Introduction
Multiple myeloma (MM) accounts for ∼10% of
hematological malignancies (1).
Despite the development of novel drug treatments and the advances
in stem cell transplantation, which have improved survival rates,
MM remains a difficult disease to cure. The involvement of the
central nervous system (CNS) in MM is rare, occurring in ∼1% of
patients (2). In these instances,
MM manifests as primary brain lesions, in the absence of initial
systemic MM and without appearing as a complication of systemic MM.
Gliomas account for 30–40% of all brain tumors (3). The World Health Organization (WHO)
divides astrocytomas into four grades, of which the WHO Grades III
(anaplastic astrocytoma) and IV (glioblastoma multiforme) are the
malignant subtypes (3). These are
invasive primary brain tumors that are difficult to treat and that
exhibit a rapid proliferation rate. Resection and radio- or
chemotherapies are the commonly accepted standard treatments,
although novel agents are being tested in clinical trials. The
coexistence of malignant astrocytoma and MM is exceedingly rare,
with few cases documented and, therefore, when a patient with MM
develops intracranial space-occupying lesions, the first diagnostic
assumption is an intracranial MM tumor, rather than a primary brain
tumor, such as astrocytoma. However, since the treatment and
prognosis of intracranial plasmacytomas and astrocytomas differ, a
definite differential diagnosis is imperative. In the current
study, we describe a case of a 49-year-old patient with MM, who
subsequently developed an anaplastic astrocytoma. In addition, we
discuss the importance of a differential diagnosis between
intracranial plasmacytoma and astrocytoma, as well the correlation
between MM and astrocytoma.
Case report
Primary treatment of the patient
A 49-year-old male was admitted to our hospital (The
First Affiliated Hospital of Zhejiang University School of
Medicine, Hangzhou, China) due to bone pain. The medical history of
the patient revealed no notable events or symptoms of fatigue,
weakness or recurrent infection during the preceding months, and
there was no evidence of mental or neurological impairment. The
results of a physical examination were as follows: total protein
level, 73.2 g/l (normal range, 60.0–83.0 g/dl); albumin level 51.1
g/l (normal range, 35.0–55.0 g/l); alkaline phosphatase level, 120
U/l (normal range, 30–115 U/l) and serum β2-microglobulin level,
3,092 μg/l (normal range, 0 to 2,300 μg/l). The serum
levels of the immunoglobulins IgG, IgA and IgM were all decreased
and a serum protein electrophoresis test did not reveal any
monoclonal peak. The 24-hour urinary protein excretion was 5.25 g
and a monoclonal peak was detected by urine protein
electrophoresis. Serum and urine immunofixation tests revealed
positive results for λ-light chains. The white blood cell (WBC)
count of the patient was 12.3×10E9/l (normal range,
4.0–10.0×10E9/l) and a bone marrow examination revealed 67.5%
atypical plasma cells. Further radiographic studies included a
normal brain computed tomography (CT) examination and a chest CT
scan that exhibited multiple rib and vertebral bone destruction. A
positron emission tomography (PET)-CT inspection indicated an
uneven bone mass density, and four ribs on the left side were
observed to be destroyed, with spindle-shaped soft tissue density
shades and increased fluorodeoxyglucose (FDG) metabolism. On the
right side, the eighth anterior rib was fractured. Following the
investigations, the patient was diagnosed with λ-light chain MM
[Durie-Salmon (DS) stage III, group A; International Staging System
(ISS) stage I).
The patient received chemotherapy, which comprised a
bortezomib-dexamethasone-cyclophosphamide regimen (1.3
mg/m2 intravenous bortezomib bolus on days 1, 4, 8 and
11; 20 mg/m2 intravenous dexamethasone on each day of
the bortezomib administration, as well as the following day; and
300 mg cyclophosphamide on days 1–4), every 21 days, for three
cycles. Four months subsequent to the end of the chemotherapy, the
patient underwent autologous stem cell transplantation. Following
the transplantation, the patient achieved a complete remission,
with negative serum and urine immunofixation results. The patient
was prescribed 100 mg thalidomide once a day for maintenance
therapy, while the serum and urine immunofixation results of the
patient were reviewed every six months, with further negative
results.
The study was approved by the Ethics Committee of
The First Affiliated Hospital of the Zhejiang University School of
Medicine, and informed consent was obtained from the
participant.
