1. Introduction
COVID-19 is a disease caused by the severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first
documented in Wuhan, China. This disease has similarities with
viral pneumonia and symptoms similar to those of SARS-CoV and
MERS-CoV. A total of 3-6 days after infection, upper or lower
respiratory tract symptoms, fever and diarrhea, or a combination of
these, appear (1). Kang et
al (2) reported that 45.8% of
COVID-19 patients not only have respiratory symptoms, but also
gastrointestinal (GI) symptoms, such as lack of appetite, diarrhea,
vomiting and abdominal pain. OF 9,696 patients, 988 were reported
to exhibit nausea and vomiting. Meanwhile, loss of appetite and
abdominal pain were reported in 20 and 27 studies, respectively.
Loss of appetite and other GI symptoms have also been found in
other cases, for example in the UK (3). In cases of reinfection with the
SARS-CoV-2 variant B.1.1.7, the symptoms and duration were similar;
however, reinfection was rare (4).
Patients with GI tract symptoms have been reported
to feel pain for a longer period of time than those without GI
tract symptoms. These patients also have higher mean liver enzyme
levels, lower monocyte counts, longer prothrombin times and require
additional antimicrobial treatment (5). Intestinal dysfunction results in
changes in intestinal microbes and increases the levels of
inflammatory cytokines (5). There
are several means by which SARS-CoV-2 can damage the GI tract.
First, the virus can damage the GI tract via an inflammatory
response. Second, it directly damages the intestinal mucosa and
causes disturbances in the GI system. Third, it can induce changes
in the composition of the intestinal flora, causing digestive
disorders. The modification in the composition of intestinal flora
causes respiratory disorders through the ‘gut-lung axis’ (6).
In patients with comorbidities, the immune system is
affected, and the severity of COVID-19 infection worsens. One
common comorbidity in children and adults is obesity, which can
compromise the function of several organs and biological systems
due to excessive adipose tissue, a deficit in lean mass, insulin
resistance, dyslipidemia, hypertension, high levels of
pro-inflammatory cytokines and low levels of essential nutrients.
Furthermore, obesity is not only associated with the immune,
respiratory, cardiovascular and urinary systems, but can also
modify the gut microbiota (dysbiosis) (7,8). Obese
patients also have longer hospitalization periods, and have higher
levels of C-reactive protein and lower lymphocyte counts, which are
considered as early indicators of a more severe COVID-19 infection
course (9). Another factor that can
worsen COVID-19 infection is diabetes, which was shown by the high
percentage of ICU admissions among diabetics and a longer
hospitalization period, although diabetes was not associated with
mortality (10). It was shown that
the most common symptoms of COVID-19 patients with diabetes were
fever, dry cough, and fatigue (11). Li et al (12) reported that COVID-19 infection
caused ketosis or ketoacidosis and induced diabetic ketoacidosis in
diabetic patients, which prolonged hospitalization and increased
mortality (12).
Infection with COVID-19 might affect the microbiome
profile, which is associated with the abundance of some microbiome
phylum. Khan et al (13)
reported that several phyla related to COVID-19 infection included
Firmicutes, Bacteroidetes, Proteobacteria and
Actinobacteria, which are also associated with the severity
of COVID-19 infection. The correlation between the gut microbiome
and COVID-19 infection is interesting. In this review, the link
between COVID-19 and the gut microbiome, as well as its potential
clinical application in the future is discussed.
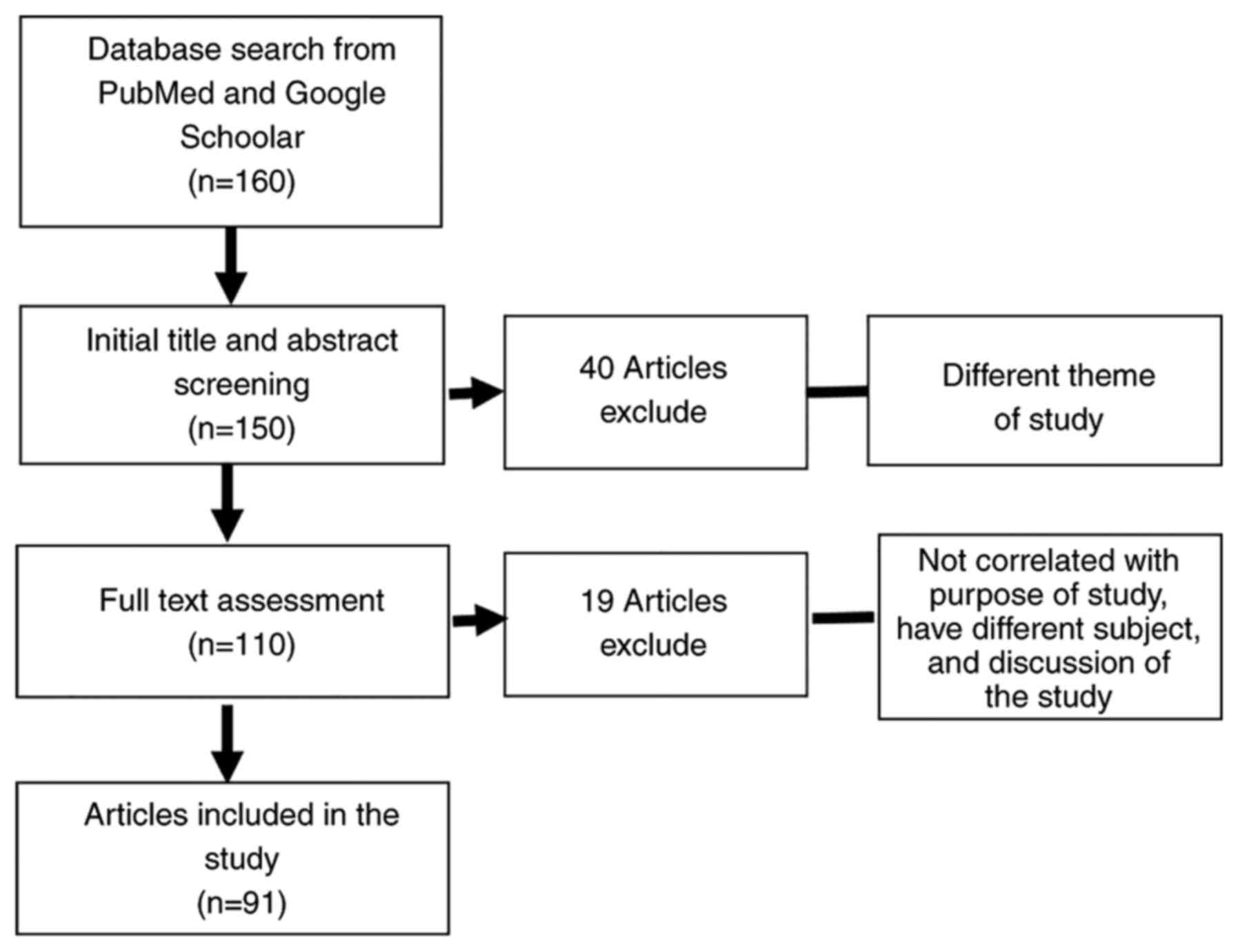
2. Literature search
A total of 160 articles from PubMed and Google
Scholar were initially obtained; 40 articles were excluded as they
did not match the research theme. The key words relevant for this
review were: ‘gut microbiota COVID-19,’ ‘gastrointestinal tract
COVID-19,’ ‘gut-lung-axis COVID-19,’ ‘probiotics microbiome
COVID-19,’ ‘drugs COVID-19,’ and ‘exercise microbiome.’ Articles
written in English published between 2011 and 2021 as well as
relevant articles from the reference lists were retrieved and
reviewed. A flow chart showing the literature review process is
shown in Fig. 1.
