Introduction
Endoscopic third ventriculostomy (ETV) is widely
used to treat hydrocephalus caused by aqueduct obstruction
(1–4). However, ETV has the risk of serious
complications, including the rupture of the basilar artery and
other injuries to the hypothalamus. Endoscopic aqueductoplasty (EA)
has gradually become an alternative treatment for obstructive
hydrocephalus (5,6). However, there are a limited number of
studies on aqueductoplasty. There have been <50 reported cases
since the 1990s. The average follow-up period is <3 years and
the success rate ranges from 30 to 100% (5,7–11).
EA may become an alternative option for patients with obstructive
hydrocephalus due to aqueduct stenosis. However, an appropriate
method must first be established to control the surgical
indications prior to surgery and to evaluate the effectiveness of
surgery. For two decades, phase-contrast cine magnetic resonance
imaging (MRI) has been used to study the physiological state of the
cerebrospinal fluid (CSF) circulation, to diagnose hydrocephalus
and to evaluate the efficacy of third ventriculostomy. This type of
MRI has been widely used by clinicians since it is non-invasive and
highly sensitive (12–14). In this study, phase-contrast cine
MRI was used for the preoperative diagnosis of obstructive
hydrocephalus and the postoperative follow-up, with satisfactory
outcomes.
Patients and methods
Patients
A total of 274 patients with obstructive
hydrocephalus who underwent endoscopic neurosurgery between
February 2007 and August 2009 were included in our study. Among
these patients, 23 had aqueduct reconstruction (Table I). The following criteria were used
to select patients for aqueductoplasty (Fig. 1): i) all patients with membranous
obstruction of the aqueduct and ii) all cases with thickening of
the ventricle floor.
 | Table ISummary of 23 patients. |
Table I
Summary of 23 patients.
| Patient | Gender/age (months or
years) | Diagnosis | Symptoms | Surgical outcome |
|---|
| 1 | F/9 y | AO | Headache,
vomiting | Improved |
| 2 | M/9 m | AO | Increased head
circumference | Improved |
| 3 | F/17 m | AO | Increased head
circumference | Improved |
| 4 | M/5 y | AO | Headache,
vomiting | Improved |
| 5 | M/5 y | AO | Increased head
circumference | Improved |
| 6 | F/5 y | AO | Increased head
circumference | Improved |
| 7 | F/2 y | AO | Increased head
circumference | Improved |
| 8 | M/18 m | AO | Increased head
circumference | Improved |
| 9 | M/19 m | AO | Increased head
circumference | Improved |
| 10 | F/33 y | AO | Headache,
vomiting | Improved |
| 11 | M/9 m | IVH | Instability of
movement | Failure |
| 12 | F/3 y | AO | Instability of
movement | Improved |
| 13 | F/16 m | AO | Increased head
circumference | Improved |
| 14 | M/26 y | AO | Headache,
vomiting | Improved |
| 15 | F/28 y | AO | Headache,
vomiting | Improved |
| 16 | F/3 m | IVH | Increased head
circumference | Failure |
| 17 | M/11 m | AO | Increased head
circumference | Improved |
| 18 | M/20 y | AO | Headache,
vomiting | Improved |
| 19 | F/24 y | AO | Headache,
vomiting | Improved |
| 20 | F/67 y | AO | Blurred vision, loss
of consciousness | Improved |
| 21 | F/6 m | AO | Increased head
circumference | Improved |
| 22 | F/16 m | AO | Increased head
circumference | Improved |
| 23 | M/17 m | AO | Increased head
circumference | Improved |
Twenty-one cases had simple membranous obstruction
at the aqueduct fistula, whereas two cases had hydrocephalus due to
intraventricular hemorrhage. In total, 10 males and 13 females
underwent aqueductoplasty, with an average age of 10.5 years (the
patients’ age ranged from 3 months to 67 years). Prior to surgery,
the patients had a variety of clinical symptoms, which included
headaches, nausea, vomiting, blurred vision, unstable movement, an
increased head circumference and a loss of consciousness. A
preoperative phase-contrast cine MRI scan confirmed the aqueduct
obstruction and the cessation of CSF flow in the aqueduct. This
study was conducted in accordance with the Declaration of Helsinki.
This study was conducted with approval from the Ethics Committee of
Xiangya Hospital, Central-South University (Changsha, China).
Written informed consent was obtained from all participants.