Secondary treatment of the patient
Twenty-two months following the autologous stem cell
transplantation, the patient presented with lower extremity
weakness, an unsteady gait and right-sided facial numbness. The
patient’s tongue deviated to the left when protruded and the
finger-nose test result was positive. Immunoglobulins (including
IgA, IgG and IgM) were all within the normal ranges and the serum
and urine immunofixation tests were negative. There were no
abnormal plasma cells in the bone marrow smears. Brain magnetic
resonance imaging (MRI) revealed a mass (27.3×34.0×30.0 mm) in the
right cerebellar hemisphere, with diffuse borders (Fig. 1). A PET-CT examination revealed
tissue occupying the right cerebellopontine angle with abnormal
increases in glucose metabolism, considered to be a malignant
tumor, and multiple sites of bone destruction with some mild
increases in glucose metabolism.
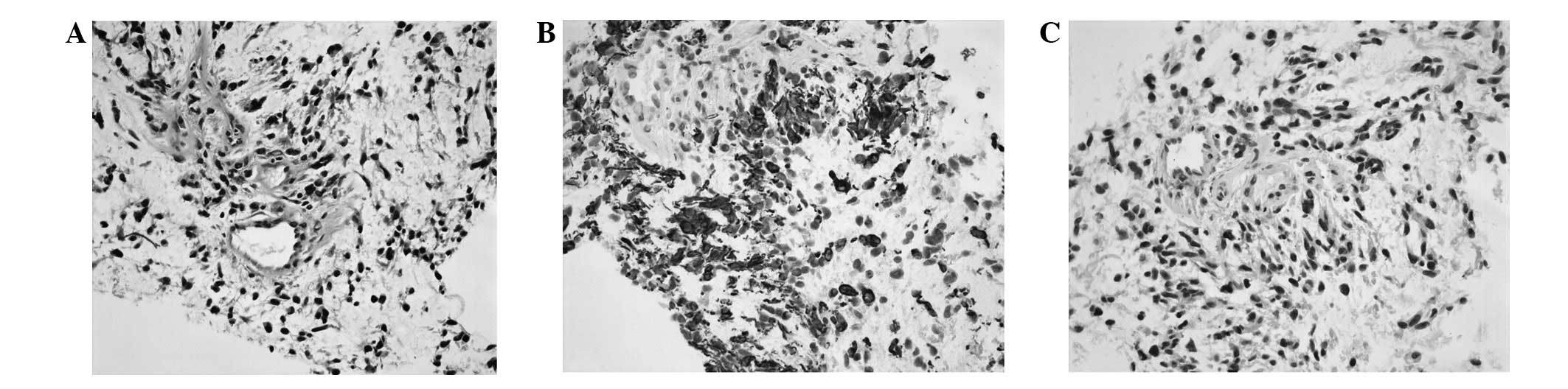
Initially, it was considered that the most likely
diagnosis for the brain lesions was a relapse of the MM. In order
to further investigate the tumor, a biopsy of the brain lesion was
performed and the immunohistochemistry results of the intracranial
needle biopsy-derived tumor cells were as follows: glial fibrillary
acidic protein (GFAP), (+++); S-100, (+++); oligodendrocyte
transcription factor-2 (Olig-2), (++); Wilms tumor-1 (WT-1), (+);
isocitrate dehydrogenase-1 (IDH1), (+−); P53, (0++);
O(6)-methylguanine-DNA methyltransferase (MGMT), (++);
neurofilament (NF), (−); synuclein (Syn), (−); CD34, (−); CD68,
(−); neuronal nuclei (Neu-N), (−); CD38, (−); CD138, (−); multiple
myeloma oncogene 1 (Mum-1), (−); Kappa, (+−); Lambda, (+−);
leukocyte common antigen (LCA), (−) and a Ki-67 labeling index of
∼10%, leading to the final diagnosis of an anaplastic astrocytoma
(WHO grade III; Fig. 2).
Due to the large size and undesirable location of
the lesion, the patient then received only localized irradiation,
as well as temozolomide chemotherapy, and was discharged from
hospital. One month subsequently, the patient became unconscious
and succumbed to cerebral hernia caused by the rapid progression of
the disease.
Discussion
The coexistence of astrocytoma and MM is extremely
rare. To the best of our knowledge, only four cases have been
reported to date (4–7). In two of the four cases, the
astrocytoma and MM were simultaneously diagnosed, while in the
remaining two cases the astrocytomas developed subsequently to MM.
