and
indomethacin for the treatment of CRC in animals. Finally, the
study aimed to determine the effect of the combined treatment of
vitamin D and indomethacin on the carcinoembryonic antigen (CEA)
and PDGF expression in CRC.
Materials and methods
Chemicals
1,2-DMH, indomethacin, vitamin D and 5-flurouracil
(5-FU) were obtained from Sigma Aldrich Co. (Merck KGaA). Certain
chemicals used, such as NaCl, EDTA and Tris buffer were purchased
from a local commercial source.
Treatment protocol and sampling
Male Albino rats (n=50) (5 weeks old, 150 g body
weight) were obtained from the Faculty of Medicine's animal house
at Assiut University (Assiut, Egypt). Animals were housed under
controlled environmental conditions (22±2˚C temperature, 50±5%
humidity, 12/12 h light/dark cycle) and had free access to a
typical grain diet and tap water. The research procedures were
carried out in compliance with the National Institute of Health
Guidelines for Animal Care (https://grants.nih.gov/grants/olaw/guide-for-the-care-and-use-of-laboratory-animals.pdf)
and approved (no. PHAB1827) by the Ethics Committee of the Faculty
of Pharmacy, Assiut University (Assiut, Egypt).
The rats were divided into five groups, with 10 rats
in each. i) The control group received 0.9% normal saline daily
during the experimental period. ii) The carcinogenic group (DMH)
was injected subcutaneously with 20 mg/kg of 1,2-DMH once a week
for 10 weeks as previously described (18) and rats were left to complete 18
weeks. iii) The prophylactic group was treated twice weekly with
vitamin D [1,000 IU (25 µg)/rat/p.o.] as previously described
(19) and daily indomethacin (2
mg/kg/p.o.) (18) for 4 weeks before
1,2-DMH injection and during the induction period for 10 weeks (14
weeks of prophylactic regimen) and rats were left to complete 18
weeks. iv) The combined treatment group was administrated
subcutaneously with 1,2-DMH once weekly for 10 weeks, and then
treated with vitamin D (1,000 IU (25 µg)/rat/p.o.) (19) and daily indomethacin (2 mg/kg/p.o.)
as previously described (20) for 8
weeks (18 weeks for treatment regimen). v) The 5-fluorouracil
(5-FU) treatment group was injected subcutaneously with 1,2-DMH
once weekly for 10 weeks, and then treated with 5-FU (100
mg/kg/i.p.) as previously described (21) once weekly for 4 weeks (14 weeks for
treatment regimen) and rats were left to complete 18 weeks.
The euthanasia of rats was carried out by ether.
Ether anesthesia was induced in a glass jar containing a cotton
wool pad soaked in anesthetic ether 30%. Each rat was removed for
orbital puncture when lightly anesthetized. The average time for
anesthesia was 4.7 min. The average volume of ether was 6.5 ml/h
(22).
Blood samples were obtained and colons were rapidly
excreted and used for RNA preparation or homogenization in 20 mM
Tris, 100 mM NaCl, 1 mM EDTA and 0.5% Triton X-100 buffer. Colon
homogenate protein content was calculated using Bradford reagent
and bovine serum albumin (BSA) as standard. The mixture of protease
inhibitors was added. Samples were aliquoted and stored at -80˚C
until use.
Sodium dodecyl sulfate-polyacrylamide
gel electrophoresis (SDS-PAGE) and western blotting
Protein concentration was determined per gram
tissue, and 1 µl of 10% tissue homogenate was added to 200 µl of
Bradford reagent. The absorbance was read at 595 nm. Loading buffer
[Tris HCL, sodium dodecyl sulfate (SDS), glycerol, bromophenol blue
and β-mercaptoethanol] was boiled with 50 µg tissue homogenate. All
proteins became negatively charged and disulphide bridges in
proteins were reduced. Using 12% polyacrylamide gel for
electrophoresis, polyacrylamide gels were formed from the
polymerization of two compounds, acrylamide and
N,N-methylenebisacrylamide. Electrophoresis chamber (OWL.