Phase-contrast cine MRI scans
All subjects underwent conventional head MRI
examination with a 1.5 Tesla MRI scanner (Signa Horizon MRI system;
GE Healthcare, Piscataway, NJ, USA). The scanning sequence included
the T1WI, T2WI and fluid attenuated inversion recovery (FLAIR)
sequences. The following scan parameters were set for the axial
position: repetition time/echo time (TR/TE), 450/12 msec; field of
view (FOV), 27×27 cm2; slice thickness, 8 mm; interval,
0.8 mm; and matrix, 256×256; whereas for the sagittal position, the
parameters were: TR/TE, 360/12 msec; FOV, 30×30 cm2;
slice thickness, 5 mm; interval, 0.6 mm; and matrix, 256×192. The
sagittal scout view sequences were used as localizers to select the
anatomic levels for the flow velocity measurements. The CSF flow
velocity was measured in the transverse plane perpendicular to the
mid-collicular level of the aqueduct (Fig. 2), in terms of the peak systolic or
diastolic velocity. The aqueduct was identified and the circular
region of interest (ROI) was placed inside it. For the GE MRI
phase-contrast cine analysis system, the following scan parameters
were used in the axial position: TR/TE at the minimum; FOV, 28×28
cm2; slice thickness, 10 mm; matrix, 256×192; number of
excitations (NEX), 2; flip angle, 15°; velocity encoding (Venc), 10
cm/sec; and slice number, 9; whereas the parameters in the sagittal
position were: TR/TE at the minimum; FOV, 14×14 cm2;
section thickness, 5 mm; matrix, 256×192; NEX, 2; flip angle, 15°;
Venc, 10 cm/sec; and slice number, 20. The encoding direction was
from the top to the bottom. The peripheral gating was selected for
the scans without slice-overlap, respiratory compensation or flow
compensation. The total scanning time was 20–25 min.
Surgical equipment
Surgical equipment included a 3.8 mm Rudolf-Fujinon
flexible electronic endoscope (Fujifilm Corporation, Tokyo, Japan),
a set of matched single and bipolar coagulation devices, pairs of