By contrast, intracranial plasmacytomas affect a certain proportion
of patients with MM, with 109 cases documented up to 2007 (8). In such cases, the intracranial
plasmacytomas developed as primary manifestations of MM, following
systemic MM, subsequent to complete remission, or during the
disease progression. Due to the rarity of brain tumor developments
in patients with MM, the complication was initially only recognized
by neurological abnormalities; however, a further diagnosis was
then made, using MRI as the main method to detect an intracranial
tumor. MRIs of intracranial plasmacytomas generally appear as iso-
to hyper-intense T1-weighted and iso- to hypo-intense T2-weighted
images, with mild to marked contrast enhancement. Since
intracranial plasmacytomas generally arise from cranial bone
lesions or primary multiple dural myelomas, they usually appear in
osseous or dural contact in MRIs, although isolated parenchymal
involvements have been sporadically observed (9). By contrast, astrocytomas often
infiltrate the white matter and may involve both hemispheres by
spreading across the corpus callosum. Furthermore, they are usually
hypo-intense in T1-weighted images and hyper-intense in T2-weighted
images, exhibiting various degrees of edema and contrast
enhancement (10). In the present
case, the lesion was mildly hypo-intense in the T1-weighted and
hyper-intense in the T2-weighted images, without osseous or dural
contact, making a diagnosis of astrocytoma more likely than that of
a CNS myeloma.
Imaging examinations are initially adequate for
diagnosis; however, an unambiguous diagnosis depends on
pathological examinations. For the specific diagnosis of
intracranial plasmacytomas, a cerebrospinal fluid (CSF) examination
remains the test most commonly used, as monoclonal plasma cells are
easily detected, and pleocytosis, as well as increased protein
levels, are very common in CNS myeloma CSFs (11). By contrast, the CSF examinations of
patients with astrocytoma rarely reveal any abnormalities, unless
tumoral hemorrhages or meningeal involvements have occurred.
Despite this, when the results of the CSF examination are negative,
a biopsy remains the only diagnostic method capable of establishing
a definite diagnosis, which is important, due to the differences in
the treatments for CNS myelomas and astrocytomas. With regard to
CNS myeloma, radiotherapy (RT) has been demonstrated to be the most
effective therapy, while novel agents, such as thalidomide,
bortezomib and lenalidomide, have also resulted in good outcomes
(12–14). By contrast, resection (or biopsy)
and RT, along with temozolomide medication, remains the standard
therapy with regard to anaplastic astrocytomas (15).
Since the incidence of astrocytomas in patients with
MM is rare, a genetic aberration correlation between the two tumor
types is difficult to establish. Bone marrow stromal cell antigen 2
(BST2) has been identified as a tumor marker for astrocytomas
(16), and was first described as
a marker for B-cell maturation. It is commonly expressed in five
different human myeloma cell lines, as well as in monoclonal
neoplastic plasma cells (17);
however, the reason for this coexisting upregulation of a
particular B-cell membrane protein in astrocytes is unclear. A
further hypothetical correlation between the two tumor types is the
commonly activated nuclear factor-κB (NF-κB) pathway and the
excessive release of interleukin (IL)-6, which have been
demonstrated to promote tumor cell proliferation and the invasion
of astrocytoma and MM (18–20).
In general, and based on current knowledge, it has been proposed
that the development of secondary malignancies following MM is most
likely a multifactorial process, involving the treatment, the MM
and the patient, as well as environmental and behavioral factors
(21).
In conclusion, this case report describes a patient,
in whom an astrocytoma developed following MM, and emphasizes the
importance of a differential diagnosis between astrocytoma and
intracranial plasmacytoma. There is a requirement for clinicians to
consider the possibility of a glioma, in addition to plasmacytoma,
when a patient with MM presents with an intracranial
space-occupying lesion.
Acknowledgements
The authors would like to thank the
doctors from the Department of Neurology and Brain Surgery of the
First Affiliated Hospital (Zhejiang University School of Medicine,
Hangzhou, China) for the help and suggestions provided in the
diagnosis and treatment of the patients. This study was supported
by a grant from the province of Zhejiang traditional Chinese
medicine Bureau (grant no. 2010ZA057).
References
|
1.
|
Dimopoulos MA and Terpos E: Multiple
myeloma. Ann Oncol. 21(Suppl 7): 143–150. 2010. View Article : Google Scholar
|
|
2.
|
Fassas AB, Muwalla F, Berryman T, et al:
Myeloma of the central nervous system: association with high-risk
chromosomal abnormalities, plasmablastic morphology and
extramedullary manifestations. Br J Haematol. 117:103–108. 2002.
