Introduction
Frontolateral partial laryngectomy and
laryngofissure for cordectomy are commonly used conservative
approaches in the treatment of early laryngeal cancer (1–3). In
these procedures, tracheotomy is a standard intervention used to
alleviate dyspnea caused by postoperative edema and the consequent
shrinking of the laryngeal cavity. The goals of oncological surgery
of the larynx are to remove the local disease and conserve the
physiological functioning of the larynx, while preserving quality
of life. Therefore, a number of procedures have been proposed to
minimize the extent of postoperative morbidity. Rebeiz et
al(4) reported the successful
completion of a combined endoscopic and open approach without
tracheotomy for T1 and T2 glottic and supraglottic cancers in a
series of 5 patients. In the case of small primary laryngeal
tumors, traditional partial laryngectomy is often considered to be
too aggressive due to the associated complications. We have
previously described the development of a novel approach, modified
frontolateral partial laryngectomy without tracheotomy, and
reviewed the results in 65 patients who underwent this new
procedure (5). In the present
study, animal experiments were performed in order to objectively
evaluate the airway provided by modified frontolateral partial
laryngectomy without tracheotomy compared with other commonly used
procedures.
Materials and methods
Animals
The present study was approved by the Animal
Research Ethics Committee of Shanghai Jiao Tong University Medical
College (Affiliated Shanghai First People’s Hospital, Shanghai,
China) and was conducted in strict compliance with its requirements
and decisions. Male and female mongrel dogs of various ages,
weighing 9–15 kg were used for the experiment. A total of 16 dogs
were divided into 2 groups denoted ex vivo and in
vivo. The ex vivo group contained 6 dogs and the in
vivo group contained 10 dogs.
Experimental procedures of the ex vivo
group
The dogs were sacrificed and their larynges were
excised for anatomical study and placed in appropriate individual
plastic vessels. The supraglottic tissue was removed to expose the
true vocal folds. Stepwise procedures were performed and, after
each step, the vocal folds were photographed from a superior
perspective using a grid placed over the vocal folds to measure the
glottal area.
Photographic images of the glottis were captured
prior to performing any procedures on the larynx. The thyroid
laminae were then incised vertically 2–3 mm posterior to the
anterior commissure and removed. In all larynges, ∼20% of the
laryngeal cavity was excised. The incisal margins of the vocal
folds were sutured to the ipsilateral thyroid perichondrium and the
glottis was then photographed. Finally, the incisal edges of the
thyroid laminae were sutured together to reconstruct the anterior
commissure. The glottis was then photographed for the third
time.
Experimental procedures of the in vivo
group
The laryngeal cavity was isolated and adequately
exposed. The epiglottis was captured and pulled forward and upward
after the mucosa of the epiglottic vallecula was cut open. The
mucosa of the lateral pharyngeal walls was cut to pull the whole
larynx out. Photographic images of the glottis were then captured
at the maximum phase to measure the maximum phase area of the
untreated glottis. Right cordectomy was performed via
laryngofissure and the incisal margins of the thyroid cartilage
were sutured together; the glottis was then photographed again at
maximum phase. Subsequently, modified frontolateral partial
laryngectomy was performed according to the procedure described
previously (5,6) and the maximum phase of the glottis
was photographed for the third time.
Data processing
Images of the ex vivo group were processed
using AutoCAD2004 image software and the following data were
obtained: i) area of the untreated glottis of the ex vivo
larynx; ii) area of the glottis of the ex vivo larynx with
the incisal margins of the thyroid cartilage sutured following
frontolateral partial laryngectomy; and iii) area of the glottis of
the ex vivo larynx following frontolateral partial
laryngectomy with the incisal margins of the anterior commissure
sutured to the homolateral perichondrium of the thyroid
cartilage.
Images of the in vivo group were processed
using AutoCAD2004 image software and the following data were
obtained: i) the maximum phase area of the untreated glottis of the
in vivo larynx; ii) the maximum phase area of the glottis of
the in vivo larynx following right cordectomy via
laryngofissure; and iii) the maximum phase area of the glottis of
the in vivo larynx following modified frontolateral partial
laryngectomy.
Statistical analysis
The data of ex vivo experiments were compared
by Student’s t-test, since the data were normally distributed. The
data of the in vivo group was compared using ANOVA and
Newman Keuls test.
