Introduction
Laparoscopically assisted vaginal hysterectomy
(LAVH) has been widely accepted as a hysterectomy procedures for
uterine myomas and adenomyosis (1,2),
usually by placing three trocars through the abdominal wall. To
further reduce the invasiveness of traditional laparoscopic
procedures, transumbilical single-incision laparoscopic surgery has
been gradually developed mainly in general surgery, since Navarra
et al introduced the ‘one-wound laparoscopic
cholecystectomy’ technique in 1997 (3). In the field of gynecology, although
the single-incision laparoscopic procedure was described in cases
of sterilization in the 1970s (4),
it has not been well developed to date.
There are several hysterectomy procedures using a
laparoscope, such as LAVH and total laparoscopic hysterectomy
(TLH), to reduce invasiveness. Total vaginal hysterectomy (TVH) is
another less invasive hysterectomy procedure without an abdominal
wound. We usually perform LAVH for patients with uterine myomas and
adenomyosis since it is less invasive than ‘open’ total abdominal
hysterectomy (TAH), safer than TVH and it requires less complicated
laparoscopic procedures than TLH. We applied single-incision
laparoscopic surgery to LAVH for 10 cases in July 2009 and
considered that it could be undertaken effectively with similar
operative results, compared to conventional multiport,
multi-incision LAVH (5). Since
then, we shifted the conventional laparoscopic procedure to a
single-incision one when performing LAVH. To better evaluate this
operation, we accumulated cases in which single-incision LAVH was
performed for uterine myomas and adenomyosis. We began to apply
single-incision LAVH in July 2009 and we planned to perform this
procedure in 50 cases until March 2010. Here, our operative
outcomes are presented and compared to conventional multiport,
multi-incision LAVH cases. We also tried to estimate the learning
curve of this method comparing the operative results of the former
and the latter cases during the study period.
Materials and methods
Patient selection
From July 2009 until March 2010 (we started to apply
single-incision LAVH in July 2009), 50 female patients underwent
single-incision LAVH for uterine myomas or adenomyosis. All
single-incision LAVHs were performed by the same operator (S.M.)
with written informed consent provided by the patients.
The mean age of the patients was 45.2±4.0 years
(range 36–53). These 50 patients suffered from one or more of the
following symptoms: pelvic pain, hypermenorrhea, dysmenorrheal and
compression syndrome, such as constipation and incontinence. In all
patients, the presence of myomas or adenomyosis was confirmed
clinically by transvaginal ultrasonography and computed tomography
or magnetic resonance imaging. Patient characteristics and
operative results, including operative time, estimated blood loss,
weight of resected uterus and additional procedures, were recorded.
Additionally, the results of 40 patients who underwent conventional
multiport, multi-incision LAVH performed by the same operator from
January until June 2009, prior to introducing single-incision LAVH,
were also recorded and compared to the single-incision LAVH cases.
The mean age of the conventional LAVH patients was 47.3±6.1 years
(range 35–65) and the indications were also uterine myomas or
adenomyosis. Gonadotropin-releasing hormone agonists (GnRHa) were
administered pre-operatively when the uterus was larger than a
baby's head size, or when complicated by anemia or endometriosis;
17 cases (34%) in the single-incision LAVH group and 12 cases (30%)
in the conventional LAVH group, respectively (P=0.69).
To estimate its learning curve, 47 completed
single-incision LAVH cases were divided into two groups; the former
24 cases (from July until November 2009) and the latter 23 cases
(from December 2009 until March 2010). We compared the operative
outcomes between the two groups.
Operative technique
LAVH consists of two main operative procedures; one
is a laparoscopic procedure and the other is a vaginal approach. We
applied single-incision laparoscopic surgery to the laparoscopic
phase of LAVH as we previously reported (5). The vaginal approach was the same as
that of the conventional LAVH.
All procedures were performed with the patient under
general anesthesia and in the lithotomy position. The Uterine
Manipulator™ (Ethicon, Tokyo, Japan) was inserted into the uterine
cavity to manipulate the uterus during the laparoscopic procedure.
