Introduction
Diabetic cardiomyopathy (DCM) is a unique
cardiovascular disease, which is characterized by myocardial
relaxation and contractional dysfunction, as a result of oxidative
stress, inflammation, cardiac fibrosis and myocardial apoptosis
(1). During previous decades,
there has been a particular focus on the role of apoptosis, i.e.,
the programmed cell death that is controlled by intrinsic genetic
mechanisms in certain physiological or pathological conditions, in
the pathogenesis of DCM.
Erythropoietin (EPO) is a glycoprotein hormone
secreted by the kidney in the adult, and by the liver in the fetus,
that stimulates the production of red blood cells by stem cells in
the bone marrow (erythropoiesis). Synthetic products of EPO, such
as recombinant human EPO (rhEPO), have been successfully applied in
clinical practice to treat anemia induced by diabetic nephropathy
(2). In addition, rhEPO has a
variety of cellular protective effects, predominantly due to its
binding to a heterodimer formed by the subunits of the EPO receptor
(EPOR) and the β common receptor (βcR, also known as CD131). CD131
expression has been exhibited in the brain, heart, liver and kidney
(3). When EPO binds to the
EPOR-CD131 heterodimer, it activates various signaling pathways
involved in cell survival, metabolism and apoptosis (3,4).
However, the long-term, high-dose application of rhEPO is likely to
cause a variety of adverse effects, including hypertension and
thrombogenesis, due to its effect on the blood hematocrit (5).
Carbamylated EPO (CEPO), a carbamoyl derivative of
EPO, has similar pharmacokinetic characteristics to EPO (6,7).
Moreover, it has been demonstrated that whilst CEPO does not
stimulate the production of red blood cells, it does bind to the
EPOR-CD131 heterodimer to exert cellular protective effects similar
to those of EPO (8–11). CEPO may limit mitochondrial
permeability transition pore opening and prevent the release of
mitochondrial contents, such as reactive oxygen species and
cytochrome c, thereby reducing apoptosis (5).
In addition, CEPO affects cellular signal
transduction, via the extracellular signal-regulated kinase
(ERK)-1/2 (12) and Akt (13) pathways. However, to date, it has
been unclear whether CEPO has a protective effect against
myocardial apoptosis in rats with DCM. In this study, we
investigated the effects of CEPO treatment on the myocardial
apoptosis and phosphatidylinositol-3-kinase (PI3K)/Akt gene
expression in the hearts of high-fat, high-carbohydrate diet-fed
rats with streptozotocin (STZ)-induced DCM.
Materials and methods
Reagents
The rhEPO (cat. no. E10–053) was obtained from Kai
Mao Biomedical Co., Ltd. (Shanghai, China), and STZ (cat. no.
S0130), diethyl pyrocarbonate (DEPC), sodium borate and potassium
cyanate were purchased from Sigma-Aldrich (St. Louis, MO, USA). The
terminal deoxynucleotidyl transferase-mediated dUTP nick end
labeling (TUNEL) kit (In Situ Cell Death Detection kit, POD)
was obtained from Roche Diagnostics, Basel, Switzerland. The
caspase-3 (cat. no. 9662), Bcl-xL (54H6; cat. no. 2764), p-PI3K
(p85; cat. no. 4292) and p-Akt [serine/threonine (Ser/Thr); cat.
no. 9611s] antibodies were purchased from Cell Signaling
Technology, Inc. (Danvers, MA, USA). The PI3K (p85α) and Akt1 mRNA
in situ hybridization kits were obtained from Tianjin
Haoyang Biological Manufacture Co., Ltd. (Tianjin, China). All the
reagents were of analytical pure grade.
CEPO synthesis
CEPO was synthesized as previously described by
Leist et al (7). In brief,
potassium cyanate was added to a mixture of 500 μl rhEPO (1
mg/ml) and 500 μl 1M sodium borate, to produce a solution
with a final concentration of 1 mol/l. This was mixed and incubated
at 37°C for 24 h to form the reaction solution. Excess potassium
cyanate was removed from the reaction solution by dialysis, and the
solution was then further concentrated by ultrafiltration (membrane
cut-off, 10 kDa). The protein concentration was measured by
Coomassie Brilliant Blue staining, and the absorbance was read at
335 nm.
Animals
Establishment of the DCM rat
model
Healthy male Wistar rats (n=120, including 20 as
controls and 100 for the DCM model; weight, 220±20 g), and the
high-fat, high-carbohydrate diet (comprising 66.6% basic rat chow,
20% sucrose, 10% lard, 3% egg yolk and 0.4% cholesterol) were
obtained from the Experimental Animal Center of Jilin University
(Changchun, China). The study was approved by the ethics committee
of The First Bethune Hospital of Jilin University. In order to
establish the diabetic model, 100 rats were fed a high-fat,
high-carbohydrate diet for four weeks, and were then injected with
STZ (50 mg/kg, intraperitoneally). A second injection of the same
dose of STZ was administered a week later. Seventy-five rats were
identified to have diabetes mellitus, according to the criterion of
a fasting blood glucose concentration >18 mmol/l, and were used
in the following experiments. The control group was fed with a
normal diet.
Animal grouping
The experiment was divided into two studies, in
order to evaluate the dose- and time-dependent responses to CEPO
administration. In study one, which analyzed the dose-response
relationship, the rats were assigned to the following groups:
Control (group A, healthy rats, n=10); DCM (group B, n=9); CEPO
(500 IU/kg; group C, n=9); CEPO (1,000 IU/kg; group D, n=9), CEPO
(2,000 IU/kg; group E, n=9) and rhEPO (1,000 IU/kg; group F, n=10),
where groups B-F comprised rats with DCM. The CEPO or rhEPO was
dissolved in 0.3 ml physiological saline, and then subcutaneously
injected twice a week for four weeks. The final numbers of
surviving rats in each group were 10, 6, 7, 7, 8 and 7,
respectively. Study two, a time-response relationship analysis,
included a short-term (four-week) intervention panel, which
comprised groups A, B, D and F, as above, and a long-term
(eight-week) intervention panel, which comprised the following
groups: Control (group A′, healthy rats, n=10); DCM (group B′,
n=9); CEPO (1,000 IU/kg; group D′, n=9) and rhEPO (1,000 IU/kg;
group F′, n=10). The final numbers of surviving rats in each group
of the long-term intervention were 10, 6, 8 and 7,
respectively.
