Introduction
Although laparoscopic surgery has become a popular
surgical option given its reduced burden on the patient, studies
have noted the occurrence of work-related musculoskeletal disorders
(WMSD) due to laparoscopic surgery (1,2). WMSD
of surgeons is prevalent, with rates ranging from 66 to 94% for
open surgery and from 73 to 100% for conventional laparoscopy. In
open surgery, WMSD is due to musculoskeletal posture, especially
involving the neck (1,3). Open surgeries are associated with
larger neck angles compared with laparoscopic surgeries. There are
also risk factors in open surgery such as the use of loupes,
headlamps and microscopes, whereas in laparoscopic surgery, in
developing WMSD, the estimated unique risk factors include table
and monitor position, long-shafted instruments, poor instrument
handle design, the small hands of surgeons and increased patient
body mass index (BMI) (4).
Bell-land General Hospital (Sakai, Japan) uses
laparoscopic coagulation shears (LCS) as an energy device for
gynecological laparoscopic surgery. Harmonic ACE® shears
(Ethicon US, LLC; Johnson and Johnson MedTech) with a shaft length
of 36-cm are usually used as the LCS when performing total
laparoscopic hysterectomy, despite some gynecological surgeons
stating that a short-shafted (i.e., a 20-cm LCS) is more useful
(5), as it helps surgeons
effortlessly maintain their shoulder position during gynecological
laparoscopic surgery. However, no reports have objectively
evaluated the benefits of using a short-shafted energy device for
gynecological laparoscopic surgery. In laparoscopic surgery, the
motion of the surgeon is restricted by the positioning of the
abdominal ports, and depends on table and monitor position, shaft
length of the instruments and instrument handle design, among other
factors (1,3). The ergonomic evaluation of a surgeon's
motion in laparoscopic surgery is considered to be meaningful, but
remains unknown without actual measurements. The present study
attempted to qualitatively capture surgeon discomfort and strain
when comparing differences between using two different instrument
lengths.
The present study investigated whether differences
in the range of motion of the face, neck, right shoulder, right
elbow and right wrist existed when using an LCS with a short 20-cm
shaft and a conventional 36-cm shaft during a gynecological
laparoscopic surgery, based on images analyzed using artificial
intelligence (AI).
Materials and methods
Laparoscopy
A 20-cm short-shafted Harmonic HD®
(Ethicon US, LLC; Johnson and Johnson MedTech) and a 36-cm
long-shafted Harmonic ACE (Ethicon US, LLC; Johnson and Johnson
MedTech) were switched between halfway through the dissection of
the right-sided uterine broad ligament, with the surgeon's actions
being video recorded (Fig. 1).
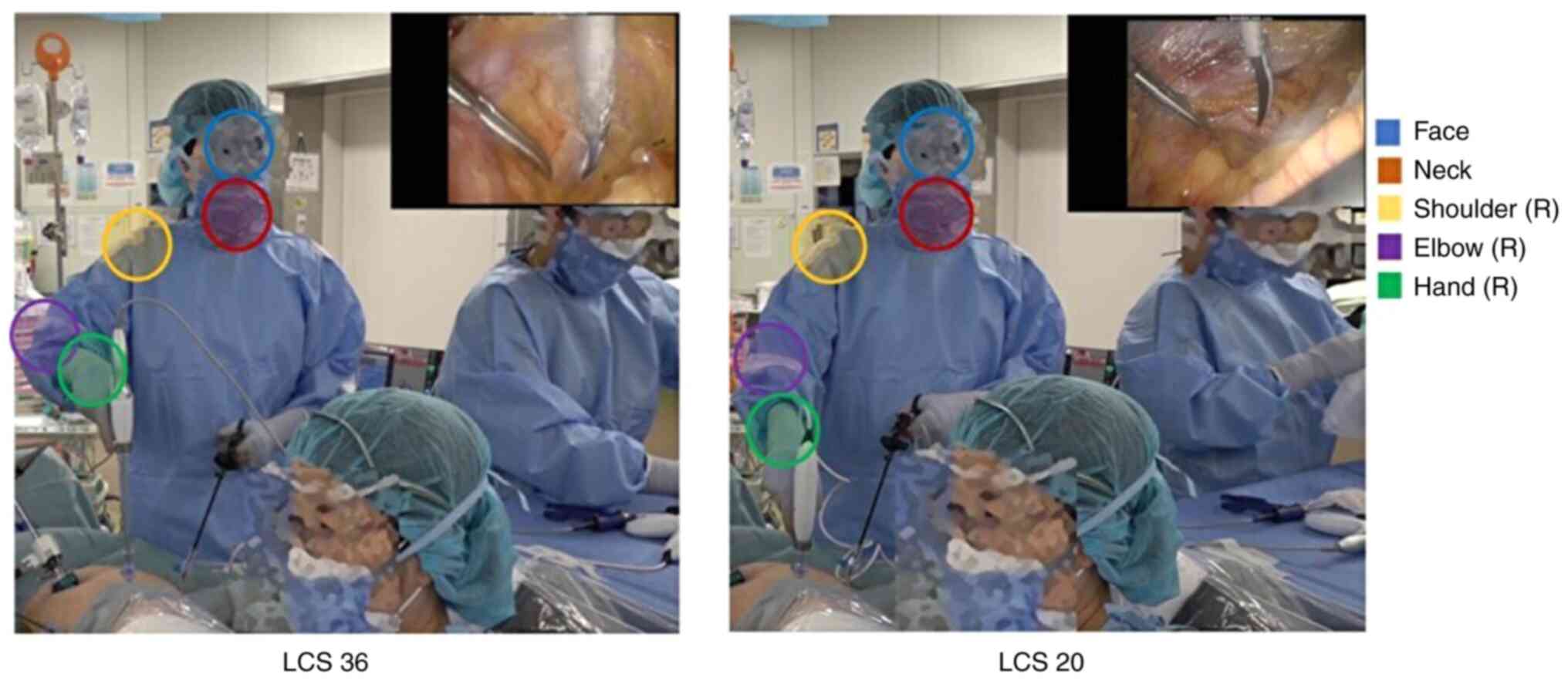 | Figure 1Images captured from a video of an
experienced surgeon showing marking by AI of the face and neck, and
the shoulder, elbow and hand on the side using the device. AI was
used to identify body parts in the video, with the range of motion
being illustrated graphically for each joint coordinate. Blue
circle, face; red circle, neck; yellow circle, shoulder; purple
circle, elbow; green circle, hand. R, right side; AI, artificial
intelligence; LCS 36, 36-cm long-shafted laparoscopic coagulation