biopsy forceps and scissors and a 2F Fogarty balloon catheter.
Surgical procedure
Under general anaesthesia, patients were placed in
the supine position with the head tilted at 30°. A scalp incision
was made above the forehead hairline and 2 cm from the two sides of
the median line. A 2-cm hole was drilled into the skull and a
sheath was used to puncture the lateral ventricle. A
ventriculoscope was inserted into the ventricle to view the
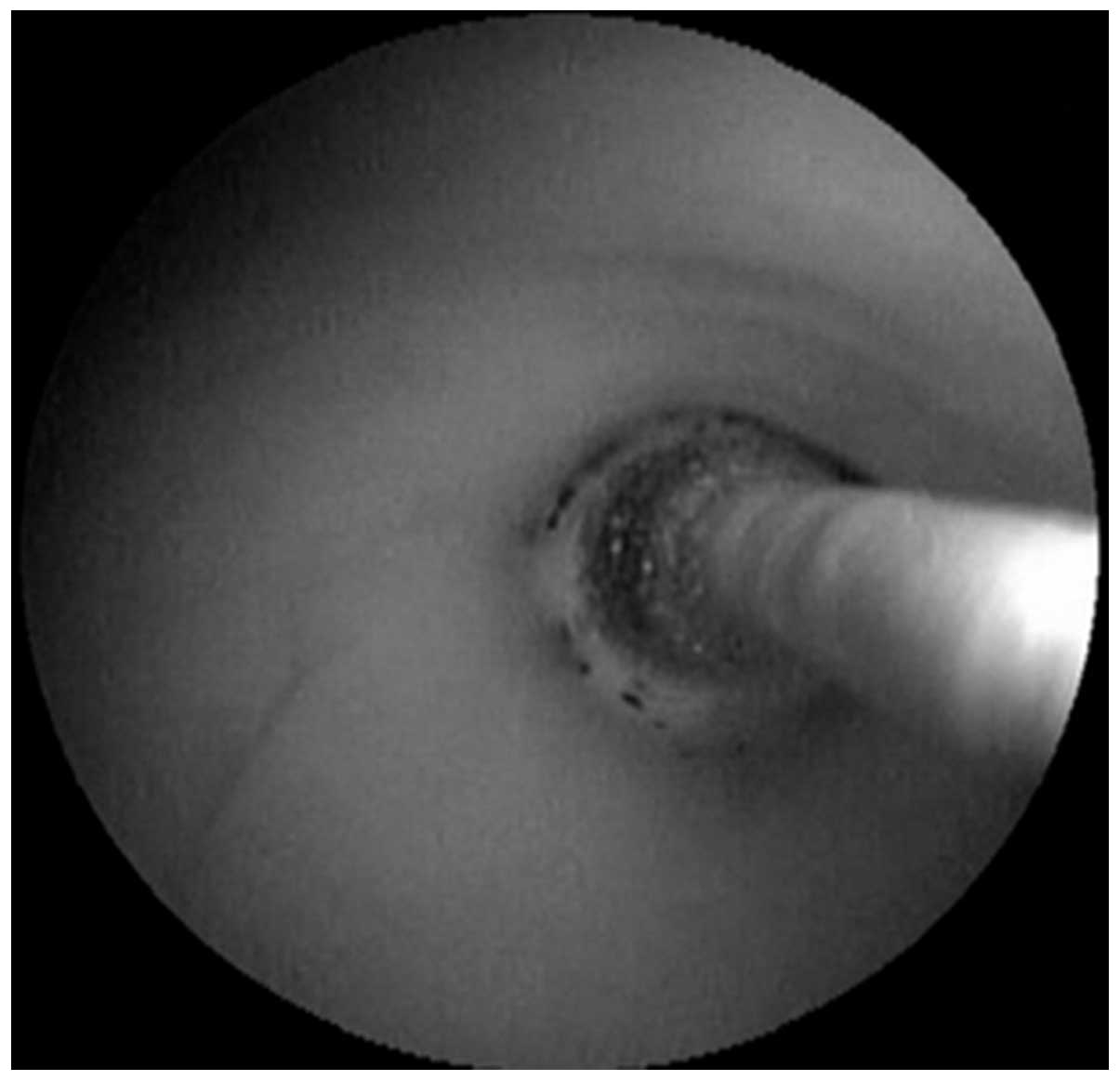
aqueduct fistula. The catheter was pushed through the membranous
obstruction and short aqueductal stenosis such that its balloon
portion was at the lower fistula of the aqueduct. The balloon was
filled with 0.1–0.2 ml normal saline to expand the aqueduct to a
diameter of 4 mm (Fig. 3). Then,
the endoscope was inserted further into the fourth ventricle to
explore whether the foramen of Luschka was obstructed (15,16).
Follow-up
All patients underwent a routine phase-contrast cine
MRI scan one week after surgery to determine whether obstruction of
the aqueduct remained. The mean follow-up duration was 19 months
(range, 16–32 months). All patients returned for follow-up after
>1 year and the phase-contrast cine MRI was repeated. Two
patients immediately had MRI scans when the symptoms of
intracranial hypertension recurred.
Statistical analysis
Statistical evaluation of the data was performed
using a commercially available software package (SPSS System for
Windows, version 17.0; SPSS Inc., Chicago, IL, USA). The mean and
standard deviation were calculated for each parameter. The t-test
was used for comparisons of different age groups. P<0.05 was
considered to indicate a statistically significant difference.
Results
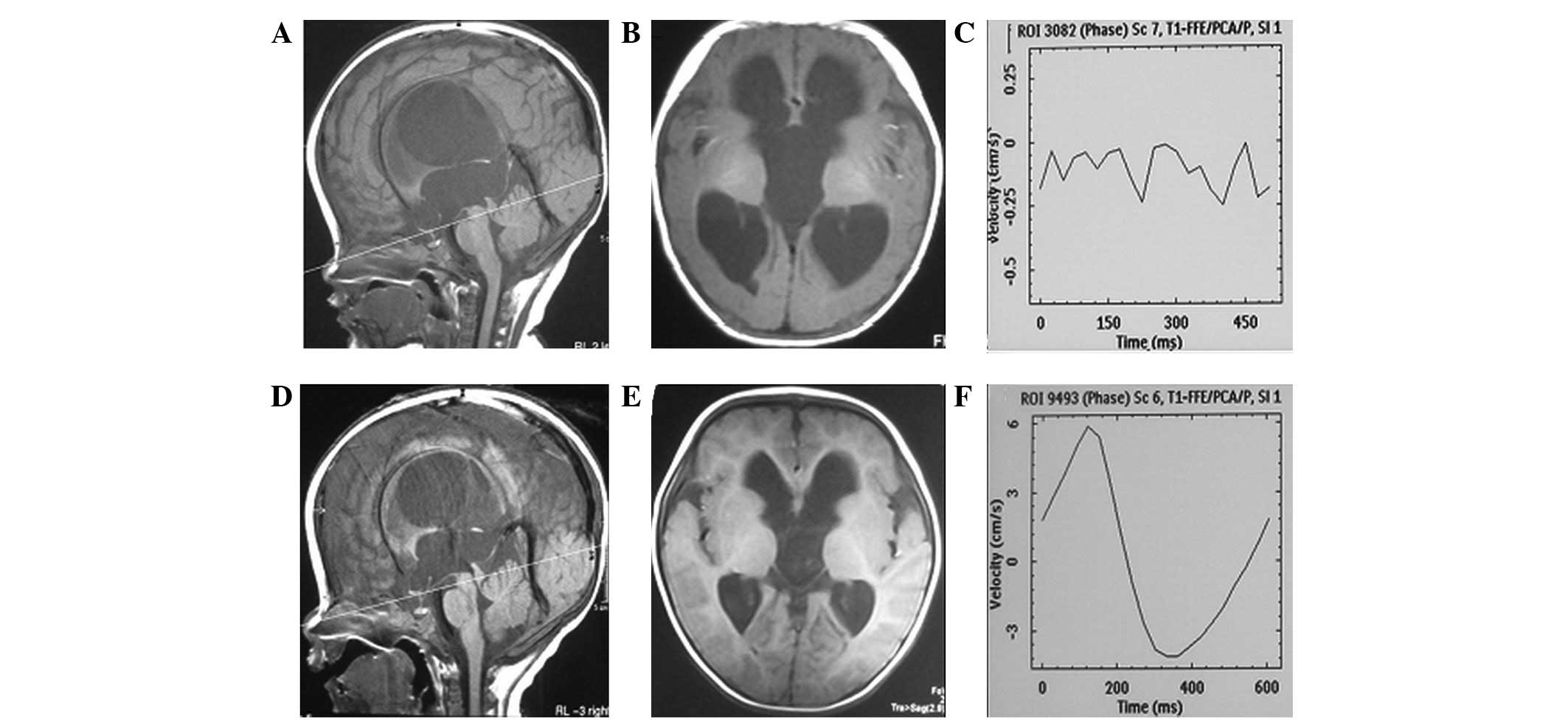
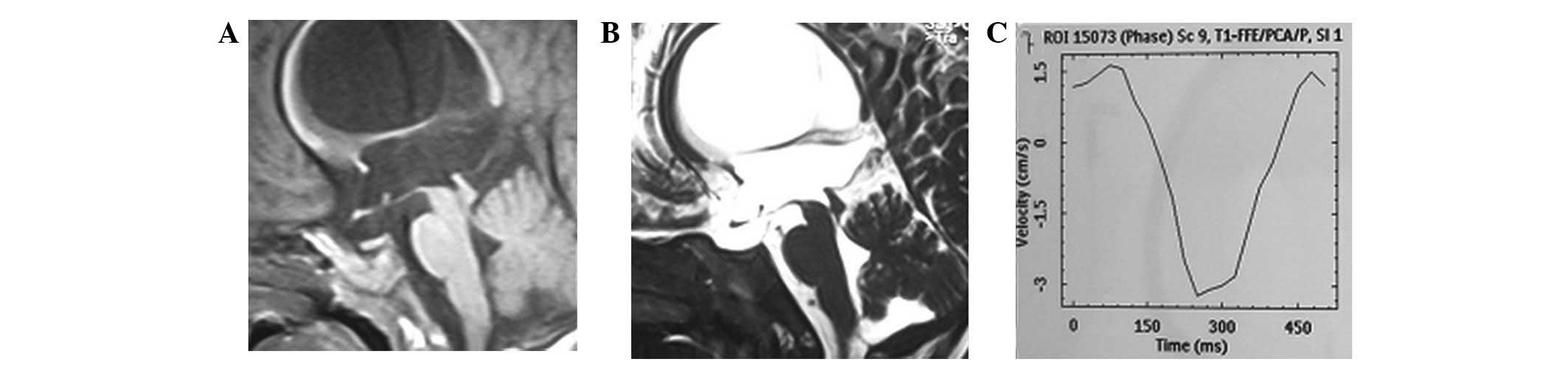
Complete aqueduct obstruction was revealed by
preoperative phase-contrast cine MRI in 23 patients (Figs. 2 and 4). During surgery, a membranous