Assays for blood samples or heart
tissues
Routine blood examination
Rats from each group were fasted for 8 h and
anesthetized with 10% chloral hydrate (0.30 g/kg), following the
intervention protocol. Blood samples were collected with red-top
normal serum and purple EDTA anticoagulation vacutainer tubes from
the right ventricles of six randomly selected rats from each group,
and were then sent for routine hematological examination at the
clinical laboratory of The First Bethune Hospital of Jilin
University (Changchun, China), using a leukocyte five-part
differential hematology analyzer.
Myocardial cell transmission electron
microscopy (TEM)
Eight weeks following the commencement of the
experiment, the rat hearts from each group were perfused with 37°C
0.9% NaCl, along with a 4°C paraformaldehyde and 4% glutaraldehyde
mixture. The heart apices (∼2 mm) were processed successively with
2.5% glutaraldehyde and 1% osmic acid fixations, ethanol series
dehydration and Epon 812 epoxy resin embedding, and were then
sectioned with an LKB 8800 Ultratome III (Bromma, Sweden). Uranyl
acetate and lead citrate double staining, and a JEM-1200EX
transmission electron microscope were used to observe the sections,
and photographic images were captured.
TUNEL investigation of myocardial cell
apoptosis in the rats
Eight weeks following the commencement of the
experiment, the rat hearts from each group were perfused and fixed
with 10% neutral buffered formalin, and then paraffin-embedded.
Sections measuring 4 μm were used for the detection of
myocardial cell apoptosis with the TUNEL kit (Roche Diagnostics),
in accordance with the manufacturer’s instructions. Apoptosis was
quantified using Image-Pro Plus 6.0 image analysis software (Media
Cybernetics, Rockville, MD, USA), in order to facilitate
quantitative analysis.
Immunohistochemistry
The paraffin-embedded heart sections were examined
for caspase-3 (1:200) and Bcl-xl (1:300) protein expression, using
a streptavidin-peroxidase (SP) assay. Cells were defined as
positive if the cytoplasm was stained brown. The integrated optical
density (IOD) of the positively-stained tissue was calculated using
Image-Pro Plus 6.0 software (Media Cybernetics).
In situ hybridization for
determination of PI3K/Akt mRNA expression
The PI3K and Akt mRNA expression was determined by
in situ hybridization assay, in accordance with the
manufacturer’s instructions. The probe sequences used for the PI3K
(p85α) mRNA were as follows: i) 5′-GTCTC CCCTC TCCCC AGTAG TTTCA
TTG; ii) 5′-ATAAG GAGAG GCGGG GCAAC ATCAG GAG and iii) 5′-GTAAG
TCGGC GAGAT AGCGT TTGAA AGC. The probe sequences used for the Akt1
mRNA were as follows: i) 5′-CCCTC CTTCA CAATG GCTAC GTCGT TCA; ii)
5′-GCTTC AGGTA CTCAA ACTCG TTCAT GGT and iii) 5′-TCTCA GTAAG CGTGT
GGGCA ACCTC ATC. Cells were defined as positive if the cytoplasm
was stained brown. The positive staining was quantified using the
IOD, which was calculated by Image-Pro Plus 6.0 software (Media
Cybernetics).
Western blot analysis of PI3K/Akt
phosphorylated protein expression
A small quantity of myocardial tissue was cut into
fragments, and then homogenized with radioimmunoprecipitation assay
(RIPA) buffer (1mM phenylmethanesulfonyl fluoride) for protein
extraction. Following the centrifugation of the lysates (13,750 × g
for 15 min at 4°C), the supernatants were quantified using a
bicinchoninic acid protein assay. The protein concentration in the
loading samples was adjusted to 80 μg/20 μl, and then
the protein samples were separated by 10% sodium dodecyl
sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) gel, and
transferred to a polyvinylidene fluoride (PVDF) solid-phase
membrane. The p-PI3K (p85) (1:1,000), p-Akt (Ser/Thr) (1:1,000) and
β-actin (1:1,000) antibodies were incubated with the PVDF membranes
for 90 min, and then the membranes were conjugated with a second
anti-immunoglobulin (Ig)-G antibody (1:2,000) for 90 min. The
immunoblotted proteins were subsequently detected using enhanced
chemiluminescence.
Statistical analysis
All data are expressed as the mean ± standard
deviation (SD). Statistical analysis was performed using SPSS
software, version 13.0 (SPSS, Inc., Chicago, IL, USA). The
difference between the means of two groups was assessed using the
Student’s t-test, while multiple means were compared using one-way
analysis of variance. P<0.05 was considered to indicate a
statistically significant difference.
Results
Routine hematological examination
Compared with the control and DCM groups, CEPO had
no effect on the red blood cell count, hematocrit or hemoglobin
levels (Table I). However,
following four weeks of treatment, rhEPO significantly increased
the number of red blood cells and the hemoglobin level in the rats
with DCM (P<0.05 for each), compared with their values in the
control group, in addition to inducing a significantly higher
hematocrit than that induced by CEPO (P<0.05). Eight weeks of
treatment with rhEPO resulted in a higher hematocrit than four
weeks of treatment (P<0.05).
 | Table I.Effects of CEPO on the erythrocyte
and hemoglobin levels in rats with DCM. |
Table I.
