Introduction
Valvular heart disease (VHD) is a cardiac condition
that may lead to morbidity and mortality due to heart failure or
sudden death (1-3).
The prevalence of VHD is 3.1% in 1,818 Latinos/Hispanics
individuals in the United States between October 2011 and June 24,
2014(4). A report from South Korea
found that incidence of non-rheumatic valvular heart disease
increased from 70.6 to 110.3/100,000 individuals from 2006 to
2011(5). Patients with VHD may
require cardiac valvular surgery if symptoms are severe or left
ventricle is dysfunction (6).
For those requiring surgical valvular treatment, the
2017 European Society of Cardiology (ESC) guidelines recommend
coronary angiography prior to valvular surgery in the high-risk
patients (7), including patients
with evidence of coronary artery disease or severe mitral
regurgitation and those aged >40 years. There are several
cardiovascular risk factors that may contribute to coronary artery
disease, such as atrial fibrillation, diabetes, obstructive sleep
apnea or dyslipidemia (8-13).
Although coronary angiography is an invasive
procedure with potential adverse side effects, it may be worthwhile
as a means of identifying clinical factors associated with coronary
artery stenosis. Additionally, a history of angina pain or
non-invasive exercise testing for coronary artery disease may not
be sensitive enough to detect stenosis. A study found that 40% of
female patients with diabetes and coronary artery disease do not
have angina chest pain and exercise testing for coronary artery
disease has a sensitivity of 26% (14,15).
Therefore, the present study aimed to evaluate which clinical
factors are predictive of coronary artery stenosis in patients with
high-risk VHD. By using clinical factors other than a history of
angina pain or results from non-invasive tests for coronary
stenosis, physicians may be able to recommend patients who require
valvular heart surgery for coronary angiography prior to valvular
surgery to test for coronary stenosis.
Materials and methods
Subjects
The present retrospective cohort study was conducted
at University Hospital, Khon Kaen University, Thailand. There were
533 patients with a mean age of 59.86 (SD 9.64) and a proportion of
male of 55.35% (295 patients). The inclusion criteria were patients
aged ≥40 years who received cardiac valve surgery and coronary
angiogram prior to cardiac valve surgery. Exclusion criteria
included patients who had prosthetic valves, received emergency
cardiac valve surgery or underwent a reoperation for cardiac valve
surgery. Data were collected between January 2018 and January 2019.
All eligible patients in the study received the standard clinical
treatment for VHD.
Baseline characteristics, co-morbid disease, causes
of VHD and current medications of eligible patients were recorded.
Valvular abnormalities were recorded for those with severe
regurgitation or stenosis by echocardiogram as proposed by a
previous study (6) and causes of
VHD were categorized as follows: Rheumatic heart disease, infective
endocarditis, prolapse, ischemic and degenerative. Coronary
stenosis was defined by a stenosis ≥50% in any coronary artery
prior to cardiac valve surgery.
Statistical analysis
Data are presented as the mean ± SD. Patients were
categorized into two groups based on the presence of coronary
stenosis. Clinical factors predictive of coronary stenosis were
computed using univariate logistic regression analysis. Factors
with P<0.20 were used for stepwise multivariate logistic
regression analysis. Factors with P<0.25 were accepted into the
final model. Hosmer-Lemeshow χ2 was performed to
evaluate goodness of fit for the final model. The significant
numerical predictive factors were calculated for sensitivity and
specificity using the area under a receiver operating
characteristic (ROC) curve. The statistical analyses were performed
using STATA software version 10.1 (College Station). P<0.05 was
considered to indicate a statistically significant difference.
