Introduction
Vascular regenerative therapy improves the flow of
blood to ischemic tissues by inducing neovascularization in
patients with vascular occlusive diseases (1–8).
Therapeutic methods include the direct delivery of vascular growth
factors including vascular endothelial growth factor, basic
fibroblast growth factor (bFGF) and hepatocyte growth factor, the
delivery of genes into host cells for the on-site production of
vascular growth factors and the direct delivery of somatic stem
cells capable of generating new vessels (9–13).
The arterial infusion of vascular growth factors may be used to
treat patients with vascular occlusive diseases in the future.
Hosaka et al (7) reported that in a rabbit hind-limb
ischemia model, functional collateral vessels were developed upon
the intra-arterial infusion of gelatin microspheres (GMS) bearing
bFGF. The arterially infused, GMS-attached bFGF was released slowly
and stimulated neovascularization. Vascular regeneration following
a single high dose of bFGF has also been demonstrated in rabbit
limb ischemia models (6,14). We attempted to induce vascular
regeneration by the iterative delivery of bFGF using an indwelling
reservoir catheter (15). We
hypothesized that, in addition to the sustained release of low-dose
bFGF from GMS, the subsequent iterative infusion of free-form bFGF
exerts a synergistic effect by maintaining high blood
concentrations of bFGF at the target site, thereby extending the
exposure time. In an effort to develop an easy-to-use test for
application in a clinical setting, we used a small-diameter
indwelling reservoir catheter to confirm improved vascular
regeneration.
Materials and methods
Animals
The study protocol was approved by the Animal
Experimentation Committee of Shiga University of Medical Science.
All experiments were performed according to the Animal Care
Guidelines of Shiga University of Medical Science. A total of nine
healthy female Japanese white rabbits weighing between 2.5 and 3.5
kg were purchased from Japan SLC Inc. (Shizuoka, Japan).
Rabbit model of hind-limb ischemia
The chronic hind-limb ischemia model was created
using our previously reported method (15). The rabbits were anesthetized with
intramuscular injections of a mixture of ketamine hydrochloride (25
mg/kg, Ketalar 50; Sankyo Yell Yakuhin Co. Ltd., Tokyo, Japan) and
medetomidine hydrochloride (0.1 mg/kg, Domitor, Meiji Seika Co.
Ltd., Tokyo, Japan). The left femoral artery was resected from the
inguinal ligament to the popliteal fossa and bifurcation of the
saphenous artery. The rabbits were then maintained for 21 days on a
normal diet.
Preparation of GMS and bFGF
impregnation
The GMS were of optimal specification as determined
in previous studies (7,15,16);
they were 30 μm in diameter and degraded within 2 weeks. Human
recombinant bFGF (group 1, 20 μg; group 2, 100 μg; Kaken
Pharmaceutical Co. Ltd., Tokyo, Japan) in 30 μl phosphate-buffered
saline (PBS) was added to 3 mg of the GMS at 4°C for 24 h to obtain
bFGF-impregnated GMS.
Reservoir implantation
At 21 days following femoral artery resection the
rabbits were anesthetized as described above and a heparin-coated
standard indwelling catheter (Toyobo Co. Ltd., Osaka, Japan) was
inserted using the left internal carotid artery approach. The
catheter was smaller than in our previous study (2 vs. 4-Fr)
(15). Prior to insertion, we
placed a 2-mm side hole 1.5 cm from the tip of the catheter. The
catheter tip was inserted into the deep femoral artery so that the
side hole was located at the branching of the internal iliac
artery. The port used in our earlier study (Clinical Supply Co.,
Ltd. Gifu, Japan) and the indwelling 2-Fr catheter were implanted
into the subcutaneous space of the nape of the neck.
Drug infusion protocols
The nine rabbits were divided into three equal
groups. The animals in group 1 received 20 μg bFGF-impregnated GMS
and then an additional 20 μg bFGF via the reservoir daily for four
consecutive days (total 100 μg), a single dose of 100 μg
bFGF-impregnated GMS was administered to group 2 and group 3 was
the saline control. The bFGF-impregnated GMS was mixed with 2 ml of
saline and infused over the course of approximately 3 min via the
reservoir port. In the three groups, the catheter was then
heparinized with 3 ml of saline containing 20 units of heparin. In
order to maintain its patency, the catheter was heparinized once
daily during the treatment period. The administration of the drug
via the port was possible without anesthesia.
Evaluation of collateral vessel
development
Collateral vessel development was evaluated by
recording the thigh temperature (thermography), blood pressure and
blood flow, and by pathological analysis. Evaluation procedures
were carried out prior to treatment and 4 weeks after the first or
only GMS administration. The rabbits were anesthetized as described
above prior to the evaluation procedures.
