Introduction
Colorectal cancer (CRC) is one of the most prevalent
malignant tumors in the world. Approximately 19 million new cases
and 10 million cancer-related deaths were estimated in 2020
(1,2). It has also been estimated that in
2015, there were 376,000 new CRC patients and 190,000 CRC-related
deaths in China (3). Although great
efforts have been made to improve the early diagnosis and treatment
of CRC, including advances in screening tools, surgical treatment,
chemotherapy, and targeted biologic therapy, a large proportion of
patients with advanced CRC still have a poor prognosis (4,5). The
5-year survival rate of early-stage CRC patients is ~90%, while it
drops to 13.1% for patients with advanced CRC (6). Since CRC presents symptoms only at an
advanced stage, the morbidity and mortality of CRC can be expected
to be reduced by early screening programs. Considering this, the
American Cancer Society has revised its guidelines for individuals
with an average CRC risk, lowering the screening age from 50 to 45
years (7). Given the limitations of
CRC screening, such as its invasiveness, high expense, and low
sensitivity and specificity, it is important to explore new early
screening molecular markers and potential therapeutic targets with
predictive or prognostic value for CRC.
According to GeneCards (https://www.genecards.org/cgi-bin/carddisp.pl?gene=RNF215),
ring finger protein 215 (RNF215) is a multichannel membrane protein
containing a ring-finger type zinc finger with 377 amino acids, 9
exons, and a molecular mass of 41101 Da. The gene is a
protein-coding gene located on 22q12.2, and an important paralog of
this gene is RNF128. To date, only a few studies have been
conducted on the RNF215 protein. Wu et al (8) reported that RNF215 interacts with p65
to reduce the production of type I interferons (IFNs); thus, it is
considered to be a key negative regulator of type I IFNs and has
been considered a potential target for disease intervention with
aberrant IFN production. Ma et al (9) suggested that high RNF215 expression is
associated with poor overall survival (OS), demonstrating its
function as a head and neck cancer (HNSC) oncogene. McIntosh et
al performed quantitative trait locus (QTL) expression
analysis, which showed that the single-nucleotide polymorphism
(SNP) variations near RNF215 were correlated with the expression
levels of the neighboring gene MTP18/SF3A1(10).
However, the association between RNF215 and CRC has
not been reported, and the exact role of RNF215 in the prognosis
and biological function of CRC has not been identified. Therefore,
the association between RNF215 and CRC was evaluated and the
possible role of RNF215 in CRC prognosis was analyzed through
datasets obtained from The Cancer Genome Atlas (TCGA). The
difference in RNF215 expression between CRC tumor and normal
tissues was investigated by analyzing the RNA sequencing (RNA-seq)
data of CRC tumors. Subsequently, the association between RNF215
expression and CRC clinicopathological characteristics as well as
prognosis was investigated. Furthermore, gene set enrichment
analysis (GSEA) was conducted to confirm the functional pathways
correlated with RNF215 in CRC. Immune infiltration and angiogenesis
were then examined to analyze their association with RNF215, and
the possible mechanism of RNF215 involvement in CRC was
investigated. Finally, the findings of the present study were
validated using immunohistochemistry (IHC) on samples from patients
with CRC obtained from the Department of Pathology, Shanghai Fifth
People's Hospital, Fudan University (Shanghai, China). The present
research demonstrated, to the best of our knowledge for the first
time, not only the importance of RNF215 but also its potential
roles as a molecular prognostic marker for prognosis and as a
therapeutic target in CRC.
Materials and methods
Data collection
RNF215 expression and clinical data of pancancer and
CRC cohorts were collected from TCGA (https://cancergenome.nih.gov/). The normalized RNA-seq
data and associated clinicopathological data of 647 CRC tumor
tissues and 51 normal tissues were also collected from the TCGA
database. The RNA-seq gene expression data in transcripts per
million reads (TPM) with CRC and clinical information were further
analyzed. The present study was conducted following the public
guidelines provided by TCGA. In addition, a total of 177 CRC
patient tissues and paired normal tissue samples were obtained from
the Department of Pathology, Shanghai Fifth People's Hospital,
Fudan University, between January 2012 and December 2016. A total
of 116 males and 61 females, with a median age at diagnosis of 67
years (range, 33-95 years) were included in the present study. The
inclusion criteria for patients with CRC were as follows: i) All of
the patients with pathological and imaging examinations who met the
CRC diagnostic standards; ii) patients who had no family history of
CRC; and iii) patients who had good mental health. The exclusion
criteria were as follows: i) patients who did not meet the
diagnostic standards of CRC; ii) patients who were diagnosed with
serious heart, lung, and other important organ diseases; and iii)
patients who were not conscious or were unable to communicate
normally. The research was conducted with approval from the Ethics
Committee of Shanghai Fifth People's Hospital, Fudan University
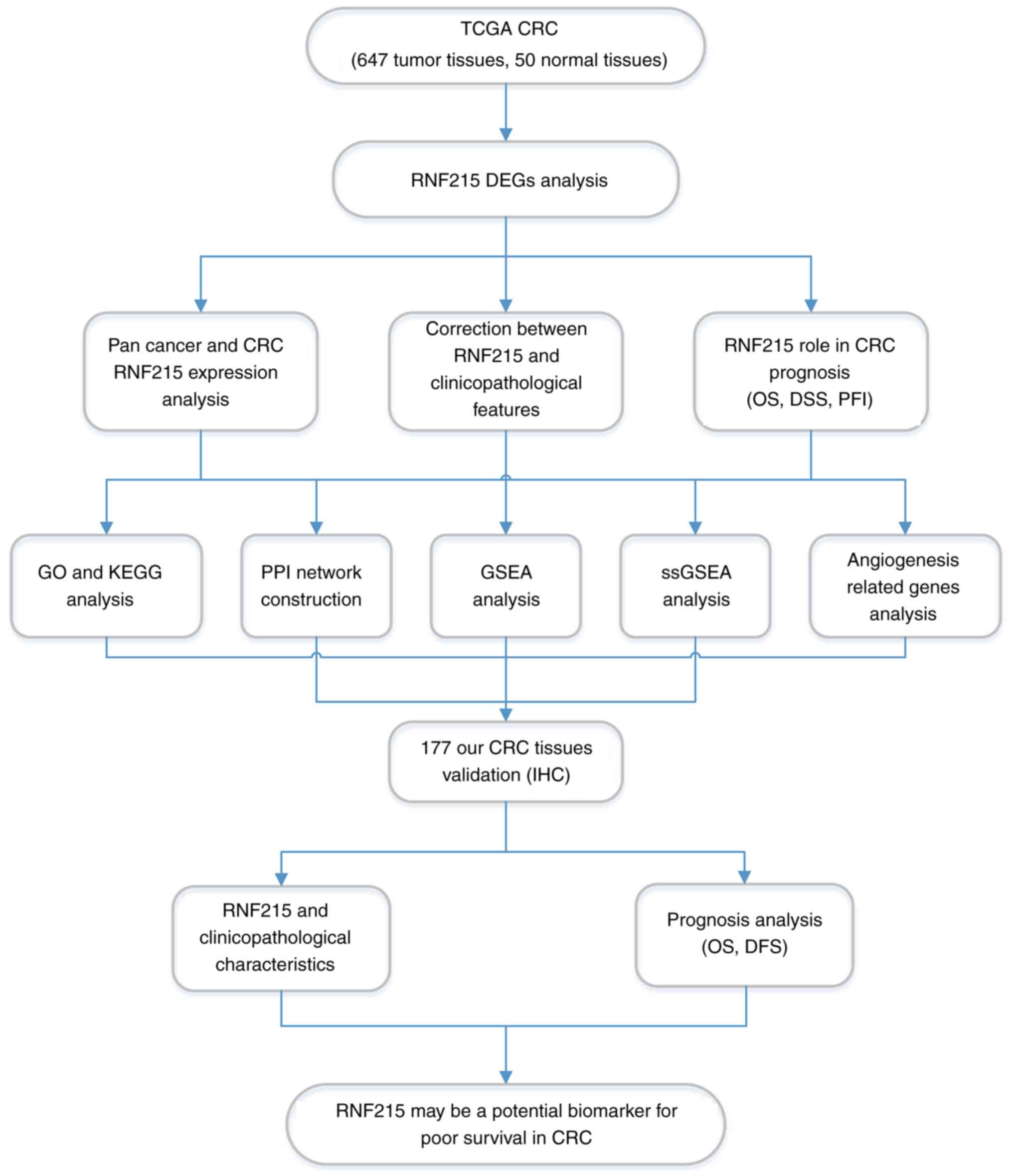
(approval no. 2021071). The study was performed according to the
flowchart in Fig. 1.
CRC differentially expressed gene
(DEG) analysis
Based on the median RNF215 expression level of TCGA
CRC patients, the patients were classified into two groups (the
low-expression group and high-expression group). A comparison of
the expression profile (HTSeq-TPM) of RNF215 between the two groups
and identification of DEGs were conducted with the R limma package
(11). Genes with a
log2|fold change (FC)|>1.5 and a false discovery rate
(FDR) <0.05 were identified as DEGs.
Functional enrichment analysis
To clarify the potential function of RNF215, the R
package DESeq2 was used to identify the differences between the two
groups (high vs. low RNF215 expression) (12) by setting the thresholds to a
log2|FC|>1.5 and an adjusted P-value (P.adj)
<0.05. Gene Ontology (GO) and Kyoto Encyclopedia of Genes and
Genomes (KEGG) enrichment analyses were conducted using the R
packages clusterProfiler and ggplot2(13). GO and KEGG analyses combined with
logFC enrichment analysis was conducted with the R packages GOplot
and ggplot2(14).
GSEA
GSEA (https://gseamsigdb.org) is a type of genome analysis
method used for interpretation of gene expression data (15). In order to clarify the potential
functions of RNF215, GSEA was conducted with the R package
clusterProfiler (version, 3.14.3) to investigate the positive
functional and pathway differences between the high- and
low-RNF215-expression groups (13).
Among the Molecular Signature Database (MSigDB) collections,
c2.cp.v7.0.symbols.gmt [Curated] was used as the reference gene
set. The RNF215 expression value was selected as a marker of
phenotype. Pathway enrichment was performed under the following
conditions: P.adj <0.05, FDR <0.25, and normalized enrichment
score (NES) >1. STRING tools (https://cn.string-db.org/) and Cytoscape software
(version, 3.9.1) were used to build the protein-protein interaction
(PPI) network (16-18).
Single-sample GSEA (ssGSEA)
The ssGSEA method was used with the R package GSA
(version, 1.34.0) to analyze CRC tumor tissues for the infiltration
of 24 immune cell species (19).
According to the marker genes of the 24 types of immunocytes
(20), the relative enrichment
fraction was calculated based on the gene expression profile in
tumor tissue. Spearman's correlation analysis was used to confirm
the correlation between RNF215 and immune cells. Detection of
immune cell infiltration was performed with the Wilcoxon rank sum
test.