3. Microbiome profile and COVID-19
The composition of the gut microbiome changes during
a mild, moderate or severe infection, and when a person recovers
from infection (14). The abundance
of Coprobacillus, Clostridium ramosum and
Clostridium is associated with the severity of COVID-19. In
addition, there was an inverse correlation between the abundance of
Faecalibacterium prausnitzii (anti-inflammatory bacteria)
and the severity of the disease (Table
I). Kim et al (15)
reported that the abundance of Firmicutes was positively
correlated with the severity of COVID-19 symptoms. However,
Firmicutes-negative patients have also been reported.
Moreira-Rosário et al (16)
reported that the ratio of Firmicutes and
Bacteroidetes decreased in COVID-19 patients admitted to the
ICU from ambulatory wards. The diversity of the gut microbiome
affects the condition of patients with COVID-19. According to Ren
et al (17),
Faecalibacterium has anti-inflammatory properties and has
been recognized as a potential biomarker of human health (17). According to Zuo et al
(14), COVID-19 patients exhibit
changes in the composition of the microbiome compared with healthy
people, which results in an increased probability of being infected
with opportunistic pathogens during hospitalization. In other
respiratory infections, such as with the respiratory syncytial
virus, microbiota diversity is associated with weight loss. Viral
respiratory infections can lead to reduced intake of nutrients that
can alter the gut microbiota (18).
In similar cases, Middle East Respiratory Syndrome (MERS) is
associated with the gut microbiome. Proteobacteria were more
abundant in fatal cases than in non-fatal cases, including species
from the Acinetobacter and Klebsiella genera.
Patients infected with 2009 influenza A H1N1 pneumonia were found
to have increased numbers of Proteobacteria compared with
non-viral cases of pneumonia (19).
However, information on the detailed mechanism of COVID-19
infection on bacteria in the intestine and the function of the
intestine itself is sparse. Several factors can affect homeostasis
in the gut, and genetic factors that can affect the gut microbiota
cannot be excluded. The present study revealed the possible
regulatory effects of COVID-19 on microbiota homeostasis that may
impact a patient's health. In this review, the possibility of
modulating the balance of gut microbiota through various factors,
such as exercise, nutrition-probiotics, prebiotics, vitamins, drugs
and herbal medicines are discussed, and these may be considered as
future treatment modalities to hasten recovery of COVID-19
patients. The microbiome profile associated with COVID-19 effects
are summarized in Table I.
 | Table IMicrobiome profile associated with a
specific COVID-19 effect. |
Table I
Microbiome profile associated with a
specific COVID-19 effect.
| First author,
year | SARS-CoV-2
effect | Microbiome
profile | Effect on GI
tract | (Refs.) |
|---|
| Zuo et al,
2020 | Indicative of a
prolonged effect of SARS-CoV-2 infection on the gut microbiomes of
patients with COVID-19. | Coprobacillus,
Clostridium ramosum, and Clostridium hathewayi | Correlated with
COVID-19 severity | (14) |
| Faecalibacterium
prausnitzii | Inverse correlation
with disease severity (anti-inflammatory bacterium) | |
| Bacteroides
dorei, Bacteroides thetaiotaomicron, Bacteroides
massiliensis, and Bacteroides ovatus | Correlated
inversely with SARS-CoV-2 | |
| Khan et al,
2021 | Gut microbiome
dysbiosis is an important predisposing factor for COVID-19 disease
severity. | Faecalibacterium
prausnitzii, Roseburia faecis, Roseburia inulinivorans,
Dorea formicigenerans, Lachnospira pectinoschiza,
Pseudobutyrivibrio xylanivorans, Clostridium
ruminantium, Butyricicoccus pullicaecorum | Firmicutes
phylum level, relative reduction abundance in asymptomatic, mild,
and severe symptoms | (13) |
| Shigella sonnei,
Shigella dysenteriae |
Proteobacteria phylum, positively
associated with severely infected COVID-19 patients | |
| Bacteroides
caccae, Bacteroides ovatus, Parabacteroides distasonis,
Bacteroides fragilis |
Bacteroidetes phylum, positively
associated with severely infected COVID-19 patients | |
| Ruminococcus
gnavus, Clostridium bolteae, Clostridium citroniae,
Clostridium hathewayi | Firmicutes
phylum, positively associated with severely infected COVID-19
patients | |
| Atopobium
rimae |
Actinobacteria phylum, positively
associated with severely infected COVID-19 patients | |
| Kim et al,
2021 | Gut microbiota
changes in patients with asymptomatic or mild symptoms. The
composition of the gut microbiota is recovered after negative
conversion of SARS-CoV-2 RNA in the respiratory tract. | Firmicutes
phylum | The most dominant
phylum in the patients with positive and negative SARS-CoV-2 | (15) |
|
Bacteroidetes phylum | The most abundant
phylum in healthy controls | |
| Ren et al,
2021 | The microbiota may
affect COVID-19 progression by secreting lipid molecules into the
blood. |
Lachnospira | Can produce SCFAs
by fermenting fiber and contribute to patient recovery | (17) |
|
Faecalibacterium | Anti-inflammatory
property and has been recognized as a potential biomarker for human
health | |
| Moreira-Rosário
et al, 2021 | Gut microbiota
dysbiosis is present in moderate and severe COVID-19 patients in
comparison with asymptomatic/mild patients. |
Bifidobacterium genus,
Collinsella genus, Roseburia, and Lachnospira
genera | Decreased tendency
from mild-to-moderate-to-severe symptoms | (16) |
| Ralstonia
genus (Proteobacteria) Firmicutes and
Bacteroidetes Phylum | Increases with the
COVID-19 severity Ratio decreases in COVID-19 patients from
ambulatory-ward-ICU | |
| Xu et al,
2021 | The dynamic change
of microbiome is complex during COVID-19. A synchronous restoration
of both the upper respiratory and gut microbiomes from early
dysbiosis towards late more diverse status has been observed in 6/8
mild COVID-19 adult patients. | Bacteroides
genus (Faecalibacterium, Roseburia, Blautia, and
Coprococcus) Neisseria and Actinomyce
Pseudomonas | Decrease gradually
from community type I to III/IV | (76) |
Pathophysiology of viral infections on
the effects of the gut microbiota
There are many variants of the SARS-CoV-2 virus, and
all have specific genetic markers associated with changes that can
result in increased transmissibility or virulence, reduced
neutralization by antibodies acquired through infection or
vaccination, and increased ability to evade detection or decreased
effectiveness of therapy or vaccination (20). SARS-CoV-2 infects human lungs, but
other studies have highlighted the vulnerability of other organs,
including the liver, brain, kidneys and intestine, to SARS-CoV-2
infection (21). Common symptoms of
SARS-CoV-2 infection include a cough, nausea, vomiting and diarrhea
followed by abdominal discomfort (22-24)
Patients with mild respiratory symptoms accompanied by GI symptoms
can experience rapid progression of infection (25). The gastric, duodenal and rectal
epithelium showed positive immunofluorescent staining of the viral
host receptor and the SARS-CoV-2 viral protein nucleocapsid. In
addition, evidence has shown that GI SARS-CoV-2 infection has the
potential for fecal-oral transmission (26).
SARS-CoV-2 enters our body via the lung parenchyma.
The angiotensin converting enzyme 2 (ACE-2) receptor, which is
widely expressed in endocrine organs, including the testes,
pancreas, thyroid, adrenal and pituitary glands, is used by
coronaviruses as the route of entry into the host cell (27). ACE-2 expression is highest in
erythrocytes and is also expressed in the small intestine, large
intestine and duodenum (25).
SARS-CoV-2 is associated with ACE-2, which can also be expressed by
fat. Obesity can inhibit macrophage activation and migration,
impair the generation of neutralizing antibodies and memory T
cells, and decrease the activation of effector cells of the immune
system, hence its correlation with chronic inflammation (28). In addition, type 2 diabetes mellitus
can increase ACE-2 expression in the lungs and other tissues due to
the hyperglycemic response. Hyperglycemia can lead to
alveolar-capillary microangiopathy and non-enzymatic protein
glycation in the lungs. This makes collagen less susceptible to
proteolysis, which causes collagen accumulation in connective
tissues in the lungs, resulting in restrictive lung disease
(29). The role of ACE-2 is
essential for numerous organs, including the lungs, kidneys and
gut. ACE-2 participates in the degradation of digestive enzymes
that yields free amino acids and influences bacterial metabolism,
generating bioactive peptide fragments that include angiotensin
ACE-2 (30,31). ACE-2 possesses RAS-independent
functions that regulate intestinal amino acid homeostasis,
antimicrobial peptide expression, and gut microbiome ecology. ACE-2
is also a key regulator of dietary amino acid homeostasis, innate
immunity, gut microbial ecology and infectious susceptibility to
colitis (31).