Thermographs (Neo Thermo TVS-700, Nippon Avionics,
Tokyo, Japan) were obtained at the surface of the lower abdomen and
bilateral thighs. The resolution was approximately 0.08°C and the
total number of pixels per view was 320×240. The region of interest
(ROI) was set at 15×15 pixels on the inner side of the bilateral
thighs to calculate the average and left-to-right ratios.
To measure the blood pressure at the popliteal
artery we used an ultrasonic Doppler flow detector (ES-1000SPII,
Hadeco Inc., Kanagawa, Japan). The left-to-right ratio was
determined with a sphygmomanometer with a pediatric cuff.
The blood flow was recorded using the same Doppler
flow detector and the left-to-right ratio was calculated.
Pathological analysis
The rabbits were sacrificed with overdose injections
of pentobarbital (Nembutal, Dainippon Sumitomo Pharma Co., Ltd.
Tokyo, Japan) at 4 weeks following treatment. Histological
specimens were prepared from the inner side of the left hind-limb
of each rabbit. Hematoxylin and eosin staining was performed to
assess the general morphology. Regenerated vessels were localized
by immunohistochemical staining with monoclonal CD31 antibody as
the primary antibody against endothelial cells. Cross-sections of
the semi-membranous muscle of the thigh were inspected at x100
magnification. The average number of CD31-positive cells per view
was counted in three consecutive views.
Statistical analysis
The temperature, blood pressure and blood flow data
were analyzed using the Student's t-test. Pathological data were
subjected to one-way ANOVA and the Tukey test. P<0.05 was
considered to indicate a statistically significant result. Analyses
were performed with SPSS software version 11.0 (SPSS, Inc.,
Chicago, IL, USA).
Results
Temperature, blood pressure, blood flow
and CD31-positive vessels
As listed in Table
I, among the three groups there was no significant difference
between the baseline values and the readings obtained at 4 weeks
post-treatment with respect to the left-to-right ratios of the
temperature (group 1, P=0.57; group 2, P=0.88; group 3, P=0.30),
blood pressure (group 1, P=0.59; group 2, P=0.83; group 3, P=0.96)
or blood flow (group 1, P=0.58; group 2, P=1.00; group 3, P=0.49;
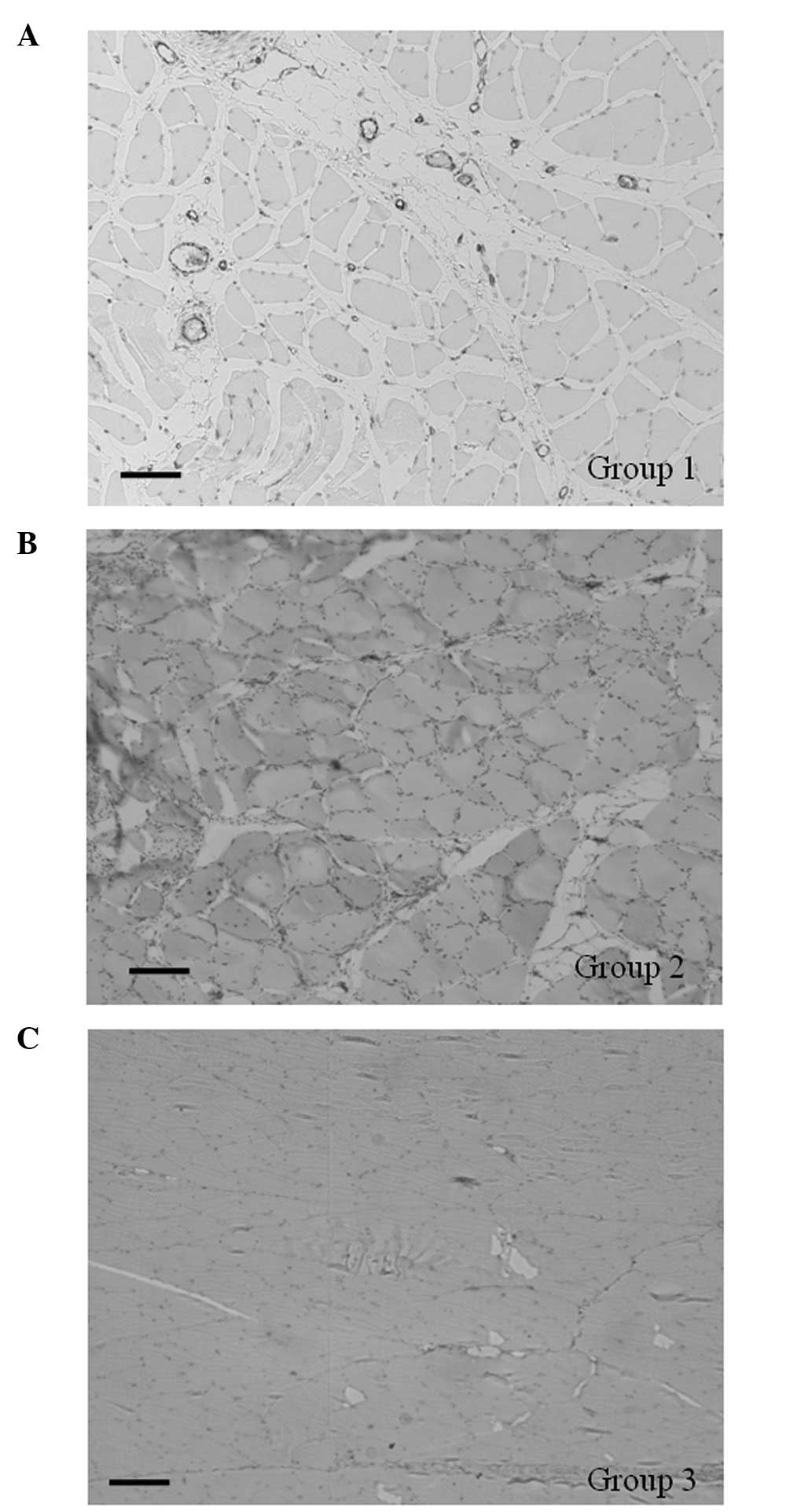
Table I). However, pathological
study of CD31-positive vessels demonstrated that the number of