Separation Systems, Inc.; Ser. no: 128460) was filled with 1X
running buffer and samples were loaded. Proteins were transferred
from gel to nitrocellulose membrane. SDS-PAGE was carried out at
100 V for 2 h. using the T-77 ECL semidry transfer unit (Amersham
Biosciences; Ser. no. 20145681) for 2 h, and the electro-transfer
was completed. The membrane was blocked for 1 h in 5% milk solution
(5 g per 100 ml of TBST buffer). The primary antibodies: rabbit
polyclonal anti-CEA (Santa Cruz Biotechnology, Inc.; cat. no.
sc-59875), anti-PDGF (Santa Cruz Biotechnology, Inc.; cat. no.
sc-365805) and β-actin were used at 1:200 dilutions. The membrane
was incubated with the primary antibodies for 1 h at room
temperature with constant agitation. Peroxidase labeled anti-rabbit
antibody (secondary antibody) was acquired from Amersham™ (GE
Healthcare) (cat. no. NIF824) and was used at a dilution 1:3,000
and incubated with the membrane for 2 h. Detection kit (ECL-Plus)
was obtained from Amersham™ Company (cat no. RPN2108). They were
incubated for 5 min at room temperature in the dark. The entire
membrane was covered by detection solution. Image J (Image J 2x.8)
(National Institutes of Health, Bethesda, MD, USA) was used to
calculate peak size.
Determination of tissue caspase-3
activity
Caspase-3 proteolytic activity was calculated using
a calorimetric assay kit (Caspase-3/CPP32, ApoTarget, Colorimetric
Protease Assay kit; Biosource Int.). Determination of caspase-3
proteolytic activity was carried out using a modified procedure as
previously described (23).
Cytosolic extracts were prepared by homogenization of the colon
tissue (50 mg) in lysis buffer. Subsequently, the homogenates were
centrifuged at 10,000 x g for 10 min. An amount of 50 µl of
reaction buffer was added to 50 µl of each sample. A maximum of 10
µl of DEVD-pNA substrates was applied to the tubes and incubated at
37˚C for 1 h. Samples were read at 405 nm using Shimadzu
Spectrophotometer, UV, 1201. Results are expressed as means ± SEM
of three separate trials (triplicate).
Determination of oxidative stress
biomarkers
Lipid peroxidation determination is dependent on the
formation of malondialdehyde (MDA) that reacts with thiobarbituric
acid to produce a colored material. The latter can be
calorimetrically calculated. Lipid peroxide levels in the tissues
were assessed as previously described (23). The results are expressed as means ±
SEM of three separate trials.
Nitric oxide (NO) levels in the tissues were
measured using a previously described method (24). Data are expressed as means ± SEM of
three separate experiments.
Tissue total antioxidant levels were estimated by
total antioxidant capacity assay Kit T-AOC (cat. no. ab65329;
Abcam). The data are expressed as means ± SEM of three separate
trials. This ELISA kit uses Sandwich-ELISA as the method. An amount
of 40 µl of sample dilution buffer was mixed with 10 µl of sample
and incubated for 30 min at 37˚C. Then the wash solution was
aspirated and refilled and discarded after resting for 30 sec. The
washing procedure was repeated 5 times. Horseradish peroxidase
(HRP)-conjugated reagent (50 µl) was added to each well except the
blank control well and incubated for 30 min at 37˚C. The washing
procedure was repeated 5 times. Chromogen solution A (50 µl) and
chromogen solution B (50 µl) were added to each well and mixed with
gentle shaking and incubated at 37˚C for 15 min. Stop solution (50
µl) was added to each well to terminate the reaction. The samples
were read at 450 nm using a microtiter plate reader.
Histopathological examinations
The colons were dissected and washed with 0.9%
sterile saline solution. Each colon was cut into small pieces and
kept in neutral buffer formalin. Formalin-fixed colon samples were
moved to 70% ethanol and coated in paraffin. Tissue sections were
treated at room temperature for 15 min with hematoxylin and eosin
(H&E) and tested for pathological changes under an optical
microscope.
Statistical analysis of the data
Data analysis was carried out using Graphpad Instat
version 3 (GraphPad Software, Inc.). The results are expressed as
mean ± SD and P<0.05 was assigned as indicative of a statistical
significant difference. Multiple comparisons were performed using
one-way ANOVA approach followed by Tukey as a multiple comparison
post hoc ANOVA test.