obstruction at the upper aqueduct, as well as short aqueductal
stenosis, were observed in 21 patients. In two patients with
intraventricular hemorrhage, the opening of the upper aqueduct was
occluded by old blood clots. Approximately one week after surgery,
smooth CSF flow was observed by phase-contrast cine MRI at the
aqueduct opening. In the postoperative MRI scans of the CSF flow,
the flow-void signal phenomenon was observed in 14 patients
(Fig. 4). The average peak flow
velocity was 4.74±1.77 cm/sec. The typical flow velocity waveform
for each cardiac cycle was a two-way flow (Fig. 2). In 21 patients, the simple
membranous obstruction did not recur during follow-up. The
ventricular size was reduced in eight patients, whereas no changes
were observed in the other patients. The one-year follow-up MRI
scans revealed that the CSF flow was smooth in all patients. The
average peak flow velocity was 4.28±2.17 cm/sec. The flow velocity
waveform for each cardiac cycle was bi-directional.
Symptoms recurred during follow-up in the two
patients with hydrocephalus due to intraventricular hemorrhage. One
patient had symptoms of intracranial hypertension one month after
aqueductoplasty. The MRI scans revealed that there was no CSF flow
in the aqueduct and a second endoscopic examination revealed that
the aqueduct opening was covered by old blood clots and a
proliferative ventricular membrane. After the obstruction was
relieved, the aqueduct was observed to be recanalized on repeated
phase-contrast cine MRI. In the second patient, the symptoms of
intracranial hypertension recurred three months after
aqueductoplasty. There was no CSF flow in the aqueduct, as revealed
by the phase-contrast cine MRI. A second endoscopy examination
confirmed restenosis in the aqueduct. The aqueduct was expanded and
then a stent was placed. The patient was free of symptoms following
stenting.