Immunohistochemistry (IHC)
A tissue microarray (TMA) was constructed using all
177 formalin-fixed paraffin-embedded (FFPE) CRC tumor tissues, and
each tumor tissue consisted of three representative 1.5 mm punches,
as described in a previous study by the authors (21). All tissues were fixed with 10%
formalin at room temperature (20˚C) for more than 24 h. Antigen
retrieval was performed with a pressure cooker (Y-60C816, Joyoung,
Hangzhou, China) for 30 min at 100˚C. To block endogenous
peroxidase, the slides were immersed in 3% hydrogen peroxide for 10
min at 20˚C.
TMA slides (3-µm thick) were automatically immunized
with a Ventana benchmark instrument (Roche Diagnostics) following
the manufacturer's instructions. Slides were incubated with a
primary antibody for 14 h at 4˚C followed by the application of a
secondary antibody [ultraView Universal HRP Multimer (55 µg/ml);
cat. no. (92)760-500; Ventana Medical Systems, Inc.] for 40 min at
37˚C. Finally, 3,3'-diaminobenzidine (DAB) was used as the
chromogenic substrate and slides were counterstained with
hematoxylin for 1 min at 20˚C. Commercially available antibodies
against RNF215 (polyclonal; 1:300; product no. Ys-9264R; Shanghai
YaJi Biotechnology Co., Ltd.) and CD34 (clone EPR2999; cat. no.
ab110643; 1:150; Abcam) were used for IHC. Appropriate positive and
negative control slides were included for each antibody. All CRC
images subjected to hematoxylin and eosin (H&E) staining and
IHC were viewed under a light microscope (BX45; Olympus
Corporation).
All immunostaining results were evaluated by two
gastrointestinal pathologists (JBW and XPL). The presence of a
brown color in the cytoplasm and membrane was considered positive
labeling. According to IHC evaluation methods adapted from previous
studies (22), the presence and
degree of RNF215 staining were divided into three categories:
Negative expression, weak expression, and overexpression. The
chi-square test or Fisher's test was conducted to identify the
association between RNF215 expression and clinicopathological
characteristics.
Statistical analysis
Statistical analyses were conducted with R software
(version, 3.6.3) and Graph Prism (version, 9.0; GraphPad Software,
Inc.; Dotmatics). The Wilcoxon rank sum test was used to compare
the expression of RNF215 in CRC tumors with that in normal tissues.
The Wilcoxon rank sum/Kruskal-Wallis test and logistic regression
were performed to demonstrate the association between CRC
clinicopathological characteristics and RNF215 expression. The CRC
clinicopathological features correlated with survival were analyzed
using the Kaplan-Meier method and Cox regression (23). Multivariate Cox analysis was
conducted to assess the effect of RNF215 expression and the other
clinicopathological features on survival. The variables with
P<0.1 in univariate Cox regression analysis were further
assessed in multivariate Cox regression analysis. Two-sided
P-values <0.05 were considered to indicate a statistically
significant difference.
Results
Pancancer and CRC RNF215 expression
analysis
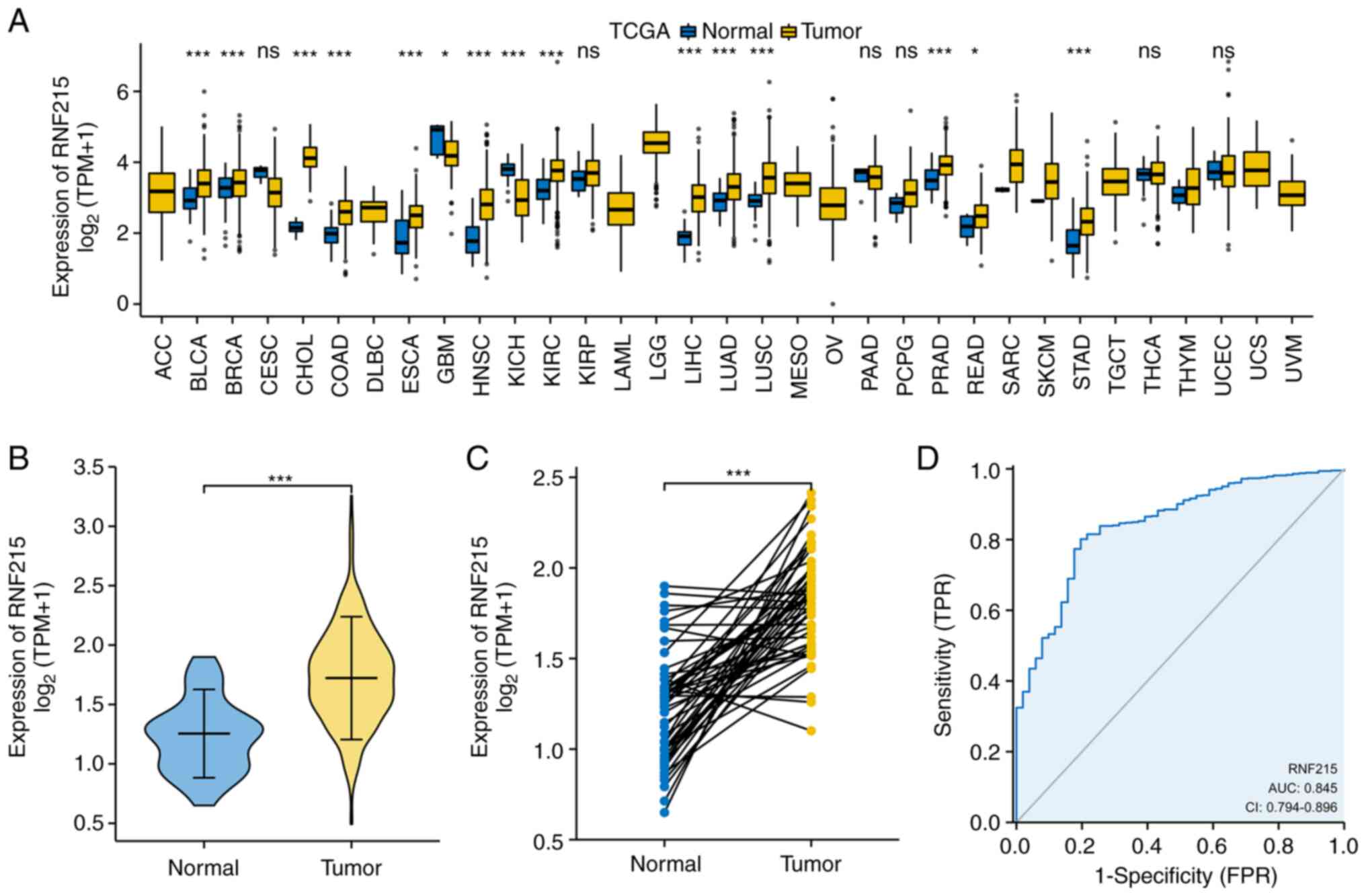
First, RNF215 expression was evaluated based on TCGA
pancancer data. The results indicated that RNF215 expression was
higher in 13 types of tumors than in their paired normal tissues,
including bladder carcinoma (BLCA), breast invasive carcinoma
(BRCA), cholangiocarcinoma (CHOL), colon adenocarcinoma (COAD),
esophageal carcinoma (ESCA), HNSC, kidney renal clear cell
carcinoma (KIRC), liver hepatocellular carcinoma (LIHC), lung
adenocarcinoma (LUAD), lung squamous cell carcinoma (LUSC),
prostate adenocarcinoma (PRAD), rectal adenocarcinoma (READ), and
stomach adenocarcinoma (STAD) (all P<0.05; Fig. 2A). Second, RNF215 expression in 647
CRC samples and 51 paracancerous samples as well as 50 CRC samples
and their paired paracancerous samples were compared. RNF215 was
overexpressed in CRC samples compared with paracancerous tissues
(P<0.001; Fig. 2B and C). The area under the receiver operating
characteristic (ROC) curve (AUC) was 0.845 (95% CI, 0.794-0.896;
P<0.001), which showed that RNF215 had high diagnostic accuracy
for CRC (Fig. 2D).
The abbreviations of TCGA cancers used in the
present study and their paired full names are displayed in Table SI.
DEG analysis in CRC
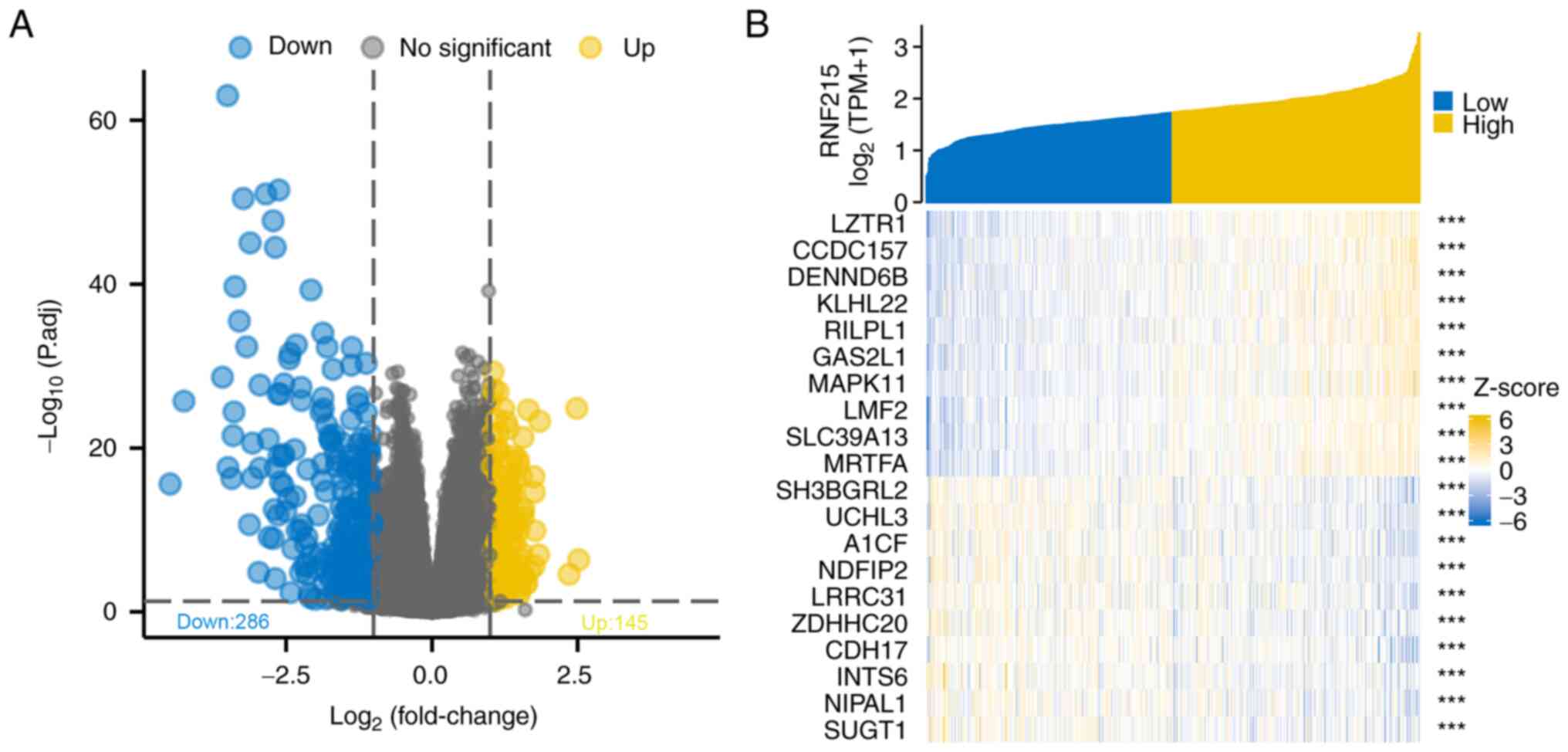
DEG analysis was conducted using cohort data from
TCGA. Based on the RNF215 expression level, the CRC patients were
classified into high and low expression groups. A total of 431 DEGs
were identified by screening, among which 145 were upregulated and
286 were downregulated (Fig. 3A). A
heatmap of gene expression was constructed and the top 10 positive
and 10 negative genes that had the greatest expression differences
in CRC were obtained (Fig. 3B).