Results
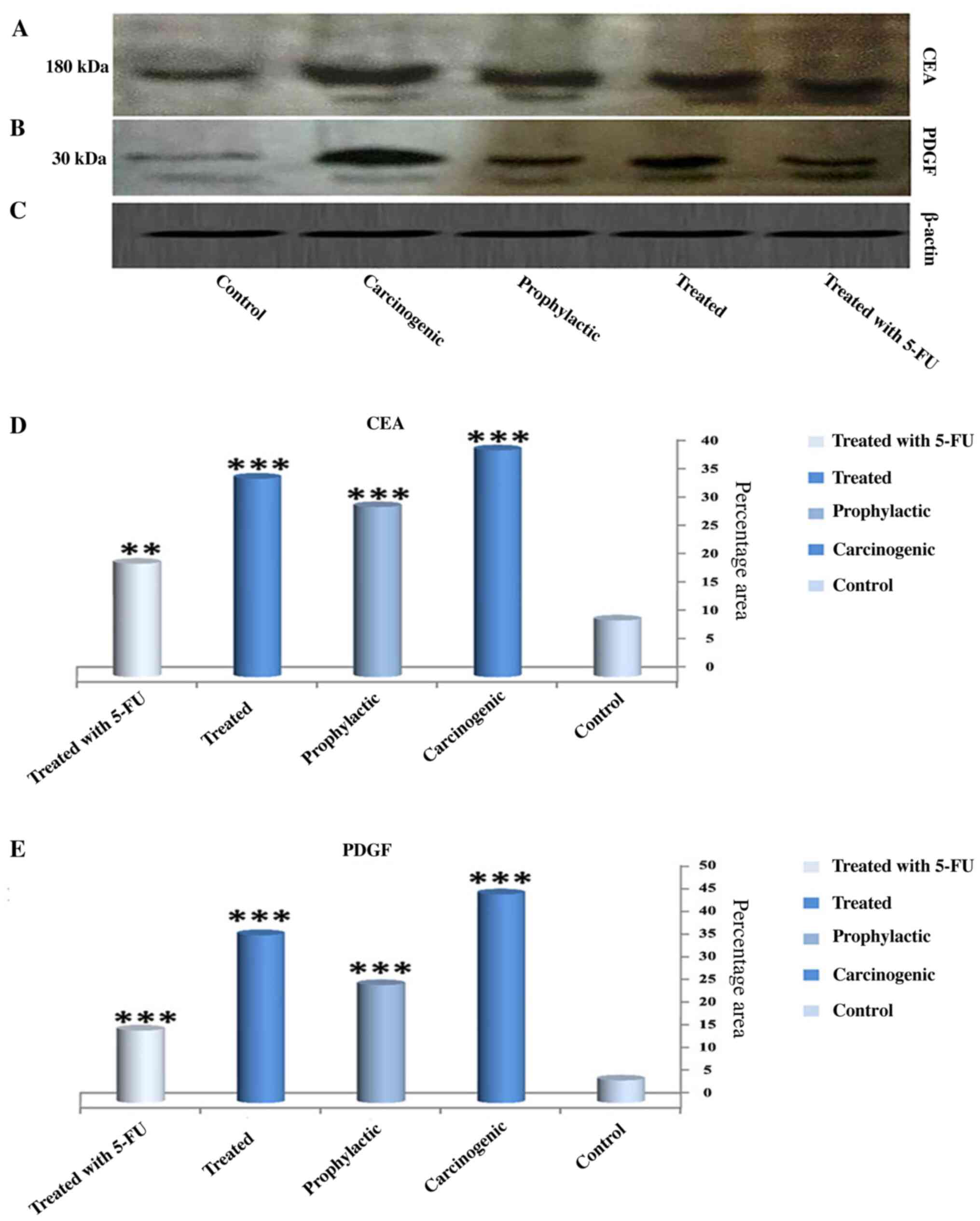
Expression of CEA and PDGF
Fig. 1A-C shows the
expression of CEA and PDGF protein by western blot analysis in all
experimental stages. A significant increase in CEA expression in
the carcinogenic group (40%) (Fig. A
and D) was noted when compared with
the control group (10%). In contrast, the expression level was
significantly decreased in the 5-FU group when compared with the
carcinogenic group and the expression level was decreased but with
a lower degree in both the prophylactic and vitamin D +
indomethacin (Treated) groups. Furthermore, the expression of PDG
(Fig. 1A and E) in the carcinogenic group reached a
maximum peak while its expression was significantly reduced in the
other groups (5-FU, prophylactic and vitamin D + indomethacin
(Treated) groups).