Of the 23 patients, only one patient reported
oculomotor nerve palsy. This patient recovered after three
months.
The average peak flow velocity one week after
surgery was similar for patients aged <2 years (4.96±1.83
cm/sec) and those who were older than 2 years (4.53±1.75 cm/sec)
(P>0.05). The average peak flow velocity, as measured at one
year after surgery, remained similar in patients aged <2 years
(4.60±2.26 cm/sec) and those older than 2 years (3.97±2.13 cm/sec;
P>0.05).
Discussion
In 1920, Dandy (15) used a probe to perform aqueduct
reconstruction through the fourth ventricle for the first time.
With the development of endoscopic equipment and technology, third
ventriculostomy has been widely used to treat patients with
hydrocephalus due to aqueduct stenosis. The procedure is relatively
safe and has fewer complications than other methods. In the
majority of cases, this procedure helps to wean patients off shunt
devices. However, certain fatal complications, including injuries
to the basilar artery, have been reported for third ventriculostomy
(17). In addition, a thick or
tough bottom in the third ventricle makes ventriculostomy difficult
to perform. Moreover, stenosis at the bottom of the third ventricle
may damage the hypothalamus or pituitary stalk. Therefore, EA is
used as an alternative option for treating patients with membranous
obstruction. When the preoperative MRI sagittal view reveals that
the third ventricle floor is flat or when the coronal MRI view
reveals that the third ventricular is narrow, the floor of the
third ventricle may be difficult to penetrate during surgery
(Fig. 1). However, judgments that
are based on the findings of MRI imaging are not always reliable.
The preoperative MRI revealed that 21 patients had a membranous
obstruction of the proximal aqueduct outlet (Fig. 1). The thickness of the membrane was
<1 mm, as measured by MRI. Two patients had a short obstruction
that was <3 mm. According to the results of the preoperative
mid-sagittal MRI, 21 cases had occlusions in the proximal inlet of
the aqueduct, in which the occluding membrane was <1 mm
(Fig. 1). Two cases had short
segmental stenosis of ∼3 mm.
Phase-contrast cine MRI provides important
information concerning the hemodynamics of the CSF circulation. The
earliest MRI examinations only provide a qualitative description of
CSF flow in the stenotic aqueduct or ventricles through the CSF
flow-void signs. Magnetic resonance T1- or T2-weighted images
improve a visualization of the anatomical structure prior to
surgery. In our study, phase-contrast MRI was used to screen
patients prior to surgery. Our results indicated that the diagnosis
of aqueduct obstruction was consistent with the intra-operative
exploration in all cases.
No specific standards exist for the evaluation of EA
efficacy. To date, the only standard that is recognised by the
majority of researchers is shunt independence. Moreover, short-term
follow-up does not identify delayed surgical failure (8). In certain patients, particularly in
pediatric patients with chronic obstructive hydrocephalus, the
clinical symptoms are not evident within a short period of time. By
contrast, long-term observation may delay the best time for
treatment. The findings from MRI are necessary to investigate
whether the aqueduct is successfully opened following surgery
(6,13,18).
In the majority of cases, a sufficient CSF flow is observed as a
flow-void signal in individual cases with relieved symptoms.