Yang et al (32) reported that the gut microbiota is
important for the regulation of colonic ACE-2 expression.
Additionally, it may contribute to the gut-lung axis pathology
during COVID-19(32). The human gut
microbiota has important roles in human physiology, including
maintenance of the epithelial barrier, inhibition of adhesion of
pathogens to the intestinal surface, modulation of the maturation
of the immune system and degradation of indigestible carbons, such
as plant polysaccharides and metabolite production (33). Humans naturally obtain gut
microbiota from the mother during breastfeeding. Thereafter,
microbiota are obtained from food intake and the environment
(34). A healthy gut microbiota is
rich in Bifidobacterium spp., Faecalibacterium spp.,
Ruminococcus spp. and Prevotella spp. (35,36).
The dominant bacterial phyla found in the intestine are
Firmicutes and Bacteroidetes (37). The intestinal barrier epithelium has
important roles; apart from being protective, it also acts as a
reservoir for host-produced antimicrobial molecules, such as
secretory and defensive IgA. There are host-microbial interactions
that are regulated through host recognition of microbe-associated
molecular patterns and bacterial metabolites; thus, if there are
changes in the host conditions and the microbiome composition, this
will contribute to differences in mucus composition and increased
susceptibility to infection (38).
Gut microbiome manipulation to alter the gut-lung
axis may potentially protect humans against respiratory infections.
The gut-lung axis can be described as a common mucosal
immunological system. There is a correlation between the gut and
lung, particularly with regard to respiratory immune and
anti-infective responses. In COVID-19, the gut can downregulate the
expression of ACE-2 in the intestine. Probiotics may have potential
use for reducing upper respiratory tract infection symptoms
(39). The gut and respiratory
tract are associated with the modulation of the immune response and
dysbiosis. There is microbial translocation with the decrease in
intestinal barrier integrity followed by a secondary infection.
Chronic lung diseases can develop along with GI tract diseases
(40). Genetic or exogenous
factors, including diets and antibiotic treatment, can alter the
composition of the gut microbiota and can result in a reduced
capacity to mount adequate local and systemic immune responses. The
gut microbe-derived components and metabolites include short-chain
fatty acids (SCFAs) associated with the gut-lung axis. The direct
effects of SCFAs is accomplished through the engagement of G
protein-coupled receptors (41).
Microbiome interaction and cytokine
regulation
There is an interaction between the microbiome and
cytokines, and this host-microbiome interaction is associated with
the production of tumor necrosis factor-α (TNF-α) and interferon
(IFN)-γ. If there is a change in the composition of the microbiome
in the digestive tract, the protective mechanism will be disrupted,
leading to an increase in the risk of infection. The gut microbiome
plays a role in homeostasis (42).
Given the importance of the gut microbiota in the immune response,
and knowing that SARS-CoV-2 progression appears to be associated
with the ‘cytokine storm’, which leads to hyper-inflammation
(elevated levels of pro-inflammatory cytokines, including TNF-α,
IL-6 and IL-1β), a particular focus should be given to the gut
microbiota (20,27). The increase in cytokine levels is
associated with severe COVID-19. In addition, the levels of
leukocytes, lymphocytes and IL-6 are also increased (40). Excessive IL-6 signaling leads to a
myriad of biological effects that contribute to organ damage, such
as inducing vascular endothelial growth factor expression in
epithelial cells and increasing vessel permeability (43).
The gut microbiota and cytokines are correlated with
each other due to butanoate metabolism and butyrate production
(44). Butyrate is involved in the
regulation of various inflammatory factors, including IL-10, IL-6
and IL-18(44). In a study by
Blanco-Melo (45), it was reported
that there was a host response to viral infection. This response
was determined by common type I and III IFNs coupled with increased
chemokines and high IL-6 expression. SARS-CoV-2 also induces the
levels of chemokines. Lin et al (46) reported that certain cytokines were
associated with the gut microbiome in patients with Parkinson's
Disease (46). In that study, a
positive correlation between the abundance of Bacteroides
genus and the plasma concentration of TNF-α in Parkinson's disease
was identified. Microbial metabolites regulate the host immune
system. Bacteroidetes and Clostridium produce SCFAs
and desaminotyrosine, which can enhance influenza-specific CD8+
T-cell functions and type I IFN signaling in macrophages,
increasing protection against influenza infection (47).
4. Modulation of the microbiome profile to
regulate the inflammatory response
Exercise
During the pandemic, working from home resulted in
changes in food intake and physical activity. According to research
by Brancaccio et al (48),
participation in physical activity decreased during the pandemic.
However, since physical activity has several beneficial effects,
certain individuals performed exercises by utilizing internet-based
platforms, such as social media (48). Physical activity can help alter the
composition of the gut microbiota (48). Quiroga et al (49) reported that in obese children who
were physically active, changes in the microbiome significantly
reduced Proteobacteria levels, which tended to be similar to
those found in healthy children. In addition, there is an
interaction between the microbiota and host cell immunity (49). Toll-like and Nod-like receptor are
signaling pathways responsible for a state of low-grade
inflammation, and their expression levels are increased during
physical exercise and obesity (49).
Exercise can affect the gut integrity and the
composition of gut microbiota in the host. In a study by Campbell
et al (50), comparisons
between groups of animals showed the presence of a diverse range of
gut microbiota (50). However,
Clostridiales dominated the fecal microbiota present in all
animal groups. Faecalibacterium prausnitzii was detected
only in animals who exercised, whereas animals with typical diets
without exercise, had large clusters of Lachnospiraceae
spp., which were not present in animals fed high-fat diets.
Allobaculum spp. and Clostridium spp. were found in
animals with regular diets who exercised, whereas animals fed
high-fat diets had microbial groups associated with
Peptococcus spp (50).
In addition, a study of rugby athletes by Clarke
et al (51) showed
significant differences between the athletes and control group. The
athletes had higher taxa microbiota: 22 phyla, 68 families and 113
genera. Exercise and protein intake increased gut microbiota
diversity in the athletes. Firmicutes and
Ruminococcaceae were abundantly present, whereas
Bacteroidetes were less abundant in the athletes (51). During exercise, TNF receptors
gradually produce TNF-α inhibitors, the levels of which increase
during and after exercise. Similarly, IL-1 receptor antagonists are
produced during exercise and remain elevated post-exercise
(52). Physical exercise acts as a
modulator of the immune system as it can increase pro- and
anti-inflammatory cytokines and secular lymphocytes, and IFN-I can
promote macrophage and lymphocyte activity. Suppression of the
IFN-I response has been noted in COVID-19. In addition, severe
COVID-19 infections have been associated with a pro-inflammatory
cytokine storm, lymphopenia, circulatory changes and viral spread
to other organs (53).
Nutrition Probiotics
Probiotics are non-pathogenic microbes that are
beneficial to humans. The most common species are
Lactobacillus and Bifidobacterium, which are present
in several fermented foods (54,55).
Probiotics provide protection as they have a low disease activity
index and cause considerably little histopathological damage in the
large intestine. In addition, probiotics are more effective in
modulating the host immune response, as they decrease IL-1β and
IL-6 levels and increase the expression of TGF-β and IL-10(56). Consumption of Lactobacillus
reuteri V3401 can reduce IL-6 and sVCAM levels (57). Probiotics have been reported to
increase the levels of IFN-I and the number and activity of
antigen-presenting cells, natural killer cells and T-cells, as well
as systemic and mucosa-specific antibodies in the lungs. Clinical
evidence indicates that modulation of the gut microbiota can
positively influence COVID-19 disease progression (58).