Effects of CEPO on the erythrocyte
and hemoglobin levels in rats with DCM.
| Treatment duration
(weeks) | No. | Group
|
|---|
| A | B | D | F |
|---|
| RBC
(1012/l) | 4 | 6 | 6.97±0.66 | 8.19±0.59 | 8.77±0.37 | 9.96±0.28a |
| 8 | 6 | 7.05±0.64 | 8.30±0.13 | 8.02±0.35 |
10.44±0.30a–c |
| HGB (g/l) | 4 | 6 | 142.5±26.60 | 150.5±12.02 | 153.0±12.73 | 187.5±4.95a |
| 8 | 6 | 144.5±14.85 | 154.0±1.41 | 149.5±10.61 |
195.5±7.78a–c |
| HCT (fl) | 4 | 6 | 0.51±0.03 | 0.46±0.04 | 0.44±0.03 | 0.55±0.01c |
| 8 | 6 | 0.51±0.07 | 0.49±0.02 | 0.46±0.04 |
0.63±0.01b–d |
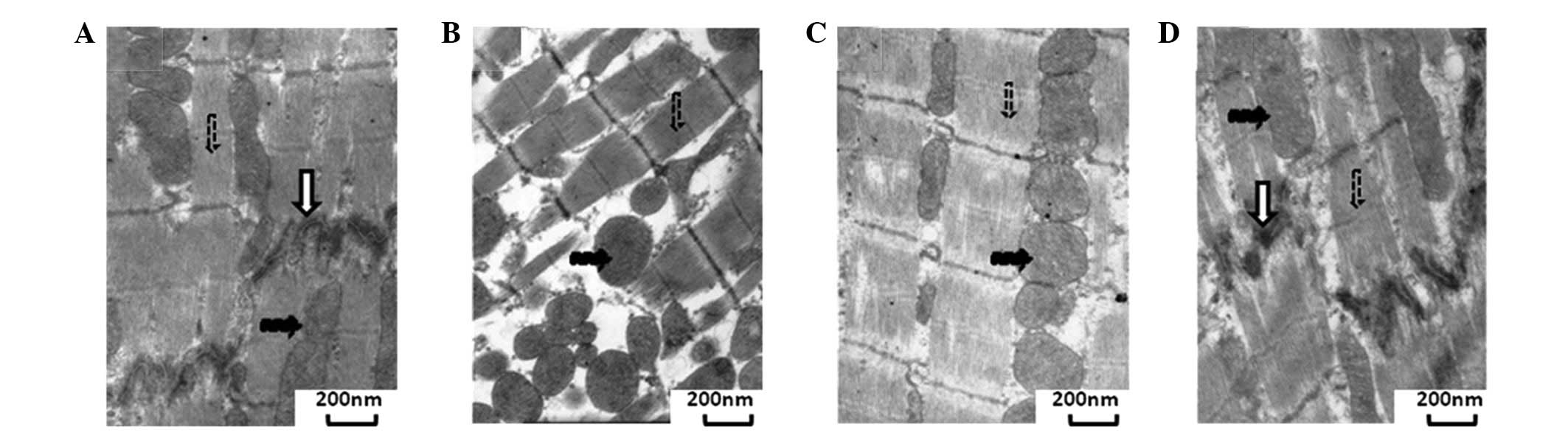
TEM of heart tissues
TEM analysis of the myocardial cells demonstrated
that in the control group, the I and A bands were clear, with
visible transverse tubules on the level of the Z line. The
mitochondria were oval in shape, and the ridge was closely spaced
with the intact membrane. The gap junctions were visible and dense.
In the DCM group, there was a reduction in the fibrin bundles in
the cytosol, and a number of bundles had dissolved in the
sarcomere, leading to matrix cavitation. The intercalated discs
were moderately separated, and the gap junctions were reduced.
There was an increase in the number of mitochondria, and several
mitochondria were small, circular and pyknotic in appearance. In
the CEPO group, the level of fibrin was reduced, and dissolution
had occurred in small sections of the sarcomeres, although in
general the I and A bands were clear. There was an increase in the
number of mitochondria, a small number of which were small and
circular in shape. In certain instances, the individual M lines and
H bands were not clear, due to a mild swelling. In the rhEPO group,
there was limited rupturing or dissolving of the fibrin in the
sarcomere, the intercalated disc cross connections were clear, and
there was only a lack of clarity in certain local structures of
individual connections (Fig.
1).
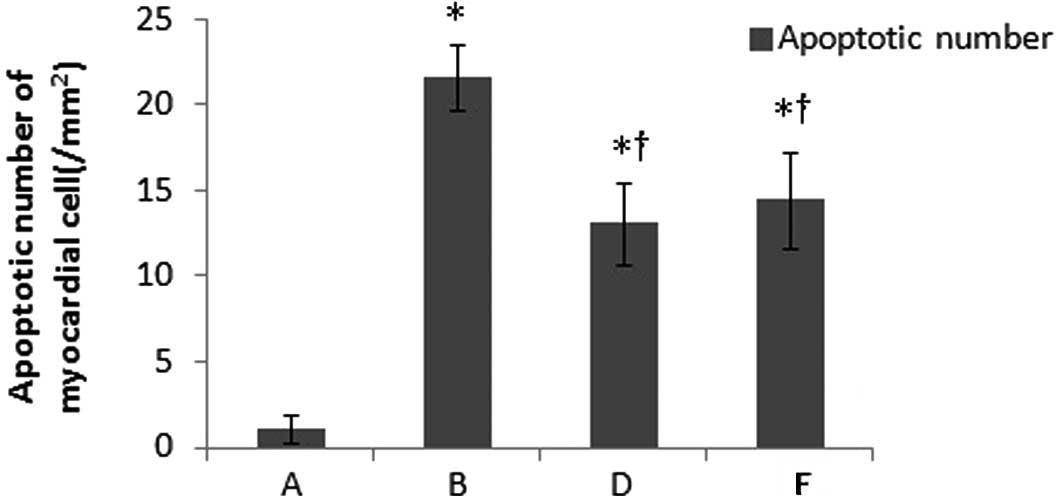
Detection of myocardial cell apoptosis
in rats with DCM
The results of the TUNEL assay demonstrated that the
nuclei of the apoptotic cells were brown, whereas those of the
normal cells were blue. There were a few, scattered apoptotic
nuclei in the control group, whereas numerous apoptotic cells were
observed in the DCM group. The number of apoptotic myocardial cells
in the DCM group was identified to be 21.557±1.915/mm2,
which was significantly higher than the number in the control group
(P<0.05). In the CEPO group, the number of apoptotic myocardial
cells was 13.083±2.371/mm2, which indicated a smaller
increase than that in the DCM group (P<0.05), although the
result remained higher than that in the control group (P<0.05).