Results
There were 533 patients who met the study criteria;
114 patients (21.38%) had coronary stenosis (Table I). The mean number of coronary
arteries exhibiting stenosis was 2.2±1.05. Patients in the coronary
stenosis group had significantly older mean age (64.31 vs. 58.64
years; P<0.001) and significantly lower estimated glomerular
filtration rate (68.47 vs. 76.81 ml/min/1.73 m2;
P<0.001) than the non-coronary stenosis group. Regarding
co-morbid diseases, the coronary stenosis group had a higher
percentage of diabetes and hypertension (21.93% vs. 9.31%; P=0.001
and 47.37% vs. 18.85%; P<0.001) but a lower proportion of atrial
fibrillation (21.93% vs. 44.15%; P<0.001) than the non-coronary
stenosis group.
 | Table IClinical features of patients with
valvular heart disease who underwent diagnostic coronary
angiography prior to cardiac valve surgery categorized by the
presence of CS. |
Table I
Clinical features of patients with
valvular heart disease who underwent diagnostic coronary
angiography prior to cardiac valve surgery categorized by the
presence of CS.
| Factor | No CS (n=419) | CS (n=114) | P-value |
|---|
| Mean age, years | 58.64 (9.26) | 64.31 (9.70) | <0.001 |
| Male sex (%) | 217 (51.79) | 78 (68.42) | 0.002 |
| Mean body mass
index | 22.57 (4.08) | 23.20 (3.78) | 0.142 |
| Mean eGFR,
ml/min/1.73 m2 | 76.81 (20.61) | 68.47 (23.34) | <0.001 |
| Co-morbidity (%) | | | |
|
Atrial
fibrillation | 185 (44.15) | 25 (21.93) | <0.001 |
|
Diabetes
mellitus | 39 (9.31) | 25 (21.93) | 0.001 |
|
Hypertension | 79 (18.85) | 54 (47.37) | <0.001 |
|
Dyslipidemia | 61 (14.56) | 27 (23.68) | 0.023 |
|
Stroke/TIA | 27 (6.44) | 4 (3.51) | 0.365 |
|
Heart
failure | 136 (32.46) | 44 (38.60) | 0.221 |
| Smoker (%) | 115 (28.47) | 38 (34.23) | 0.243 |
| Valve abnormality
(%) | | | |
|
Aortic
regurgitation | 114 (27.21) | 22 (19.30) | 0.091 |
|
Aortic
stenosis | 155 (36.99) | 43 (37.72) | 0.913 |
|
Mitral
regurgitation | 158 (37.71) | 60 (52.63) | 0.005 |
|
Mitral
stenosis | 191 (45.58) | 16 (14.04) | <0.001 |
|
Tricuspid
regurgitation | 149 (35.56) | 28 (24.56) | 0.033 |
| Mean number of
abnormal valves | 1.83 (0.90) | 1.48 (0.72) | <0.001 |
| Causes of VHD
(%) | | | |
|
Ischemic | 0 (0.00) | 19 (16.67) | <0.001 |
|
Prolapse | 33 (7.88) | 6 (5.26) | 0.421 |
|
Degenerative | 98 (23.39) | 40 (35.09) | 0.016 |
|
Rheumatic
heart disease | 230 (54.89) | 26 (22.81) | <0.001 |
|
Infective
endocarditis | 17 (4.07) | 2 (1.75) | 0.391 |
| Medication (%) | | | |
|
ACEI/ARB | 77 (18.42) | 34 (29.82) | 0.009 |
|
Aspirin | 114 (27.27) | 65 (57.02) | <0.001 |
|
β
blocker | 142 (33.97) | 42 (36.84) | 0.580 |
|
Digoxin | 115 (27.51) | 14 (12.28) | 0.001 |
|
Diuretic | 268 (64.11) | 51 (44.74) | <0.001 |
|
Warfarin | 176 (42.11) | 19 (16.67) | <0.001 |
Coronary stenosis group had more patients with
mitral regurgitation (52.63 vs. 37.71%; P=0.005) but fewer patients
with tricuspid regurgitation (24.56 vs. 35.56%; P=0.033) and mitral
stenosis (14.04 vs. 45.58%; P<0.001) than the non-coronary
stenosis group. The coronary stenosis group had a greater
occurrence of degenerative causes of VHD (35.09%; P=0.016), while
the non-coronary stenosis group had more patients with rheumatic
heart disease (54.89%; P<0.001). The coronary stenosis group had
a higher proportion of patients receiving
angiotensin-converting-enzyme inhibitor/angiotensin receptor
blocker (ACEI/ARB) and aspirin therapy than the non-coronary
stenosis group (29.82% vs. 18.42%; P=0.009). Patients with
rheumatic heart disease had a significantly lower mean age than
those without (56.07 vs. 63.35 years; P<0.001), while patients
with ischemic VHD had slightly older age than those with
non-ischemic VHD (62.63 vs. 59.75 years; P=0.202).