Results
Experimental results of the ex vivo
group
The ex vivo glottises were stationary and the
areas were relatively constant without the effect of respiration
and thus simple to measure. The distance and angle of the scales
may greatly affect measurements of the glottic area. Therefore, in
the present study the scales were placed strictly on the same plane
as the vocal cords and photographed at a distance of 30 cm to
provide accurate measurements.
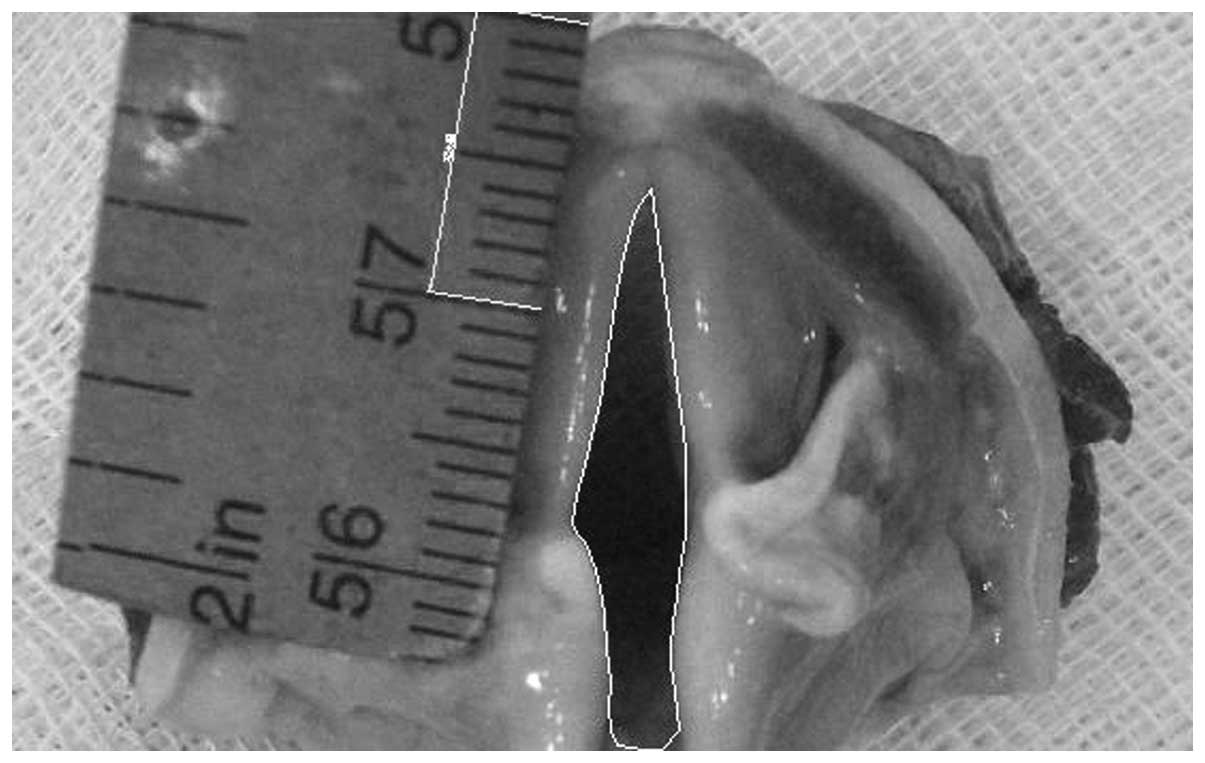
The processing of all images was completed using
AutoCAD2004 image software. An image of the primitive glottis is
shown in Fig. 1, with white lines
which are polylines of the glottic area. The scale is a standard
for the glottic area.
The experimental results of the ex vivo group
are shown in Table I. The 3 sets
of data are normally distributed. A paired t-test of the areas of
the primitive glottises and glottises with closed thyroid cartilage
revealed no significant differences (P>0.05). However,
significant differences were revealed by a paired t-test of the
areas of the primitive glottises and glottises with opened thyroid
cartilage (P<0.05). The interior of the larynx in cross-section
is triangular. In the experiments on the ex vivo group,
attempts were made to confirm whether changing the shape of the
glottis (with the front part resected) to a trapezoid by suturing
the sternohyoid muscle to the laryngeal lumen, significantly
decreases the area of the glottis. The statistical data above show
that area of the glottis was enlarged in certain cases by changing
its shape to a trapezoid.
 | Table I.Experimental data concerning glottis
area in the ex vivo group. |
Table I.