Association of RNF215 expression and
clinicopathological characteristics in CRC
A total of 644 primary CRC specimens with clinical
and RNF215 expression data were obtained from TCGA. There were 343
males and 301 females in the cohort with median ages of 69 and 66
years, respectively. Significant differences were identified
between the high- and low-RNF215-expression groups in age
(P=0.001), lymphatic invasion (P=0.017), and OS (P=0.018; Table SII). No other positive associations
were identified between RNF215 expression and other
clinicopathological characteristics. Univariate logistic regression
analysis indicated that the upregulation of RNF215 in CRC was
positively correlated with age (P<0.001) and lymphatic
infiltration (P=0.014) but not with other clinicopathological
features, as shown in Table I.
 | Table IRing finger protein 215 expression is
associated with pathological characteristics (logistic regression)
in colorectal cancer. |
Table I
Ring finger protein 215 expression is
associated with pathological characteristics (logistic regression)
in colorectal cancer.
|
Characteristics | Total (N) | Odds ratio
(OR) | P-value |
|---|
| T stage (T3 and T4
vs. T1 and T2) | 641 | 0.905
(0.616-1.329) | 0.610 |
| N stage (N1 and N2
vs. N0) | 640 | 1.136
(0.831-1.556) | 0.424 |
| M stage (M1 vs.
M0) | 564 | 1.153
(0.733-1.818) | 0.539 |
| Pathologic stage
(stage III and IV vs. stage I and II) | 623 | 1.149
(0.838-1.578) | 0.389 |
| Primary therapy
outcome (PR and CR vs. PD and SD) | 312 | 1.260
(0.637-2.538) | 0.510 |
| Sex (male vs.
female) | 644 | 0.894
(0.655-1.218) | 0.477 |
| Race (Black or
African American and White vs. Asian) | 394 | 1.076
(0.331-3.497) | 0.900 |
| Age (>65 vs.
≤65) | 644 | 0.585
(0.426-0.801) | <0.001 |
| Weight (>90 vs.
≤90) | 348 | 0.896
(0.566-1.420) | 0.641 |
| Height (≥170 vs.
<170) | 329 | 1.082
(0.701-1.669) | 0.722 |
| BMI (≥25 vs.
<25) | 329 | 0.960
(0.604-1.524) | 0.862 |
| Residual tumor (R1
and R2 vs. R0) | 510 | 1.471
(0.779-2.839) | 0.239 |
| CEA level (>5
vs. ≤5) | 415 | 0.915
(0.614-1.363) | 0.661 |
| Perineural invasion
(yes vs. no) | 235 | 1.292
(0.717-2.355) | 0.396 |
| Lymphatic invasion
(yes vs. no) | 582 | 1.522
(1.091-2.128) | 0.014 |
| History of colon
polyps (yes vs. no) | 555 | 1.027
(0.719-1.467) | 0.884 |
| Colon polyps
present (yes vs. no) | 323 | 1.250
(0.778-2.016) | 0.357 |
| Location (colon vs.
rectum) | 644 | 0.878
(0.616-1.250) | 0.471 |
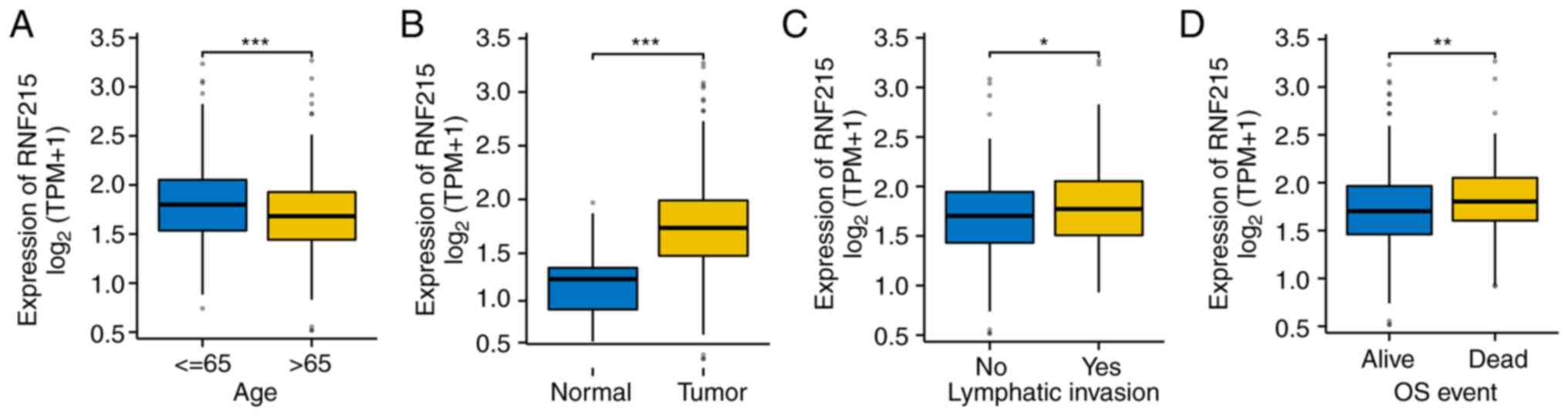
As indicated in Fig.
4, high RNF215 expression was positively correlated with age
(P<0.001), tumor presence (P<0.001), lymphatic invasion
(P<0.05), and OS event (P<0.01).
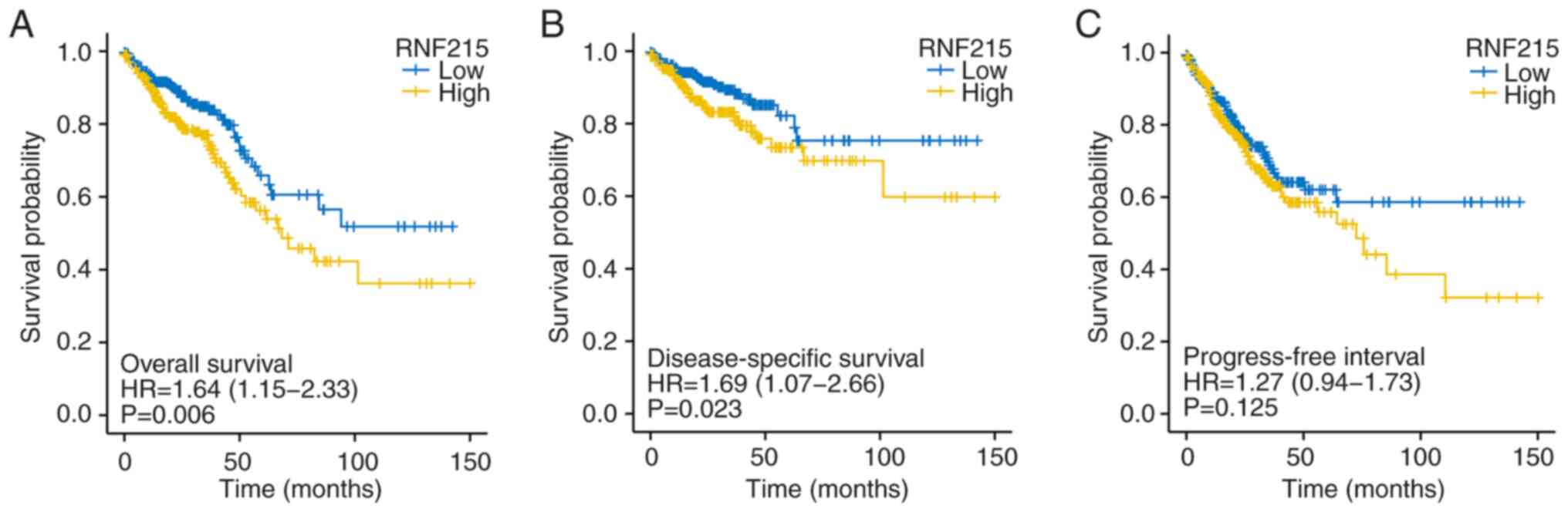
Prognostic role of RNF215 in CRC
patients
To further identify the association between RNF215
expression and CRC prognosis, the survival rates of the high- and
low-RNF215-expression groups were compared. Kaplan-Meier survival
analysis indicated that patients with high RNF215 expression had
poorer OS [median, 20.70 months vs. 24.33 months; HR=1.64
(1.15-2.33); P=0.006], poorer disease-specific survival [DSS;
median, 19.97 months vs. 23.93 months; HR=1.69 (1.07-2.66);
P=0.023], and a shorter progression-free interval [PFI; median,
17.80 months vs. 20.07 months; HR=1.27 (0.94-1.73); P=0.125],
although the PFI difference was not significant (Fig. 5). T stage, N stage, pathological
stage, age, primary therapy outcome, residual tumor, CEA level,
lymphatic invasion, and RNF215 expression were included in the
multivariate Cox analysis. Multivariate analysis revealed that
RNF215 remained independently associated with OS [HR=1.859
(1.254-2.755), P=0.002], as well as other characteristics; the
details are presented in Table
II.
| Table IIUnivariate and multivariate analysis
of clinicopathological characteristics that are correlated with the
overall survival of patients with colorectal cancer. |
Table II
Univariate and multivariate analysis
of clinicopathological characteristics that are correlated with the
overall survival of patients with colorectal cancer.
| | Univariate
analysis | Multivariate
analysis |
|---|
|
Characteristics | Total (N) | Hazard ratio (95%
CI) | P-value | Hazard ratio (95%
CI) | P-value |
|---|
| T stage | | | | | |
|
(T1 and T2
vs. T3 and T4) | 640 | 2.468
(1.327-4.589) | 0.004 | 2.248
(1.017-4.967) | 0.045 |
| N stage | | | | | |
|
(N0 vs. N1
and N2) | 639 | 2.627
(1.831-3.769) | <0.001 | 0.527
(0.201-1.382) | 0.193 |
| M stage | | | | | |
|
(M0 vs.
M1) | 563 | 3.989
(2.684-5.929) | <0.001 | 2.492
(1.540-4.033) | <0.001 |
| Pathologic
stage | | | | | |
|
(stage I and
II vs. stage III and IV) | 622 | 2.988
(2.042-4.372) | <0.001 | 4.142
(1.417-12.104) | 0.009 |
| Age (>65 vs.