Factors included in the stepwise logistic regression
analysis were age, sex, body mass index, estimated glomerular
filtration rate, atrial fibrillation, diabetes mellitus,
hypertension, dyslipidemia, rheumatic heart disease, mitral
regurgitation, mitral stenosis, tricuspid regurgitation and history
of smoking, heart failure and stroke/TIA. There were eight factors
included in the final model predictive of coronary stenosis
(Table II). A total of six factors
were significant risk factors for coronary stenosis. Of these, four
factors were positively associated with coronary stenosis, namely
age, male sex, mitral regurgitation and hypertension, while two
factors were negatively associated with coronary stenosis, namely
estimated glomerular filtration rate and rheumatic heart disease.
Hypertension had the highest adjusted odds ratio at 2.596 (95%
confidence interval of 1.574, 4.280; P<0.05), while both high
estimated glomerular filtration rate and rheumatic heart disease
had adjusted odds ratios of 0.985 (95% confidence interval of
0.981, 0.997; P<0.05). The Hosmer-Lemeshow χ2 value
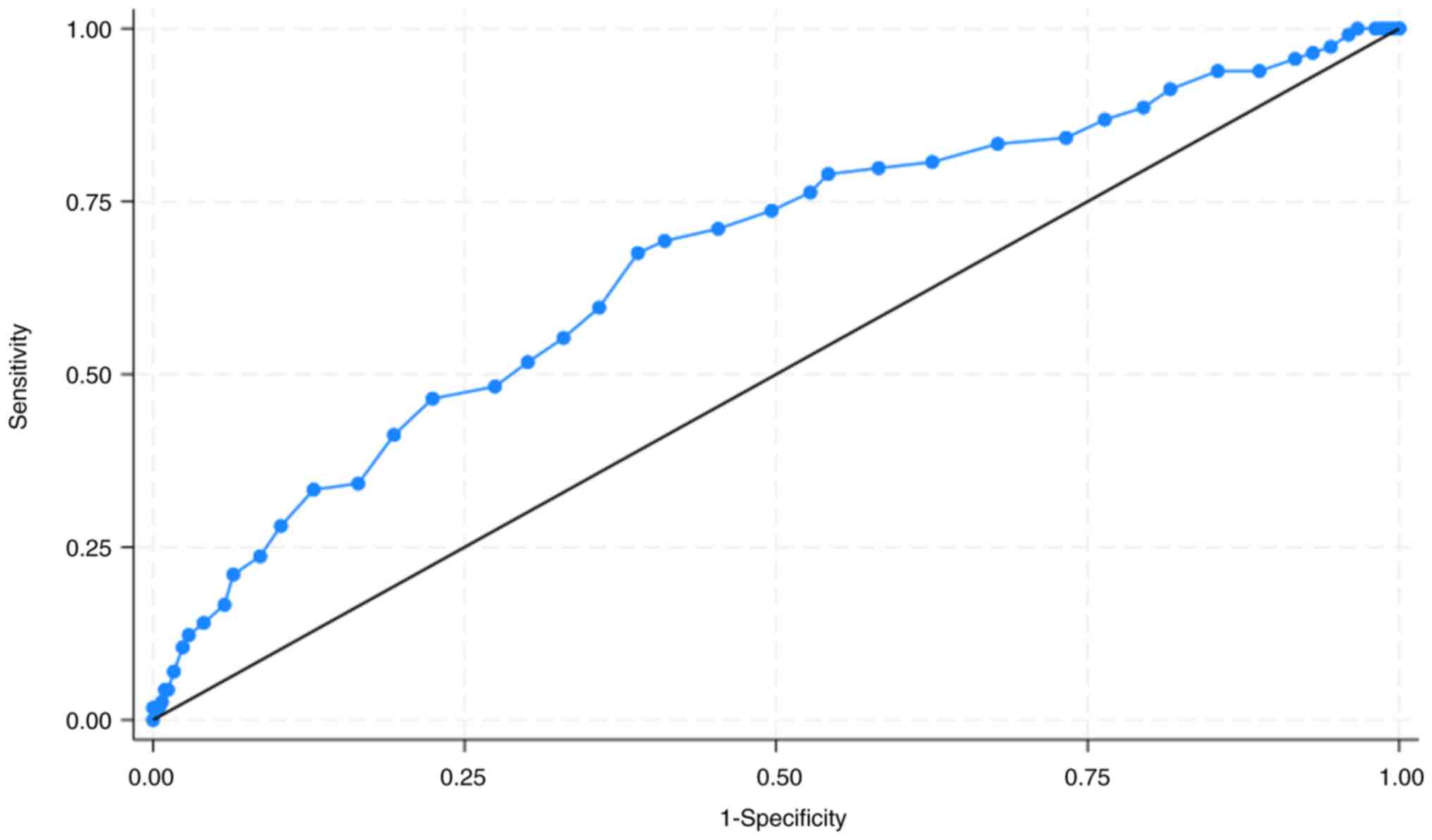
of the final model was 8.64 (P=0.374; data not shown). Patient age
>55 years had a sensitivity and specificity of coronary stenosis
of 80.70 and 37.47%, respectively. The area under ROC curve was
66.45% (95% confidence interval, 60.69, 72.21; Fig. 1).
| Table IIClinical factors predictive of
coronary stenosis in patients with valvular heart disease patients
who received diagnostic coronary angiography prior to cardiac valve
surgery. |
Table II
Clinical factors predictive of
coronary stenosis in patients with valvular heart disease patients
who received diagnostic coronary angiography prior to cardiac valve
surgery.
| Factor | Unadjusted odds ratio
(95% confidence interval) | Adjusted odds ratio
(95% confidence interval) |
|---|
| Age | 1.066 (1.041,
1.091) | 1.038 (1.009,
1.068)a |
| Male sex | 2.016 (1.300,