Experimental data concerning glottis
area in the ex vivo group.
| Primitive glottis
(mm2) | Glottis with sutured
anterior margins of thyroid cartilage (mm2) | Glottis with anterior
ends of thyroid cartilage opened using a cartilage flap
(mm2) |
|---|
| No. 1 | 48.41 | 19.52 | 61.15 |
| No. 2 | 32.61 | 15.14 | 39.8 |
| No. 3 | 54.78 | 27.57 | 54.18 |
| No. 4 | 16.28 | 9.91 | 38.65 |
| No. 5 | 40.37 | 14.67 | 39.37 |
| No. 6 | 45.81 | 30.05 | 66.22 |
| Mean | 39.71 | 19.48 | 49.90 |
| SD | 13.71 | 7.89 | 12.25 |
| t-score | | 5.74 | 2.47 |
| P-value | | 0.023 | 0.057 |
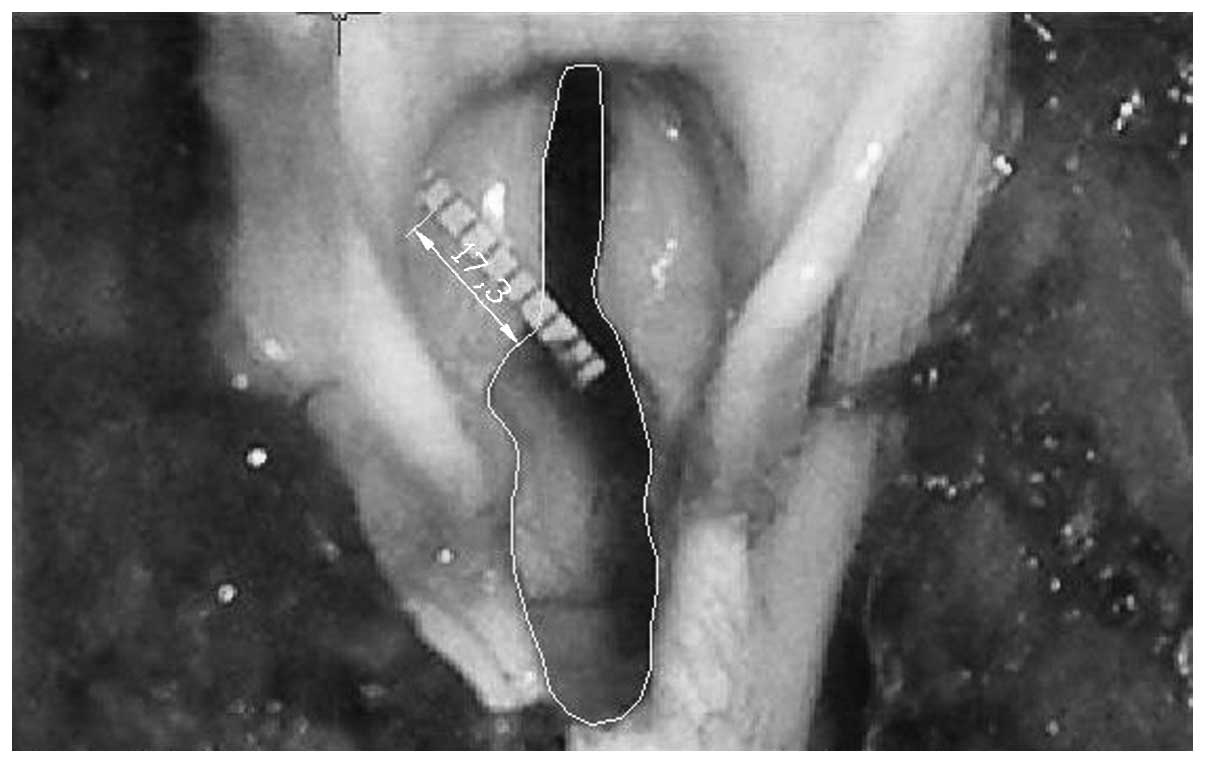
A glottis following modified frontolateral partial
laryngectomy is shown in Fig. 2.
The white lines are polylines of the glottic area and the scale is
a standard for the vocal area.