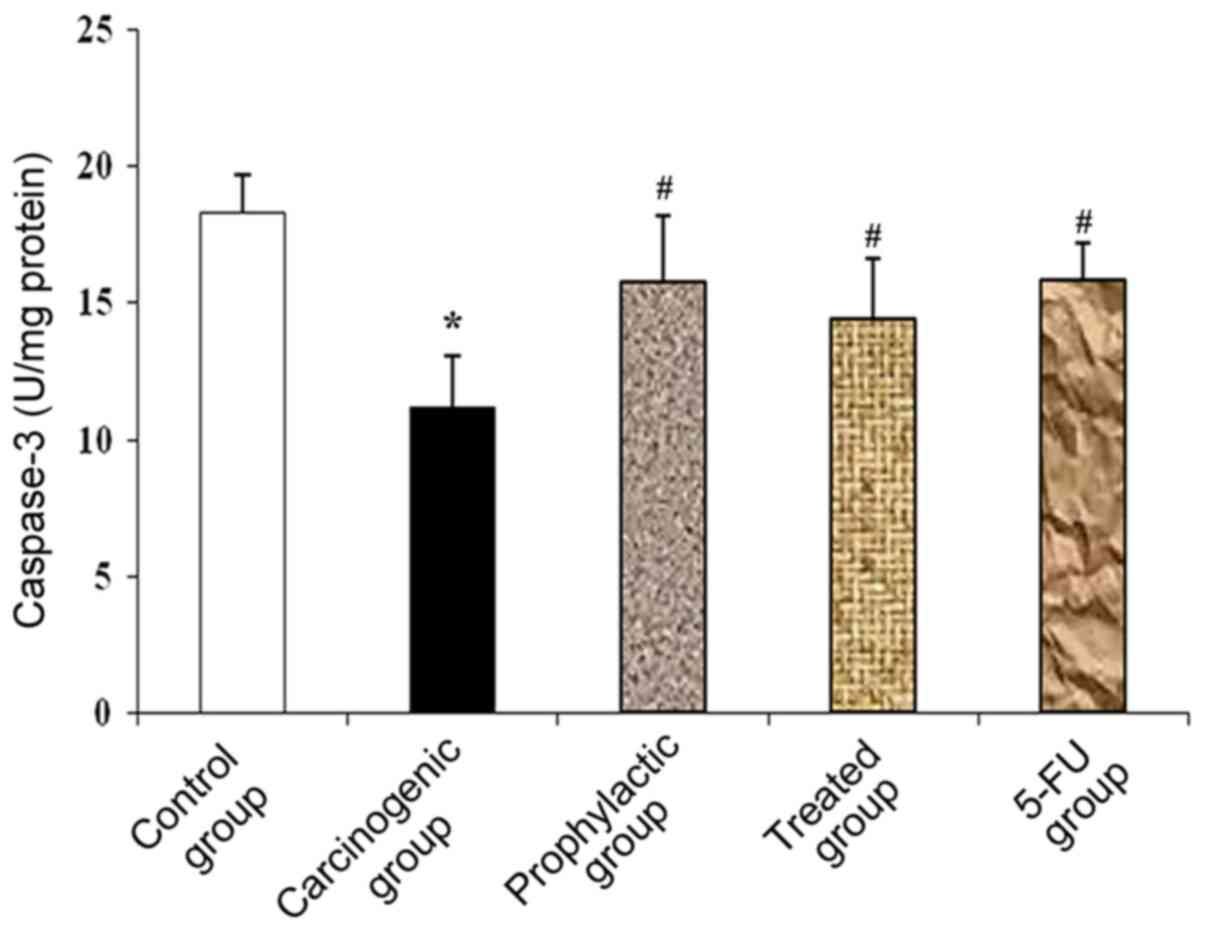
Tissue caspase-3 activity
In the carcinogenic group, there was a significant
decrease in caspase-3 levels compared to the control group. This
significant reduction was reversed as an increase in caspase-3
levels was noted in the prophylactic group, vitamin D +
indomethacin (Treated group) and 5-FU group when compared with the
carcinogenic group (Fig. 2).
Oxidative stress levels
Table I summarizes
the oxidative stress levels in the different groups. The
carcinogenic group exhibited a significant increase in both NO and
MDA levels when compared to the control group. The prophylactic,
vitamin D + indomethacin and 5-FU groups, on the other hand,
exhibited significantly reduced levels of oxidative stress induced
by NO and MDA.
 | Table IEffects of Vitamin D and indomethacin
combination on NO, MDA and total antioxidants. |
Table I
Effects of Vitamin D and indomethacin
combination on NO, MDA and total antioxidants.
| Biochemical
indices | Control | Carcinogenic | Prophylactic | Vitamin D +
indomethacin | 5-FU |
|---|
| NO (µM/g wet
tissue) | 28.89±3.07 |
69.24±4.95a |
45.11±3.10b |
51.08±3.29b |
42.88±4.91b |
| MDA (µM/g wet
tissue) | 1.65±0.95 |
6.22±0.58a |
3.01±1.04b |
3.71±0.642b |
3.48±0.92b |
| TAC (U/mg
protein) | 29.94±4.54 |
12.13±2.66a |
23.87±3.1b |
19.77±2.84b |
21.98±3.30b |
Furthermore, total antioxidant capacity (TAC) was
significantly reduced in the carcinogenic group when compared with
the control group, while the prophylactic, vitamin D + indomethacin
and 5-FU groups exhibited significantly increased TAC when compared
with the carcinogenic group (Table
I).
