Introduction
Advances in microsurgical instruments and refinement
of surgical techniques have made it possible to operate on the
frontotemporal-zygomatic arch (1).
The range of this approach can reach the anterior cranial and
middle cranial base regions, posterior cranial fossa and up to 1/3
of the clival area (2). The
petroclival region, a clinically significant and complicated area,
can be divided into 3 parts: The superior, located in the starting
point of the cranial nerve stem brain, the middle, located between
the starting point of the trigeminal and glossopharyngeal nerves,
and the inferior, located under the starting point of the
glossopharyngeal nerve also including the foramen occipitale magnum
(3,4). The postauricular, transpetrous and
presigmoid approaches combine a supra/infratentorial exposure with
partial petrosectomy to access the third to twelfth cranial nerves
and the anterolateral to the brainstem. It provides a shorter
working distance to the large petrosal, petroclival,
cerebellopontine and cerebellomedullary cisternal lesions (5). The microanatomy for surgery on the
superior petroclival region through the frontotemporal-zygomatic
arch approach remains unclear (6).
Therefore, the aim of the present study was to provide a foundation
of microanatomy for surgery on this region via the
frontotemporal-zygomatic arch approach. We show that this approach
provides excellent exposure of the superior petroclival region with
minimal brain retraction and nerve injury.
Materials and methods
Specimens
Ten adult cadaver heads (20 sides) fixed by 10%
formalin, 7 male (16 sides) and 3 female (6 sides), were used in
this study. None of the cadaver heads used had any malformations,
surgical traumas, disease or any surgical traces in the skull. All
the specimens used were obtained from people who had donated their
body to science and research. Ethical permission for this study was
granted by the Ethical Committee of Zhejiang University School of
Medicine (Hangzhou, China).
Surgical instruments
Surgical instruments used included an operating
head-frame, high-speed drill, common craniocerebral surgical
instruments, microsurgical instruments, an electric suction
apparatus, and a pair of scissors and razor.
Observing and measuring equipment
These included an operating microscope, digital
camera, triangle, sliding caliper (degree of accuracy 0.02 mm),
measure gauge, conimeter (degree of accuracy: 1), galvanizer
etc.
Methods
The frontotemporal-zygomatic arch approach includes
the following surgical steps: Firstly, it begins with normal
surgery on the skull, exposing the bone flap and applying the
orbitozygomatic osteotomy technique to remove the
frontotemporal-zygomatic arch.
The first step to the exposure of the superior
petroclival region, is extradural, the anterior processus
clinoideus resection. It must be carefully executed in order to
protect the crucial structures which surround it, while removing
the processus clinoideus anterior. The structures include the optic
nerve on the medial wall, the oculomotor nerve on the lateral wall
and the internal carotid artery on the inferior wall. After
removing the processus clinoideus anterior, the field of vision is
greatly improved. Then gradually retract the frontal lobe, the
optic chiasm and the anterior communicating artery complex, thus
exposing the pituitary stalk behind the optic chiasm. Unfolding the
lilliquist membrane between the internal carotid artery and optic
nerve, along the posterior communicating and cerebral arteries to
reach the P1–2 junction, eventually reveals the basilar artery
bifurcation and the petroclival region.
By observing the course, distribution and
relationship between the nerves and blood vessels, a number of
significant data were measured. With the removal of the processus
clinoideus anterior, processus dorsi sellae and partial petrosal
bones, the range of exposure were measured.
Results
Exposure of optic nerve
Though the optic nerve is not located on the
superior petroclival region, is still an essential nerve through
the frontotemporal-zygomatic arch approach. During the surgery the
distal end branch of the arteria cerebri aborales and the furcation
of the internal carotid artery can be observed after the following
steps: Unfolding the cerebral dura mater, retracting the frontal
and temporal lobe, opening the lateral fissure of telencephalon by
an arachniod knife, separating the sylvian vein, dragging the
sylvian vein away to the side of temporal lobe, separating the
lateral fissure and identifying the remote branch of the middle
cerebral artery bifurcation of internal carotid artery by being
separated. Fig. 1 shows the
interspace between the optic nerve and the posterior communicating
artery. Further steps in accordance with the method exposed the
basilar artery before removing the processus clinoideus anterior,
in which the length of the optic nerve was 10.22 mm (9.20–11.94),
and after the removal of the processus clinoideus anterior the
length was 22.62 mm (20.36–24.48).