3.128) | 2.210 (1.340,
3.646)a |
| Body mass
index | 1.038 (0.987,
1.092) | 1.041 (0.981,
1.105) |
| eGFR | 0.980 (0.970,
0.991) | 0.985 (0.981,
0.997)a |
| Atrial
fibrillation | 0.355 (0.219,
0.576) | 0.584 (0.321,
1.059) |
| Mitral
regurgitation | 1.835 (1.209,
2.786) | 1.878 (1.160,
3.041)a |
| Hypertension | 3.873 (2.490,
6.024) | 2.596 (1.574,
4.280)a |
| Rheumatic heart
disease | 0.242 (0.150,
0.391) | 0.985 (0.981,
0.997)a |
Discussion
The present study showed a prevalence of coronary
stenosis in patients with VHD of 21.38%, which was lower than a
previous report from Lebanon (27.75%) (16). These differences may be due to a
different study population (17).
Unlike the report from Lebanon, the present study did not find
significant differences in aortic stenosis. The aforementioned
report showed that severe aortic stenosis is the most common form
of VHD associated significant coronary stenosis (16). The present study found mitral
regurgitation was the most common type of VHD associated with CAD
and was independently associated with significant coronary
stenosis, as previously reported (7).
Other than mitral regurgitation, the present study
showed predictors for coronary stenosis in VHD were age, sex,
estimated glomerular filtration rate, hypertension and rheumatic
heart disease. Certain cardiovascular risk factors included in the
analysis were not retained in the final model, such as atrial
fibrillation, diabetes and dyslipidemia. As previously reported,
age, male sex and hypertension were associated with coronary artery
disease (18-21),
while low glomerular filtration rate may increase risk of coronary
artery disease (22). A previous
study found that age and male sex have an adjusted odds ratio of
1.0560 and 2.6003, which were comparable to those found in the
present study (23). The 2017 ESC
guidelines recommend pre-operative coronary angiogram in patients
with VHD aged >40 years (7);
here, patient age >55 years had a sensitivity of 80%.