≤65) | 643 | 1.939
(1.320-2.849) | <0.001 | 3.179
(2.027-4.986) | <0.001 |
| Sex | | | | | |
| (female vs.
male) | 643 | 1.054
(0.744-1.491) | 0.769 | | |
| Primary therapy
outcome (PD and SD vs. PR and CR) | 312 | 0.109
(0.058-0.202) | <0.001 | 0.084
(0.023-0.314) | <0.001 |
| BMI (≥25 vs.
<25) | 329 | 0.649
(0.394-1.069) | 0.090 | 1.701
(0.351-8.235) | 0.509 |
| Residual tumor (R0
vs. R1 and R2) | 509 | 4.609
(2.804-7.577) | <0.001 | 14.670
(1.230-174.902) | 0.034 |
| CEA level (≥5 vs.
<5) | 414 | 2.620
(1.611-4.261) | <0.001 | 1.840
(0.817-4.145) | 0.141 |
| Perineural invasion
(positive vs. negative) | 235 | 1.692
(0.907-3.156) | 0.099 | 1.496
(0.636-3.520) | 0.356 |
| Lymphatic invasion
(positive vs. negative) | 581 | 2.144
(1.476-3.114) | <0.001 | 2.561
(1.093-6.002) | 0.030 |
| Location (colon vs.
rectum) | 643 | 0.799
(0.519-1.230) | 0.308 | | |
| RNF215 (low vs.
high) | 643 | 1.641
(1.154-2.334) | 0.006 | 1.859
(1.254-2.755) | 0.002 |
Based on the results of the Cox proportional hazards
regression model, T stage, N stage, M stage, TP53 status, age,
lymphatic invasion, and RNF215 expression were selected for
inclusion in the nomogram (Fig.
6A). The concordance index (C-index) of the prognostic model
was 0.777 (0.752-0.803). A calibration plot of the
nomogram-predicted survival probability was constructed to assess
the consistency between the predicted OS and the actual OS, and it
suggested that the nomogram prediction was credible (Fig. 6B).
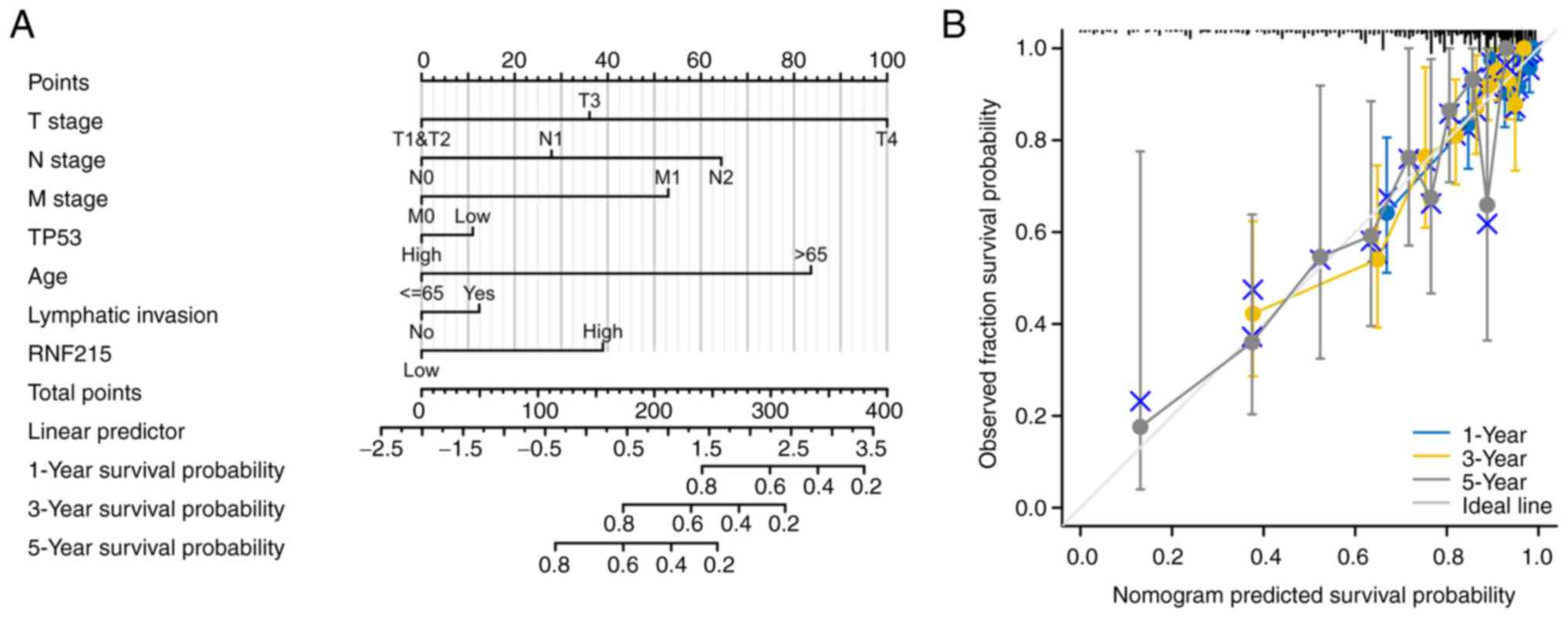 | Figure 6Nomogram and calibration curve. (A)
Nomogram for predicting the probability of 1-, 3-, and 5-year OS
for colorectal cancer patients. T stage, N stage, M stage, TP53
status, age, lymphatic invasion, and ring finger protein 215
expression were selected for inclusion in the nomogram. (B)
Calibration curve of the nomogram for predicting the probability of
OS at 1, 3, and 5 years, indicating the credibility of the
prediction. OS, overall survival; RNF215, ring finger protein
215. |
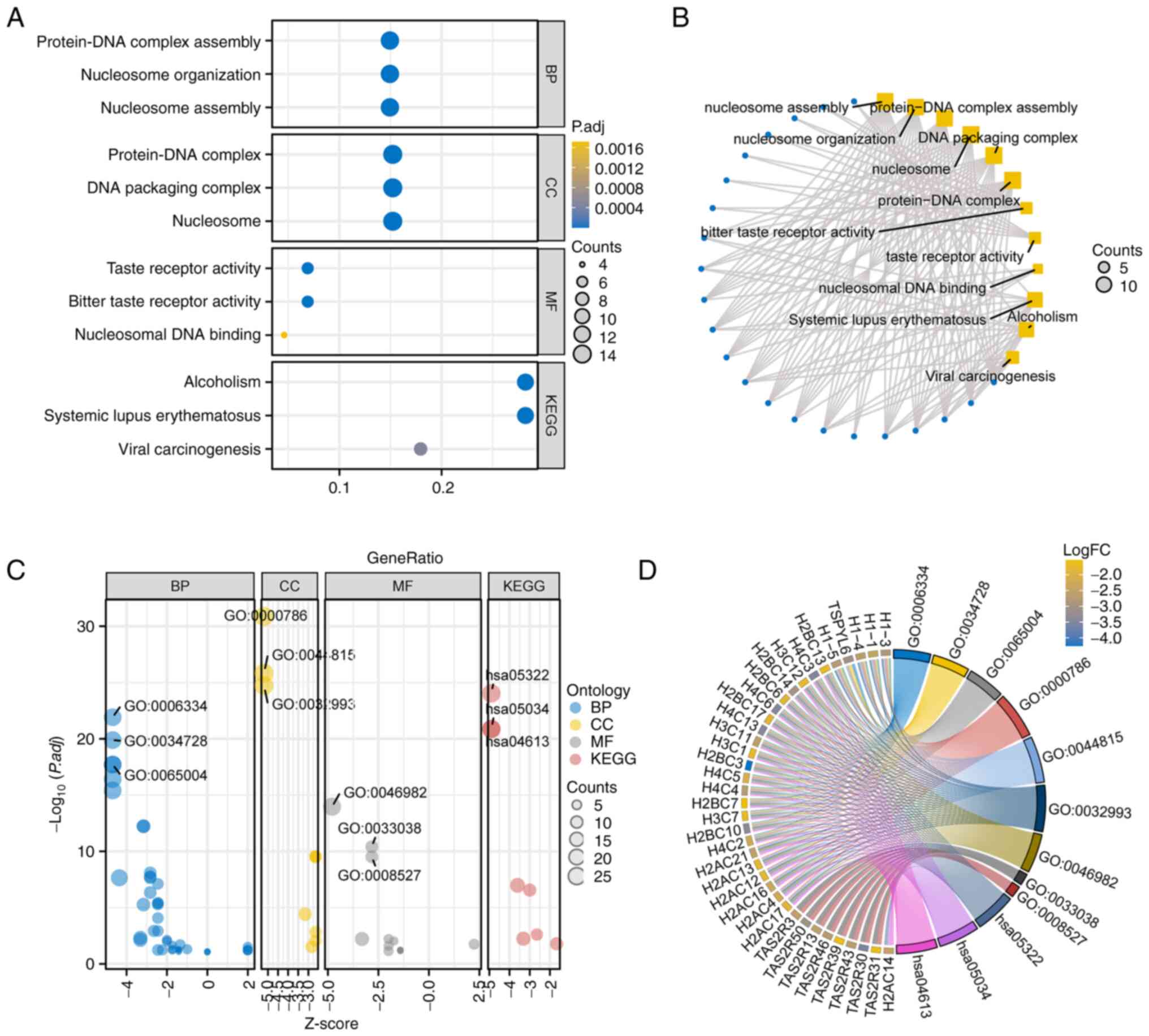
GO and KEGG analyses and PPIs
The function of RNF215 was predicted by GO and KEGG
analyses using the R package clusterProfiler (version, 3.14.3)
(13). According to cutoffs of a
P.adj <0.05 and q-value <0.2, the 96 GO/KEGG items were
divided into four groups: The biological process (BP) group (74
items), the cellular component (CC) group (9 items), the molecular
function (MF) group (7 items), and the KEGG group (6 items); the
details are presented in Table
SIII. GO term analysis for the BP category suggested that
‘nucleosome organization’, ‘chromatin assembly’, and ‘nucleosome
assembly’ were positively enriched. GO term analysis for the CC
category showed that the ‘protein-DNA complex assembly’, ‘DNA
packaging complex’, and ‘nucleosome’ were positively enriched. The
MF analysis showed that ‘taste receptor activity’, ‘bitter taste
receptor activity’, and ‘nucleosomal DNA binding’ were positively
enriched. KEGG analysis suggested that ‘alcoholism’, ‘systemic
lupus erythematosus’, and ‘viral carcinogenesis’ were the most
positively enriched pathways. All the significant GO/KEGG pathways
are presented in Fig. 7A and
B, and the GO/KEGG results combined
with the logFC results are shown in Fig. 7C and D.