Experimental results of the in vivo
group
The experimental results of the in vivo group
are shown in Table II. ANOVA was
performed on all data and the Newman-Keuls method was used for
group comparisons. No significant differences were observed between
the glottic area before and after cordectomy (Q=0.047, P>0.05)
or between the glottic areas prior to cordectomy and following
laryngoplasty (Q=8.78, P>0.05), which demonstrates that modified
frontolateral partial laryngectomy does not reduce the glottic area
more than cordectomy does. However, the tissue excised by the
cordectomy did not include the anterior commissure. When the
anterior commissure is involved in carcinoma, the cordectomy is not
a feasible therapy. No significant difference was identified
between the glottic area prior to surgery and following
laryngoplasty (Q=8.74, P>0.05). The statistical data revealed
that the glottic area was not reduced significantly following
laryngoplasty, which supports the feasibility of modified
frontolateral partial laryngectomy without tracheotomy.
| Table II.Experimental data concerning glottis
area in the in vivo group. |
Table II.
Experimental data concerning glottis
area in the in vivo group.
| Glottis before
operation (mm2) | Glottis after
laryngofissure (mm2) | Glottis after
laryngoplasty (mm2) |
|---|
| No. 1 | 49.83 | 54.28 | 43.58 |
| No. 2 | 17.35 | 13.55 | 13.53 |
| No. 3 | 24.62 | 14.68 | 12.28 |
| No. 4 | 33.79 | 26.64 | 23.28 |
| No. 5 | 29.16 | 28.91 | 18.17 |
| No. 6 | 45.53 | 51.57 | 37.06 |
| No. 7 | 36.96 | 40.4 | 29.16 |
| No. 8 | 18.33 | 18.54 | 15.16 |
| No. 9 | 62.68 | 68.17 | 46.22 |
| No. 10 | 65.04 | 67.02 | 57.45 |
| Mean | 38.33 | 38.38 | 29.59 |
| SD | 17.08 | 20.92 | 15.78 |
| Q-value | - | 0.05 | 8.74 |
| P-value | - | 0.98 | 0.25 |
Discussion
Conventionally, laryngofissure and cordectomy have
been the primary means of eradicating early and selected invasive
glottic squamous cell carcinomas (3). A number of studies have reported the
efficacy of microendoscopic laser surgery in obtaining success
rates in early cancers similar to conventional partial laryngectomy
(7,8). However, when the anterior commissure
is involved, partial laryngectomy is the optimal treatment option
for glottic cancers since the anatomical region is not easily
visualized endoscopically and safe excision margins may be
compromised. Furthermore, the anterior commissure lacks an
anatomical barrier to regional spread such as the adjacent
perichondrium of the thyroid cartilage. Consequently, the intrinsic
vulnerability of this structure may lead to unrecognized
microinvasion or macroinvasion, resulting in the mistreatment of
highly progressed T4a cancers that are incorrectly diagnosed as
early glottic lesions (2).
Therefore, partial laryngectomy is considered to be superior to
laser surgery in the treatment of glottic cancer involving the
anterior commissure.
Tracheotomy is routinely performed in patients
undergoing partial laryngectomy due to the high risk of
postoperative dyspnea originating from a narrowed laryngeal lumen
or laryngeal edema. Postoperative care for the tracheotomy is
burdensome for the patient and provider and is associated with
prolonged hospitalization and significant morbidity. Even temporary
tracheotomy is associated with increased complication rates,
suggesting that prophylactic tracheotomy at the time of surgery is
less than ideal. Although Muscatello et al(3) and Wolfensberger and Dort (9) have reportedly avoided tracheotomy in
the treatment of glottic carcinomas with cordectomy via
laryngofissure or endoscopic laser surgery, the feasibility of
frontolateral partial laryngectomy without tracheotomy remains
uncertain. In 2005, Brumund et al(10) reported a series of 270 patients
with invasive glottic squamous cell carcinomas managed with
frontolateral partial laryngectomy without tracheotomy. The present
study examined the efficacy of a novel surgical approach, the
modified frontolateral partial laryngectomy without tracheotomy, in
achieving tumor control and restoring proper laryngeal function
(11).
The feasibility and effectiveness of the modified
frontolateral partial laryngectomy are functions of the anatomical
association between the laryngeal lumen and its surrounding
structures. The interior of the larynx in cross-section is
triangular due to the contour of the thyroid cartilage.