We completely extroflexed the umbilicus and made a longitudinal
skin incision of ∼2 cm, bluntly dissecting the subcutaneous tissue
to the fascia. As the first trocar, a 5-mm XCEL Bladeless Trocar™
(Ethicon Endo-Surgery, USA), was inserted with the closed method
using a 5-mm 0-degree rigid laparoscope. After insertion,
pneumoperitoneum was induced with carbon dioxide (CO2)
maintained at 8–10 mmHg, and the abdominal cavity was explored with
a 5-mm 30-degree rigid laparoscope. The second and third 5-mm
working trocars (Lina Port™; LiNA Medical, Glostrup, Denmark) were
placed through separate fascial punctures within one skin incision
in the umbilicus. Two working trocars were inserted inferiorly to
the camera trocar site, crossing each other. All three trocars were
placed through one skin incision at different fascial sites to
create a triangulated arrangement (Fig. 1). Both roticulating and straight
forceps were used depending upon the operative findings to create
the necessary operative field.
Round ligament, fallopian tube, ovarian ligament
and/or vesicouterine excavation peritoneum were cut with a vessel
sealing system such as LigaSure™ (Covidien, MA, USA) and/or
electric scissors during the laparoscopic procedure. Then, we
shifted to the vaginal approach. Uterine artery and lateral
cervical ligaments were cut and the resected uterus was removed
transvaginally. The peritoneum and vaginal walls were closed with
the vaginal approach. After confirming sufficient hemostasis
laparoscopically, the fascial incisions were closed with a 0-Vicryl
suture. The umbilicus was carefully reconstructed with a 4-0 Vicryl
suture, allowing it to be replaced to its original position. As a
result, the abdominal wound appeared completely invisible.
Statistical analysis
All results are expressed as the means ± standard
deviation. Operative time was defined as the time from skin
incision to time of closure. Comparisons between the two groups
were performed using the Mann-Whitney U-test for independent sample
for continuous values and the χ2 test or Fisher's exact
test for categorical variables. Statistical analysis was performed
with SPSS version 10.0 (SPSS, Chicago, IL, USA).
P<0.05 was considered statistically significant
and all reported P-values were two-sided.
Results
Fifty patients underwent single-incision LAVH from
July 2009 until March 2010. Before applying single-incision LAVH,
40 patients underwent conventional multiport, multi-incision LAVH
during the first half of 2009.
Regarding the characteristics of the patients, only
body mass index was significantly different between the
single-incision and conventional LAVH, as shown in Table I (22.0±2.7 vs. 23.6±3.5, P=0.03).
Table II shows the operative
results of single-incision and conventional LAVH. We completed 47
of 50 (94%) single-incision LAVHs in this study. We experienced 3
conversion cases to conventional multiport surgery from
single-incision LAVH, and no conversion case to TAH from
conventional LAVH (3/50, 6% vs. 0/40, 0%, P=0.12). We did not
experience any conversions to TAH from single-incision LAVH. The
reasons for conversion were as follows: strong pelvic adhesion in 2
cases and large uterine myomas in 1 case that made it difficult to
create the necessary operative field or to manipulate the forceps.
Operative time, estimated blood loss and weight of the resected
uterus were statistically similar, but more additional procedures,
such as salpingo-oophorectomy and adhesiolysis, were required in
the conventional LAVH group (27.7% in single-incision vs. 57.5% in
the conventional group, P<0.01). None of the patients required a
blood transfusion and no major perioperative complications, such as
organ damage, reoperation, surgical site infections or hernias,
were encountered in either group.
 | Table I.Characteristics of the patients who
underwent single-incision LAVH and conventional multiport,
multi-incision LAVH. |
Table I.