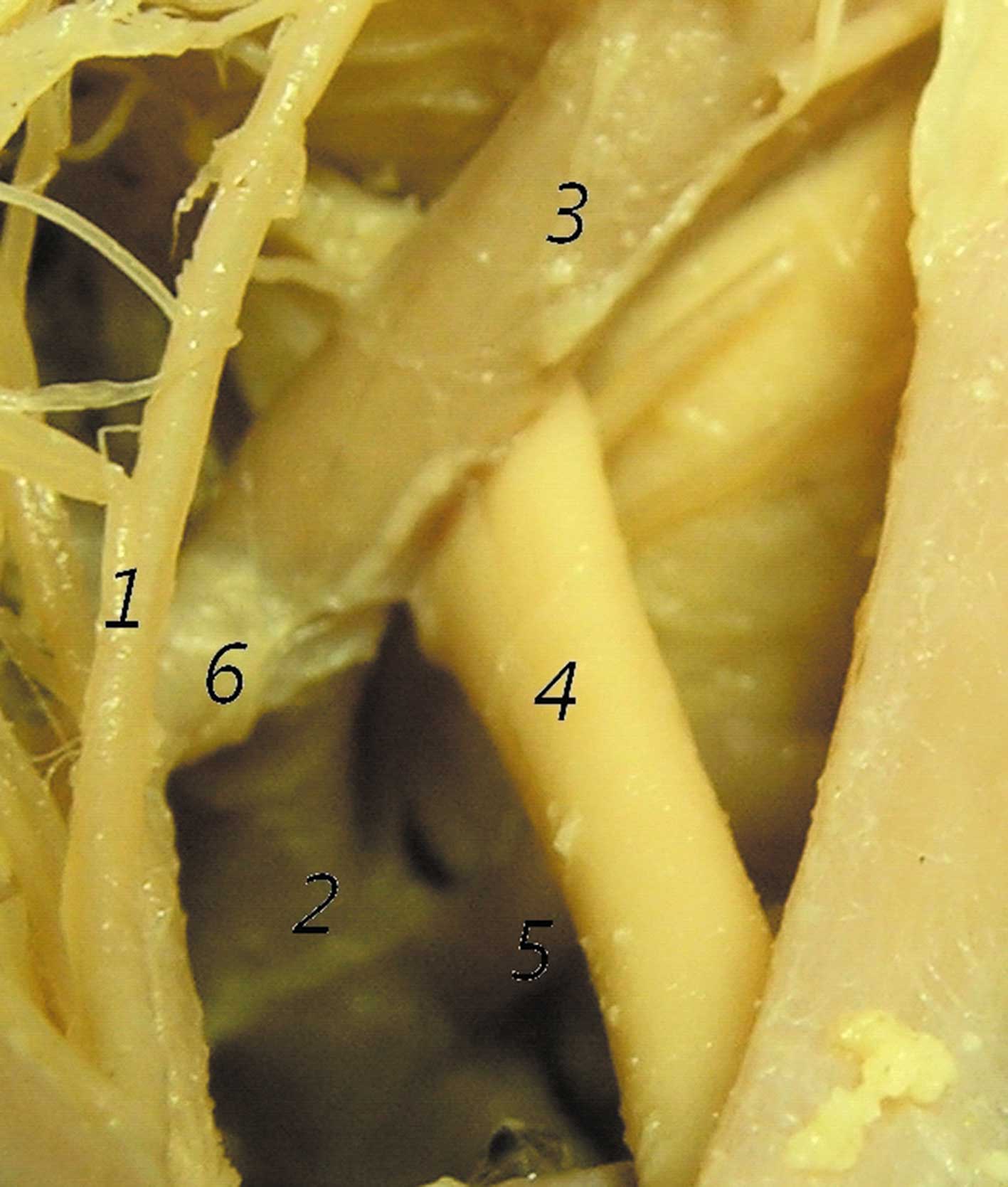
Exposure of oculomotor and trochilear
nerves
The oculomotor nerve went through the superior
cerebellar and posterior cerebral arteries (Fig. 2). The distance of the inferior
extremity between the posterior cerebral artery and the lower edge
of the cerebellar tentorium was approximately 18.32 mm
(17.04–19.88). The trochlear nerve went through the inferior part
of the caudal colliculus located on the mesencephalicus
lateralis dorsalis, reaching the inferior edge of the
cerebellar tentorium at the border between the cerebral peduncle
and the cerebellar tentorium. The distance was approximately 6.02
mm (4.28–6.98) after the trochlear nerve went into the free edge of
the cerebellar tentorium.
Relative vessels on the superior
petroclival region
The artery of the superior petroclival region
includes the posterior cerebral, superior cerebellar and basilar
arteries. According to its course, the posterior cerebral artery
can be divided into the frontal, lateral and posterior segments.