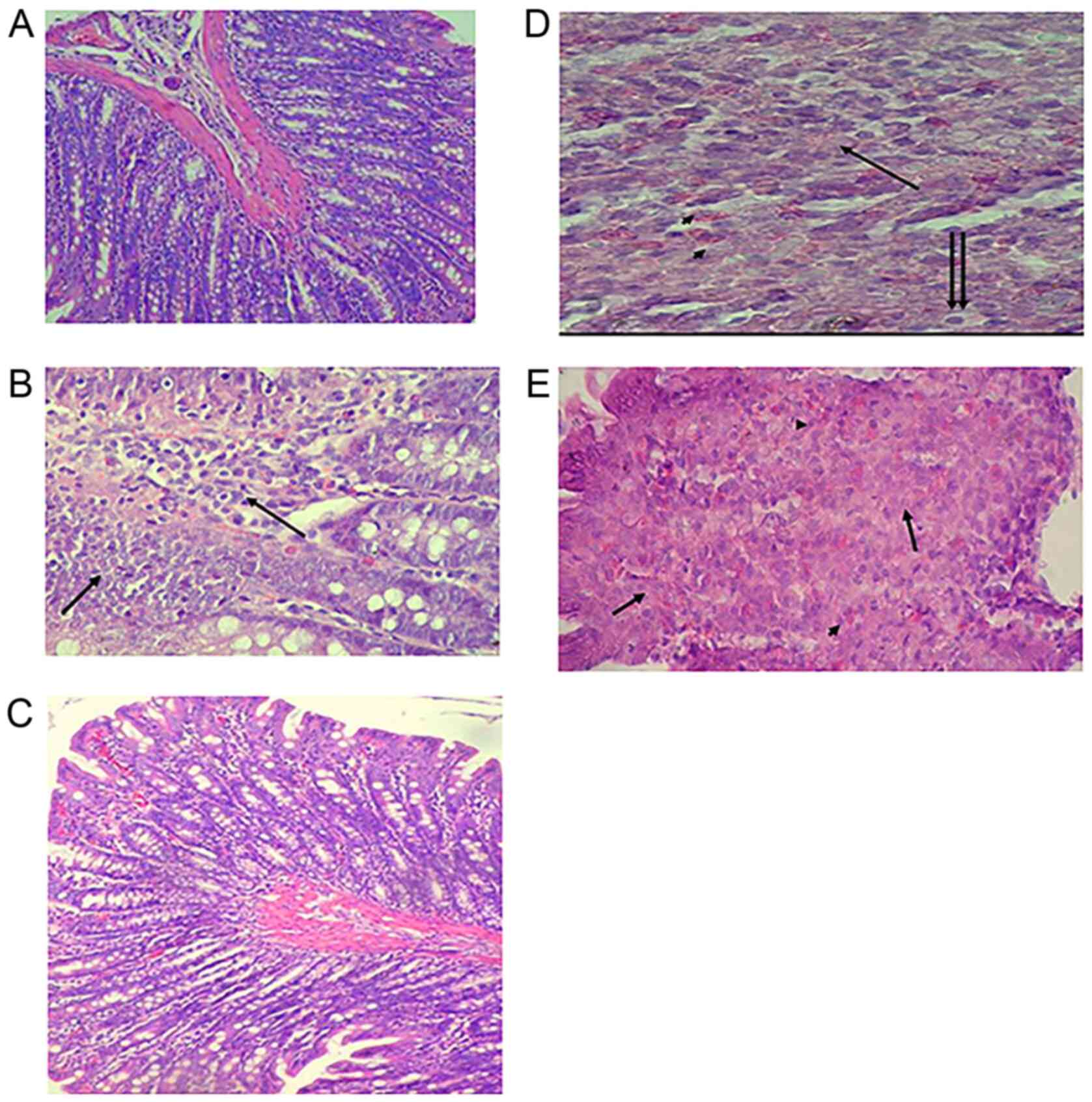
Histopathological results
To assess the changes in colon cells after DMH,
vitamin D + indomethacin and 5-FU administration, H&E-stained
slides were examined. Colon section from the rats in the control
group shows normal histological structure (Fig. 3A). On the other hand, the
carcinogenic group demonstrated proliferation of tumor cells from
the epithelial layer infiltrating the submucosa. The tumor cells
(arrows) are polyhedral cells with hyperchromatic nuclei (Fig. 3B). The prophylactic group showed more
or less normal histological appearance (Fig. 3C). Furthermore, the vitamin D +
indomethacin group showed infiltrating tumor cells undergoing
either necrosis (arrow) or apoptosis (double arrows) with
infiltration of mast cells (arrow heads) (Fig. 3D). Finally, the 5-FU group showed
colon adenocarcinoma with tumor cell necrosis (arrows) and heavy
infiltration with mast cells (arrow heads) (Fig. 3E).