Rheumatic heart disease was negatively associated
with coronary stenosis. Even though a previous study found that
mitral regurgitation is the most common type of rheumatic heart
disease (24), only 101 patients in
the present study had mitral regurgitation from rheumatic heart
disease (39.45%). The aforementioned negative association may be
explained by patient age since mitral regurgitation was negatively
associated with age (coefficient of -0.188) (24). Patients with rheumatic heart disease
may be younger and therefore at a lower risk for coronary artery
disease. Here, patients with rheumatic heart disease had a
significantly lower mean age than those without. A study from
Brazil found that only 4% of patients with rheumatic heart disease
have coronary artery disease compared with 33.61% of patients
without rheumatic heart disease (25). A study from China found that
patients with rheumatic heart disease undergoing valvular surgery
for coronary artery disease are older than those without coronary
artery disease (63 vs. 54 years; P<0.01) (26). Although the mean age of the present
study was comparable with the aforementioned studies, the present
study found that rheumatic heart disease was protective factor for
coronary stenosis in patients who underwent valvular surgery.
Risk factors for coronary stenosis in patients with
VHD include male sex, age >55 years, hypertension and low
estimated glomerular filtration rate. Those with rheumatic heart
disease may be at a lower risk of coronary artery disease. Finally,
these risk factors were identified independently of chest pain or
other non-invasive exercise testing for coronary artery disease.
Physicians may consider these risk factors when deciding on
pre-operative coronary angiography prior to cardiac valve surgery
in patients with VHD who are aged >40 years, regardless of
history of angina pain or non-invasive exercise testing for
coronary artery disease.
There are limitations in the present study. First,
the present study population was a single, referral, university
hospital resulting in small sample size. An interpretation of the
results should be performed cautiously as the logistic model may
lack sufficient power. The trace back power of the dataset was
99.7%. Second, certain factors for coronary artery disease were not
included such as obstructive sleep apnea (27-34).
Clinicians may use the model as a guide to evaluate the risk of
coronary stenosis. Finally, the prevalence of rheumatic heart
disease was high (48.03%). The results of this study may be
applicable for populations with a similar prevalence of rheumatic
heart disease. The primary outcome of this study was presence of
coronary stenosis of >50%, not the percentage of coronary
stenosis. The presence of significant coronary stenosis may be more
clinical relevant than the percentage of coronary stenosis as the
guideline recommends coronary bypass graft surgery prior to heart
valve surgery if coronary stenosis is over 50% (7).
Clinical factors predictive of coronary stenosis in
patients with high-risk VHD were age >55 years, male sex, mitral
regurgitation and hypertension, while high estimated glomerular
filtration rate and rheumatic heart disease were protective
factors. Patients who are identified as higher risk based on these
risk factors should be considered for coronary angiogram prior to
cardiac valve surgery.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
SW and KS conceived and designed the study. DK and
VC interpreted data. KS performed statistical analysis. All authors
have read and approved the final manuscript. SW and DK confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board at the Ethical Committee of Khon Kaen University,
Thailand (approval no. HE591473.) The requirement for informed
consent was waived due to the retrospective nature of the
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rizzi MA, Sarasola AG, Arbé AA, Mateo SH,
Gil V, Llorens P, Jacob J, Martín-Sánchez FJ, Puente PH, Escoda R,
et al: Factors associated with in-hospital mortality and adverse
outcomes during the vulnerable post-discharge phase after the first
episode of acute heart failure: Results of the NOVICA-2 study. Clin
Res Cardiol. 110:993–1005. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Noubiap JJ, Nyaga UF, Ndoadoumgue AL,
Nkeck JR, Ngouo A and Bigna JJ: Meta-Analysis of the incidence,
prevalence, and correlates of atrial fibrillation in rheumatic
heart disease. Glob Heart. 15(38)2020.PubMed/NCBI View
Article : Google Scholar
|
|
3
|
Henriques de Gouveia RHAM and Corte Real
Gonçalves FMA: Sudden cardiac death and valvular pathology.
Forensic Sci Res. 4:280–286. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Rubin J, Aggarwal SR, Swett KR, Kirtane
AJ, Kodali SK, Nazif TM, Pu M, Dadhania R, Kaplan RC and Rodriguez
CJ: Burden of valvular heart diseases in hispanic/latino
individuals in the United States: The echocardiographic study of
latinos. Mayo Clin Proc. 94:1488–1498. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Jang SY, Ju EY, Seo SR, Choi JY, Park SJ,
Kim DK and Park SW: Changes in the etiology of valvular heart
disease in the rapidly aging Korean population. Int J Cardiol.