Fermented milk and yogurt are the most common
consumed forms of probiotics. In a study by McNulty et al
(59), probiotic bacterial strains
were shown to affect the gut microbiota. There were no significant
changes in the bacterial composition or representation of
gene-encoding enzymes after consuming fermented milk (59). However, the results of fecal sample
sequencing and urine metabolite spectrometry showed significant
changes in the expression of microbiome-encoded enzymes involved in
various metabolic pathways, the most prominent of which were
related to carbohydrate metabolism. Bacterial strains present in
fermented milk or yogurt were not associated with the abundance of
these phyla microbiota in the gut. There were differences in
Bifidobacterium strains in individuals who consumed
fermented milk mixed with probiotic strains and
Bifidobacterium probiotics compared to
Lactobacillus-fermented milk. Fermented probiotic milk and
yogurt intake were associated with the levels of ingested bacteria
(60). The composition of different
bacteria in probiotic products can affect the environment of the
gut microbiota, and the interaction between the gut microbiota and
host will provide protection against viral infections. Probiotics
provide protection, treatment and prevention of illness in the
digestive system.
Prebiotics
Consumption of prebiotics is a dietary strategy that
can modify the GI microbiota for health benefits (61). Prebiotics are substrates selectively
utilized by host microorganisms that confer a health benefit.
Prebiotics enhance the growth of Bifidobacteria and
Lactobacilli, which have beneficial effects on system-wide
metabolism and physiology. Prebiotics are predominantly
carbohydrate-based, but other substances, such as polyphenols and
polyunsaturated fatty acids, may exert prebiotic effects.
Bacteroides, one of the microbiome genera, can break down
high molecular weight polysaccharides (62).
Prebiotics are fibers that cannot be digested by the
host but are metabolized by the colonic microbiome, resulting in
the growth of certain bacteria. Intervention with prebiotics,
probiotics, or synbiotics is important, as it can alter the
composition of gut microbiota in the GI tract. This is essential
for the development of appropriate immune regulatory networks,
which influences disease risk later in life (63). Dietary consumption of certain food
products can result in significant changes in the gut microbiota
composition. The change in Bifidobacteria may be attributed
to prebiotics (64). The concept of
prebiotics is based on increasing the presence of beneficial
microorganisms in the gut microbiota, such as Bifidobacteria
and Lactobacilli. Since the diversity of the gut microbiota
has expanded, there may be other potential beneficial genera, such
as Roseburia, Eubacterium, Faecalibacterium,
Akkermansia, Christensenella and
Propionibacteria (58).
Prebiotics, probiotics, fermented foods and synbiotics can modulate
the gut and extend its benefits to distant sites, such as the
respiratory tract (65).
Vitamins
COVID-19 is associated with vitamin D deficiency.
The rate of SARS-CoV-2 infection was significantly lower in vitamin
D-deficient patients supplemented with cholecalciferol than those
without supplementation (66).
According to Robles-Vera et al (67), the abundance of Prevotella
and Actinomyces increased, whereas that of
Odoribacteraceae and genus Butyricimonas decreased in
mice on a vitamin D-free diet. Vitamin D deficiency did not induce
intestinal dysbiosis, but it resulted in several specific changes
to the bacterial taxa, which might play a pathophysiological role
in the immunological dysregulation associated with hypovitaminosis
(67). Vitamin D is now recognized
as a hormone with several extra-skeletal actions, including in the
immune system. The microbiome is correlated with the levels of
vitamin D, and Firmicutes phylum, Clostridia class
and Clostridia order have been recognized as butyrate
producers. Some of the genera identified were Ruminococcus,
Coprococcus and Blautia obeum species. Specific
microbiota, known as butyrate producers, provide potential targets
for intervention, either through dietary modification or vitamin D
supplementation (68). Vitamin D
deficiency is associated with the cytokine storm and an increased
likelihood of requiring a ventilator in hospitalized COVID-19
patients. Meanwhile, dexamethasone appears to mitigate the adverse
effects of vitamin D deficiency (69).
Vitamin A (VA) exhibits pharmacological activity in
the management of pneumonia. The mechanisms of action of VA against
SARS-CoV-2 include enrichment of immunoreactions, inhibition of
inflammatory reactions and biological processes related to reactive
oxygen species (70). VA can assist
in promoting intestinal immunity and epithelial integrity (71). According to a study by Liang et
al (28), VA may contribute to
the clinical management of CHOL/COVID-19 by inducing cell repair,
suppressing oxidative stress and inflammatory reactions, and
ameliorating immunity (28). One of
the roles of VA is regulating the proliferation of B- and T-cell
differentiation and interaction, including induced T-cell migration
(72). VA can affect gut immunity
and epithelial integrity, factors that may, in turn, modulate
microbiome development. In neonates, VA is associated with a
relatively higher abundance of Bifidobacterium, and a good
VA status is associated with a higher abundance of other genera,
such as Akkermansia (71).
Drug-related
Over the course of a humans life, an individual will
be exposed to numerous drugs, including vaccinations, painkillers,
antibiotics and contraceptives. COVID-19 treatment requires
limiting viral multiplication and neutralizing tissue damage
induced by an inappropriate immune reaction (73). The microbiome can act as a drug as
it can secrete enzymes with a biocatalyst effect (74). Drugs can affect the composition of
the microbiome in terms of abundance, diversity and function. If
there is a deviation, then this will result in dysbiosis. Changes
in the microbiome due to administration of drugs can be temporary
or long-term (74). There is a
positive correlation between the quantity of drugs taken and
overall microbiome composition (74). Bifidobacterium decreases
during multidrug treatment, which in elderly COVID-19 patients, not
only causes dysbiosis in the intestine but also increases bacterial
resistance, and in adults the dynamic changes to the microbiome was
complex during COVID-19 infection (75,76).
Antibiotic use (and misuse) and polypharmacy may promote the
selection of resistant commensal strains, which constitute a
reservoir of transmittable resistance factors in elderly
populations with comorbidities (75).
Antibiotic-induced alterations of the gut
microbiome, as an ecologically complex system, may also result in
metabolic changes in the host, increasing the risk of weight gain
and obesity, altering the immune response and increasing
susceptibility to other infections from a loss of colonization
resistance (74,77). The top microbiome-associated drugs
include proton pump inhibitors lipid-lowering statins, laxatives,
metformin, β-blockers, ACE inhibitors and selective serotonin
reuptake inhibitors (77).
The uncontrolled inflammatory process is of
particular concern in cases of COVID-19. Research by Dormont et
al (78) reported that cases of
COVID-19 that resulted in death might be caused by virus-induced
hyper-inflammation; multidrug nanoparticles (NPs) were the topic of
this study. These multidrug NPs enable efficient encapsulation of
drugs, reduce side effects and promise anti-inflammatory and
protective effects in lethal endotoxemia and systemic shock models
(78). The combination of
traditional Chinese and Western medicine may carry risks of
herb-drug interaction (HDI) (79).
A study by Liu et al (79)
reported that HDIs primarily occurred in the GI tract, and
typically led to diarrhea, but this did not develop or was milder
when taking a single drug. According to Dai et al (80), the consistency between the gut
microflora and glycosidase system indicates the inhibition of
darunavir on the activity of β-glucosidase and β-glucuronidase.
Regarding darunavir (with a high HDI risk), when patients with
COVID-19 use traditional herbal and anti-coronavirus medicines in
combination, it is necessary to adjust the intake interval to avoid
alteration of the efficacy and toxicity to prevent/mitigate adverse
effects (80).
Hydroxychloroquine (HCQ) is an anti-malarial drug
that can be used as treatment of COVID-19, and the combination of
chloroquine and HCQ is already used in the treatment of COVID-19.