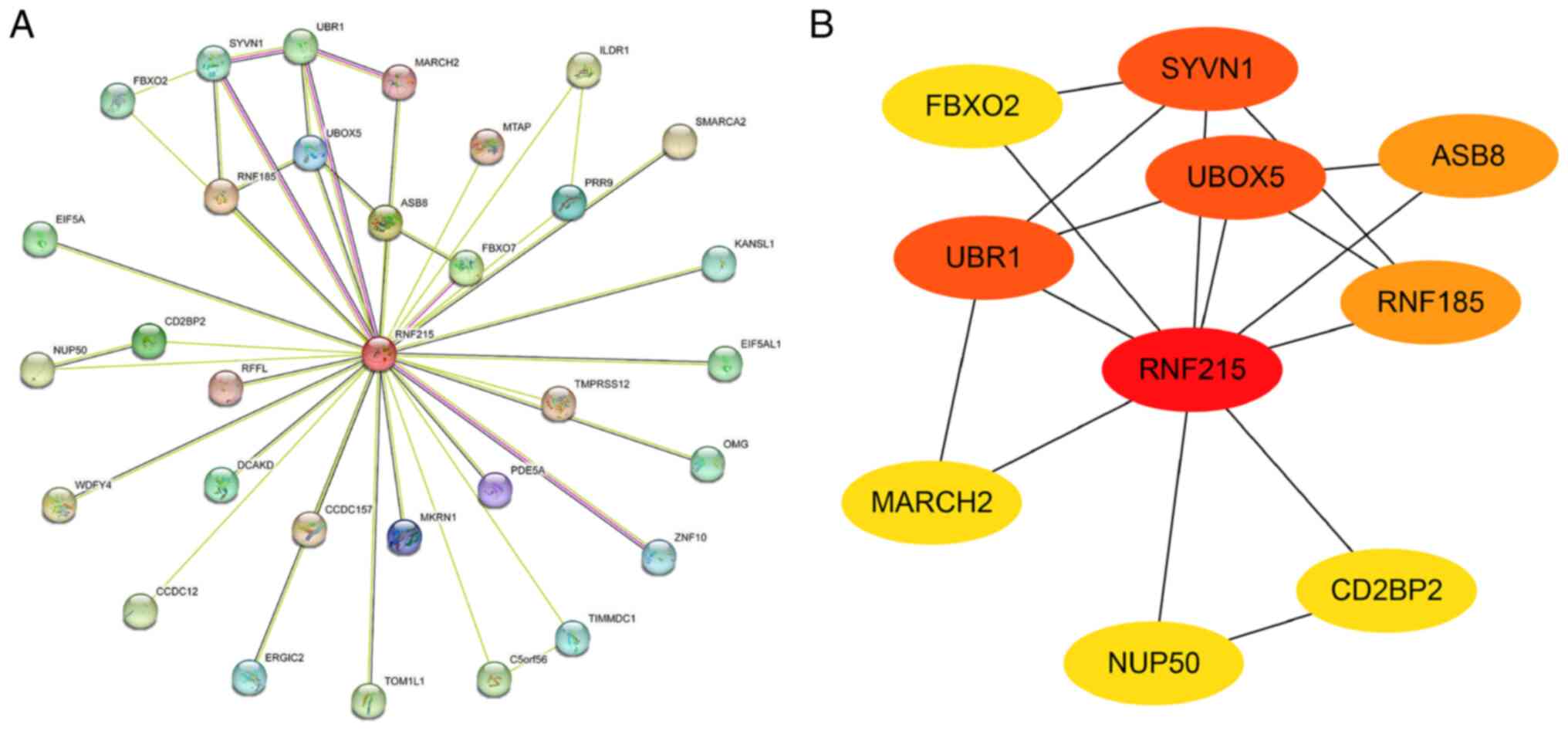
To further identify the possible molecular role of
RNF215 in tumorigenesis, the known RNF215-interacting proteins and
expression-correlated genes were filtered out with the STRING tool
(Fig. 8A). Subsequently, a second
network was constructed using the tsv file and input in Cytoscape
(version, 3.9.1). The top nine hub genes obtained by the maximal
clique centrality (MCC) methods (one of the algorithms in the
plug-in Cytohubba) and according to the node degree was screened,
including FBXO2, SYVN1, UBR1, UBOX5, ASB8, RNF185, MARCH2, NUP50,
and CD2BP2, as shown in Fig. 8B.
Therefore, RNF215 may participate in tumorigenesis by interacting
with these proteins.
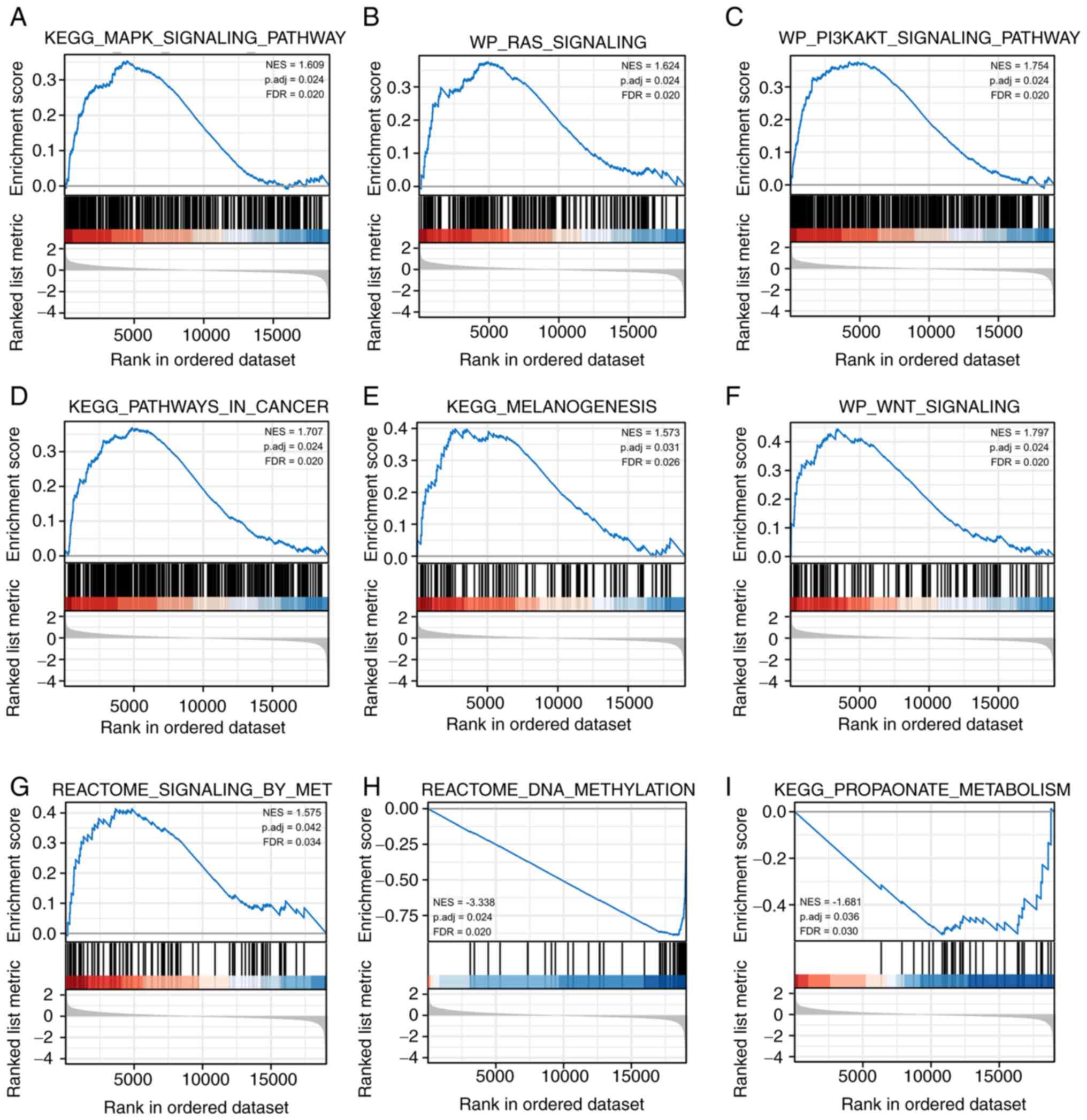
GSEA
To investigate the signaling pathways differentially
activated in CRC, GSEA was then performed on the basis of the
RNF215 low- and high-expression datasets. A total of 318 items
satisfied the conditions of an FDR <0.25 and a P.adj <0.05.
GSEA suggested that RNF215 was involved in several key pathways and
biological processes associated with tumor occurrence, including
the KEGG MAPK signaling pathway (NES=1.609, P.adj=0.024,
FDR=0.020), the WP RAS signaling pathway (NES=1.624, P.adj=0.024,
FDR=0.020), the WP PI3KAKT signaling pathway (NES=1.754,
P.adj=0.024, FDR=0.020), KEGG pathways in cancer (NES=1.707,
P.adj=0.024, FDR=0.020), KEGG melanogenesis (NES=1.573,
P.adj=0.031, FDR=0.026), the WP WNT signaling pathway (NES=1.797,
P.adj=0.024, FDR=0.020), and Reactome signaling by MET (NES=1.575,
P.adj=0.042, FDR=0.034) (Fig.
9A-G). Reactome DNA methylation (NES=-3.338, P.adj=0.024,
FDR=0.020) and KEGG propanoate metabolism (NES=-1.681, P.adj=0.036,
FDR=0.030) were also identified (Fig.
9H and I). The results revealed
that RNF215 may contribute to the development of CRC progression by
participating in some CRC-associated signaling pathways. The
detailed GSEA results are shown in Table SIV.