The frontal segment of the midbrain was completely exposed, with
the length from the initial point of the basilar artery, and the
junction of the posterior communicating and posterior cerebral
arteries being 6.58 mm (5.42–7.84). The superior cerebellar artery
can also be divided into 4 segments according to its course: The
anterior pontomesencephalic below the oculomotor nerve, the lateral
pontomesencephalic course, below the trochlear and above the
trigeminal nerve, the cerebellomesencephalic course in the groove
between the cerebellum and the upper brain stem, and the cortical
which is distributed on the cerebellar surface. The length of
exposure of the anterior pontomesencephalic segment in this
approach of the superior cerebellar artery was approximately 5.6 mm
(4.38–6.82). However, the basilar artery was well exposed, with a
length of exposure above the middle segment of approximately 15.52
mm (14.22–16.70).
Results of relative structure
removed
The approach was conducted in the superior
petroclival region, going through the metasellar and alar bones. As
the approach deepened into the brain and narrowed the surgical
space, the anterior and posterior clinoid processes had to be
removed. The resection of the anterior clinoid process, had no
effect on the petroclival region the structure revealed, though it
increased the light in the surgical area. However, the removal of
the posterior clinoid process, inevitably results in the hemorrhage
of the sinus cavernosus due to the oculomotor nerve going through
its superolateral part. The removal of the posterior clinoid
process can enhance the exposure of the basilar artery, though
affecting less the exposure of the petroclival region. The removal
of the apex of the petrous part, can enhance the exposure to the
middle and inferior parts of petroclival region which has little
influence on the superior petroclival region. Some structures, such
as the trigeminal, vestibulocochlear, facial and abducent nerves
can be observed.
Discussion
Although CSF cytology, CT and MRI scanning are the
most essential techniques used for the diagnosis of brain tumors
(7), surgery on the superior
petroclival region has many difficulties. Neurosurgeons use
anterior aspect approaches including transcavernous transpetrous,
transcrusal and subtemporal keyhole (4,8,9).
Currently, the subtemporal approach is used more compared to the
others (10). With these
approaches, neurosurgeons have limited access and cannot achieve
complete results following surgery for meningioma and trigeminal
neuroma near the parasellar region and interpeduncular fossa
(11). In addition, a
frontotemporal craniotomy has been reported to provide a wide
exposure of the anterior temporal base, thus allowing oblique
access to the interpeduncular cistern with minimal brain retraction
(12). This study provides an
experimental basis for the temporal orbital-zygomatic arch approach
to the petroclival region, thus fully exposing the petroclival
region.
Previously, the subtemporal approach was uded
through the cerebellar tentorium, easily inducing severe temporal
lobe stretch (13). Studies have
been carried out to describe the meningeal anatomy related to this
approach as well as the dural incisions, to develop a subtemporal
interdural approach to dumbbell-shaped trigeminal schwannomas that
effectively converts a multiple-compartment tumor into a
single-compartment tumor (14). By
removing the petrous apex of the temporal bone and zygomatic arch,
doctors could achieve greater exposure. This can significantly
reduce the traction of the temporal lobe, and enlarge the surgical
perspective as well as the exposure of the petroclival region
(15). Hakuba et al were
first to propose the orbital zygomatic arch infratemporal approach
in 1986. Sixteen patients with parasellar tumors, 9 patients with
basilar tip aneurysms, and 1 patient with a P-1 distal aneurysm,
were operated on using this orbitozygomatic infratemporal approach,
with excellent results (16).
Deliberately excluding the microsurgical aspects of the lesions
treated, doctors observed that the frontotemporal-orbitozygomatic
approach was principally indicated for lesions requiring a
multidirectional approach, such as sphenopetroclival tumors,
aneurysms of the basilar tip and intracavemous lesions, while the
frontotemporal-orbital approach proved to be excellent for more
medial lesions, such as meningiomas of the luberculum sellae and
cramopharyngiomas (17). Standard
approaches to rostral middle fossa, such as the subtemporal,
pterional, or orbitozygomatic, require significant brain retraction
or manipulation of the temporalis muscle. Ong et al found
that the endoscopic sublabial transmaxillary approach provides safe
and direct access to this region (18). In comparison to subtemporal
approach, the present study found that tumors in the superior
petroclival region can grow to the posterolateral or middle
petroclival regions. However, when the main body of the tumor was
in the superior petroclival region, and grew to the direction of
the saddle and cavernous sinus, the frontotemporal-zygomatic arch
approach has more advantages. With the endoscope in the promotion
of brain surgery, the surgery can have the same operating range as
the frontotemporal-zygomatic arch approach, which can reach the
posterior cavernous sinus, suprasellar and superior petroclival
regions.
In summary, the endoscope is currently used more as
an aid, as it still cannot replace the role of the microscope.
Surgical limitations can be overcome by combining the surgical
microscope and endoscope (19).