shears; LCS 20, 20-cm long-shafted laparoscopic coagulation
shears. |
Matlab's OpenPose® (version R2023a; The
MathWorks, Inc.) was used to analyze human postures by identifying
the coordinates of specific joints, including the head, neck, right
shoulder, right elbow and right hand, within images generated by
the video. After pinpointing these joints, their trajectories were
plotted to visually represent their movement over time. To assess
the movement distance of each joint, the distance on a plane was
calculated from their median values, allowing the precise
quantification of their motion (Fig.
2).
OpenPose employs a sophisticated algorithm that
starts by detecting individual body parts within an image, such as
the nose and left elbow. Following this initial identification, it
adopts a bottom-up approach, assembling individual figures by
piecing together these body parts into reasonable combinations
(6). This method enables the
accurate estimation of the human posture, even in images with
several people, by analyzing how these body parts come together to
form individual poses. This approach was instrumental in the
present analysis, offering a detailed understanding of human
posture and movement in various scenarios.
An identical duration (2 min) of the same
laparoscopic hysterectomy procedure was separately analyzed when
using the long-shafted and the short-shafted LCS, and the surgeon's
motions during this period were analyzed with OpenPose. The range
of motion for the face, neck, shoulder, elbow and the hand on the
side using the device was also analyzed in a physician with limited
years of experience (in training for certification) who performed a
dissection of the left-sided broad ligament of the uterus. Surgical
procedures were performed as a set sequence of movements, and
comparisons were made between similar surgical procedures.
Statistical analysis
The data acquired by OpenPose are presented as the
median (IQR). Continuous variables with non-parametric
distributions were analyzed using Wilcoxon signed-rank test for the
paired data. All statistical analyses were performed using
JMP® software, version 16 (SAS Institute, Inc.).
Ethics
With regard to the use of a human surgery case for
research, the present study was conducted following the ethical
principles of the Declaration of Helsinki, and with the approval of
the Ethical Committee of Belland General Hospital (Sakai, Japan;
approval no. 2023-0021). A comprehensive explanation was provided
to the patient involved in this study before obtaining written
consent for the academic use of their surgical records.
Results
One case of hysterectomy surgery was used for the
present study and analyzed. The patient was 52-year-old woman
(gravida 1, para 1), with a height, body weight and BMI of 156 cm,
59 kg and 26.2 kg/m2 (normal range, 18.5 to 25
kg/m2), respectively. A total laparoscopic hysterectomy
was performed due to myomas. The surgeon stood on the left side of
the patient, the surgical assistant stood on the right side of the
patient and the assistant handling the manipulator for uterine
manipulation stood between the patient's legs. During the surgery,
the study hypothesis that a shorter instrument shaft will result in
less movement of the joints was tested.
During the procedure, the surgical motions were
compared for a trainee surgeon and an experienced surgeon.