 | Figure 9Enrichment plots from gene set
enrichment analysis. Some items were enriched in ring finger
protein 215-related colorectal cancer. (A) KEGG MAPK signaling
pathway (NES=1.609, P.adj=0.024, FDR=0.020). (B) WP RAS signaling
pathway (NES=1.624, P.adj=0.024, FDR=0.020). (C) WP PI3KAKT
signaling pathway (NES=1.754, P.adj=0.024, FDR=0.020). (D) KEGG
pathways in cancer (NES=1.707, P.adj=0.024, FDR=0.020). (E) KEGG
melanogenesis (NES=1.573, P.adj=0.031, FDR=0.026). (F) WP WNT
signaling pathway (NES=1.797, P.adj=0.024, FDR=0.020). (G) Reactome
signaling by MET (NES=1.575, P.adj=0.042, FDR=0.034). (H) Reactome
DNA methylation (NES=-3.338, P.adj=0.024, FDR=0.020). (I) KEGG
propanoate metabolism (NES=-1.681, P.adj=0.036, FDR=0.030). KEGG,
Kyoto Encyclopedia of Genes and Genomes; NES, normalized enrichment
score; P.adj, adjusted P-value; FDR, false discovery rate. |
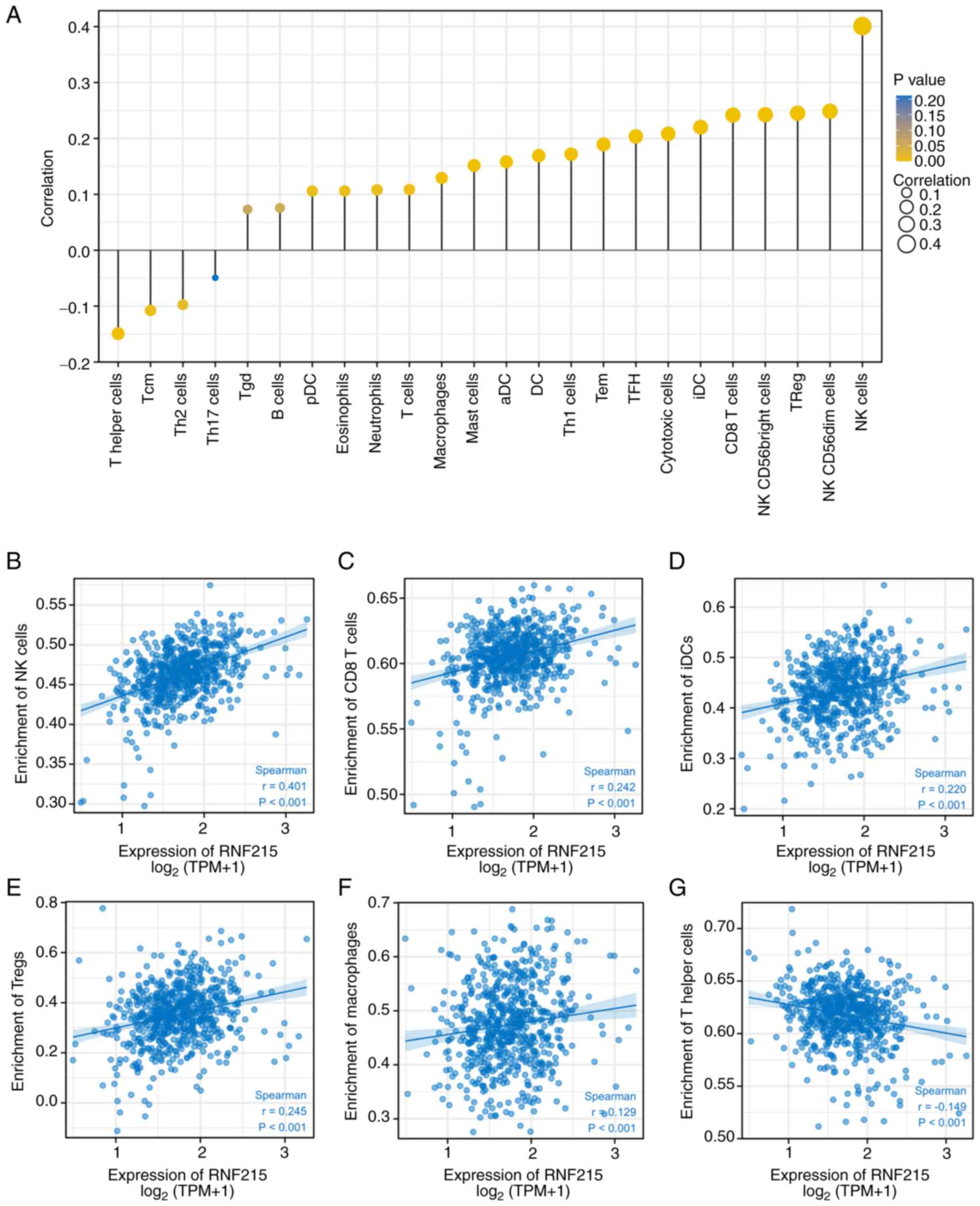
Correlation of RNF215 expression and
immune cell infiltration levels in CRC
The relationship between RNF215 and 24 immune cell
infiltrates quantified by ssGSEA in the CRC microenvironment of
tumors were investigated using Spearman's correlation analysis
(Fig. 10A). RNF215 expression
showed a positive linear correlation with the infiltration levels
of natural killer (NK) cells (r=0.401, P<0.001), CD8 T cells
(r=0.242, P<0.001), Tregs (r=0.245, P<0.001; Fig. 10A-F). RNF215 expression was also
negatively correlated with infiltration of T helper cells
(R=-0.149, P<0.001; Fig. 10G).
These results revealed that RNF215 may regulate immune cell
infiltration in CRC tumors.
Analysis of RNF215 expression and
angiogenesis
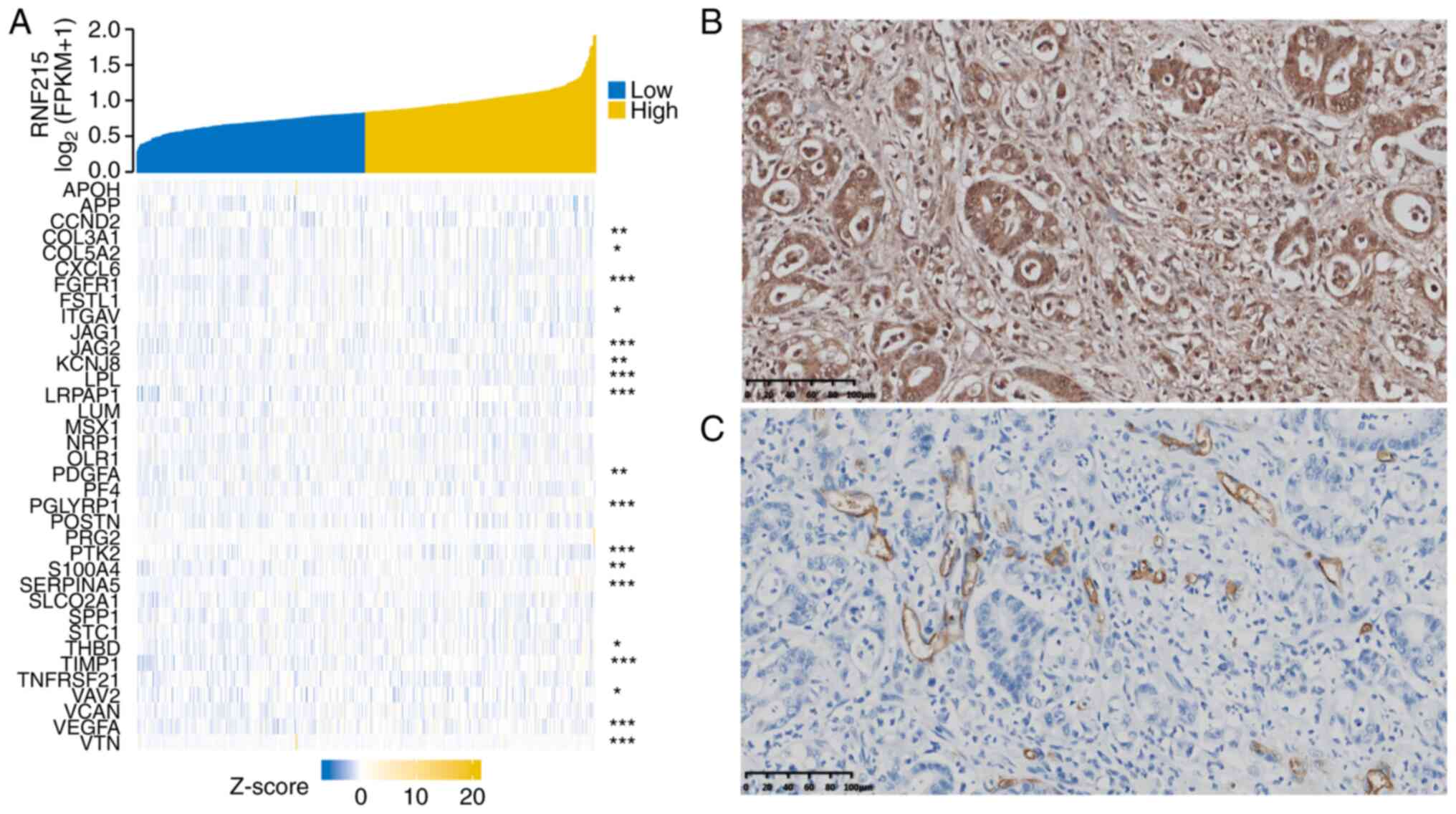
To further clarify the association between RNF215
and angiogenesis, a coexpression analysis between RNF215 and
angiogenesis-associated markers in CRC was performed using the TCGA
dataset, as shown in Fig. 11A. In
addition, 36 angiogenesis-associated genes were acquired from the
MSigDB Team (Hallmark gene set); the details are shown in Table SV. The present study confirmed that
many of the genes involved in angiogenesis (such as APP, COL3A1,
JAG2, PDGFA, S100A4, and VEGFA) were consistent with the trend in
RNF215 expression in CRC. The immunohistochemical results indicated
that RNF215 was present in the vascular tissues around CRC tumors
(Fig. 11B and C), indicating that RNF215 may be involved
in angiogenesis in CRC.
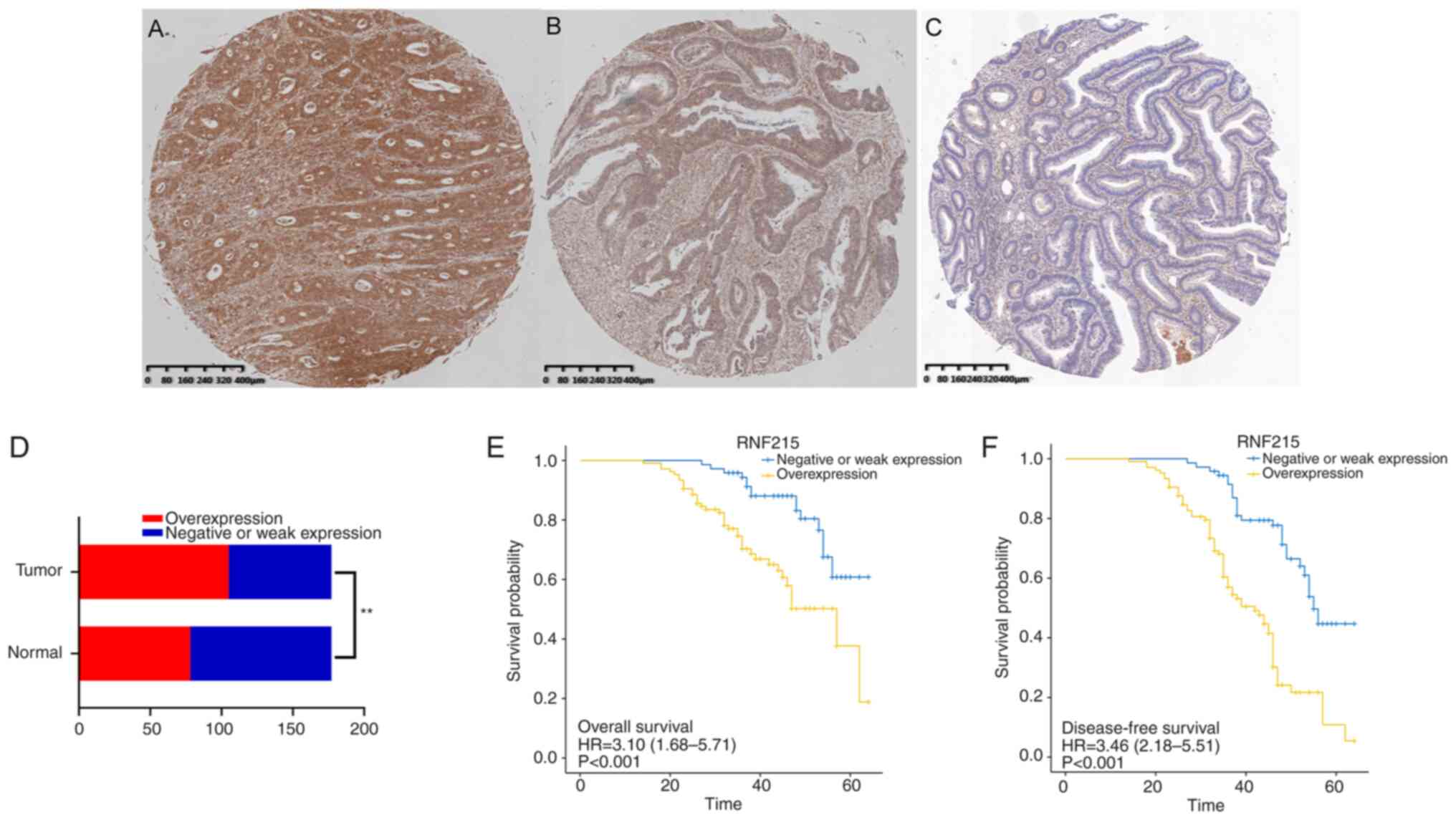
Validation of RNF215 expression by
IHC
IHC was performed on 177 CRC tumor and corresponding
normal tissues obtained from the Department of Pathology, Shanghai
Fifth People's Hospital, Fudan University. Representative images of
RNF215 expression are shown in Fig.