The rhEPO group demonstrated a similar result to that of the CEPO
group, with the number of apoptotic myocardial cells observed to be
14.476±2.804/mm2 (Fig.
2).
Immunohistochemistry for caspase-3 and
Bcl-xl
The caspase-3 protein expression level in the rats
with DCM was significantly increased to ∼4-fold that of the control
group, whereas the Bcl-xl protein expression was significantly
reduced in the four- and eight-week treatment groups. In comparison
with the DCM group, the CEPO and rhEPO treatments significantly
ameliorated the increase in caspase-3 and the reduction in Bcl-xl
protein levels, exhibiting a dose-dependent relationship
(P<0.05). Treatment with 1,000 IU/kg CEPO demonstrated a similar
effect to the same dose of rhEPO on the amelioration of the
caspase-3 and Bcl-xl protein expression in the diabetic hearts
(P>0.05). Of note, the eight-week CEPO and rhEPO treatments
demonstrated an enhanced effect on the suppression of caspase-3
protein expression, compared with the four-week treatments;
however, no difference was observed in Bcl-xl protein expression
between the four- and eight-week treatments (Fig. 3).
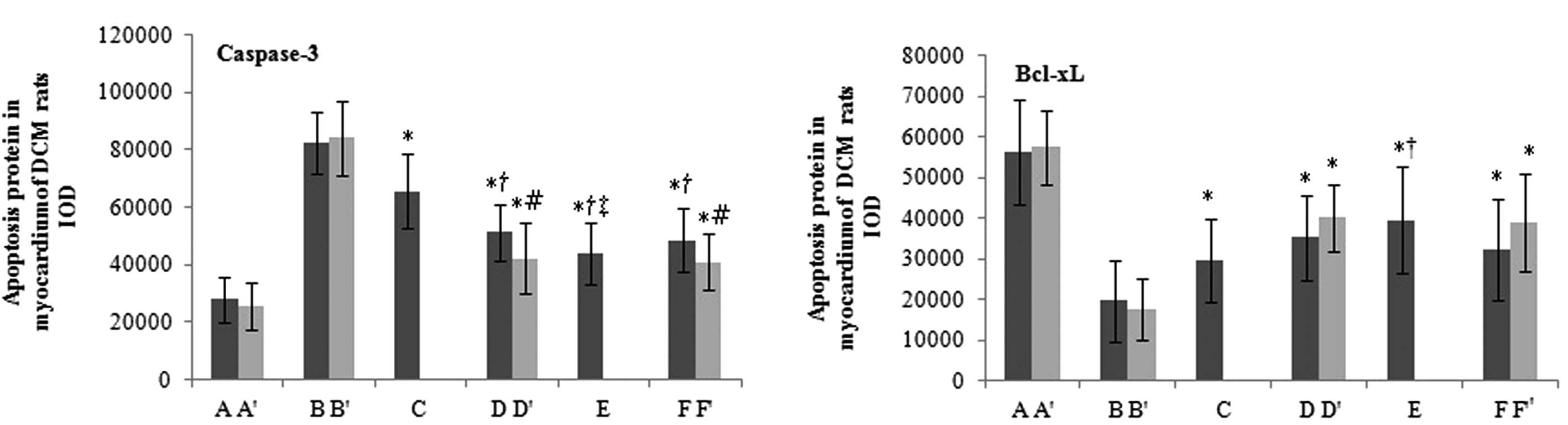 | Figure 3.Effects of carbamylated erythropoietin
(CEPO) on caspase-3 and Bcl-xl protein expression in the myocardial
immunohistochemical examination of rats with diabetic
cardiomyopathy (DCM). Rats were assigned to the following groups
for a four-week treatment intervention (black bars): A, control; B,
DCM; C, CEPO (500 IU/kg); D CEPO (1,000 IU/kg); E, CEPO (2,000
IU/kg); and F, recombinant human (rh)-EPO (1,000 IU/kg). For the
eight-week treatment intervention (grey bars), the groups were as
follows: A′, control; B′, DCM; D′, CEPO (1,000 IU/kg); and F′,
rhEPO (1,000 IU/kg). Groups A and A′ comprised healthy rats,
whereas groups B-F and B′-F′ comprised rats with DCM.
*P<0.05 vs. DCM, †P<0.05 vs. CEPO (500
IU/kg), ‡P<0.05 vs. CEPO (1,000 IU/kg),
§P<0.05 vs. CEPO (2,000 IU/kg) groups and
#P<0.05 vs. the four-week treatment course group.