Discussion
The anticancer activity of indomethacin, a standard
cyclooxygenase (COX)-1 and -2 antagonist commonly used in the
clinic for its potent anti-inflammatory and analgesic properties,
has been described both in vitro as well as in vivo
(25). Several experimental and
clinical studies have reported that the pathways involved in the
therapeutic effects of indomethacin and vitamin D in colon cancer
are still limited (26). The present
study found that combined treatment of vitamin D and indomethacin
was associated with a lower risk of colon cancer in a rat model. In
addition, the results showed that the combination of indomethacin
and vitamin D had anti-colon cancer effect.
Our findings concerning the antitumor activity of
vitamin D are agreed with those of Feldman et al (27), who stated that calcitriol controls a
variety of cellular pathways that may have a role to play in
evaluating cancer risk and prognosis. It is also proposed that
vitamin D deficiency raises the risk of developing cancer and that
reducing the shortage and adding supplementation of vitamin D could
be an inexpensive, effective and safe way to reduce cancer
incidence and improve cancer prognosis and outcome.
Colon receptors contain vitamin D receptors and
vitamin D binds to these receptors. This may prevent the growth of
oncogenes and may prevent the spread of cancer cells to other parts
of the body. It is therefore believed that vitamin D can help
protect against colorectal cancer (CRC) by reducing the likelihood
that cancer cells can develop and spread (10).
Correlations between high vitamin D levels and the
reduced risk and progression of CRC are still being investigated
and more studies are needed (28).
This is in agreement with the results of the present study. We
hypothesized that the anticancer activity of indomethacin and
vitamin D may involve enhancement of apoptotic markers and the
reduction of oxidative stress markers.
CEA is a well-known soluble tumor marker and an
onco-fetal glycoprotein. Although its existence is primarily
confined to the large intestine in healthy tissues, it is
overexpressed in most gastrointestinal malignancies, breast cancer,
thyroid cancer and lung cancer (29). The present study proposed that there
are various colon cancer markers such as CEA and PDGF. Thus, in the
present study, both CEA and PDGF expression levels were increased
in the carcinogenic group due to inflammation or cancer progression
in the CRC tissues, while their levels were reduced during
treatment with indomethacin and vitamin D. Such results indicate
that indomethacin and vitamin D combination therapy decreases the
severity of inflammation and colon cancer.
Pan et al (30) indicated that PDGF is known to
encourage the development of new blood vessels that are essential
to the growth and metastasis of tumors. PDGF in portal vein blood
tumor drainage may be useful predictive factors for CRC synchronous
liver metastasis. Such results are confirmed by our findings which
demonstrated increased PDGF in the development of inflammation and
cancer. PDGF is currently reported as a major inflammatory growth
factor following acute and chronic tissue injury playing a central
role in the repair process (25).
In this research, indomethacin and vitamin D are
associated with biochemical and morphological changes, including
apoptosis enhancement and oxidative stress reduction. Thus, the
activity of caspase-3 was estimated to demonstrate the possible
mechanisms of indomethacin and vitamin D-mediated anti-inflammatory
and/or antitumor effect.
The present study reported that the determination of
caspase-3 activity has revealed that during inflammation and
progression of cancer stage, levels of caspase-3 are markedly
decreased. On the other hand, its levels were increased in the
indomethacin and vitamin D treatment group. These results are in
harmony with the results reported by Jung et al (31), Okda et al (32) and Katary et al (33). The authors showed that caspase-3,
which is a pro-apoptotic protein, was increased after the damage of
hepatocellular carcinoma which occurred by CCl4, while its level
was decreased due to the partial repairing occurred.
In the present study, we observed increased serum NO
and MDA levels in the carcinogenic group and decreased levels in
the indomethacin + vitamin D and 5-FU treatment groups by reducing
oxidative stress markers. Decreased levels of oxidative stress
factors were observed in the prophylactic and treated groups. There
was a statistically significant increase in the total oxidative
stress markers (NO and MDA) in colon tissues of the carcinogenic
group compared to the control group. Histopathological examinations
were performed. The results of the histopathological examinations
confirmed that there was marked improvement in colon cells in the
prophylactic and treatment groups. Unfortunately, the present study
had a histopathological limitation because the weight and numbers
of tumors were not calculated.