positive vessels was significantly higher in group 1 than the other
groups (P<0.05; Table II,
Fig. 1).
 | Table I.Evaluation of collateral vessel
development. |
Table I.
Evaluation of collateral vessel
development.
| Group 1
| Group 2
| Group 3
|
|---|
| (Lt/Rt) | Pre-treatment | 4 weeks
following | P-value | Pre-treatment | 4 weeks
following | P-value | Pre-treatment | 4 weeks
following | P-value |
|---|
| Surface
temperature | 0.99 (0.01) | 0.98 (0.03) | 0.57 | 1.01 (0.04) | 1.01 (0.02) | 0.88 | 1.01 (0.02) | 1.04 (0.04) | 0.30 |
| Blood pressure | 0.54 (0.15) | 0.60 (0.10) | 0.59 | 0.80 (0.85) | 0.92 (0.26) | 0.83 | 1.05 (0.22) | 1.06 (0.32) | 0.96 |
| Blood flow | 0.63 (0.29) | 0.74 (0.07) | 0.58 | 1.18 (0.81) | 1.18 (0.39) | 1.00 | 0.73 (0.26) | 1.10 (0.78) | 0.49 |
| Table II.Average number of CD31-positive cells
in the left semimembranous muscle 4 weeks after treatment. |
Table II.
Average number of CD31-positive cells
in the left semimembranous muscle 4 weeks after treatment.
| Group 1 | Group 2 | Group 3 |
|---|
| CD31-positive
cells/mm2 | 540.32a,b (82.51) | 205.69a (68.89) | 44.36 (26.37) |
Discussion
We present pathological evidence that the iterative
delivery of low-dose bFGF (20 μg ×5) via an implanted reservoir
induced vascular regeneration more effectively than a single
administration of 100 μg. However, the evaluation methods used in
this experimental study cannot be applied in a clinical setting. In
efforts to make regenerative medicine relevant to interventional
radiology (IR), we modified the methods of Hosaka et al
(7) and Seko et al
(15) to obtain more favorable
regenerative results using a reservoir system for the delivery of
drugs.
We introduced a 4-Fr indwelling catheter in our
previous study to investigate vascular regeneration (15) and failed to observe vascular
changes on angiographs and in the body surface temperature, blood
pressure and blood flow. In the present study we provide
pathological evidence that iterative drug administration using a
reservoir effectively induced vascular regeneration. In our
previous study, angiographic findings, the body surface
temperature, blood pressure and blood flow were less favorable 2
weeks after placement of the reservoir. In accordance with the
hypothesis that the 4-Fr catheter was too big, we used a 2-Fr
indwelling catheter in the current study.