Chloroquine does not affect the expression of ACE-2 on cell
surfaces, but it inhibits terminal glycosylation of the ACE-2
receptor for cell entry, which is targeted by SARS-CoV and
SARS-CoV-2. HCQ can be used as treatment for rheumatoid arthritis
(73). Pan et al (81) reported that HCQ did not increase
intestinal permeability. The effect of HCQ was detected on gene
expression of tight junction-associated proteins in colonic tissue,
and there was no statistically significant change in the mRNA
expression levels of several claudins (1, 2, 4, 5, 8 and 14),
occludin, cadherin 1, mucin 2 and zonula occludens 1 (ZO-1) after
HCQ challenge for 14 days. However, HCQ could alter the gut
microbiota composition, and the dominant phyla in these groups were
Bacteroidetes and Firmicutes (81). Million et al (82) reported that simultaneous intake of
HCQ and azithromycin (AZ) could be used as a treatment for
COVID-19. Clinical results of a combination of HCQ and AZ reported
mild adverse events (GI or skin symptoms, headache, insomnia and
transient blurred vision). However, AZ can induce a modest decline
in the microbiota and a shift in taxonomic composition driven by a
reduction in Proteobacteria and Verrucomicrobia
(specifically, Akkermansia muciniphila) (83). Moreover, the combination of AZ and
florfenicol can alter the gut microbiota composition and decrease
the abundance and diversity. At the phylum level, the ratio of
Firmicutes/Bacteroidetes increased significantly in
the antibiotic groups (84). Drug
treatment in COVID-19 patients can affect the GI microbiome.
However, the gut microbiome can provide efficacy and safety by
changing the structure of the drug enzymatically and altering the
bioavailability, bioactivity or toxicity of the drug.
Herbal
Herbal medicines have several benefits for the GI
tract and can serve as alternative treatments. The Nutrition Care
(NC) Gut Relief Formula contains a combination of herbs and
nutrients, including curcumin, aloe vera, slippery elm, guar gum,
pectin, peppermint oil and glutamine. The NC Gut Relief Formula
significantly improved GI tract problems and the microbiome
profile, and reduced or increased inflammation (85). Traditional Chinese herbal medicines
have played a vital role in the treatment of SARS, and combined
with Western medicines, significantly improve the symptoms of SARS
(86). Herbal medicines have fewer
side effects than classic pharmaceuticals (87).
Herbal medicine and functional foods contain fiber,
polyphenols and polysaccharides, exerting prebiotic-like activities
to prevent and treat cardiometabolic diseases (88). The abundance of Bacteroidetes
and Akkermansia, Bifidobacteria,
Lactobacillus, Bacteroides and Prevotella is
increased by herbal medicine and functional foods. A recent study
showed that curcumin improved intestinal barrier function by
modulating intracellular signaling and organizing tight junctions,
providing a mechanism where curcumin modulates chronic inflammatory
diseases (88). Peterson et
al (89) reported that herbal
medicines drove the formation of unique microbial communities.
Herbal medicines also induced blooms of butyrate and propionate
production.
Herbal medicines can modulate the gut microbiota in
a manner predicted to improve colonic epithelium function, reduce
inflammation and provide protection from opportunistic bacteria.
Herbal medicine, or natural active ingredients, can reduce blood
glucose and lipid levels and lower body and visceral adipose
weights (90). Herbs can restore
the structure of the intestinal floral, and herbs can aid COVID-19
treatment by modulating the immune system. The intestinal flora is
closely related to the expression profile of tight junction
proteins in the intestinal epithelial cells, including claudin-1,
occludin and ZO-1. Five main categories of herbal ingredients can
affect the intestinal flora: Glycosides, flavonoids, alkaloids,
phenylpropanoids and organic acids. China's guidelines mentioned
that herbs and prebiotics can be used in the treatment of COVID-19,
especially for maintaining intestinal floral homeostasis and
preventing secondary bacterial infections. One of the beneficial
effects of herbal based medicines is they inhibit the activity of
SARS-CoV-2 3C-like protease (91).
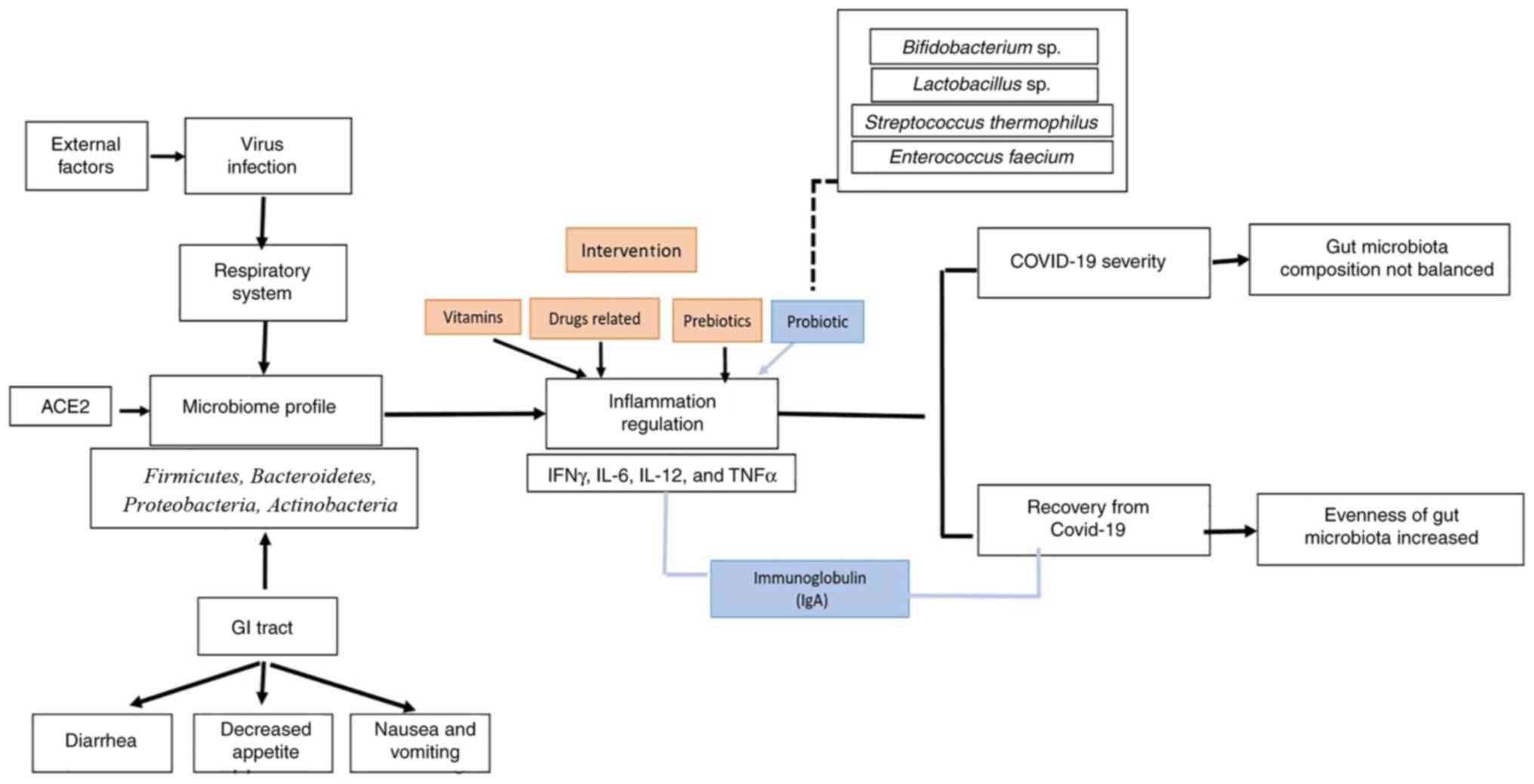
5. Conclusions
The modulation of the factors that control the
physiological growth of the gut microbiome will determine the
proportionate ratio of microbiome types, which is important for
modulating cytokine levels that impact inflammatory processes, such
as in the case of COVID-19 infection (Fig. 2). This review highlights the
potential future directions and clinical applications for
subsequent studies. It hypothesized that modulation of the
microbiome may hasten the recovery process or reduce the severity
of an illness via regulation of the inflammatory process.
Acknowledgements
The authors would like to thank Mr. Deby Fajar
Mardhian (Department of Dental Materials and Technol, Universitas
Padjadjaran) who assisted in reviewing and proofreading the
manuscript.