12A-C. The results indicated that RNF215 expression was higher
in CRC tissues than in corresponding normal tissues (P<0.01), as
shown in Fig. 12D. Compared to
patients with CRC with negative or weak RNF215 expression in the
present study, patients with CRC with RNF215 overexpression were
younger, had more lymphatic invasion, and had more distant
metastases (P<0.05). Furthermore, patients with CRC with RNF215
overexpression had poorer OS and DFS than patients with CRC with
negative or weak RNF215 expression (P<0.001), as revealed in
Fig. 12E and F. The clinicopathological details of
RNF215 expression in the patients with CRC are presented in
Table III.
| Table IIIAssociation between RNF215 expression
and clinicopathological characteristics in patients with colorectal
cancer. |
Table III
Association between RNF215 expression
and clinicopathological characteristics in patients with colorectal
cancer.
|
Characteristics | Negative or low
expression of RNF215 | Overexpression of
RNF215 | P-value |
|---|
| n | 72 (%) | 105 (%) | |
| Sex, n (%) | | | 0.3017 |
|
Male | 50 (28.25) | 65 (36.72) | |
|
Female | 22 (12.43) | 40 (22.60) | |
| Age, n (%) | | | 0.0381 |
|
≤65 | 25 (14.12) | 53 (29.94) | |
|
>65 | 47 (26.55) | 52 (29.38) | |
| Localization, n
(%) | | | 0.4815 |
|
Right
colon | 27 (15.25) | 34 (19.21) | |
|
Left
colon | 45 (25.42) | 71 (40.11) | |
| Configuration, n
(%) | | | 0.3046 |
|
Endophytic | 48 (27.12) | 62 (35.03) | |
|
Exophytic | 24 (13.56) | 43 (24.29) | |
| Size, n (%) | | | 0.2314 |
|
≤3.5 cm | 13 (7.34) | 27 (15.25) | |
|
>3.5
cm | 59 (33.33) | 78 (44.07) | |
| Pathologic stage, n
(%) | | | 0.0793 |
|
Stage
I-II | 30 (17.88) | 32 (17.88) | |
|
Stage
III-IV | 42 (23.46) | 73 (40.78) | |
| T stage, n (%) | | | |
|
T1-T2 | 4 (2.26) | 16 (9.04) | 0.0543 |
|
T3-T4 | 68 (38.42) | 89 (50.28) | |
| N stage, n (%) | | | 0.7832 |
|
N0 | 44 (24.86) | 62 (35.03) | |
|
N1-N2 | 28 (15.82) | 43 (24.29) | |
| M stage, n (%) | | | 0.0026 |
|
M0 | 52 (29.38) | 52 (29.38) | |
|
M1 | 20 (11.30) | 53 (29.94) | |
| Perineural
invasion, n (%) | | | 0.7759 |
|
Negative | 50 (28.25) | 75 (42.37) | |
|
Positive | 22 (12.43) | 30 (16.95) | |
| Lymphatic invasion,
n (%) | | | 0.0325 |
|
Negative | 48 (27.12) | 53 (29.94) | |
|
Positive | 24 (13.56) | 52 (29.38) | |
Discussion
RNF215 is a protein-coding gene located in the
membrane or intracellularly. According to GeneCards (https://www.genecards.org/), RNF215 is predicted to
have ubiquitin-protein ligase activity and is involved in Golgi to
vacuolar transport, vacuolar protein targeting, and
ubiquitin-dependent protein decomposition processes. It is also
predicted to be an integral component of the cell membrane, to be
part of the nuclear Golgi transport complex, and to be active in
the endosomes, membranes, and trans-Golgi networks. To date, only a
few studies have been reported on RNF215 (8-10);
however, no studies have reported on the association between RNF215
and CRC.
In the present research, bioinformatics analysis
indicated that the RNF215 expression value in CRC tumor tissues was
higher than that in paired or unpaired normal tissues, suggesting
that RNF215 may play an important role in CRC tumorigenesis and
progression. Moreover, ROC analysis revealed that the AUC for CRC
was 0.845, indicating that RNF215 may be a potential molecular
biomarker. Therefore, the association between RNF215 expression and
clinicopathological features was further explored. High RNF215
expression was positively associated with age (P=0.001), lymphatic
invasion (P=0.017), and OS (P=0.018). Since a role of RNF215 in CRC
progression has not been reported, the clinical role of RNF215 has
not been determined. The prognostic gene signature was first
modeled according to the Kaplan-Meier curve of RNF215, which showed
that it performed well in predicting CRC survival. The present
study revealed poorer OS, DSS, and PFI in CRC patients with high
RNF215 expression, although the PFI difference was not significant.
In addition, the multivariate analysis suggested that RNF215 was an
independent factor affecting CRC survival (P=0.002). According to
the Cox proportional hazards regression results, the prognostic
model had a C-index of 0.777 and was reliable. All these results
indicate that RNF215 may be a potential molecular biomarker of
CRC.
To further investigate the potential value of RNF215
in CRC, GO and KEGG analyses and GSEA were conducted on RNF215. In
GO analysis, BP terms associated with nucleosomes were identified,
including ‘nucleosome organization’, ‘nucleosome assembly’,
‘nucleosome’, ‘nucleosomal DNA binding’ and ‘DNA packaging
complex’. KEGG analysis showed that ‘alcoholism’, ‘systemic lupus
erythematosus’, and ‘viral carcinogenesis’ were the most
significantly enriched pathways. Previous research has revealed
that viral carcinogenesis may participate in the tumorigenesis in
numerous types of cancers, such as cervical and oropharyngeal
cancers (24), Markel cell
carcinoma, and Kaposi sarcoma (25). RNF215 coupled with its coexpressed
genes may be involved in cell signaling and the viral oncogenic
pathway, which in turn may be necessary for the tumorigenesis and
development of CRC.
In GSEA, multiple pathways were positively enriched
and associated with high RNF215 expression, including the KEGG MAPK
signaling pathway, the WP RAS pathway, the WP PI3KAKT signaling
pathway, and KEGG pathways in cancer. Slattery et al
suggested that the MAPK signaling pathway is dysregulated in CRC
(26). In addition, a study by Li
et al has suggested that Mex3a promotes tumorigenesis via
the RAP1/MAPK signaling pathway in CRC (27). Some other studies have investigated
whether dysregulated signaling through RAS/RAF/MEK/ERK is a common
event in CRC (28,29). Kasprzak et al indicated that
the components of the IGF axis may interact directly or indirectly
and that these interactions may be related to activation of the
PI3K/Akt signaling pathway (30).
Furthermore, it has been demonstrated that the ubiquitin ligase
NEDD4 may be an oncogene in endometrial cancer and may stimulate
activation of the IGF-1R/PI3K/Akt signaling pathway (31). Yi et al suggested that the
frequently highly mutated genes in CRC liver metastases were mainly
enriched in gastric acid secretion, biliary secretion, and
melanogenesis (32). Overall, the
data of the present study confirmed that RNF215 may be necessary
for regulating CRC invasion; nevertheless, more research is
required to further elucidate the possible modulatory mechanisms of
RNF215 in CRC. In addition, nine top hub genes (FBXO2, SYVN1, UBR1,
UBOX5, ASB8, RNF185, MARCH2, NUP50, and CD2BP2) were identified to
be associated with RNF215 using STRING and Cytoscape software,
suggesting that these genes may be involved in CRC
carcinogenesis.
Some studies have suggested that the CRC
microenvironment could contribute to changes in immunity during CRC
development (33-35).
In order to explore the immune infiltration in CRC, ssGSEA and
Spearman's correlation analysis based on transcriptomic data was
performed to evaluate the correlations of RNF215 with immune cell
populations. The present study revealed that RNF215 expression was
positively associated with immune cells, including NK cells, NK
CD56dim cells, and neutrophils; these immune cells may play an
important role in CRC tumorigenesis. Some researchers have
postulated that the immune microenvironment and immune-related
mechanisms of tumor cells are important components of tumor
development and tumor treatment efficiency and are closely related
to clinical efficacy (5,20). The findings from the present study
demonstrated that RNF215 participates in the regulation of immune
infiltrates in the local CRC microenvironment. However, a nonbiased
approach is required to further analyze the role and pathway of
RNF215 in CRC immune infiltration.
Another focus of the present research was to
determine the role of RNF215 in CRC angiogenesis. The present study
indicated that in CRC, RNF215 is highly coexpressed with multiple
factors, including APP, COL3A1, JAG2, PDGFA, S100A4 and VEGFA,
which have been confirmed to be necessary for angiogenesis in
various tumors (36-38).
The immunohistochemical results revealed that RNF215 was present in
the vascular tissues around colorectal tumors, suggesting a close
association between RNF215 and vascular development. The angiogenic
process of CRC is complex, and future studies need to further
investigate the value of RNF215 in the targeted adjustment of
angiogenesis in animal models.
To further verify the possible role of RNF215 in
CRC, immunohistochemical analysis was carried out on samples from
177 patients with CRC from the Department of Pathology, Shanghai
Fifth People's Hospital, Fudan University, and the association
between RNF215 expression and clinicopathological features was
estimated. The results revealed significant associations between
RNF215 expression and age, lymphatic invasion, and metastasis,
mostly in line with the TCGA results. The small differences may
have been due to the number of cases or to differences in ethnicity
and geographical location.