No significant differences were observed in physical
findings, including the body surface temperature, blood pressure
and blood flow, among the three rabbit groups. By contrast,
pathological study revealed that the number of CD31-positive cells
was significantly higher in rabbits treated by the iterative
delivery of low-dose bFGF via the 2-Fr catheter than it was when
iterative drug delivery was via the 4-Fr catheter (435.5
vessels/mm2 vs. 159.6/mm2) (15). We suggest that this difference was
due to replacing the larger with the smaller diameter catheter.
However, the number of vessels regenerated by the single
administration of bFGF was not affected by the size of the
catheter; 208.9/mm2 with the 4-Fr and
163.4/mm2 with the 2-Fr catheter. Thus, from a
pathological viewpoint, iterative or fractionated administration
using a small diameter catheter was more effective.
Certain institutions are already practicing vascular
regeneration therapy and the outcome is believed to be best
determined by assessing the degree of symptom improvement (2,17,18)
by, for example, perfusion study using CT or MRI, contrast-enhanced
ultrasonography or optical CT. We did not include angiographic
findings in our efficacy evaluation as our earlier study suggested
that their quantification was affected by the ROI used and thus
there were variations in the ratios of vascular regeneration.
Several previous studies have reported on how bFGF
bonds to GMS and is slowly released from GMS (19–22).
We obtained bFGF impregnated-GMS through the same method described
in these previous studies.
There are concerns that bFGF released slowly from
GMS may occlude vessels in the ischemic lower limb, resulting in
symptom exacerbation. To address this issue, Hosaka et al
(7) studied the effects of the
delivery of 3 mg of GMS of varying sizes on the status of the lower
rabbit limb. They concluded that GMS 29 μm in diameter efficiently
stimulated vascular regeneration without aggravating pre-existing
ischemia. Based on their findings, we used 3 mg of 30-μm diameter
GMS.
We placed the reservoir catheters so that the
infused bFGF was distributed slowly from the internal iliac artery
to the lower limb. An IR list would make it possible to pinpoint
the catheter placement on vessels requiring regeneration by
analyzing vascular images (23,24).
Our study on regenerative medicine may yield benefits for patients
with vascular diseases.
In conclusion, our evaluation of drug delivery
methods aimed at inducing neovascularization revealed that the
iterative low-dose (20 μg x5) delivery via an indwelling 2-Fr
catheter was more effective than the administration of a single
(100 μg) dose. Physical parameters, i.e. blood pressure, blood flow
and temperature, were not affected by either of the delivery
methods investigated.
References
|
1.
|
Lara-Hernandez R, Lozano-Vilardell P,
Blanes P, Torreguitart-Mirada N, Galmés A and Besalduch J: Safety
and efficacy of therapeutic angiogenesis as a novel treatment in
patients with critical limb ischemia. Ann Vasc Surg. 24:287–294.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Morishita R, Makino H, Aoki M, et al:
Phase I/IIa clinical trial of therapeutic angiogenesis using
hepatocyte growth factor gene transfer to treat critical limb
ischemia. Arterioscler Thromb Vasc Biol. 31:713–720. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Gabr H, Hedayet A, Imam U and Nasser M:
Limb salvage using intramuscular injection of unfractionated
autologous bone marrow mononuclear cells in critical limb ischemia:
a prospective pilot clinical trial. Exp Clin Transplant. 9:197–202.
2011.
|
|
4.
|
Powell RJ, Comerota AJ, Berceli SA, et al:
Interim analysis results from the RESTORE-CLI, a randomized,
double-blind multicenter phase II trial comparing expanded
autologous bone marrow-derived tissue repair cells and placebo in
patients with critical limb ischemia. J Vasc Surg. 54:1032–1041.
2011. View Article : Google Scholar
|
|
5.
|
Asano T, Kaneko E, Shinozaki S, et al:
Hyperbaric oxygen induces basic fibroblast growth factor and
hepatocyte growth factor expression, and enhances blood perfusion
and muscle regeneration in mouse ischemic hind limbs. Circ J.
71:405–411. 2007. View Article : Google Scholar
|
|
6.
|
Baffour R, Berman J, Garb JL, Rhee SW,
Kaufman J and Friedmann P: Enhanced angiogenesis and growth of
collaterals by in vivo administration of recombinant basic
fibroblast growth factor in a rabbit model of acute lower limb
ischemia: dose-response effect of basic fibroblast growth factor. J
Vasc Surg. 16:181–191. 1992. View Article : Google Scholar
|
|
7.
|
Hosaka A, Koyama H, Kushibiki T, et al:
Gelatin hydrogel micro-spheres enable pinpoint delivery of basic
fibroblast growth factor for the development of functional
collateral vessels. Circulation. 110:3322–3328. 2004. View Article : Google Scholar
|
|
8.
|
Nakajima H, Sakakibara Y, Tambara K, et
al: Therapeutic angio-genesis by the controlled release of basic
fibroblast growth factor for ischemic limb and heart injury: toward
safety and minimal invasiveness. J Artif Organs. 7:58–61. 2004.