View Article : Google Scholar
|
|
3.
|
Schneider T, Mawrin C, Scherlach C, Skalej
M and Firsching R: Gliomas in adults. Dtsch Arztebl Int.
107:799–807. 2010.PubMed/NCBI
|
|
4.
|
Kato I, Kinouchi H, Imaizumi S, Katakura R
and Yoshimoto T: An autopsy case of cerebral astrocytoma associated
with multiple myeloma. No Shinkei Geka. 17:877–881. 1989.(In
Japanese).
|
|
5.
|
Gisserot O, de Jaureguiberry JP, Ribeil
JA, Villemagne B and Jaubert D: Cerebral glioblastoma complicating
the course of myeloma. Presse Med. 26:11971997.(In French).
|
|
6.
|
González Silva M: Second neoplasm in a
patient diagnosed with IgD myeloma. Presentation of a case and
review of the literature. Sangre (Barc). 38:47–49. 1993.(In
Spanish).
|
|
7.
|
Sonoda Y, Kumabe T, Umezawa K, Shimizu H,
Murakawa Y, Kanamaru R and Yoshimoto T: Rapid growth of
glioblastoma during therapy for multiple myeloma: case report. No
Shinkei Geka. 26:737–741. 1998.(In Japanese).
|
|
8.
|
Nieuwenhuizen L and Biesma DH: Central
nervous system myelomatosis: review of the literature. Eur J
Haematol. 80:1–9. 2008.
|
|
9.
|
Cerase A, Tarantino A, Gozzetti A, et al:
Intracranial involvement in plasmacytomas and multiple myeloma: a
pictorial essay. Neuroradiology. 50:665–674. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Sathornsumetee S, Rich JN and Reardon DA:
Diagnosis and treatment of high-grade astrocytoma. Neurol Clin.
25:1111–1139. 2007. View Article : Google Scholar
|
|
11.
|
Schluterman KO, Fassas AB, Van Hemert RL
and Harik SI: Multiple myeloma invasion of the central nervous
system. Arch Neurol. 61:1423–1429. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Quach H, Ryan G, Ganju V and Prince HM:
Effective treatment of leptomeningeal multiple myeloma with total
craniospinal irradiation supported by second allogeneic donor stem
cell infusion. Bone Marrow Transplant. 35:423–424. 2005. View Article : Google Scholar
|
|
13.
|
Gozzetti A, Cerase A, Lotti F, et al:
Extramedullary intracranial localization of multiple myeloma and
treatment with novel agents: a retrospective survey of 50 patients.
Cancer. 118:1574–1584. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Synhaeve NE, van der Heul C and Tijssen
CC: Intracranial mass of multiple myeloma with good response to
chemotherapy. BMJ Case Rep. 2012:2012.PubMed/NCBI
|
|
15.
|
Weller M: Novel diagnostic and therapeutic
approaches to malignant glioma. Swiss Med Wkly.
141:w132102011.PubMed/NCBI
|
|
16.
|
Wainwright DA, Balyasnikova IV, Han Y and
Lesniak MS: The expression of BST2 in human and experimental mouse
brain tumors. Exp Mol Pathol. 91:440–446. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Goto T, Kennel SJ, Abe M, Takishita M,
Kosaka M, Solomon A and Saito S: A novel membrane antigen
selectively expressed on terminally differentiated human B cells.
Blood. 84:1922–1930. 1994.PubMed/NCBI
|
|
18.
|
Goswami S, Gupta A and Sharma SK:
Interleukin-6-mediated autocrine growth promotion in human
glioblastoma multiforme cell line U87MG. J Neurochem. 71:1837–1845.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Liu Q, Li G, Li R, et al: IL-6 promotion
of glioblastoma cell invasion and angiogenesis in U251 and T98G
cell lines. J Neurooncol. 100:165–176. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Tanabe K, Matsushima-Nishiwaki R,
Yamaguchi S, Iida H, Dohi S and Kozawa O: Mechanisms of tumor
necrosis factor-alpha-induced interleukin-6 synthesis in glioma
cells. J Neuroinflammation. 7:162010. View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Thomas A, Mailankody S, Korde N,
Kristinsson SY, Turesson I and Landgren O: Second malignancies
after multiple myeloma: from 1960s to 2010s. Blood. 119:2731–2737.
2012. View Article : Google Scholar : PubMed/NCBI
|