174:355–359. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Brinkley DM and Gelfand EV: Valvular heart
disease: Classic teaching and emerging paradigms. Am J Med.
126:1035–1042. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Falk V, Baumgartner H, Bax JJ, De Bonis M,
Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Muñoz DR, et al:
2017 ESC/EACTS Guidelines for the management of valvular heart
disease. Eur J Cardiothorac Surg. 52:616–664. 2017.
|
|
8
|
Khamsai S, Chootrakool A, Limpawattana P,
Chindaprasirt J, Sukeepaisarnjaroen W, Chotmongkol V, Silaruks S,
Senthong V, Sittichanbuncha Y, Sawunyavisuth B and Sawanyawisuth K:
Hypertensive crisis in patients with obstructive sleep
apnea-induced hypertension. BMC Cardiovasc Disord.
21(310)2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Soontornrungsun B, Khamsai S,
Sawunyavisuth B, Limpawattana P, Chindaprasirt J, Senthong V,
Chotmongkol V and Sawanyawisuth K: Obstructive sleep apnea in
patients with diabetes less than 40 years of age. Diabetes Metab
Syndr. 14:1859–1863. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Khamsai S, Mahawarakorn P, Limpawattana P,
Chindaprasirt J, Sukeepaisarnjaroen W, Silaruks S, Senthong V,
Sawunyavisuth B and Sawanyawisuth K: Prevalence and factors
correlated with hypertension secondary from obstructive sleep
apnea. Multidiscip Respir Med. 16(777)2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Khamsai S, Kachenchart S, Sawunyavisuth B,
Limpawattana P, Chindaprasirt J, Senthong V, Chotmongkol V,
Pongkulkiat P and Sawanyawisuth K: Prevalence and risk factors of
obstructive sleep apnea in hypertensive emergency. J Emerg Trauma
Shock. 14:104–107. 2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Manasirisuk P, Chainirun N, Tiamkao S,
Lertsinudom S, Phunikhom K, Sawunyavisuth B and Sawanyawisuth K:
Efficacy of generic atorvastatin in a real-world setting. Clin
Pharmacol Adv Appl. 13:45–51. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Sanlung T, Sawanyawisuth K, Silaruks S,
Khamsai S, Limpawattana P, Chindaprasirt J, Senthong V, Kongbunkiat
K, Timinkul A, Phitsanuwong C, et al: Clinical characteristics and
complications of obstructive sleep apnea in srinagarind hospital. J
Med Assoc Thai. 103(36)2020.
|
|
14
|
Krul MM, Bogaard K, Knol RJ, van Rossum
AC, Knaapen P, Cornel JH and van der Zant FM: Coronary artery
disease in patients with atypical chest pain with and without
diabetes mellitus assessed with coronary CT angiography. BMJ Open
Diabetes Res Care. 2(e000004)2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Goldkorn R, Naimushin A, Shlomo N, Dan A,
Oieru D, Moalem I, Rozen E, Gur I, Levitan J, Rosenmann D, et al:
Comparison of the usefulness of heart rate variability versus
exercise stress testing for the detection of myocardial ischemia in
patients without known coronary artery disease. Am J Cardiol.
115:1518–1522. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Matta A and Moussallem N: Coronary artery
disease is associated with valvular heart disease, but could it Be
a predictive factor? Indian Heart J. 71:284–287. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Rostomian AH, Soverow J and Sanchez DR:
Exploring Armenian Ethnicity as an independent risk factor for
cardiovascular disease: Findings from a prospective cohort of
patients in a County Hospital. JRSM Cardiovasc Dis.