Characteristics of the patients who
underwent single-incision LAVH and conventional multiport,
multi-incision LAVH.
| Single-incision LAVH
(n=50) | Conventional LAVH
(n=40) | P-value |
|---|
| Age, in years | 45.2±4.0 (36–53) | 47.3±6.1 (35–65) | 0.08 |
| BMI, in
kg/m2 | 22.0±2.7
(16.4–28.4) | 23.6±3.5
(17.5–30.5) | 0.03 |
| History of vaginal
delivery | 42 (84%) | 36 (90%) | 0.60 |
| Indications | | | 0.63 |
| Myoma | 45 (95%) | 38 (95%) | |
| Adenomyosis | 5 (10%) | 2 (5%) | |
| Pre-operative GnRHa
administration | 17 (34%) | 12 (30%) | 0.69 |
| Table II.Operative results and comparison
between completed single-incision LAVH and conventional multiport,
multi-incision LAVH. |
Table II.
Operative results and comparison
between completed single-incision LAVH and conventional multiport,
multi-incision LAVH.
| Single-incision LAVH
(n=47) | Conventional LAVH
(n=40) | P-value |
|---|
| Operative time
(min) | 65.0±17.0
(37–110) | 63.9±22.5
(30–120) | 0.51 |
| Estimated blood loss
(ml) | 359±261
(46–1,389) | 344±242
(46–1,107) | 0.83 |
| Weight of resected
uterus (g) | 324±173 (86–850) | 369±199
(114–950) | 0.38 |
| Additional
procedures | 13 (27.7%) | 23 (57.5%) | <0.01 |
|
Salpingo-oophorectomy | 4 | 10 | |
| Adhesiolysis | 9 | 13 | |
| Conversion | to conventional
LAVH | to TAH | 0.12 |
| 3/50 (6%) | 0 | |
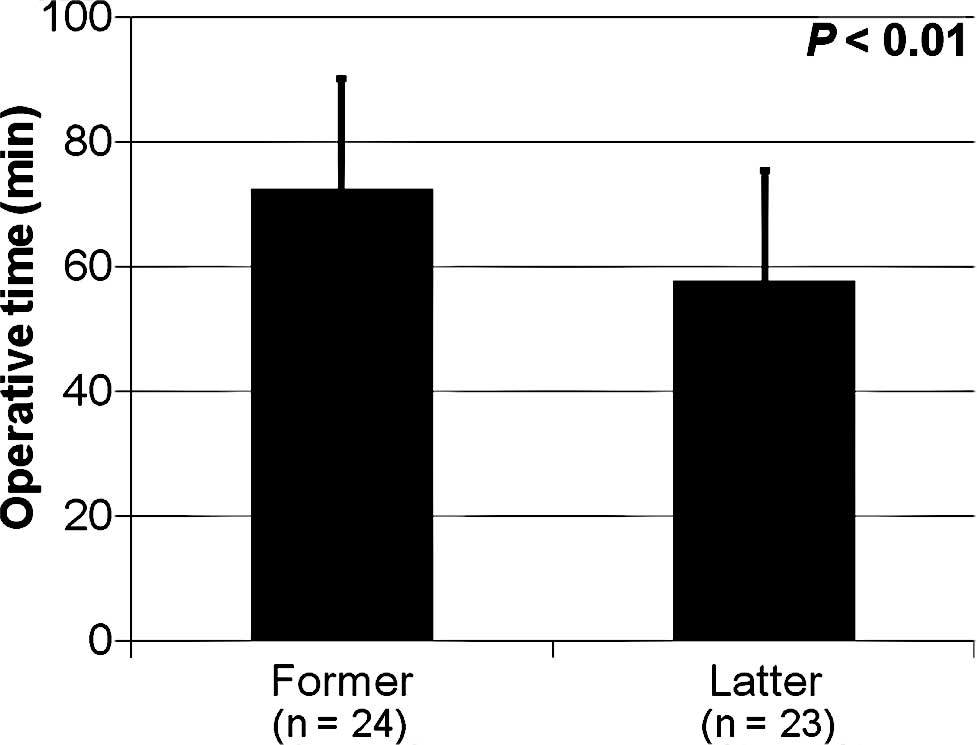
Upon dividing the 47 completed single-incision LAVH
cases into two groups by the period in which the operation was
performed, the operative time was significantly shortened during
the study period, as shown in Fig.