View Article : Google Scholar
|
|
9.
|
Qu D, Li J, Li Y, Gao Y, Zuo Y, Hsu Y and
Hu J: Angiogenesis and osteogenesis enhanced by bFGF ex vivo gene
therapy for bone tissue engineering in reconstruction of calvarial
defects. J Biomed Mater Res A. 96:543–551. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Yasuda Y, Koyama H, Tabata Y, Fujihara Y,
Oba M, Uchinuma E and Takato T: Controlled delivery of bFGF
remodeled vascular network in muscle flap and increased perfusion
capacity via minor pedicle. J Surg Res. 147:132–137. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Katsuno A, Aimoto T, Uchida E, Tabata Y,
Miyamoto M and Tajiri T: The controlled release of basic fibroblast
growth factor promotes a rapid healing of pancreaticojejunal
anastomosis with potent angiogenesis and accelerates apoptosis in
granulation tissue. J Surg Res. 167:166–172. 2011. View Article : Google Scholar
|
|
12.
|
Matsuura M, Okazaki K, Nishio A, et al:
Therapeutic effects of rectal administration of basic fibroblast
growth factor on experimental murine colitis. Gastroenterology.
128:975–986. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Song K, Rao NJ, Chen ML, Huang ZJ and Cao
YG: Enhanced bone regeneration with sequential delivery of basic
fibroblast growth factor and sonic hedgehog. Injury. 42:796–802.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Takeshita S, Zheng LP, Brogi E, et al:
Therapeutic angiogenesis. A single intraarterial bolus of vascular
endothelial growth factor augments revascularization in a rabbit
ischemic hind limb model. J Clin Invest. 93:662–670. 1994.
View Article : Google Scholar
|
|
15.
|
Seko A, Nitta N, Sonoda A, Ohta S,
Takahashi M, Murata K and Tabata Y: Vascular regeneration by
repeated infusions of basic fibroblast growth factor in a rabbit
model of hind-limb ischemia. AJR Am J Roentgenol. 192:W306–310.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Tabata Y and Ikada Y: Synthesis of gelatin
microspheres containing interferon. Pharm Res. 6:422–427. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Marui A, Tabata Y, Kojima S, et al: A
novel approach to therapeutic angiogenesis for patients with
critical limb ischemia by sustained release of basic fibroblast
growth factor using biodegradable gelatin hydrogel: an initial
report of the phase I-IIa study. Circ J. 71:1181–1186. 2007.
View Article : Google Scholar
|
|
18.
|
Henry TD, Hirsch AT, Goldman J, et al:
Safety of a non-viral plasmid-encoding dual isoforms of hepatocyte
growth factor in critical limb ischemia patients: a phase I study.
Gene Ther. 18:788–794. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Isogai N, Morotomi T, Hayakawa S, Munakata
H, Tabata Y, Ikada Y and Kamishi H: Combined chondrocyte-copolymer
implantation with slow release of basic fibroblast growth factor
for tissue engineering an auricular cartilage construct. J Biomed
Mater Res A. 74:408–418. 2005. View Article : Google Scholar
|
|
20.
|
Igai H, Chang SS, Gotoh M, et al:
Regeneration of canine tracheal cartilage by slow release of basic
fibroblast growth factor from gelatin sponge. ASAIO J. 52:86–91.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Igai H, Yamamoto Y, Chang SS, Yamamoto M,
Tabata Y and Yokomise H: Tracheal cartilage regeneration by slow
release of basic fibroblast growth factor from a gelatin sponge. J
Thorac Cardiovasc Surg. 134:170–175. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Igai H, Chang SS, Gotoh M, Yamamoto Y,
Yamamoto M, Tabata Y and Yokomise H: Widespread and early tracheal
cartilage regeneration by synchronous slow release of b-FGF and
BMP-2. ASAIO J. 55:266–270. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Hamada A, Yamakado K, Nakatsuka A, Takaki
H and Takeda K: Clinical utility of coaxial reservoir system for
hepatic arterial infusion chemotherapy. J Vasc Interv Radiol.
18:1258–1263. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Liang HL, Huang JS, Lin YH, Lai KH, Yang
CF and Pan HB: Hepatic arterial infusion chemotherapy for advanced
hepatocellular carcinoma by placing a temporary catheter via the
subclavian route. Acta Radiol. 48:734–740. 2007. View Article : Google Scholar : PubMed/NCBI
|