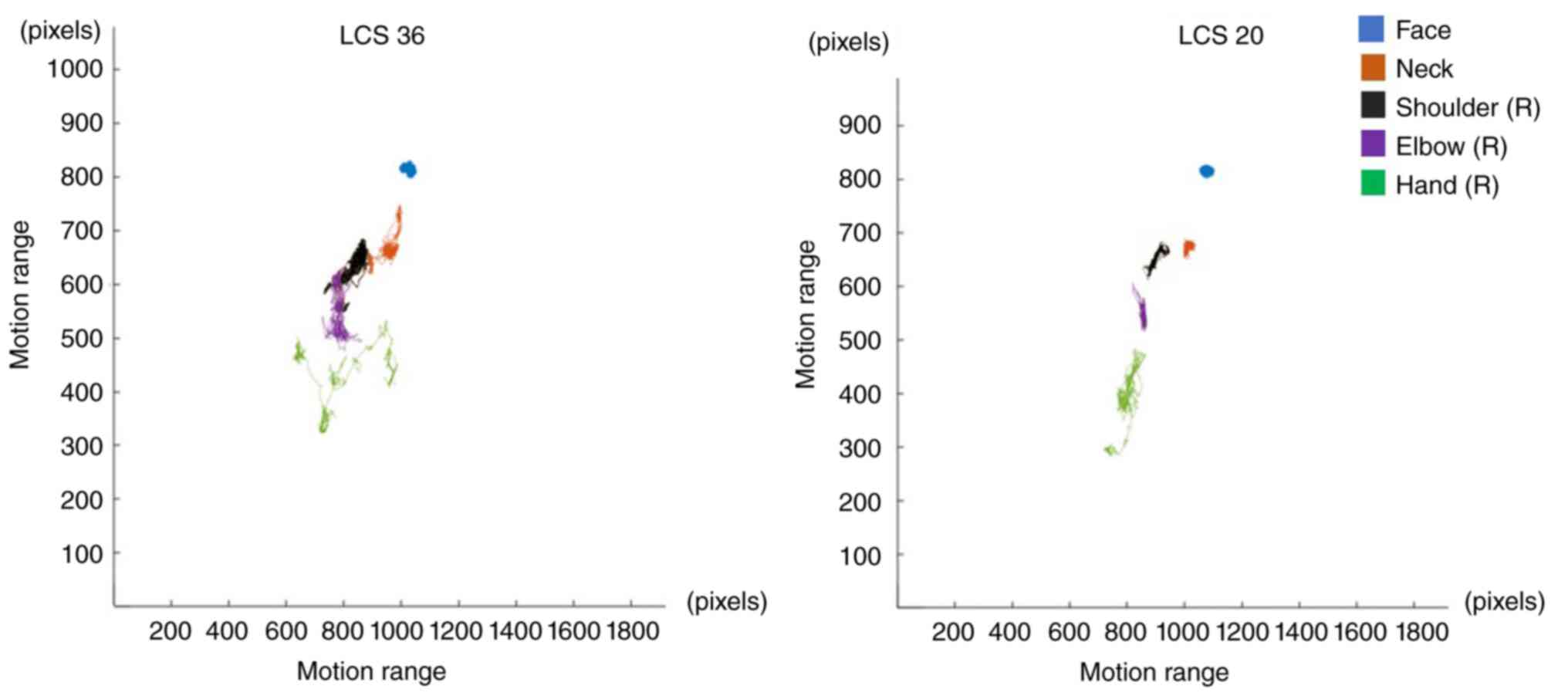
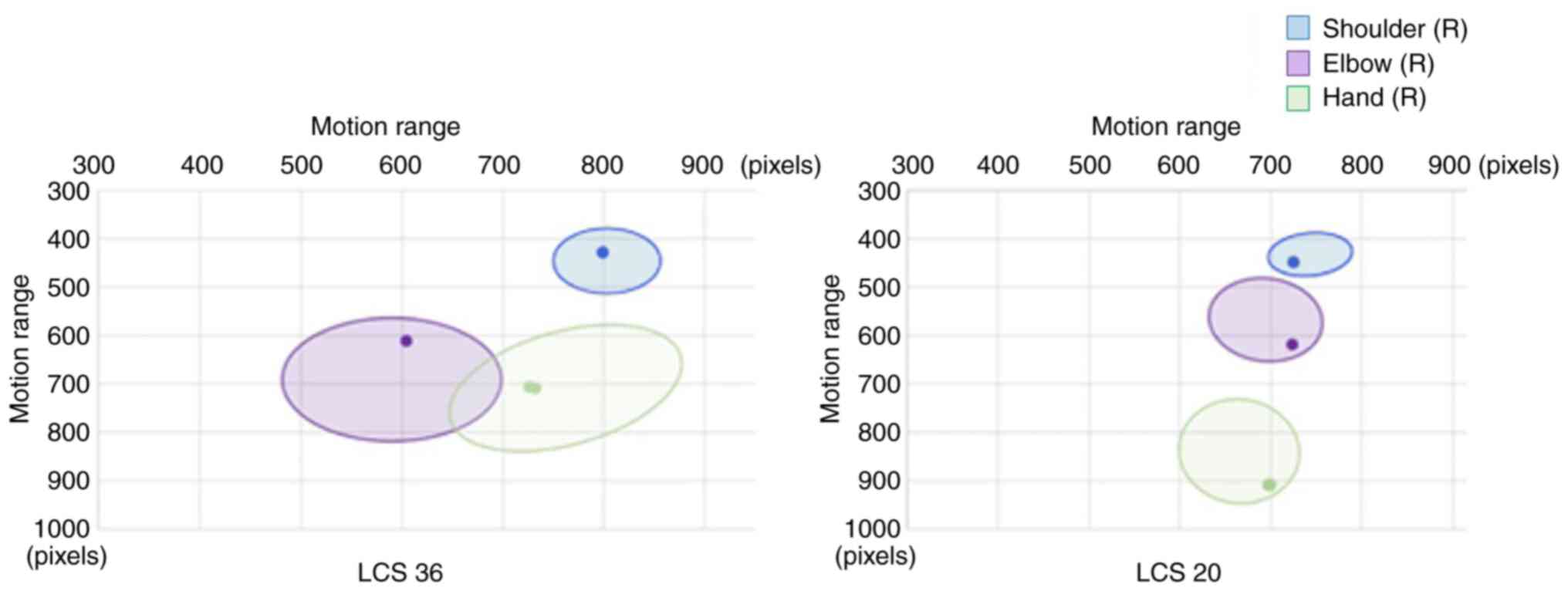
The range of motion for the face and neck did not
notably differ between the 20-cm short-shafted LCS and the 36-cm
long-shafted LCS; however, the range of motion for the shoulder,