Funding
Funding: This study was supported by a WCR grant from the
Ministry Education and Culture (grant no. 1207/UN6.3.1/PT.00/2021),
and an Academic Leadership grant (grant no.
1959/UN6.3.1/PT.00/2021).
Availability of data and materials
The datasets used and/or analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
NN, IM, LA, HG and RL performed the literature
search and assisted in drafting and revising the manuscript. All
authors have read and approved the final manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Chan JFW, Yuan S, Kok KH, To KK, Chu H,
Yang J, Xing F, Liu J, Yip CC, Poon RW, et al: A familial cluster
of pneumonia associated with the 2019 novel coronavirus indicating
person-to-person transmission: A study of a family cluster. Lancet.
395:514–523. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kang MK, Kim KO, Kim MC, Cho JH, Kim SB,
Park JG, Kim KH, Lee SH, Jang BI and Kim TN: Clinical
characteristics of coronavirus disease 2019 patients with diarrhea
in Daegu. Korean J Intern Med. 35:1261–1269. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tariq R, Saha S, Furqan F, Hassett L,
Pardi D and Khanna S: Prevalence and Mortality of COVID-19 patients
with gastrointestinal symptoms: A systematic review and
Meta-analysis. Mayo Clin Proc. 95:1632–1648. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Graham MS, Sudre CH, May A, Antonelli M,
Murray B, Varsavsky T, Kläser K, Canas LS, Molteni E, Modat M, et
al: Changes in symptomatology, reinfection, and transmissibility
associated with the SARS-CoV-2 variant B.1.1.7: An ecological
study. Lancet Public Heal. 6:e335–e345. 2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Cascella M, Rajnik M, Cuomo A, Dulebohn SC
and Di Napoli R: Features, evaluation and treatment coronavirus
(COVID-19. Review from StatPearls Publishing, Treasure Island (FL),
10 Mar, 2020.
|
|
6
|
Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J,
Li P, Hu B, Wang J, Hu C, et al: Clinical characteristics of
COVID-19 patients with digestive symptoms in Hubei, China: A
descriptive, cross-sectional, multicenter study. Am J
Gastroenterol. 115:766–773. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Nogueira-de-Almeida CA, Del Ciampo LA,
Ferraz IS, Del Ciampo IRL, Contini AA and Ued FDV: COVID-19 and
obesity in childhood and adolescence: A clinical review. J Pediatr
(Rio J). 95:546–558. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Yang J, Hu J and Zhu C: Obesity aggravates
COVID-19: A systematic review and meta-analysis. J Med Virol.
93:257–261. 2021.
|
|
9
|
Gao F, Zheng KI, Wang XB, Sun QF, Pan KH,
Wang TY, Chen YP, Targher G, Byrne CD, George J and Zheng MH:
Obesity is a risk factor for greater COVID-19 severity. Diabetes
Care. 43:e72–e74. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Al-Salameh A, Lanoix JP, Bennis Y,
Andrejak C, Brochot E, Deschasse G, Dupont H, Goeb V, Jaureguy M,
Lion S, et al: Characteristics and outcomes of COVID-19 in
hospitalized patients with and without diabetes. Diabetes Metab Res
Rev. 37(e3388)2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Wang F, Yang Y, Dong K, Yan Y, Zhang S,
Ren H, Yu X and Shi X: Clinical characteristics of 28 patients with
Diabetes and COVID-19 in Wuhan, China. Endocr Pract. 26:668–674.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Li J, Wang X, Chen J, Zuo X, Zhang H and
Deng A: COVID-19 infection may cause ketosis and ketoacidosis.
Diabetes Obes Metab. 22:1935–1941. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Khan M, Mathew BJ, Gupta P, Garg G,
Khadanga S, Vyas AK and Singh AK: Gut dysbiosis and il-21 response
in patients with severe covid-19. Microorganisms.
9(1292)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zuo T, Zhang F, Lui GCY, Yeoh YK, Li AYL,
Zhan H, Wan Y, Chung ACK, Cheung CP, Chen N, et al: Alterations in
gut microbiota of patients with COVID-19 during time of
hospitalization. Gastroenterology. 159:944–955.e8. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kim HN, Joo EJ, Lee CW, Ahn KS, Kim HL,
Park Dong-II and Park SK: Reversion of gut microbiota during the
recovery Phase in patients with asymptomatic or mild Covid-19:
Longitudinal study. Microorganisms. 9(1237)2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Moreira-Rosário A, Marques C, Pinheiro H,
Araújo JR, Ribeiro P, Rocha R, Mota I, Pestana D, Ribeiro R,
Pereira A, et al: Gut microbiota diversity and C-reactive protein
are predictors of disease severity in COVID-19 patients. Front
Microbiol. 12(705020)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ren Z, Wang H, Cui G, Lu H, Wang L, Luo H,
Chen X, Ren H, Sun R, Liu W, et al: Alterations in the human oral
and gut microbiomes and lipidomics in COVID-19. Gut. 70:1253–1265.
2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Groves HT, Higham SL, Moffatt MF, Cox MJ
and Tregoning JS: Respiratory viral infection alters the gut
microbiota by inducing Inappetence. MBio. 11:e03236–19.
2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Aljabr W, Alruwaili M, Penrice-Randal R,
Alrezaihi A, Harrison AJ, Ryan Y, Bentley E, Jones B, Alhatlani BY,
AlShahrani D, et al: Amplicon and Metagenomic Analysis of Middle
East Respiratory Syndrome (MERS) Coronavirus and the Microbiome in
Patients with Severe MERS. mSphere. 6(e0021921)2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Raman R, Patel KJ and Ranjan K: COVID-19:
Unmasking emerging SARS-CoV-2 variants, vaccines and therapeutic
strategies. Biomolecules. 11(993)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Trypsteen W, Van Cleemput J, Snippenberg
WV, Gerlo S and Vandekerckhove L: On the whereabouts of SARS-CoV-2
in the human body: A systematic review. PLoS Pathog.
16(e1009037)2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Holshue ML, DeBolt C, Lindquist S, Lofy
KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural
A, et al: First Case of 2019 novel coronavirus in the united
states. N Engl J Med. 382:929–936. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He
JX, Liu L, Shan H, Lei CL, Hui DSC, et al: Clinical characteristics
of coronavirus disease 2019 in china. N Engl J Med. 382:1708–1720.
2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Sultan S, Altayar O, Siddique SM, Davitkov
P, Feuerstein JD, Lim JK, Falck-Ytter Y and El-Serag HB: AGA
Institute. Electronic address: simpleewilson@gastro.org. AGA
institute rapid review of the gastrointestinal and liver
manifestations of COVID-19, Meta-analysis of international data,
and recommendations for the consultative management of patients
with COVID-19. Gastroenterology. 159:320–334.e27. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Zhang J, Garrett S and Sun J:
Gastrointestinal symptoms, pathophysiology, and treatment in
COVID-19. Genes Dis. 8:385–400. 2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Xiao F, Tang M, Zheng X, Liu Y, Li X and
Shan H: Evidence for gastrointestinal infection of SARS-CoV-2.
Gastroenterology. 158:1831–1833.e3. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Clemente-Suárez VJ, Ramos-Campo DJ,
Mielgo-Ayuso J, Dalamitros AA, Nikolaidis PA, Hormeño-Holgado A and
Tornero-Aguilera JF: Nutrition in the actual covid-19 pandemic. A
narrative review. Nutrients. 13(1924)2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Liang X, Zhou R, Li Y, Yang L, Su M and
Lai KP: Clinical characterization and therapeutic targets of
vitamin A in patients with hepatocholangiocarcinoma and coronavirus
disease. Aging (Albany NY). 13:15785–15800. 2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Rajpal A, Rahimi L and Ismail-Beigi F:
Factors leading to high morbidity and mortality of COVID-19 in
patients with type 2 diabetes. J Diabetes. 12:895–908.