9(2048004020956853)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Yu YT, Hou ZH, Lu B, An YQ, Gao Y, Yin WH
and Ren XS: Prevalence of coronary artery disease in symptomatic
patients with zero coronary artery calcium score in different age
population. Int J Cardiovasc Imaging. 37:723–729. 2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Faber M, Will A, Hendrich E, Martinoff S
and Hadamitzky M: Sex- and age-specific differences in the
long-term prognostic value of morphological plaque features
detected by coronary computed tomography angiography. J Cardiovasc
Comput Tomogr. 15:274–280. 2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Manfrini O, Yoon J, van der Schaar M,
Kedev S, Vavlukis M, Stankovic G, Scarpone M, Miličić D, Vasiljevic
Z, Badimon L, et al: Sex differences in modifiable risk factors and
severity of coronary artery disease. J Am Heart Assoc.
9(e017235)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Whelton SP, McEvoy JW, Shaw L, Psaty BM,
Lima JAC, Budoff M, Nasir K, Szklo M, Blumenthal RS and Blaha MJ:
Association of normal systolic blood pressure level with
cardiovascular disease in the absence of risk factors. JAMA
Cardiol. 5:1011–1018. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Shroff GR, Sanchez OA, Miedema MD, Kramer
H, Ix JH, Duprez DA and Jacobs DR Jr: Coronary artery calcium
progresses rapidly and discriminates incident cardiovascular events
in chronic kidney disease regardless of diabetes: The Multi-Ethnic
Study of Atherosclerosis (MESA). Atherosclerosis. 310:75–82.
2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Sharma K, Singhal R, Jadhav N, Shah K and
Patil S: Evaluation of SERENE-CAG score for assessing suitability
for coronary angiography preoperatively in patients undergoing
valve replacement surgery. Indian Heart J. 70 (Suppl 3):S189–S193.
2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Butt HI, Shahbaz A, Nawaz H and Butt K:
Comparative clinical characteristics of rheumatic heart disease
patients undergoing surgical valve replacement. Cureus.
11(e4889)2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Li BL, Li L, Hou XL, He B, Zhang GX, Chen
KB and Xu ZY: Prevalence of coronary artery disease in patients
with rheumatic heart disease in China. Zhonghua Yi Xue Za Zhi.
87:3313–3316. 2007.PubMed/NCBI(In Chinese).
|
|
26
|
Kruczan DD, Silva NA, Pereira Bde B, Romão
VA, Correa Filho WB and Morales FE: Coronary artery disease in
patients with rheumatic and non-rheumatic valvular heart disease
treated at a public hospital in Rio de Janeiro. Arq Bras Cardiol.
90:197–203. 2008.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Perera A, Mudannayake SD, Azamathulla HM
and Rathnayake U: Recent climatic trends in Trinidad and Tobago,
West Indies. Asia-Pac J Sci Technol. 25(25)2020.
|
|
28
|
Jeerasuwannakul B, Sawunyavisuth B,
Khamsai S and Sawanyawisuth K: Prevalence and risk factors of
proteinuria in patients with type 2 diabetes mellitus. Asia-Pac J
Sci Technol. 26(26)2021.
|
|
29
|
Suebsamran P, Aekplakorn W, Chamnan P,
Bumrerraj S, Kuhiranyaratn P and Kessomboon P: Association of body
mass index and other factors with metabolically unhealthy status:
Results from the national health examination survey IV. Asia-Pac J
Sci Technol. 26(26)2021.
|
|
30
|
Sawunyavisuth B: What are predictors for a
continuous positive airway pressure machine purchasing in
obstructive sleep apnea patients? Asia-Pac J Sci Technol.
23:APST–23. 2018.
|
|
31
|
Sawunyavisuth B, Ngamjarus C and
Sawanyawisuth K: Any effective intervention to improve CPAP
adherence in children with obstructive sleep apnea: A systematic
review. Glob Pediatr Health. 8(2333794X211019884)2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Hlaing SS, Puntumetakul R, Wanpen S and
Saiklang P: Updates on core stabilization exercise and
strengthening exercise: A review article. Asia-Pac J Sci Technol.
26:APST–26. 2021.
|
|
33
|
Kaewkes C, Sawanyawisuth K and
Sawunyavisuth B: Are symptoms of obstructive sleep apnoea related
to good continuous positive airway pressure compliance? ERJ Open
Res. 6:00169–02019. 2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sawunyavisuth B: What personal experiences
of CPAP use affect CPAP adherence and duration of CPAP use in OSA
patients? J Med Assoc Thai. 101(S245)2018.
|