In conclusion, in the present study, the use of
vitamin D and indomethacin significantly reduced colon cancer
incidence. Vitamin D is one of natural antioxidant which reduces
oxidative stress markers and inflammation. Biochemical and
molecular research associated with the administration of vitamin D
and indomethacin shows that it has the ability to reduce the
occurrence of colon carcinomas. This combination eliminates toxic
side effects of chemotherapy and decreases colon cancer
incidence.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TMO and MMAA conceived the research concept,
experiment design and methodology. MMAA and MAK carried out the
animal modeling and animal handling. TMO performed the western blot
analysis. TMO, MK and MMAA analyzed and interpreted the results.
SKAE performed the histological examination and analysis of the
colon sections. TMO and SKAE drafted the manuscript. MMAA was a
major contributor in editing and writing the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The research procedures were performed in compliance
with the National Institute for Animal Care Health Guidelines and
approved by the Faculty of Pharmacy's Ethics Committee, Assiut
University (Assiut, Egypt).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung JJY, Chiu HM, Jung KW, Jun JK,
Sekiguchi M, Matsuda T and Kyaw MH: Increasing trend in young-onset
colorectal cancer in Asia: more cancers in men and more rectal
cancers. Am J Gastroenterol. 114:322–329. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Lofano K, Principi M, Scavo MP, Pricci M,
Ierardi E and Di Leo A: Dietary lifestyle and colorectal cancer
onset, recurrence, and survival: Myth or reality? J Gastrointest
Cancer. 44:1–11. 2013.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wolpin BM and Mayer RJ: Systemic treatment
of colorectal cancer. Gastroenterology. 134:1296–1310.
2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Meeker S, Seamons A, Paik J, Treuting PM,
Brabb T, Grady WM and Maggio-Price L: Increased dietary vitamin D
suppresses MAPK signaling, colitis, and colon cancer. Cancer Res.
74:4398–4408. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Garland CF and Garland FC: Do sunlight and
vitamin D reduce the likelihood of colon cancer? Int J Epidemiol.
9:227–231. 1980.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Deeb KK, Trump DL and Johnson CS: Vitamin
D signalling pathways in cancer: Potential for anticancer
therapeutics. Nat Rev Cancer. 7:684–700. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
7
|
Ng K, Meyerhardt JA, Wu K, Feskanich D,
Hollis BW, Giovannucci EL and Fuchs CS: Circulating
25-hydroxyvitamin D levels and survival in patients with colorectal
cancer. J Clin Oncol. 26:2984–2991. 2008.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ananthakrishnan AN, Khalili H, Higuchi LM,
Bao Y, Korzenik JR, Giovannucci EL, Richter JM, Fuchs CS and Chan
AT: Higher predicted vitamin D status is associated with reduced
risk of Crohn's disease. Gastroenterology. 142:482–489.
2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Fichera A, Little N, Dougherty U, Mustafi
R, Cerda S, Li YC, Delgado J, Arora A, Campbell LK, Joseph L, et
al: A vitamin D analogue inhibits colonic carcinogenesis in the
AOM/DSS model. J Surg Res. 142:239–245. 2007.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Gorham ED, Garland CF, Garland FC, Grant
WB, Mohr SB, Lipkin M, Newmark HL, Giovannucci E, Wei M and Holick
MF: Optimal vitamin D status for colorectal cancer prevention: A
quantitative meta analysis. Am J Prev Med. 32:210–216.
2007.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rayyan Y, Williams J and Rigas B: The role
of NSAIDs in the prevention of colon cancer. Cancer Invest.
20:1002–1011. 2002.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Rao P and Knaus EE: Evolution of
nonsteroidal anti-inflammatory drugs (NSAIDs): Cyclooxygenase (COX)
inhibition and beyond. J Pharm Pharm Sci. 11:81s–110s.
2008.PubMed/NCBI View
Article : Google Scholar
|
|
13
|
Woo JK, Kang JH, Jang YS, Ro S, Cho JM,
Kim HM, Lee SJ and Oh SH: Evaluation of preventive and therapeutic
activity of novel non-steroidal anti-inflammatory drug, CG100649,
in colon cancer: Increased expression of TNF-related
apoptosis-inducing ligand receptors enhance the apoptotic response
to combination treatment with TRAIL. Oncol Rep. 33:1947–1955.
2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Vane JR and Botting RM: Mechanism of
action of anti-inflammatory drugs. Adv Exp Med Biol. 433:131–138.
1997.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lai SW and Liao KF: Aspirin use after
diagnosis improves survival in older adults with colon cancer. J Am
Geriatr Soc. 61:843–844. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Peyre M, Salaud C, Clermont-Taranchon E,
Niwa-Kawakita M, Goutagny S, Mawrin C, Giovannini M and Kalamarides
M: PDGF activation in PGDS-positive arachnoid cells induces
meningioma formation in mice promoting tumor progression in
combination with Nf2 and Cdkn2ab loss. Oncotarget. 6:32713–32722.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zhou J, Tang ZY, Fan J, Wu ZQ, Li XM, Liu
YK, Liu F, Sun HC and Ye SL: Expression of platelet-derived
endothelial cell growth factor and vascular endothelial growth
factor in hepatocellular carcinoma and portal vein tumor thrombus.