IOD, integrated optical density. |
In situ hybridization for
determination of PI3K/Akt mRNA expression
Compared with the control group, the levels of
myocardial cell PI3K (p85α) and Akt1 mRNA expression were increased
in the DCM group (P<0.05). CEPO treatment further increased the
levels of PI3K (p85α) and Akt1 mRNA expression in the heart tissues
of the diabetic rats (P<0.05 for each), and the increase was
dose-dependent (P<0.05). No significant differences were
observed in the levels of PI3K (p85α) and Akt1 mRNA expression
between the CEPO and rhEPO groups that received the same dosage
(P>0.05). There was a higher elevation in the levels of PI3K
(p85α) and Akt1 mRNA expression in the hearts of the rats with DCM
following eight weeks of treatment, as opposed to four-weeks, but
the difference was not significant (Fig. 4).
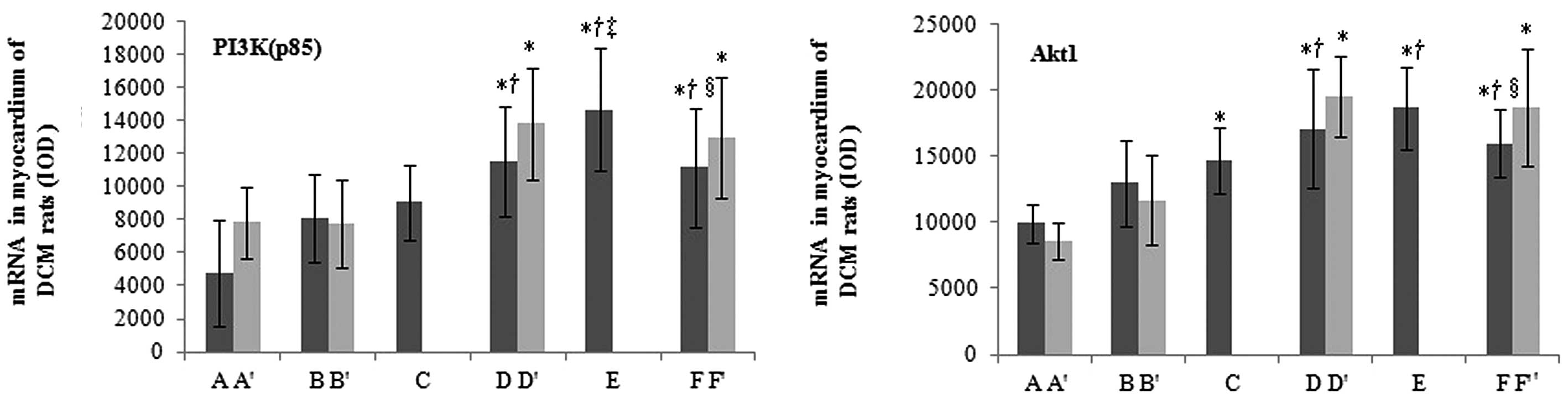 | Figure 4.Effects of carbamylated erythropoietin
(CEPO) on phosphatidylinositol-3-kinase (PI3K)/Akt mRNA expression
(examined by in situ hybridization) in the myocardial
tissues of rats with diabetic cardiomyopathy (DCM). Rats were
assigned to the following groups for a four-week treatment
intervention (black bars): A, control; B, DCM; C, CEPO (500 IU/kg);
D CEPO (1,000 IU/kg); E, CEPO (2,000 IU/kg); and F, recombinant
human (rh)-EPO (1,000 IU/kg). For the eight-week treatment
intervention (grey bars), the groups were as follows: A′, control;
B′, DCM; D′, CEPO (1,000 IU/kg); and F′, rhEPO (1,000 IU/kg).
*P<0.05 vs. DCM, †P<0.05 vs. CEPO (500
IU/kg), ‡P<0.05 vs. CEPO (1,000 IU/kg) and
§P<0.05 vs. CEPO (2,000 IU/kg) groups. IOD,
integrated optical density. |
Western blot analysis of PI3K/Akt
phosphorylated protein expression
Similar to the mRNA expression, the p-PI3K (85) and
p-Akt (Ser/Thr) protein expression levels in the myocardial cells
of the rats with DCM were significantly increased, compared with
those of the normal control rats (P<0.05). In comparison with
the rats with DCM, CEPO treatment further increased the p-PI3K
(p85) and p-Akt (Ser/Thr) protein expression levels in the
myocardial cells, in a dose-dependent manner (P<0.05). There
were no significant differences in the PI3K (p85) and p-Akt
(Ser/Thr) protein expression levels between the same-dose CEPO and
rhEPO groups (P>0.05). No significant difference was observed
between the four- and eight-week treatment regimens (Fig. 5).