The frontotemporal-zygomatic arch approach to the petroclival
region significantly exposes the various parts of the structure,
and can be used to reach the anterior petroclival region. However,
it should be noted that this leads to cerebrospinal fluid leakage
and intracranial infection. The application of this approach
requires further research.
Acknowledgements
This research study was supported by
the Health Bureau of Zhejiang Province (no. 2007A089).
References
|
1
|
Schwartz MS, Anderson GJ, Horgan MA,
Kellogg JX, McMenomey SO and Delashaw JB Jr: Quantification of
increased exposure resulting from orbital rim and orbitozygomatic
osteotomy via the frontotemporal transsylvian approach. J
Neurosurg. 91:1020–1026. 1999. View Article : Google Scholar
|
|
2
|
Campero A, Campero AA, Socolovsky M, et
al: The transzygomatic approach. J Clin Neurosci. 17:1428–1433.
2010. View Article : Google Scholar
|
|
3
|
Fournier HD, Mercier P and Roche PH:
Surgical anatomy of the petrous apex and petroclival region. Adv
Tech Stand Neurosurg. 32:91–146. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang H, Zhou F, Zhang R, Zhong P and Tan
D: Opening cranial cisterns by the anterior subtemporal keyhole
approach to the superior petroclival region: anatomical study and
comparative analysis. Surg Neurol. 72:124–130. 2009. View Article : Google Scholar
|
|
5
|
Behari S, Tyagi I, Banerji D, et al:
Postauricular, transpetrous, presigmoid approach for extensive
skull base tumors in the petroclival region: the successes and the
travails. Acta Neurochir (Wien). 152:1633–1645. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jian FZ, Santoro A, Innocenzi G, Wang XW,
Liu SS and Cantore G: Frontotemporal orbitozygomatic craniotomy to
exposure the cavernous sinus and its surrounding regions.
Microsurgical anatomy. J Neurosurg Sci. 45:19–28. 2001.
|
|
7
|
Liu J, Jia H, Yang Y, Dai W, Su X and Zhao
G: Cerebrospinal fluid cytology and clinical analysis of 34 cases
with leptomeningeal carcinomatosis. J Int Med Res. 37:1913–1920.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Roche PH, Mercier P and Fournier HD:
[Temporopolar epidural transcavernous transpetrous approach.
Technique and indications]. Neurochirurgie. 53:23–31. 2007.
|
|
9
|
Horgan MA, Delashaw JB, Schwartz MS,
Kellogg JX, Spektor S and McMenomey SO: Transcrusal approach to the
petroclival region with hearing preservation. Technical note and
illustrative cases. J Neurosurg. 94:660–666. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pichierri A, D'Avella E, Ruggeri A,
Tschabitscher M and Delfini R: Endoscopic assistance in the
epidural subtemporal approach and Kawase approach: anatomic study.
Neurosurgery. 67:ons29–37. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Behari S, Jaiswal S, Garg P and Jaiswal
AK: Bilateral eyebrow incision, mini-supraorbital craniotomy with
extended frontobasal approach for extensive anterior and middle
cranial fossa skull base tumors. Acta Neurochir (Wien).
153:527–531. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Deda H and Ugur HC: Zygomatic anterior
subtemporal approach for lesions in the interpeduncular cistern.
Skull Base. 11:257–264. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chernov MF: Far posterior subtemporal
approach to the dorsolateral brainstem and tentorial ring:
technique and clinical experience. Neurosurgery. 54:1028–1029.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Youssef S, Kim EY, Aziz KM, Hemida S,
Keller JT and van Loveren HR: The subtemporal interdural approach
to dumbbell-shaped trigeminal schwannomas: cadaveric prosection.
Neurosurgery. 59:ONS270–278. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Goel A: Extended lateral subtemporal
approach for petroclival meningiomas: report of experience with 24
cases. Br J Neurosurg. 13:270–275. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hakuba A, Liu S and Nishimura S: The
orbitozygomatic infratemporal approach: a new surgical technique.
Surg Neurol. 26:271–276. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Santoro A, Salvati M, Vangelista T,
Delfini R and Cantore GP: Fronto-temporo-orbito-zygomatic approach
and variants. Surgical technique and indications. J Neurosurg Sci.
47:141–147. 2003.PubMed/NCBI
|
|
18
|
Ong BC, Gore PA, Donnellan MB, Kertesz T
and Teo C: Endoscopic sublabial transmaxillary approach to the
rostral middle fossa. Neurosurgery. 62:30–37. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Inoue K, Seker A, Osawa S, Alencastro LF,
Matsushima T and Rhoton AL Jr: Microsurgical and endoscopic anatomy
of the supratentorial arachnoidal membranes and cisterns.
Neurosurgery. 65:644–665. 2009. View Article : Google Scholar : PubMed/NCBI
|