2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Penninger JM, Grant MB and Sung JJY: The
role of angiotensin converting enzyme 2 in modulating gut
microbiota, intestinal inflammation, and coronavirus infection.
Gastroenterology. 160:39–46. 2021.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Hashimoto T, Perlot T, Rehman A,
Trichereau J, Ishiguro H, Paolino M, Sigl V, Hanada T, Hanada R,
Lipinski S, et al: ACE2 links amino acid malnutrition to microbial
ecology and intestinal inflammation. Nature. 487:477–481.
2012.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Yang T, Chakraborty S, Saha P, Mell B,
Cheng X, Yeo JY, Mei X, Zhou G, Mandal J, Golonka R, et al:
Gnotobiotic rats reveal that gut microbiota regulates colonic mRNA
of Ace2, the receptor for SARS-CoV-2 Infectivity. Hypertension.
76:e1–e3. 2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Sánchez B, Delgado S, Blanco-Míguez A,
Lourenço A, Gueimonde M and Margolles A: Probiotics, gut
microbiota, and their influence on host health and disease. Mol
Nutr Food Res. 61(1600240)2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Putignani L, Del Chierico F, Petrucca A,
Vernocchi P and Dallapiccola B: The human gut microbiota: A dynamic
interplay with the host from birth to senescence settled during
childhood. Pediatr Res. 76:2–10. 2014.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Hills RD Jr, Pontefract BA, Mishcon HR,
Black CA, Sutton SC and Theberge CR: Gut Microbiome: Profound
implications for diet and disease. Nutrients.
11(1613)2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Villapol S: Gastrointestinal symptoms
associated with COVID-19: Impact on the gut microbiome. Transl Res.
226:57–69. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lv Y, Qin X, Jia H, Chen S, Sun W and Wang
X: The association between gut microbiota composition and BMI in
Chinese male college students, as analysed by next-generation
sequencing. Br J Nutr. 122:986–995. 2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Wiertsema SP, van Bergenhenegouwen J,
Garssen J and Knippels LMJ: The interplay between the gut
microbiome and the immune system in the context of infectious
diseases throughout life and the role of nutrition in optimizing
treatment strategies. Nutrients. 13(886)2021.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Mullish BH, Marchesi JR, McDonald JAK,
Pass DA, Masetti G, Michael DR, Plummer S, Jack AA, Davies TS,
Hughes TR and Wang D: Probiotics reduce self-reported symptoms of
upper respiratory tract infection in overweight and obese adults:
Should we be considering probiotics during viral pandemics? Gut
Microbes. 13:1–9. 2021.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Aktas B and Aslim B: Gut-lung axis and
dysbiosis in COVID-19. Turk J Biol. 44:265–272. 2003.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Dang AT and Marsland BJ: Microbes,
metabolites, and the gut-lung axis. Mucosal Immunol. 12:843–850.
2019.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Taco-Masias AA, Fernandez-Aristi AR,
Cornejo-Tapia A, Aguilar-Luis MA, del Valle LJ, Silva-Caso W,
Zavaleta-Gavidia V, Weilg P, Cornejo-Pacherres H, Bazán-Mayra J, et
al: Gut microbiota in hospitalized children with acute infective
gastroenteritis caused by virus or bacteria in a regional Peruvian
hospital. PeerJ. 8(e9964)2020.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Liu B, Li M, Zhou Z, Guan X and Xiang Y:
Can we use interleukin-6 (IL-6) blockade for coronavirus disease
2019 (COVID-19)-induced cytokine release syndrome (CRS)? J
Autoimmun. 111(102452)2020.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Zhang X, Shi L, Sun T and Guo K: Dysbiosis
of gut microbiota and its correlation with dysregulation of
cytokines in psoriasis patients. BMC Microbiol.
21(78)2021.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Blanco-Melo D, Nilsson-Payant BE, Liu WC,
Uhl S, Hoagland D, Møller R, Jordan TX, Oishi K, Panis M, Sachs D,
et al: Imbalanced host response to SARS-CoV-2 drives development of
COVID-19. Cell. 181:1036–1045.e9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Lin CH, Chen CC, Chiang HL, Liou JM, Chang
CM, Lu TP, Chuang EY, Tai YC, Cheng C, Lin HY and Wu MS: Altered
gut microbiota and inflammatory cytokine responses in patients with
Parkinson's disease. J Neuroinflammation. 16(129)2019.PubMed/NCBI View Article : Google Scholar
|
|
47
|
He Y, Wang J, Li F and Shi Y: Main
clinical features of COVID-19 and potential prognostic and
therapeutic value of the microbiota in SARS-CoV-2 infections. Front
Microbiol. 11(1302)2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Brancaccio M, Mennitti C, Gentile A,
Correale L, Buzzachera CF, Ferraris C, Montomoli C, Frisso G,
Borrelli P and Scudiero O: Effects of the covid-19 pandemic on job
activity, dietary Behaviours and physical activity habits of
university population of Naples, federico II-Italy. Int J Environ
Res Public Health. 18(1502)2021.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Quiroga R, Nistal E, Estébanez B, Porras
D, Juárez-Fernández M, Martínez-Flórez S, García-Mediavilla MV, de
Paz JA, González-Gallego J, Sánchez-Campos S and Cuevas MJ:
Exercise training modulates the gut microbiota profile and impairs
inflammatory signaling pathways in obese children. Exp Mol Med.
52:1048–1061. 2020.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Campbell SC, Wisniewski PJ, Noji M,
McGuinness LR, Häggblom MM, Lightfoot SA, Joseph LB and Kerkhof LJ:
The effect of diet and exercise on intestinal integrity and
microbial diversity in mice. PLoS One. 11(e0150502)2016.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Clarke SF, Murphy EF, O'Sullivan O, Lucey
AJ, Humphreys M, Hogan A, Hayes P, O'Reilly M, Jeffery IB,
Wood-Martin R, et al: Exercise and associated dietary extremes
impact on gut microbial diversity. Gut. 63:1913–1920.
2014.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Metsios GS, Moe RH and Kitas GD: Exercise
and inflammation. Best Pract Res Clin Rheumatol.
34(101504)2020.PubMed/NCBI View Article : Google Scholar
|
|
53
|
da Silveira MP, da Silva Fagundes KK,
Bizuti MR, Starck É, Rossi RC and de Resende E Silva DT: Physical
exercise as a tool to help the immune system against COVID-19: An
integrative review of the current literature. Clin Exp Med.
21:15–28. 2021.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Singh K and Rao A: Probiotics: A potential
immunomodulator in COVID-19 infection management. Nutr Res.
87:1–12. 2021.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Lehtoranta L, Pitkäranta A and Korpela R:
Probiotics in respiratory virus infections. Eur J Clin Microbiol
Infect Dis. 33:1289–1302. 2014.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Celiberto LS, Pinto RA, Rossi EA, Vallance
BA and Cavallini DCU: Isolation and characterization of potentially
probiotic bacterial strains from mice: Proof of concept for
personalized probiotics. Nutrients. 10(1684)2018.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Tenorio-Jiménez C, Martínez-Ramírez MJ,
Del Castillo-Codes I, Arraiza-Irigoyen C, Tercero-Lozano M, Camacho
J, Chueca N, García F, Olza J, Plaza-Díaz J, et al:
Lactobacillus reuteri V3401 reduces inflammatory biomarkers
and modifies the gastrointestinal microbiome in adults with
metabolic syndrome: The PROSIR study. Nutrients.
11(1761)2019.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Walton GE, Gibson GR and Hunter KA:
Mechanisms linking the human gut microbiome to prophylactic and
treatment strategies for COVID-19. Br J Nutr. 126:219–227.
2021.PubMed/NCBI View Article : Google Scholar
|
|
59
|
McNulty NP, Yatsunenko T, Hsiao A, Faith
JJ, Muegge BD, Goodman AL, Henrissat B, Oozeer R, Cools-Portier S,
Gobert G, et al: The impact of a consortium of fermented milk
strains on the gut microbiome of gnotobiotic mice and monozygotic
twins. Sci Transl Med. 3(106ra106)2011.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Redondo-Useros N, Gheorghe A, Díaz-Prieto
LE, Villavisencio B, Marcos A and Nova E: Associations of probiotic
fermented milk (PFM) and yogurt consumption with
Bifidobacterium and Lactobacillus components of the
gut microbiota in healthy adults. Nutrients. 11(651)2019.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Holscher HD: Dietary fiber and prebiotics
and the gastrointestinal microbiota. Gut Microbes. 8:172–184.