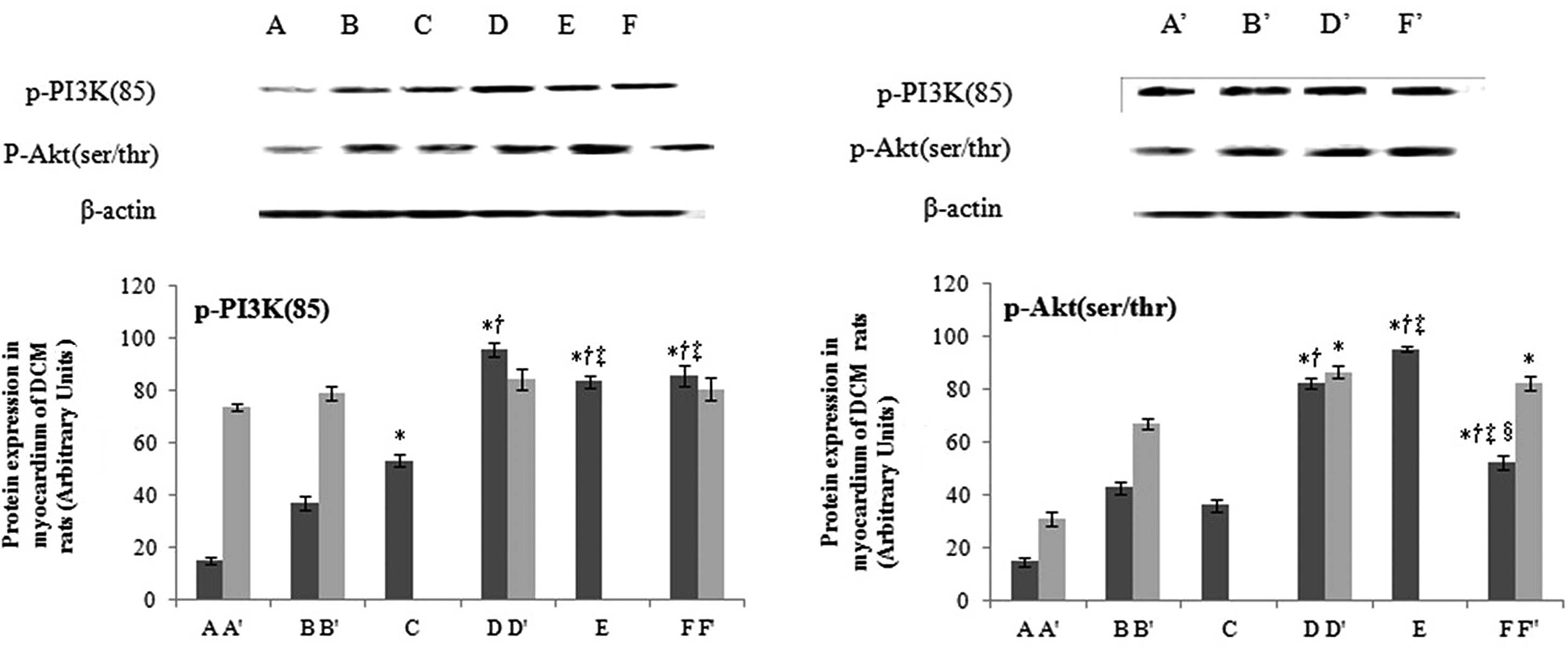 | Figure 5.Effects of carbamylated erythropoietin
(CEPO) on phosphatidylinositol-3-kinase (PI3K)/Akt protein
expression (examined by western blot analysis) in the myocardial
tissues of rats with diabetic cardiomyopathy (DCM). Rats were
assigned to the following groups for a four-week treatment
intervention (black bars): A, control; B, DCM; C, CEPO (500 IU/kg);
D CEPO (1,000 IU/kg); E, CEPO (2,000 IU/kg); and F, recombinant
human (rh)-EPO (1,000 IU/kg). For the eight-week treatment
intervention (grey bars), the groups were as follows: A′, control;
B′, DCM; D′, CEPO (1,000 IU/kg); and F′, rhEPO (1,000 IU/kg).
*P<0.05 vs. DCM, †P<0.05 vs. CEPO (500
IU/kg), ‡P<0.05 vs. CEPO (1,000 IU/kg) and
§P<0.05 vs. CEPO (2,000 IU/kg) groups. |
Discussion
In this study we revealed that CEPO, a carbamoyl
derivative of EPO that does not affect erythropoiesis, attenuated
myocardial pathological damage, at least in part through the
activation of the PI3K/Akt signaling pathway, which regulates
myocardial cell apoptosis in diabetes mellitus.
It has previously been demonstrated that CEPO exerts
a protective effect against apoptosis in central and peripheral
nervous system (8,14,15),
cardiovascular (16–18) and urinary system diseases (11,19,20),
as well as in diabetic peripheral neuropathy-induced peripheral
nerve muscular atrophy (21).
However, whether CEPO is able to confer protection against DCM
remains unknown.
CEPO and rhEPO exert their anti-apoptotic effects
through their capacity to bind to EPOR-CD131, as EPO does (3,4).
However, they differ in their effects on erythropoiesis. rhEPO
binds to its classic receptor, (EPOR)2, and stimulates
red blood cell proliferation and differentiation, under the
regulation of hypoxia and vasoconstriction (14), which in turn is apt to result in an
excessive hematocrit and thrombogenesis. CEPO does not bind to
(EPOR)2, and therefore it does not increase the the risk
of blood clots by causing the excessive production of red blood
cells, even when it is used for long-term high-dose treatment, or
in the case of severe hypoxia (7,12).
In the present study, we revealed that the long-term use of CEPO
did not cause an elevation in the number of red blood cells in rats
with DCM. These results suggested that the application of CEPO may
reduce the risk of adverse effects, including thrombosis and high
blood pressure.
In the current study we used healthy male Wistar
rats, fed with a high-fat, high-carbohydrate diet, and treated with
STZ injections, to successfully generate rats with diabetes
mellitus. We used a TUNEL assay and TEM to observe myocardial cell
apoptosis, and demonstrated that CEPO and rhEPO protected
myocardial cells from apoptosis by reducing apoptotic rates and by
improving cell ultrastructure. These results were consistent with
the findings of previous studies (4,5).
Cell apoptosis is regulated through the balance
between pro- and anti-apoptotic proteins. Among those, caspase-3,
which belongs to the cysteinyl aspartate-specific protease
(caspase) family, is vital in initiating the process of apoptosis.
In the diabetic condition, high blood glucose-induced oxidative
stress activates the mitochondrial cytochrome c-mediated
caspase-3 pathway, resulting in myocardial cell apoptosis (22). Elevated caspase-3 expression has
been observed in the myocardial tissues of a number of pathological
conditions, including diabetes (23,24),
diabetic myocardial ischemia (25), myocardial infarction (26) and ischemia/reperfusion injury
(27), leading to increased
apoptosis. The inhibition of caspase-3 expression may confer
protection against diabetes-induced myocardial apoptosis (28). By contrast, Bcl-xl, which belongs
to the B cell lymphoma/leukemia-2 (Bcl-2) family, is considered to
be one of the major anti-apoptotic proteins. Bcl-xl is a dominant
subtype of the Bcl-x (Bcl-211) gene-encoding products (29), and its structure is similar to that
of Bcl-2. Bcl-xl has been demonstrated to be important in
protecting against the apoptosis of cardiomyocytes (30). In the current study, the expression
level of caspase-3 protein was increased, and that of Bcl-xl
protein was decreased in rats with DCM, compared with the levels in
the control group. CEPO treatment significantly downregulated
caspase-3 and upregulated Bcl-xl protein expression, suggesting
that CEPO has protective effects against apoptosis in DCM
myocardial cells. The binding of EPO to EPOR-CD131 affects multiple
signal transduction pathways, including the PI3K/Akt pathway, which
is crucial for insulin signal transduction, the cell cycle, and
cell growth and survival (31).