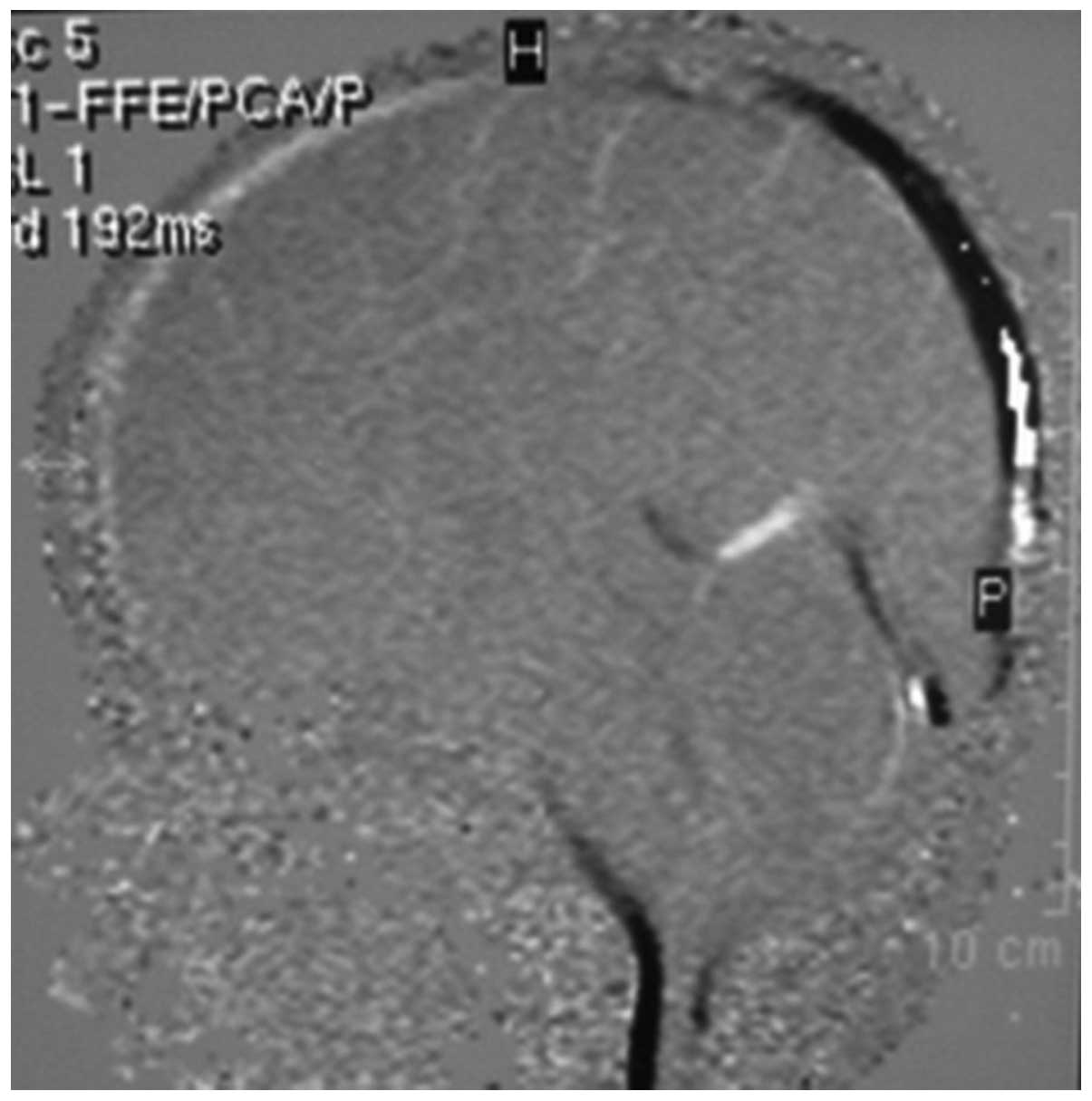
However, from the sagittal T1- and T2-weighted images, the CSF
flow-void signs within the aqueduct and the fourth ventricle are
not observed. The CSF flow waveform shows the respective flow
pattern, which indicates that the aqueduct is open (Fig. 5). In the majority of cases in this
study, the flow-void signals of CSF were detected following
surgery. In a few cases with clinical improvement following
surgery, the flow void was not detected; however, the CSF cine
images revealed that the aqueduct was opened following surgery.
The imaging evaluation criteria generally include
the reduction of the ventricle size and subarachnoid space, the
absorption of periventricular edema and the CSF flow-void signal
phenomenon. However, 50% of patients with improved symptoms have
little or no significant changes in ventricle size following
surgical treatment. The absorption of periventricular edema remains
controversial (9). The
subarachnoid width may only be used as a secondary indicator. In
addition, the CSF flow-void signal phenomenon is not observed in a
number of patients. Previous reports indicated that ventricle size
did not change in 11–38% of patients who received third
ventriculostomy (13,14).
Schroeder et al(6) assessed the CSF circulation by
phase-contrast MRI in 14 healthy volunteers and eight patients who
underwent EA. No significant differences in the CSF time index,
peak velocity, average flow velocity or volume between the two
groups were observed, which suggested that the CSF circulation was
normal following aqueductoplasty.
EA is an important alternative treatment for
obstructive hydrocephalus when third ventriculostomy is difficult
to perform. However, the success rate varies in different reports
due to the small sample sizes and the short follow-up times. The
intraoperative implantation of a stent remains controversial. Thus,
the evaluation of postoperative efficacy becomes particularly
important. In addition to symptom relief, imaging results are
essential for the evaluation of postoperative efficacy.
Phase-contrast MRI has been used to study CSF circulation for
>20 years. This technique is widely used for the clinical
diagnosis of hydrocephalus. Kim et al(19) recommended phase-contrast MRI as a
significant method for the evaluation of the position and severity
of obstruction in patients with obstructive hydrocephalus. In the
current study, the results of post-aqueductoplasty phase-contrast
MRI indicated that the aqueduct was unobstructed in 23 patients.