J Cancer Res Clin Oncol. 126:57–61. 2000.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Sumiyoshi H and Wargovich MJ:
Chemoprevention of 1,2-dimethylhydrazine-induced colon cancer in
mice by naturally occurring organosulfur compounds. Cancer Res.
50:5084–5087. 1990.PubMed/NCBI
|
|
19
|
Lappe JM, Travers-Gustafson D, Davies KM,
Recker RR and Heaney RP: Vitamin D and calcium supplementation
reduces cancer risk: Results of a randomized trial. Am J Clin Nutr.
85:1586–1591. 2007.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Quidville V, Segond N, Pidoux E, Cohen R,
Jullienne A and Lausson S: Tumor growth inhibition by indomethacin
in a mouse model of human medullary thyroid cancer: Implication of
cyclooxygenases and 15-hydroxyprostaglandin dehydrogenase.
Endocrinology. 145:2561–2571. 2004.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gupta S, Khan H, Barik S and Negi MP:
Clinical benefits of concurrent capecitabine and cisplatin versus
concurrent cisplatin and 5-flurouracil in locally advanced squamous
cell head and neck cancer. Drug Discov Ther. 7:36–42.
2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Miranda EG, Nascimento VP, Waisberg DR,
Sousa MW, Lima MF, Silva DS and Waisberg J: Inhalation anesthesia
equipment for rats with provision of simultaneous anesthetic and
oxygen. Acta Cir Bras. 26:140–143. 2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Buege JA and Aust SD: Microsomal lipid
peroxidation. Methods Enzymol. 52:302–310. 1978.PubMed/NCBI View Article : Google Scholar
|
|
24
|
van Bezooijen RL, Que I, Ederveen AG,
Kloosterboer HJ, Papapoulos SE and Löwik CW: Plasma nitrate+nitrite
levels are regulated by ovarian steroids but do not correlate with
trabecular bone mineral density in rats. J Endocrinol. 159:27–34.
1998.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Martin P and Nunan R: Cellular and
molecular mechanisms of repair in acute and chronic wound healing.
Br J Dermatol. 173:370–378. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Hull MA, Gardner SH and Hawcroft G:
Activity of the non-steroidal anti-inflammatory drug indomethacin
against colorectal cancer. Cancer Treat Rev. 29:309–320.
2003.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Feldman D, Krishnan AV, Swami S,
Giovannucci E and Feldman BJ: The role of vitamin D in reducing
cancer risk and progression. Nat Rev Cancer. 14:342–357.
2014.PubMed/NCBI View
Article : Google Scholar
|
|
28
|
Welsh J: Cellular and molecular effects of
vitamin D on carcinogenesis. Arch Biochem Biophys. 523:107–114.
2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Ojima T, Iwahashi M, Nakamura M, Matsuda
K, Nakamori M, Ueda K, Naka T, Ishida K, Primus FJ and Yamaue H:
Successful cancer vaccine therapy for carcinoembryonic antigen
(CEA)-expressing colon cancer using genetically modified dendritic
cells that express CEA and T helper-type 1 cytokines in CEA
transgenic mice. Int J Cancer. 120:585–593. 2007.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Pan HD, Peng YF, Xiao G and Gu J: High
levels of serum platelet-derived growth factor-AA and human
epidermal growth factor receptor-2 are predictors of colorectal
cancer liver metastasis. World J Gastroenterol. 23:1233–1240.
2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Jung MY, Kang HJ and Moon A:
Capsaicin-induced apoptosis in SK-Hep-1 hepatocarcinoma cells
involves Bcl-2 downregulation and caspase-3 activation. Cancer
Lett. 165:139–145. 2001.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Okda TM, Abd-Alhaseeb MM, Barka K and
Ragab NM: Ginger potentiates the effects of silymarin on liver
fibrosis induced by CCL4: The role of galectin-8. Eur Rev Med
Pharmacol Sci. 23:885–891. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Katary MA, Abdelsayed R, Alhashim A,
Abdelhasib M and Elmarakby AA: Salvianolic acid B slows the
progression of breast cancer cell growth via enhancement of
apoptosis and reduction of oxidative stress, inflammation, and
angiogenesis. Int J Mol Sci. 20(5653)2019.PubMed/NCBI View Article : Google Scholar
|