2017.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Sanders ME, Merenstein DJ, Reid G, Gibson
GR and Rastall RA: Probiotics and prebiotics in intestinal health
and disease: From biology to the clinic. Nat Rev Gastroenterol
Hepatol. 16:605–616. 2019.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Frei R, Akdis M and O'Mahony L:
Prebiotics, probiotics, synbiotics, and the immune system:
Experimental data and clinical evidence. Curr Opin Gastroenterol.
31:153–158. 2015.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Costabile A, Deaville ER, Morales AM and
Gibson GR: Prebiotic potential of a maize-based soluble fibre and
impact of dose on the human gut microbiota. PLoS One.
11(e0144457)2016.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Antunes AEC, Vinderola G, Xavier-Santos D
and Sivieri K: Food research international. Food Res Int.
37:195–197. 2004.
|
|
66
|
Oristrell J, Oliva JC, Casado E, Subirana
I, Domínguez D, Toloba A, Balado A and Grau M: Vitamin D
supplementation and COVID-19 risk: A population-based, cohort
study. J Endocrinol Invest: Jul 17, 2021 (Epub ahead of print).
|
|
67
|
Robles-Vera I, Callejo M, Ramos R, Duarte
J and Perez-Vizcaino F: Impact of Vitamin D deficit on the rat gut
microbiome. Nutrients. 11(2564)2019.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Thomas RL, Jiang L, Adams JS, Xu ZZ, Shen
J, Janssen S, Ackermann G, Vanderschueren D, Pauwels S, Knight R,
et al: Vitamin D metabolites and the gut microbiome in older men.
Nat Commun. 11(5997)2020.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Wenban C, Heer RS, Baktash V, Kandiah P,
Katsanouli T, Pandey A, Goindoo R, Ajaz A, Van den Abbeele K,
Mandal AKJ and Missouris CG: Dexamethasone treatment may mitigate
adverse effects of vitamin D deficiency in hospitalized Covid-19
patients. J Med Virol. 93:6605–6610. 2021.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Li R, Wu K, Li Y, Liang X, Tse WKF, Yang L
and Lai KP: Revealing the targets and mechanisms of vitamin A in
the treatment of COVID-19. Aging (Albany NY). 12:15784–15796.
2020.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Huda MN, Ahmad SM, Kalanetra KM, Taft DH,
Alam MJ, Khanam A, Raqib R, Underwood MA, Mills DA and Stephensen
CB: Neonatal Vitamin A supplementation and Vitamin A status are
associated with gut microbiome composition in Bangladeshi infants
in early infancy and at 2 years of age. J Nutr. 149:1075–1088.
2019.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Murni IK, Prawirohartono EP and Triasih R:
Potential role of vitamins and Zinc on acute respiratory infections
including Covid-19. Glob Pediatr Heal. 8:1–8. 2021.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Iyer M, Jayaramayya K, Subramaniam MD, Lee
SB, Dayem AA, Cho SG and Vellingiri B: COVID-19 : An update on
diagnostic and therapeutic approaches. BMB Rep. 53:191–205.
2020.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Brusselaers N: Prescribed drugs and the
microbiome. Gastroenterol Clin North Am. 48:331–342.
2019.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Zeppa SD, Agostini D, Piccoli G and
Stocchi V: Gut microbiota status in COVID-19 : An unrecognized
player? Front Cell Infect Microbiol. 10(576551)2020.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Xu R, Lu R, Zhang T, Wu Q, Cai W, Han X,
Wan Z, Jin X, Zhang Z and Zhang C: Temporal association between
human upper respiratory and gut bacterial microbiomes during the
course of COVID-19 in adults. Commun Biol. 4(24)2021.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Weersma RK, Zhernakova A and Fu J:
Interaction between drugs and the gut microbiome. Gut.
69:1510–1519. 2020.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Dormont F, Brusini R, Cailleau C, Reynaud
F, Peramo A, Gendron A, Mougin J, Gaudin F, Varna M and Couvreur P:
Squalene-based multidrug nanoparticles for improved mitigation of
uncontrolled inflammation in rodents. Sci Adv.
6(eaaz5466)2020.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Liu L, Zheng Y, Yang J, Lv J and Fan C:
Clinical observation on 13 novel coronavirus pneumonia cases
treated with integrated traditional Chinese and Western Medicine.
Zhejiang J Integr Tradit West Med. 30:349–351. 2020.
|
|
80
|
Dai T, Wang M, Wang P, Dai L, Dai R and
Meng Q: Inhibition effects of eight anti-coronavirus drugs on
glycosides metabolism and glycosidases in human gut microflora.
Pharmazie. 76:195–201. 2021.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Pan ZY, Chang YX, Han N, Hou FY, Lee BJY,
Zhi FC, Yang RF and Bi YJ: Short-term high-dose gavage of
hydroxychloroquine changes gut microbiota but not the intestinal
integrity and immunological responses in mice. Life Sci.
264(118450)2020.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Million M, Lagier J, Gautret P, Colson P,
Fournier PE, Amrane S, Hocquart M, Mailhe M, Esteves-Vieira V,
Doudier B, et al: Early treatment of COVID-19 patients with
hydroxychloroquine and azithromycin: A retrospective analysis of
1061 cases in Marseille France. Travel Med Infect Dis.
35(101738)2020.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Parker EPK, Praharaj I, John J, Kaliappan
SP, Kampmann B, Kang G and Grassly NC: Changes in the intestinal
microbiota following the administration of azithromycin in a
randomised placebo-controlled trial among infants in south India.
Sci Rep. 7(9168)2017.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Li R, Wang H, Shi Q, Wang N, Zhang Z,
Xiong C, Liu J, Chen Y, Jiang L and Jiang Q: Effects of oral
florfenicol and azithromycin on gut microbiota and adipogenesis in
mice. PLoS One. 12(e0181690)2017.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Ried K, Travica N, Dorairaj R and Sali A:
Herbal formula improves upper and lower gastrointestinal symptoms
and gut health in Australian adults with digestive disorders. Nutr
Res. 76:37–51. 2020.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Li Y, Liu X, Guo L, Li J, Zhong D, Zhang
Y, Clarke M and Jin R: Traditional Chinese medicine for treating
novel coronavirus (2019-nCoV) pneumonia: Protocol for a systematic
review and meta-analysis. Syst Rev. 9(75)2020.PubMed/NCBI View Article : Google Scholar
|
|
87
|
de Munter J, Pavlov D, Gorlova A, Sicker
M, Proshin A, Kalueff AV, Svistunov A, Kiselev D, Nedorubov A,
Morozov S, et al: Increased oxidative stress in the prefrontal
cortex as a shared feature of depressive- and PTSD-like syndromes:
Effects of a standardized herbal antioxidant. Front Nutr.
8(661455)2021.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Lyu M, Wang YF, Fan GW, Wang XY, Xu SY and
Zhu Y: Balancing herbal medicine and functional food for prevention
and treatment of cardiometabolic diseases through modulating gut
microbiota. Front Microbiol. 8(2146)2017.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Peterson CT, Sharma V, Uchitel S,
Denniston K, Chopra D, Mills PJ and Peterson SN: Prebiotic
potential of herbal medicines used in digestive health and disease.
J Altern Complement Med. 24:656–665. 2018.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Ma J, Zhou Q and Li H: Gut microbiota and
nonalcoholic fatty liver disease: Insights on mechanisms and
therapy. Nutrients. 9(1124)2017.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Chen Z, Lv Y, Xu H and Deng L: Herbal
medicine, gut microbiota, and COVID-19. Front Pharmacol.
12(646560)2021.PubMed/NCBI View Article : Google Scholar
|