During follow-up, the reduction in ventricle size was observed in
eight patients and the CSF flow-void signal phenomenon was observed
in four patients. In two patients with recurrence of intracranial
hypertension, phase-contrast MRI did not show any CSF flow inside
the aqueduct. The second endoscopic exploration revealed that the
aqueduct was closed. The test results were consistent with the
clinical findings.
Enchev et al(20) proposed that EA carries potential
risks that should not be underestimated. The authors demonstrated
that direct surgery-related complications, including damage to the
fornix, aqueductal roof or floor of the third ventricle,
venous-arterial bleeding and particularly injury to the eloquent
periaqueductal grey structures may occur; these complications
should be carefully considered prior to surgery. In 21 patients,
the obstructive hydrocephalus was caused by the membrane that
occluded the proximal inlet of the aqueduct. The fiber-scope should
be set at a right angle to the inlet of the aqueduct. Fenestration
of the septum was carefully performed using the balloon technique.
Opening a thin membrane is a relatively easy and safe
neuroendoscopic procedure (Fig.
6). Compared with a membranous septum, short segmental stenosis
is more difficult to conduct surgery on. The potential risk of
injury to the midbrain is associated with the length of the
stenosis (10).
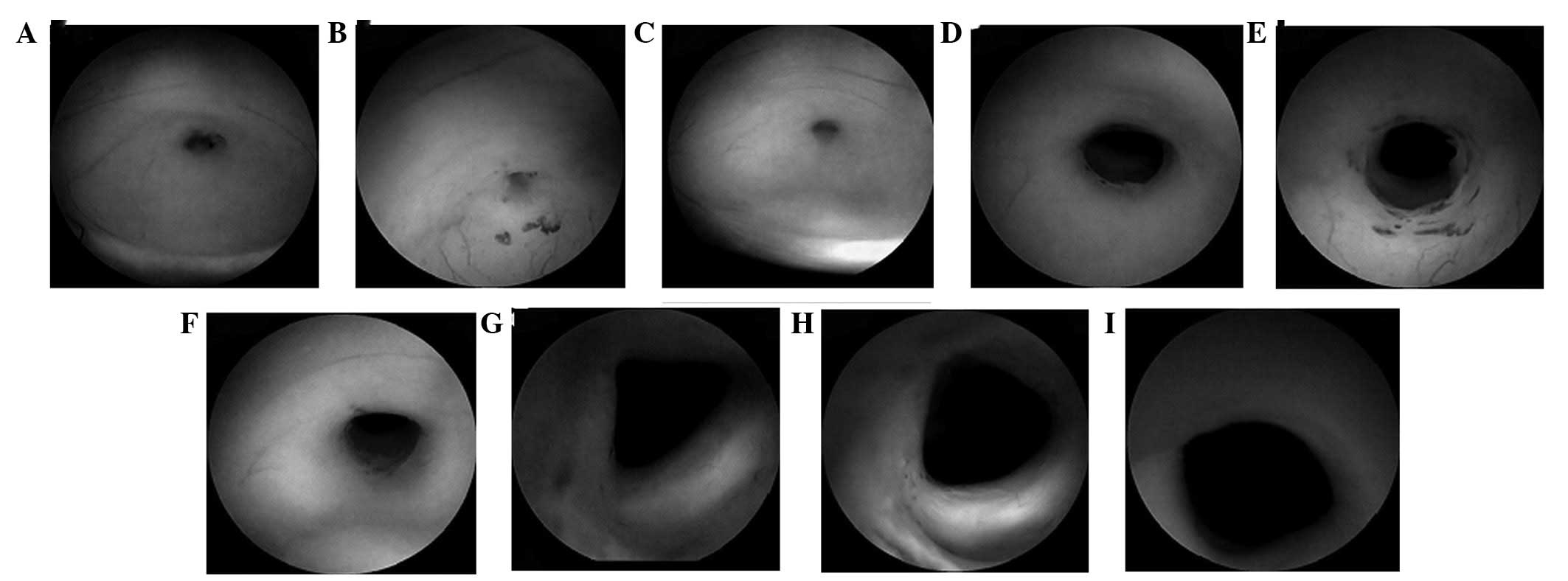 | Figure 6(A,B,C) Membrane occluding the
proximal inlet of the aqueduct; the membranous obstruction is
translucent. (D,E,F) The stoma to the fourth ventricle following
neuroendoscopic aqueductoplasty (EAP). (G,H,I) Intracanalicular
structures with no injury. (A,D,G) were from one patient, (B,E,H)
were from another patient and (C,F,I) were from another
patient. |
ETV has become the first line treatment option for
obstructive hydrocephalus; however, aqueductoplasty may be used
when surgery using ETV would be difficult. In certain cases, EA
should be considered as an alternative treatment option in patients
with short or membranous stenosis of the rostral aqueduct. The
potential risk of injury to the midbrain and periaqueductal grey
matter is low. Phase-contrast cine MRI may be a valuable tool in
the evaluation of a hydrocephalic ventricle system.