Although the present study, to the best of our
knowledge is the first to investigate the correlation between
RNF215 and CRC, there are still several limitations that need to be
recognized. First, the main data in the research was obtained from
TCGA, and immunohistochemical analysis was only conducted to
validate the conclusions. Furthermore, in vitro and in
vivo experimental studies are required. Second, the sample size
of the present study was relatively small; a larger sample size is
needed to improve the reliability of the results, which may affect
the data on the expression of RNF215. Finally, the present research
had limitations inherent to the retrospective research design.
Thus, further prospective studies with large sample sizes are
required to validate the results in the future.
In conclusion, in the present study, comprehensive
bioinformatics analysis and immunohistochemical verification were
mainly conducted. The findings of the present study indicated that
high RNF215 expression is predictive of poor prognosis in CRC.
RNF215 may become a novel biomarker for predicting poor prognosis
and a molecular target for immunotherapy in CRC in the future.
However, the study was limited by a small sample size and a lack of
adequate experimental validation. Thus, studies with larger sample
sizes as well as further cytological, histological, and
experimental animal studies are required to confirm the findings of
the present study.
Supplementary Material
Cancer types from The Cancer Genome
Atlasdatabase.
Association between RNF215 expression
and clinicopathological parameters in patientswith colorectal
cancer from The Cancer Genome Atlas.
Results of GO/KEGG analysis.
Results of ring finger protein 215
gene set enrichment analysis.
Summary of 36 recognized
angiogenesis-associated genes.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the High-level
Professional Physician Training Program of Minhang District,
Shanghai City (grant no. 2020MZYS10).
Availability of data and materials
The public data of the study are available from TCGA
(https://portal.gdc.cancer.gov/). The
other data that support the findings of this study are available
from the corresponding author upon reasonable request.
Authors' contributions
JBW conceptualized the study and its methodology and
wrote and prepared the original draft. HL performed the
immunohistochemical experiments and data analysis. XJL curated the
data and performed statistical analysis. XPL designed the study and
revised the final manuscript. JBW and HL confirm the authenticity
of all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The studies involving human participants were
reviewed and approved by the Ethical Committee of Shanghai Fifth
People's Hospital, Fudan University, Shanghai, China (approval no.
2021071). The patients/participants provided their written informed
consent to participate in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Xia C, Dong X, Li H, Cao M, Sun D, He S,
Yang F, Yan X, Zhang S, Li N and Chen W: Cancer statistics in China
and United States, 2022: Profiles, trends, and determinants. Chin
Med J (Engl). 135:584–590. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Chen W, Zheng R, Baade PD, Zhang S, Zeng
H, Bray F, Jemal A, Yu XQ and He J: Cancer statistics in China,
2015. CA Cancer J Clin. 66:115–132. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mattiuzzi C, Sanchis-Gomar F and Lippi G:
Concise update on colorectal cancer epidemiology. Ann Transl Med.
7(609)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Shang Y, Zhang Y, Liu J, Chen L, Yang X,
Zhu Z, Li D, Deng Y, Zhou Z, Lu B and Fu CG: Decreased E2F2
expression correlates with poor prognosis and immune infiltrates in
patients with colorectal cancer. J Cancer. 13:653–668.
2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Simon K: Colorectal cancer development and
advances in screening. Clin Interv Aging. 11:967–976.
2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kasi PM, Shahjehan F, Cochuyt JJ, Li Z,
Colibaseanu DT and Merchea A: Rising proportion of young
individuals with rectal and colon cancer. Clin Colorectal Cancer.
18:e87–e95. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wu Y, Chen D, Hu Y, Zhang S, Dong X, Liang
H, Liang M, Zhu Y, Tan C, An S, et al: Ring finger protein 215
negatively regulates type I IFN production via blocking NF-κB p65
activation. J Immunol. 209:2012–2021. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ma J, Li R and Wang J: Characterization of
a prognostic four-gene methylation signature associated with
radiotherapy for head and neck squamous cell carcinoma. Mol Med
Rep. 20:622–632. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
McIntosh LA, Marion MC, Sudman M, Comeau
ME, Becker ML, Bohnsack JF, Fingerlin TE, Griffin TA, Haas JP,
Lovell DJ, et al: Genome-wide association meta-analysis reveals
novel juvenile idiopathic arthritis susceptibility loci. Arthritis
Rheumatol. 69:2222–2232. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW,
Shi W and Smyth GK: limma powers differential expression analyses
for RNA-sequencing and microarray studies. Nucleic Acids Res.
43(e47)2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Love MI, Huber W and Anders S: Moderated
estimation of fold change and dispersion for RNA-seq data with
DESeq2. Genome Biol. 15(550)2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yu G, Wang LG, Han Y and He QY:
clusterProfiler: An R package for comparing biological themes among
gene clusters. OMICS. 16:284–287. 2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Walter W, Sánchez-Cabo F and Ricote M:
GOplot: An R package for visually combining expression data with
functional analysis. Bioinformatics. 31:2912–2914. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Subramanian A, Tamayo P, Mootha VK,
Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub
TR, Lander ES and Mesirov JP: Gene set enrichment analysis: A
knowledge-based approach for interpreting genome-wide expression
profiles. Proc Natl Acad Sci USA. 102:15545–15550. 2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Shannon P, Markiel A, Ozier O, Baliga NS,
Wang JT, Ramage D, Amin N, Schwikowski B and Ideker T: Cytoscape: A
software environment for integrated models of biomolecular
interaction networks. Genome Res. 13:2498–2504. 2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
von Mering C, Huynen M, Jaeggi D, Schmidt
S, Bork P and Snel B: STRING: A database of predicted functional
associations between proteins. Nucleic Acids Res. 31:258–261.
2003.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Szklarczyk D, Gable AL, Nastou KC, Lyon D,
Kirsch R, Pyysalo S, Doncheva NT, Legeay M, Fang T, Bork P, et al:
The STRING database in 2021: Customizable protein-protein networks,
and functional characterization of user-uploaded gene/measurement
sets. Nucleic Acids Res. 49 (D1):D605–D612. 2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hänzelmann S, Castelo R and Guinney J:
GSVA: Gene set variation analysis for microarray and RNA-seq data.
BMC Bioinformatics. 14(7)2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Bindea G, Mlecnik B, Tosolini M,
Kirilovsky A, Waldner M, Obenauf AC, Angell H, Fredriksen T,
Lafontaine L, Berger A, et al: Spatiotemporal dynamics of
intratumoral immune cells reveal the immune landscape in human
cancer. Immunity. 39:782–795. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wu JB, Sarmiento AL, Fiset PO, Lazaris A,
Metrakos P, Petrillo S and Gao ZH: Histologic features and genomic
alterations of primary colorectal adenocarcinoma predict growth
patterns of liver metastasis. World J Gastroenterol. 25:3408–3425.
2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Chaves FN, Bezerra TMM, Moraes DC, Costa
SFDS, Silva PGB, Alves APNN, Costa FWG, Bernardes VF and Pereira
KMA: Loss of heterozygosity and immunoexpression of PTEN in oral
epithelial dysplasia and squamous cell carcinoma. Exp Mol Pathol.
112(104341)2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Liu J, Lichtenberg T, Hoadley KA, Poisson
LM, Lazar AJ, Cherniack AD, Kovatich AJ, Benz CC, Levine DA, Lee
AV, et al: An integrated TCGA pan-cancer clinical data resource to
drive high-quality survival outcome analytics. Cell.
173:400–416.e11. 2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hoppe-Seyler K, Bossler F, Braun JA,
Herrmann AL and Hoppe-Seyler F: The HPV E6/E7 oncogenes: Key
factors for viral carcinogenesis and therapeutic targets. Trends
Microbiol. 26:158–168. 2018.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Krump NA and You J: Molecular mechanisms
of viral oncogenesis in humans. Nat Rev Microbiol. 16:684–698.
2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Slattery ML, Mullany LE, Sakoda LC, Wolff
RK, Samowitz WS and Herrick JS: The MAPK-signaling pathway in
colorectal cancer: Dysregulated genes and their association with
MicroRNAs. Cancer Inform. 17(1176935118766522)2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Li H, Liang J, Wang J, Han J, Li S, Huang
K and Liu C: Mex3a promotes oncogenesis through the RAP1/MAPK
signaling pathway in colorectal cancer and is inhibited by
hsa-miR-6887-3p. Cancer Commun (Lond). 41:472–491. 2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Stec R, Bodnar L, Charkiewicz R, Korniluk
J, Rokita M, Smoter M, Ciechowicz M, Chyczewski L, Nikliński J,
Kozłowski W and Szczylik C: K-Ras gene mutation status as a
prognostic and predictive factor in patients with colorectal cancer
undergoing irinotecan- or oxaliplatin-based chemotherapy. Cancer
Biol Ther. 13:1235–1243. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Meador CB and Pao W: Old habits die hard:
Addiction of BRAF-mutant cancer cells to MAP kinase signaling.
Cancer Discov. 5:348–350. 2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kasprzak A, Kwasniewski W, Adamek A and
Gozdzicka-Jozefiak A: Insulin-like growth factor (IGF) axis in
cancerogenesis. Mutat Res Rev Mutat Res. 772:78–104.
2017.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Zhang Y, Goodfellow R, Li Y, Yang S,
Winters CJ, Thiel KW, Leslie KK and Yang B: NEDD4 ubiquitin ligase
is a putative oncogene in endometrial cancer that activates
IGF-1R/PI3K/Akt signaling. Gynecol Oncol. 139:127–133.
2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Yi H, Liao ZW, Chen JJ, Shi XY, Chen GL,
Wu GT, Zhou DY, Zhou GQ, Huang JY, Lian L, et al: Genome variation
in colorectal cancer patient with liver metastasis measured by
whole-exome sequencing. J Gastrointest Oncol. 12:507–515.
2021.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Sharp SP, Avram D, Stain SC and Lee EC:
Local and systemic Th17 immune response associated with advanced
stage colon cancer. J Surg Res. 208:180–186. 2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Tse BCY, Welham Z, Engel AF and Molloy MP:
Genomic, microbial and immunological microenvironment of colorectal
polyps. Cancers (Basel). 13(3382)2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Wang W, Zhong Y, Zhuang Z, Xie J, Lu Y,
Huang C, Sun Y, Wu L, Yin J, Yu H, et al: Multiregion single-cell
sequencing reveals the transcriptional landscape of the immune
microenvironment of colorectal cancer. Clin Transl Med.
11(e253)2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zhang Y, Yang F, Peng X, Li X, Luo N, Zhu
W, Fu M, Li Q and Hu G: Hypoxia constructing the prognostic model
of colorectal adenocarcinoma and related to the immune
microenvironment. Front Cell Dev Biol. 9(665364)2021.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Krämer M, Plum PS, Velazquez Camacho O,
Folz-Donahue K, Thelen M, Garcia-Marquez I, Wölwer C, Büsker S,
Wittig J, Franitza M, et al: Cell type-specific transcriptomics of
esophageal adenocarcinoma as a scalable alternative for single cell
transcriptomics. Mol Oncol. 14:1170–1184. 2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Ambartsumian N, Klingelhöfer J and
Grigorian M: The multifaceted S100A4 protein in cancer and
inflammation. Methods Mol Biol. 1929:339–365. 2019.PubMed/NCBI View Article : Google Scholar
|