PI3K is an enzyme complex consisting of a regulatory subunit, p85,
and a catalytic subunit, p110. There are five subtypes of the
regulatory subunit: p85α and -β, p55γ and -α, and p50α. Among
these, p85α is the sole subtype to be correlated with the glucose
transporter 4 (31,32). The activation of PI3K subsequently
activates its downstream Ser/Thr protein kinase, Akt, also known as
protein kinase B. When Ser 308 and Thr 473 of Akt are
phosphorylated, Akt is activated (33). The phosphorylation of Akt (p-Akt)
further leads to the phosphorylation of Ser 196 of caspase-9, and
Ser 136 of Bcl-2-associated death promoter protein, which deprives
them of pro-apoptotic effects (34). High blood glucose, which leads to
myocardial oxidative stress, activates numerous inflammatory
cytokines, and induces myocardial apoptosis through the Akt pathway
(35). Myocardial atrophy in rats
with DCM is correlated with impaired Akt phosphorylation (36). In the current study, CEPO increased
PI3K (p85α) and Akt1 mRNA expression levels, and also enhanced
p-PI3K (p85) and p-Akt (Ser/Thr) protein expression levels in the
hearts of rats with DCM, in a dose-dependent manner. This suggested
that CEPO may exert anti-apoptotic effects in DCM through the
activation of the PI3K/Akt pathway, as rhEPO does. Notably,
although CEPO demonstrated a dose-dependent effect on DCM in this
study, the long-term (8-week) treatment of CEPO failed to
demonstrate a significant increase in PI3K (p85) and Akt1 mRNA
expression, and did not demonstrate a significant benefit, when
compared with the short-term (four-week) treatment. Therefore, a
time-dependent response of DCM to CEPO was not established.
In conclusion, CEPO exhibited myocardial protection,
without adverse effects on erythropoiesis, in rats with DCM, at
least in part through the activation of the PI3K/Akt pathway.
However, this study was based on animal models in vivo, and
detailed molecular mechanisms should be further investigated using
in vitro studies. Clinical trials may also be considered to
validate the results in humans, following further pre-clinical
studies.
Acknowledgements
The authors would like to thank
Medjaden Bioscience Limited (Hong Kong, China) for assisting in the
preparation of this manuscript.
References
|
1.
|
Fonarow GC and Srikanthan P: Diabetic
cardiomyopathy. Endocrinol Metab Clin North Am. 35:575–599. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Diskin CJ, Stokes TJ, Dansby LM, Radcliff
L and Carter TB: Beyond anemia: the clinical impact of the
physiologic effects of erythropoietin. Semin Dial. 21:447–454.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Brines M, Grasso G, Fiordaliso F, et al:
Erythropoietin mediates tissue protection through an erythropoietin
and common beta-subunit heteroreceptor. Proc Natl Acad Sci USA.
101:14907–14912. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Moon C, Krawczyk M, Paik D, et al:
Erythropoietin, modified to not stimulate red blood cell
production, retains its cardioprotective properties. J Pharmacol
Exp Ther. 316:999–1005. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Coleman TR, Westenfelder C, Tögel FE, et
al: Cytoprotective doses of erythropoietin or carbamylated
erythropoietin have markedly different procoagulant and vasoactive
activities. Proc Natl Acad Sci USA. 103:5965–5970. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Park KD, Mun KC, Chang EJ, Park SB and Kim
HC: Inhibition of erythropoietin activity by cyanate. Scand J Urol
Nephrol. 38:69–72. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Leist M, Ghezzi P, Grasso G, et al:
Derivatives of erythropoietin that are tissue protective but not
erythropoietic. Science. 305:239–242. 2004.PubMed/NCBI
|
|
8.
|
Adembri C, Massagrande A, Tani A, et al:
Carbamylated erythropoietin is neuroprotective in an experimental
model of traumatic brain injury. Crit Care Med. 36:975–978. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Bianchi R, Brines M, Lauria G, et al:
Protective effect of erythropoietin and its carbamylated derivative
in experimental Cisplatin peripheral neurotoxicity. Clin Cancer
Res. 12:2607–2612. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Fiordaliso F, Chimenti S, Staszewsky L, et
al: A nonerythropoietic derivative of erythropoietin protects the
myocardium from ischemia-reperfusion injury. Proc Natl Acad Sci
USA. 102:2046–2051. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Imamura R, Okumi M, Isaka Y, et al:
Carbamylated erythropoietin improves angiogenesis and protects the
kidneys from ischemia-reperfusion injury. Cell Transplant.
17:135–141. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Fantacci M, Bianciardi P, Caretti A, et
al: Carbamylated erythropoietin ameliorates the metabolic stress
induced in vivo by severe chronic hypoxia. Proc Natl Acad Sci USA.
103:17531–17536. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Xu X, Cao Z, Cao B, et al: Carbamylated
erythropoietin protects the myocardium from acute
ischemia/reperfusion injury through a PI3K/Akt-dependent mechanism.