Geometrically, the area of a triangle is less than that of a
trapezoid or rectangle of equivalent base and height. In the
present approach, we aimed to transform the natural triangular
contour into a trapezoid to achieve a greater cross-sectional area.
To achieve this, the sternohyoid muscle was sutured to the
laryngeal lumen and the thyroid lamina was vertically incised,
resulting in abduction of the anterior part of the thyroid
cartilage. In addition, the muscular fascia was retroflexed and
sutured to the contra-lateral side, bringing the larynx into the
desired trapezoidal or rectangular conformation. To expand the
breadth of the laryngeal cavity, the sternohyoid fascia was
reverted, covering the anterior larynx and completing the
ladder-shaped lumen. Although the anteroposterior diameter of the
neolarynx was decreased, the cross-sectional area was sufficiently
enlarged to allow normal respiration, even in the absence of an
endotracheal tube.
In the present study, on the basis of clinical
study, animal model establishment and computer technology, it was
demonstrated that expanding the anterior end of the laryngeal
cavity and changing the shape from the original triangle into a
trapezoid with equal bottom length and height was able to
considerably increase the effective respiratory area. This result
demonstrates the theoretical basis of modified frontolateral
partial laryngectomy and validates its efficacy and
feasibility.
In conclusion, these animal experiments demonstrated
the feasibility of modified frontolateral partial laryngectomy
without tracheotomy. The present data indicate that it is a safe
and reliable method for excising the anterior 20% of the vocal cord
and thyroid cartilage without the necessity of tracheotomy. This
procedure, therefore, represents a new, less invasive technique for
the treatment of glottic squamous cell carcinoma.
Acknowledgements
The authors would like to thank
Professor Xiaoyan Li and Allison Maytag for critical reading of the
manuscript.
References
|
1.
|
Dedivitis RA, Guimarães AV and Guirado CR:
Outcome after partial frontolateral laryngectomy. Int Surg.
90:113–118. 2005.PubMed/NCBI
|
|
2.
|
Olsen KD and DeSanto LW: Partial vertical
laryngectomy - indications and surgical technique. Am J
Otolaryngol. 11:153–160. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Muscatello L, Laccourreye O, Biacabe B, et
al: Laryngofissure and cordectomy for glottic carcinoma limited to
the mid third of the mobile true vocal cord. Laryngoscope.
107:1507–1510. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Rebeiz EE, Wang Z, Annino DJ, et al:
Preliminary clinical results of window partial laryngectomy: a
combined endoscopic and open technique. Ann Otol Rhinol Laryngol.
109:123–127. 2000. View Article : Google Scholar
|
|
5.
|
Dong P, Li X, Xie J, Li L and Xu H:
Modified frontolateral partial laryngectomy without tracheotomy.
Otolaryngol Head Neck Surg. 141:70–74. 2009. View Article : Google Scholar
|
|
6.
|
Dong P, Wang Q, Li XY, et al: Modified
frontolateral partial larnygectomy without tracheostomy for early
laryngeal cancer of the true vocal cord. Zhonghua Zhong Liu Za Zhi.
29:707–709. 2007.(In Chinese).
|
|
7.
|
Gallo A, de Vincentiis M, Manciocco V, et
al: CO2 laser cordectomy for early-stage glottic
carcinoma: a long-term follow-up of 156 cases. Laryngoscope.
112:370–374. 2002.
|
|
8.
|
Bocciolini C, Presutti L and Laudadio P:
Oncological outcome after CO2 laser cordectomy for
early-stage glottic carcinoma. Acta Otorhinolaryngol Ital.
25:86–93. 2005.PubMed/NCBI
|
|
9.
|
Wolfensberger M and Dort JC: Endoscopic
laser surgery for early glottic carcinoma: a clinical and
experimental study. Laryngoscope. 100:1100–1105. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Brumund KT, Gutierrez-Fonseca R, Garcia D,
et al: Frontolateral vertical partial laryngectomy without
tracheotomy for invasive squamous cell carcinoma of the true vocal
cord: a 25-year experience. Ann Otol Rhinol Laryngol. 114:314–322.
2005.PubMed/NCBI
|
|
11.
|
Dong P, Wang J, Jin B, et al: Surgery on
laryngeal carcinoma - retrospective analysis of 205 cases. Zhonghua
Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 40:591–594. 2005.(In
Chinese).
|