elbow and hand became notably broader when using the long-shafted
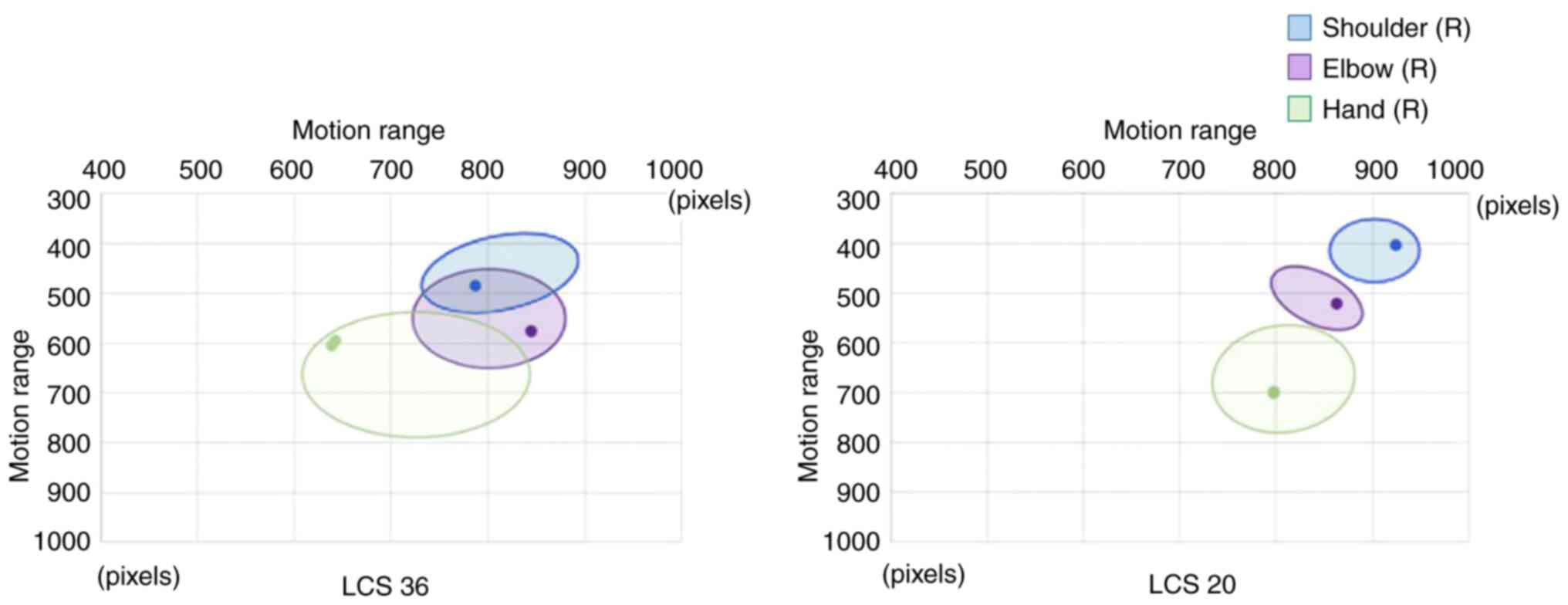
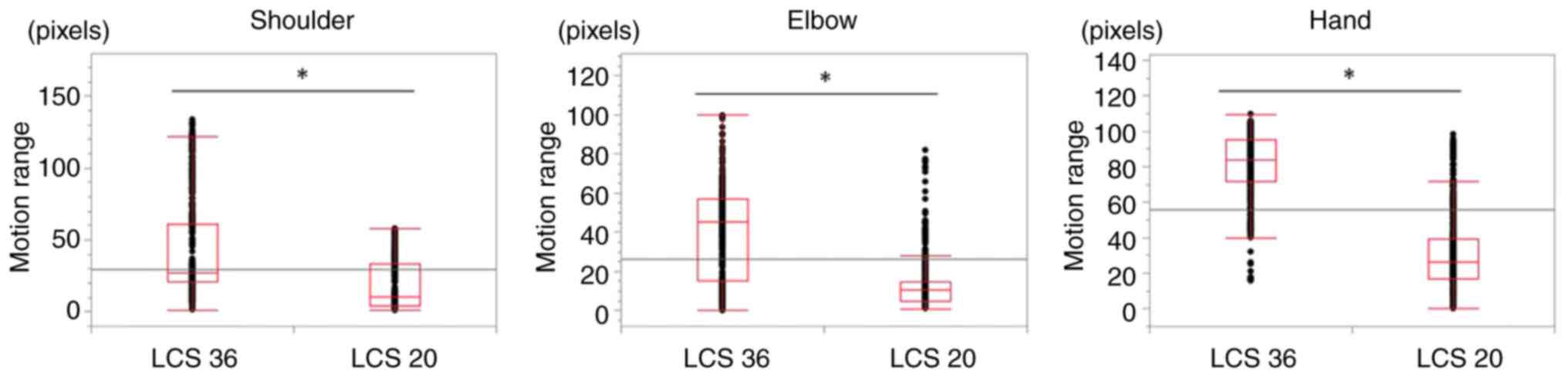
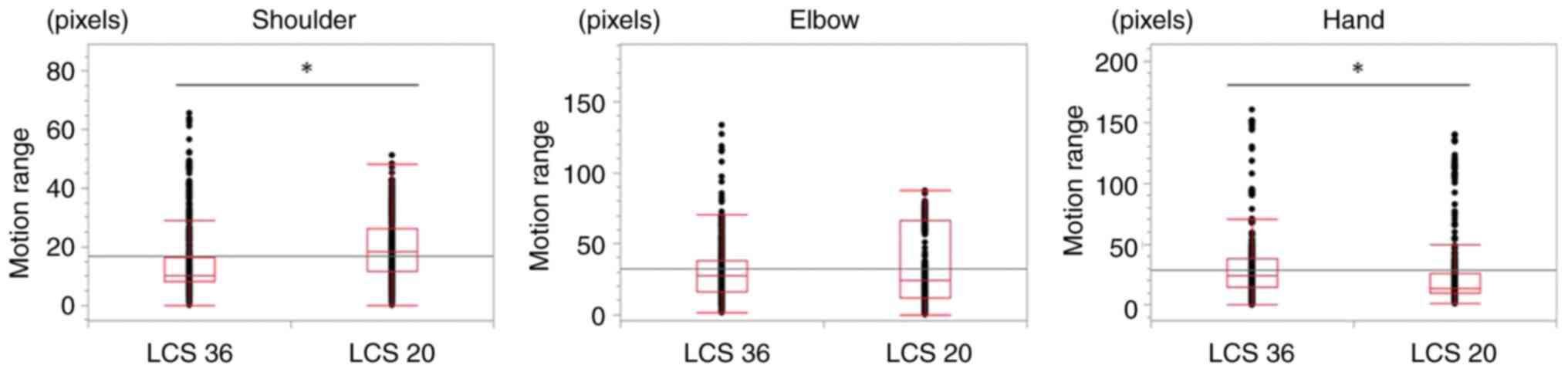
LCS compared with that when using the short-shafted LCS (Figs. 3 and 4). The distance traveled from the center
of the shoulder, elbow and hand joints was significantly smaller
with the short-shafted LCS than with the long-shafted LCS
(P<0.0001; Fig. 5).