Surgery. 146:506–514. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
King VR, Averill SA, Hewazy D, Priestley
JV, Torup L and Michael-Titus AT: Erythropoietin and carbamylated
erythropoietin are neuroprotective following spinal cord
hemisection in the rat. Eur J Neurosci. 26:90–100. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Xiong Y, Mahmood A, Zhang Y, et al:
Effects of posttraumatic carbamylated erythropoietin therapy on
reducing lesion volume and hippocampal cell loss, enhancing
angiogenesis and neuro-genesis, and improving functional outcome in
rats following traumatic brain injury. J Neurosurg. 114:549–559.
2011.
|
|
16.
|
Moon C, Krawczyk M, Lakatta EG and Talan
MI: Therapeutic effectiveness of a single vs multiple doses of
erythropoietin after experimental myocardial infarction in rats.
Cardiovasc Drugs Ther. 20:245–251. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Robey TE, Saiget MK, Reinecke H and Murry
CE: Systems approaches to preventing transplanted cell death in
cardiac repair. J Mol Cell Cardiol. 45:567–581. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Xu K, George I, Klotz S, et al:
Erythropoietin derivate improves left ventricular systolic
performance and attenuates left ventricular remodeling in rats with
myocardial infarct-induced heart failure. J Cardiovasc Pharmacol.
56:506–512. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Abe T, Isaka Y, Imamura R, et al:
Carbamylated erythropoietin ameliorates cyclosporine nephropathy
without stimulating erythropoiesis. Cell Transplant. 21:571–580.
2012. View Article : Google Scholar
|
|
20.
|
Imamura R, Isaka Y, Sandoval RM, et al: A
nonerythropoietic derivative of erythropoietin inhibits
tubulointerstitial fibrosis in remnant kidney. Clin Exp Nephrol.
16:852–862. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Schmidt RE, Green KG, Feng D, et al:
Erythropoietin and its carbamylated derivative prevent the
development of experimental diabetic autonomic neuropathy in
STZ-induced diabetic NOD-SCID mice. Exp Neurol. 209:161–170. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Cai L, Wang Y, Zhou G, Chen T, Song Y, Li
X and Kang YJ: Attenuation by metallothionein of early cardiac cell
death via suppression of mitochondrial oxidative stress results in
a prevention of diabetic cardiomyopathy. J Am Coll Cardiol.
48:1688–1697. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Chen J, Cha-Molstad H, Szabo A and Shalev
A: Diabetes induces and calcium channel blockers prevent cardiac
expression of proapoptotic thioredoxin-interacting protein. Am J
Physiol Endocrinol Metab. 296:E1133–E1139. 2009. View Article : Google Scholar
|
|
24.
|
Li JH, Zhang N and Wang JA: Improved
anti-apoptotic and anti-remodeling potency of bone marrow
mesenchymal stem cells by anoxic pre-conditioning in diabetic
cardiomyopathy. J Endocrinol Invest. 31:103–110. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Liu HR, Tao L, Gao E, et al: Rosiglitazone
inhibits hypercholesterolaemia-induced myeloperoxidase upregulation
- a novel mechanism for the cardioprotective effects of PPAR
agonists. Cardiovasc Res. 81:344–352. 2009.
|
|
26.
|
Bäcklund T, Palojoki E, Saraste A, et al:
Sustained cardiomyocyte apoptosis and left ventricular remodelling
after myocardial infarction in experimental diabetes. Diabetologia.
47:325–330. 2004.PubMed/NCBI
|
|
27.
|
Chowdhry MF, Vohra HA and Galiñanes M:
Diabetes increases apoptosis and necrosis in both ischemic and
nonischemic human myocardium: role of caspases and poly-adenosine
diphosphate-ribose polymerase. J Thorac Cardiovasc Surg.
134:124–131.e3. 2007. View Article : Google Scholar
|
|
28.
|
Xu J, Wang G, Wang Y, Liu Q, Xu W, Tan Y
and Cai L: Diabetes- and angiotensin II-induced cardiac endoplasmic
reticulum stress and cell death: metallothionein protection. J Cell
Mol Med. 13:1499–1512. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Carrington EM, McKenzie MD, Jansen E, et
al: Islet beta-cells deficient in Bcl-xL develop but are abnormally
sensitive to apoptotic stimuli. Diabetes. 58:2316–2323. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Morrissy S, Xu B, Aguilar D, Zhang J and
Chen QM: Inhibition of apoptosis by progesterone in cardiomyocytes.
Aging Cell. 9:799–809. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31.
|
Matsui T and Davidoff AJ: Assessment of
PI-3 kinase and Akt in ischemic heart diseases in diabetes. Methods
Mol Med. 139:329–338. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32.
|
Williams DL, Ozment-Skelton T and Li C:
Modulation of the phosphoinositide 3-kinase signaling pathway
alters host response to sepsis, inflammation, and
ischemia/reperfusion injury. Shock. 25:432–439. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Dhanasekaran A, Gruenloh SK, Buonaccorsi
JN, et al: Multiple antiapoptotic targets of the PI3K/Akt survival
pathway are activated by epoxyeicosatrienoic acids to protect
cardiomyocytes from hypoxia/anoxia. Am J Physiol Heart Circ
Physiol. 294:H724–H735. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34.
|
Amaravadi R and Thompson CB: The survival
kinases Akt and Pim as potential pharmacological targets. J Clin
Invest. 115:2618–2624. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Westermann D, Van Linthout S, Dhayat S, et
al: Cardioprotective and anti-inflammatory effects of interleukin
converting enzyme inhibition in experimental diabetic
cardiomyopathy. Diabetes. 56:1834–1841. 2007. View Article : Google Scholar
|
|
36.
|
Bilim O, Takeishi Y, Kitahara T, et al:
Diacylglycerol kinase zeta inhibits myocardial atrophy and restores
cardiac dysfunction in streptozotocin-induced diabetes mellitus.
Cardiovasc Diabetol. 7:22008. View Article : Google Scholar : PubMed/NCBI
|