References
|
1.
|
Jenkinson MD, Hayhurst C, Al-Jumaily M,
Kandasamy J, Clark S and Mallucci CL: The role of endoscopic third
ventriculostomy in adult patients with hydrocephalus. J Neurosurg.
110:861–866. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Kulkarni AV, Drake JM, Mallucci CL, et al:
Endoscopic third ventriculostomy in the treatment of childhood
hydrocephalus. J Pediatr. 155:254–259. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Ogiwara H, Dipatri AJ Jr, Alden TD, Bowman
RM and Tomita T: Endoscopic third ventriculostomy for obstructive
hydrocephalus in children younger than 6 months of age. Childs Nerv
Syst. 26:343–347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Sacko O, Boetto S, Lauwers-Cances V, Dupuy
M and Roux FE: Endoscopic third ventriculostomy: outcome analysis
in 368 procedures. J Neurosurg Pediatr. 5:68–74. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Ersahin Y: Endoscopic aqueductoplasty.
Childs Nerv Syst. 23:143–150. 2007. View Article : Google Scholar
|
|
6.
|
Schroeder HW, Schweim C, Schweim KH and
Gaab MR: Analysis of aqueductal cerebrospinal fluid flow after
endoscopic aqueductoplasty by using cine phase-contrast magnetic
resonance imaging. J Neurosurg. 93:237–244. 2000. View Article : Google Scholar
|
|
7.
|
da Silva LR, Cavalheiro S and Zymberg ST:
Endoscopic aqueductoplasty in the treatment of aqueductal stenosis.
Childs Nerv Syst. 23:1263–1268. 2007.
|
|
8.
|
Fritsch MJ, Kienke S and Mehdorn HM:
Endoscopic aqueductoplasty: stent or not to stent? Childs Nerv
Syst. 20:137–142. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Garg AK, Suri A, Sharma BS, Shamim SA and
Bal CS: Changes in cerebral perfusion hormone profile and
cerebrospinal fluid flow across the third ventriculostomy after
endoscopic third ventriculostomy in patients with aqueductal
stenosis: a prospective study. Clinical article. J Neurosurg
Pediatr. 3:29–36. 2009. View Article : Google Scholar
|
|
10.
|
Miki T, Nakajima N, Wada J and Haraoka J:
Indications for neuroendoscopic aqueductoplasty without stenting
for obstructive hydrocephalus due to aqueductal stenosis. Minim
Invasive Neurosurg. 48:136–141. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Oertel JM, Baldauf J, Schroeder HW and
Gaab MR: Endoscopic options in children: experience with 134
procedures. J Neurosurg Pediatr. 3:81–89. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Alperin N, Vikingstad EM, Gomez-Anson B
and Levin DN: Hemodynamically independent analysis of cerebrospinal
fluid and brain motion observed with dynamic phase contrast MRI.
Magn Reson Med. 35:741–754. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Bargalló N, Olondo L, Garcia AI, Capurro
S, Caral L and Rumia J: Functional analysis of third
ventriculostomy patency by quantification of CSF stroke volume by
using cine phase-contrast MR imaging. AJNR Am J Neuroradiol.
26:2514–2521. 2005.PubMed/NCBI
|
|
14.
|
Stivaros SM, Sinclair D, Bromiley PA, Kim
J, Thorne J and Jackson A: Endoscopic third ventriculostomy:
predicting outcome with phase-contrast MR imaging. Radiology.
252:825–832. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Dandy WE: The diagnosis and treatment of
hydrocephalus resulting from strictures of the aqueduct of Sylvius.
Surg Gynecol Obstet. 31:340–358. 1920.
|
|
16.
|
Schroeder HW and Gaab MR: Endoscopic
aqueductoplasty: technique and results. Neurosurgery. 45:508–518.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Lipina R, Reguli S, Dolezilová V,
Kuncíková M and Podesvová H: Endoscopic third ventriculostomy for
obstructive hydrocephalus in children younger than 6 months of age:
is it a first-choice method? Childs Nerv Syst. 24:1021–1027. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Schroeder HW, Oertel J and Gaab MR:
Endoscopic treatment of cerebrospinal fluid pathway obstructions.
Neurosurgery. 60(Suppl 1): S44–S52. 2007. View Article : Google Scholar
|
|
19.
|
Kim MH, Shin KM and Song JH: Cine MR CSF
flow study in hydrocephalus: what are the valuable parameters? Acta
Neurochir Suppl. 71:343–346. 1998.PubMed/NCBI
|
|
20.
|
Enchev Y and Oi S: Historical trends of
neuroendoscopic surgical techniques in the treatment of
hydrocephalus. Neurosurg Rev. 31:249–262. 2008. View Article : Google Scholar : PubMed/NCBI
|