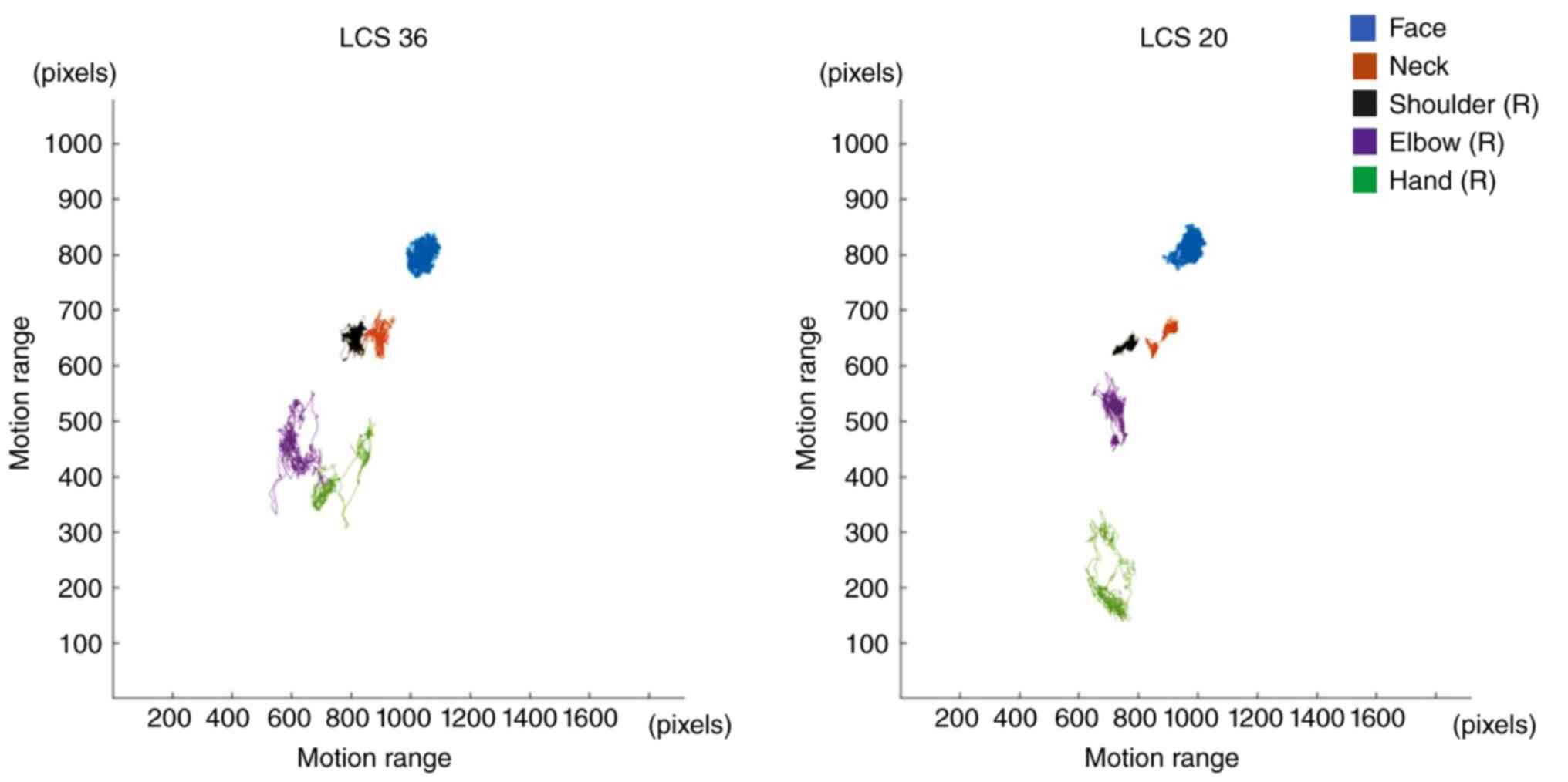
The range of motion for the face, neck, shoulder,
elbow and the hand on the side using the device was also analyzed
in a physician with limited years of experience (in training for
certification) who performed a dissection of the left-sided broad
ligament of the uterus. Similarly, the results in a physician with
limited years of experience showed that the range of motion for the
shoulder, elbow and hand was wider with the long-shafted LCS than
with the short-shafted LCS (Figs. 6
and 7). Furthermore, comparing the
aforementioned results with those in the more experienced surgeon
revealed that the head, neck, shoulder, elbow and hand all had a
greater range of motion. Furthermore, the distances traveled from
the center of the shoulder joint and the center of the hand joint
were significantly smaller with the long-shafted LCS than with the
short-shafted LCS (P<0.0001), whereas no significant difference
was observed between the types of LCS for the moving distance of
the elbow joint (Fig. 8).
Discussion
WMSD, which is prevalent among surgeons performing
gynecological surgeries, refers to repetitive motion injuries that
may damage the muscles, nerves and joints, commonly affecting the
neck, shoulders, back and hands. In addition to chronic pain, these
disorders may decrease job satisfaction and productivity. Factors
that can contribute to musculoskeletal disorders include increased
patient BMI, small hand size of surgeons, especially female
surgeons, and the design of surgical instruments and energy
devices. Therefore, establishing measures to address
musculoskeletal disorders is essential (1,2,4,7).