2 and Table III; 73.0±17.6 min
for the former 24 cases vs. 58.0±12.2 min for the latter 23 cases
(P<0.01). These results suggest a short learning curve for
single-incision LAVH. There was no significant difference between
the two subgroups with respect to estimated blood loss, weight of
resected uterus and additional procedures (Table III).
| Table III.Operative results of completed
single-incision LAVH cases and comparison between the two
periods. |
Table III.
Operative results of completed
single-incision LAVH cases and comparison between the two
periods.
| Former cases
(n=24) | Latter cases
(n=23) | P-value |
|---|
| Operative time
(min) | 73.0±17.6
(42–110) | 58.0±12.2
(37–85) | <0.01 |
| Estimated blood loss
(ml) | 355±213 (73–909) | 363±312
(46–1,389) | 0.59 |
| Weight of resected
uterus (g) | 349±203 (94–850) | 298±138 (86–598) | 0.59 |
| Additional
procedures | 6 (25%) | 7 (30.4%) | 0.68 |
|
Salpingo-oophorectomy | 2 | 2 | |
| Adhesiolysis | 4 | 5 | |
Discussion
The main operative results, including operative
time, estimated blood loss and weight of resected uterus, were
compared and there was no significant difference between
single-incision LAVH and conventional LAVH. In addition, we first
showed an even shorter learning curve for single-incision LAVH
based on our operative results.
First, there was no significant difference between
single-incision LAVH and conventional LAVH when the main operative
results were compared. The main procedure of LAVH is the vaginal
approach and this is the same in both single-incision and
conventional LAVH. Therefore, operative time and estimated blood
loss were not influenced by the laparoscopic procedure when
performing single-incision LAVH. These laparoscopic procedures
through one skin incision within the umbilicus may be performed
with similar operative results to those of the conventional
multiport, multi-incision LAVH. Through these outcomes, it may be
possible to consider the indication of single-incision LAVH to be
same as that of conventional LAVH. In addition, approximately 30%
of the patients were administered GnRHa before surgery in this
study. GnRHa administration is helpful to extend the indications
for single-incision LAVH.
Second, we first showed an even shorter learning
curve for single-incision LAVH. Although another comparable
operative outcome of single-port-access LAVH has been reported
(6), the learning curve of this
procedure has not been evaluated before. Completing a new surgical
procedure requires appropriate training and experience. It is
expected that the mean procedure duration will be gradually
shortened with increasing surgical experience (1,7). It
has been reported and estimated that a surgeon will be able to
establish proficiency after having performed more than 50
conventional LAVHs (8). However,
in this study the operative time was significantly shortened during
a period of 9 months (less than 50 cases) without special equipment
or training. Therefore, there is an even shorter learning curve for
single-incision LAVH based on our operative results. This is
because the techniques necessary for conventional multiport LAVH
are identical to those required to perform and complete the
single-incision laparoscopic procedures. Also, difficulties are
more likely to be encountered very early in the learning phase with
respect to single-incision LAVH.
During this study period, we experienced three
conversions from single-incision to conventional multiport LAVH.
Although we achieved a high success rate with both single-incision
(94%) and conventional LAVH (100%), surgeons should not persist in
completing laparoscopic procedures in single-incision LAVH, as
single-incision procedures can easily be converted to a
conventional multiport LAVH in the event problems arise. As a
result, severe perioperative complications, such as blood
transfusion and adjacent organ damage are avoided.
In the development of the single-incision surgical
technique, many different choices and combinations of operative
devices, including trocars and forceps, for gynecologic surgery
have been proposed (9,10). For the trocars, the combination of
the XCEL Bladeless Trocar™ (camera trocar) and the Lina Port™
(lateral trocars) was chosen to minimize the conflict between the
operative instruments and the camera. A comparison and evaluation
of the operative outcomes with the different choices and
combinations of surgical devices, such as trocars and forceps,
during the operation are warranted. As for the application to other
gynecologic diseases, we have already applied single-incision
laparoscopic surgery to various ovarian procedures such as
salpingo-oophorectomy and cystectomy, as well as the additional
procedures of single-incision LAVH. A comparison of the
single-incision technique, as applied to these different
procedures, with conventional multiport methods is also warranted
as it would be possible to evaluate its versatility as well.