By analyzing images using AI, the current study
evaluated the impact of LCS shaft length on the range of motion of
the neck, shoulder, elbow and hand, which is considered crucial to
minimize strain. First, to trace of the movements of the face and
and neck, and the shoulder, elbow and hand on the side using the
device during surgery, deep learning AI was employed using MATLAB
software. To identify body parts in an image, OpenPose uses a
pretrained neural network that predicts heatmaps and part affinity
fields for body parts in an input image. The images were cut from
the video and adapted to the neural network. Range of motion
(pixels) was illustrated graphically for each joint coordinate, and
statistical analysis was performed to determine changes in
position. Figs. 4 and 7 illustrate the distance traveled from the
center of the joints, depicting the percentage change from the
center to the tip.
The present study findings showed that the
short-shafted LCS promoted a smaller range of motion than the
long-shafted LCS. The association between a narrower range of
motion and a reduction in WMSD is not directly described in the
literature. Manasnayakorn et al (8) reported that the use of short-length
needle holders in laparoscopic surgery leads to less muscle
workload. It is possible that a small range of motion is a result
of use of short-shafted instruments, and is a factor for reduced
muscle workload, which is caused by short-shafted devices during
laparoscopic surgery. Manasnayakorn et al (8) also investigated the operation speed
and accuracy when using short-length needle holders. It was
concluded that short-length devices may lead to improved execution
time and that the accuracy of operative motion with short-length
devices is not different from that of standard-length devices.
It is necessary to evaluate whether a broader range
of motion with the long-shafted LCS has any disadvantages in terms
of surgical precision and efficiency. In future, any wobbling of
the tip of the instrument and the surgical duration should be
assessed. When using a long-shafted instrument, instability of the
upper limb and device tip wobbling are anticipated. Comparisons of
the range of motion of the device tip of two instruments with
different shaft lengths should be considered. It is possible that
one of other factors that causes WMSD is the time that the limb is
held in a difficult position against gravity. Bell-land General
Hospital has recorded cases of adhesion due to conditions such as
endometriosis within the abdominal cavity, where adhesiolysis
surgery was performed for a prolonged period and the limb was held
in a difficult position, increasing fatigue as the surgery duration
lengthened. In the future, it is necessary to consider comparisons
of surgical duration with two instruments of different shaft
lengths, to determine, for example, whether using LCS with a
shorter shaft results in shorter surgical times.
In the present analysis, the physician who performed
the dissection of the right-sided broad ligament of the uterus was
a qualified and certified laparoscopic surgeon with extensive
experienced in the field. The range of motion for the face, neck,
shoulder, elbow and hand was also analyzed in a physician with
limited years of experience (in training for certification) who
performed a dissection of the left-sided broad ligament of the
uterus. The results in the physician with limited years of
experience similarly showed that the range of motion for the
shoulder, elbow and hand was wider with the long-shafted LCS than
with the short-shafted LCS. Comparing the results with those in the
more experienced surgeon revealed that the head, neck, shoulder,
elbow and hand all had a greater range of motion. Furthermore, the
distance traveled from the center of the shoulder and hand in the
less experienced surgeon was significantly smaller with the
long-shafted LCS than with the short-shafted LCS, whereas no
significant difference was observed for the elbow between both
types of LCS. However, in the more experienced surgeon, the range
of motion for every joint was significantly smaller when using the
short-shafted LCS than when using the long-shafted LCS. These
results suggest that factors potentially hindering the effective
use of surgical instruments, such as surgeon left-handedness or
limited/fewer years of surgical experience, may have contributed to
the observed variability.
One study on gynecological oncologists revealed that
88% of the participants reported pain from laparoscopy, with 29%
seeking treatment (9). Static
posture, excessive shoulder internal rotation, elbow deviation and
hand deviation are more common in laparoscopic surgery than in open
surgery (10,11). As assessed by electromyography in a
previous study, greater forearm, deltoid and thenar muscle force is
required during laparoscopic surgery than during open knot tying
and grasping (12,13). Furthermore, the ideal monitor
position was reported to be below the surgeon's eye level, at a
distance of 60 cm from the front of the surgeon (11,14,15).
This clearly indicates that the surgeon's posture, the height of
the surgical field and the position of the monitor are important
when performing the surgery.
A limitation for the present study is that it only
evaluated one case performed by one surgeon. Further verification
on multiple cases by multiple surgeons is necessary in the
future.
In conclusion, the current study examined the
differences in posture and range of motion when using a 20-cm
short-shafted LCS and a 36-cm long-shafted LCS, in a single case of
laparoscopic hysterectomy. Notably, the findings showed that the
short-shafted LCS promoted a narrower range of motion than the
long-shafted LCS, indicating the possibility of reducing the burden
placed on the surgeon's body during surgery.
As minimally invasive laparoscopic surgery becomes
more prevalent, ongoing efforts to explore innovations to improve
WMSD are necessary. The present findings would suggest room for
further exploration and refinement to improve the ergonomics of
surgical instruments and help reduce the incidence of WMSD during
evolving gynecological laparoscopic surgery.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
MO was responsible for writing the manuscript and
preparation of the sample dataset, including the analysis and
interpretation of the data. NM was responsible for study design,
interpretation of the results and study supervision. ST, MM, KM,
TM, AI and JO were responsible for preparation of the electric
sample dataset for the movement distance of each joint analyzed by
OpenPose, including the analysis and interpretation of the data. TM
supervised the study, and checked and fixed the final manuscript.
All authors have read and approved the contents of the manuscript.
MO, NM, ST, MM, KM, TM, AI, JO and TM confirm the authenticity of
all the raw data.
Ethics approval and consent to
participate
The present study was conducted following the
ethical principles of the Declaration of Helsinki, and with the
approval of the Ethical Committee of Belland General Hospital
(Sakai, Japan; approval no. 2023-0021). A comprehensive explanation
was provided to the patient involved in this study before obtaining
written consent for the academic use of their surgical records.
Patient consent for publication
The patient provided written consent for their
information to be published.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Catanzarite T, Tan-Kim J and Menefee SA:
Ergonomics in gynecologic surgery. Curr Opin Obstet Gynecol.
30:432–440. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zahiri HR, Addo A and Park AE:
Musculoskeletal disorders in minimally invasive surgery. Adv Surg.
53:209–220. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Morandeira-Rivas A, Millán-Casas L,
Moreno-Sanz C, Herrero-Bogajo ML, Tenías-Burillo JM and
Giménez-Salillas L: Ergonomics in laparoendoscopic single-site
surgery: Survey results. J Gastrointest Surg. 16:2151–2159.
2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lin E, Young R, Shields J, Smith K and
Chao L: Growing pains: Strategies for improving ergonomics in
minimally invasive gynecologic surgery. Curr Opin Obstet Gynecol.
35:361–367. 2023.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yoshiyuki O: ‘Introduction and results of
laparoscopic total hysterectomy (TLH) using a short shaft energy
device with consideration for ergonomics’ of Presentaion. Japan
Society for Endoscopic Surgery, Nagoya, 2022.
|
|
6
|
Cao Z, Hidalgo G, Simon T, Wei SE and
Sheikh Y: OpenPose: Realtime Multi-Person 2D pose estimation using
part affinity fields. IEEE Trans Pattern Anal Mach Intell.
43:172–186. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Reddy PP, Reddy TP, Roig-Francoli J, Cone
L, Sivan B, DeFoor WR, Gaitonde K and Noh PH: The impact of the
alexander technique on improving posture and surgical ergonomics
during minimally invasive surgery. pilot study. J Urol. 186 (Suppl
4):S1658–S1662. 2011.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Manasnayakorn S, Cuschieri A and Hanna GB:
Ideal manipulation angle and instrument length in hand-assisted
laparoscopic surgery. Surg Endosc. 22:924–929. 2008.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Franasiak J, Ko EM, Kidd J, Secord AA,
Bell M, Boggess JF and Gehrig PA: Physical strain and urgent need
for ergonomic training among gynecologic oncologists who perform
minimally invasive surgery. Gynecol Oncol. 126:437–442.
2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Nguyen NT, Ho HS, Smith WD, Philipps C,
Lewis C, De Vera RM and Berguer R: An ergonomic evaluation of
surgeons' axial skeletal and upper extremity movements during
laparoscopic and open surgery. Am J Surg. 182:720–724.
2001.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Vereczkei A, Feussner H, Negele T,
Fritzsche F, Seitz T, Bubb H and Horváth OP: Ergonomic assessment
of the static stress confronted by surgeons during laparoscopic
cholecystectomy. Surg Endosc. 18:1118–1122. 2004.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Berguer R, Chen J and Smith WD: A
comparison of the physical effort required for laparoscopic and
open surgical techniques. Arch Surg. 138:967–970. 2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Berguer R, Gerber S, Kilpatrick G and
Beckley D: An ergonomic comparison of in-line vs pistol-grip handle
configuration in a laparoscopic grasper. Surg Endosc. 12:805–808.
1998.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Veelen MA, Jakimowicz JJ, Goossens RH,
Meijer DW and Bussmann JB: Evaluation of the usability of two types
of image display systems, during laparoscopy. Surg Endosc.
16:674–678. 2002.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Matern U, Faist M, Kehl K, Giebmeyer C and
Buess G: Monitor position in laparoscopic surgery. Surg Endosc.
19:436–440. 2005.PubMed/NCBI View Article : Google Scholar
|