We presented data for a sequential comparison, but
the conventional LAVHs in this study were performed before applying
the single-incision surgical technique. This factor may have
introduced certain biases, particularly as it relates to surgical
experience and the learning curve. Therefore, it is necessary to
provide a comparison of cases performed concurrently. To further
establish the level of reliability for single-incision LAVH, more
cases and randomized controlled trials are required to precisely
evaluate the efficacy and safety, including complication rates.
In conclusion, single-incision LAVH can be performed
as effectively as conventional multiport LAVH with a short learning
curve. It may be a promising alternative method for the treatment
of certain patients with uterine myomas and adenomyosis as even a
less invasive gynecological operation is required without visible
scars.
References
|
1.
|
Seow KM, Tsou CT, Lin YH, Hwang JL, Tsai
YL and Huang LW: Outcomes and complications of laparoscopically
assisted vaginal hysterectomy. Int J Gynaecol Obstet. 95:29–34.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Drahonovsky J, Haakova L, Otcenasek M,
Krofta L, Kucera E and Feyereisl J: A prospective randomized
comparison of vaginal hysterectomy, laparoscopically assisted
vaginal hysterectomy, and total laparoscopic hysterectomy in women
with benign uterine disease. Eur J Obstet Gynecol Reprod Biol.
148:172–176. 2010. View Article : Google Scholar
|
|
3.
|
Navvara G, Pozza E, Occhionorelli S,
Carcoforo P and Donini I: One-wound laparoscopic cholecystectomy.
Br J Surg. 84:6951997. View Article : Google Scholar
|
|
4.
|
Wheeless CR Jr: Outpatient laparoscope
sterilization under local anesthesia. Obstet Gynecol. 39:767–770.
1972.PubMed/NCBI
|
|
5.
|
Koyanagi T and Motomura S: Transumbilical
single-incision laparoscopic surgery: application to
laparoscopically assisted vaginal hysterectomy. Arch Gynecol
Obstet. 283:305–309. 2011. View Article : Google Scholar
|
|
6.
|
Kim TJ, Lee YY, Cha HH, et al:
Single-port-access laparoscopic-assisted vaginal hysterectomy
versus conventional laparoscopic-assisted vaginal hysterectomy: a
comparison of perioperative outcomes. Surg Endosc. 24:2248–2252.
2010. View Article : Google Scholar
|
|
7.
|
Chapron C, Querleu D, Bruhat MA, Madelenat
P, Fernandez H, Pierre F and Dubuisson JB: Surgical complications
of diagnostic and operative gynaecological laparoscopy: a series of
29,966 cases. Hum Reprod. 13:867–872. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Hwang JL, Seow KM, Tsai YL, Huang LW,
Hsieh BC and Lee C: Comparative study of vaginal, laparoscopically
assisted vaginal and abdominal hysterectomies for uterine myoma
larger than 6 cm in diameter or uterus weighing at least 450 g: a
prospective randomized study. Acta Obstet Gynecol Scand.
81:1132–1138. 2002. View Article : Google Scholar
|
|
9.
|
Lee YY, Kim TJ, Kim CJ, et al: Single-port
access laparoscopic-assisted vaginal hysterectomy: a novel method
with a wound retractor and a glove. J Minim Invasive Gynecol.
16:450–453. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Lim MC, Kim TJ, Kang S, Bae DS, Park SY
and Seo SS: Embryonic natural orifice transumbilical endoscopic
surgery (E-NOTES) for adnexal tumors. Surg Endosc. 23:2445–2449.
2009. View Article : Google Scholar : PubMed/NCBI
|