Introduction
Gastric subepithelial tumors (SETs) have a
prevalence of ∼0.4% and are usually detected incidentally during
upper gastrointestinal (GI) endoscopy (1). The SET appears as a mass, bulge or
impression covered by normal epithelium with a protrusion to the
inside (intramural tumor) or outside (extramural tumor) of the
gastric wall (2). The majority of
the tumors are benign, but potentially and overtly malignant
lesions should not be neglected (3). According to current guidelines, large
(diameter, >3 cm) or symptomatic SETs require surgery due to
their malignant potential. However, the detection of a small SET
(diameter, ≤3 cm) presents diagnostic and therapeutic dilemmas. The
differential diagnosis is long and includes nonneoplastic lesions,
benign neoplasms and potentially and overtly malignant tumors.
Small asymptomatic SETs require periodic follow-up by endoscopy,
particularly by endoscopic ultrasound (EUS) examinations (4,5).
However, the definite discrimination of benign lesions from
malignant lesions may only be achieved by histopathological
examination (6). Previous studies
have shown that a standard endoscopic forceps biopsy and EUS-guided
fine needle aspiration (EUS-FINE) typically fails to obtain
material adequate for diagnosis (7–9).
Therefore, an accurate histopathological diagnosis may only be
performed by removal of the SET.
Traditionally, surgical approaches for removal
include open and laparoscopic or thoracoscopic surgery. Endoscopic
methods, including snare polypectomy, band ligation and endoscopic
submucosal dissection (ESD), have been used for the removal of GI
SETs, but their use has generally been restricted to tumors located
in the muscularis mucosae or submucosal layers (10,11).
En bloc resection of subepithelial tumors originating from the
muscularis propria layer using ESD remains problematic (12). The location of the tumor is a point
of concern when performing this procedure. Due to the knife
vertically orienting to the muscularis propria layer as a result of
retroflexion of the endoscope, when the tumor is in the fundus the
dissection is more challenging and more-time is taken for the
resection than when the tumor is in the body or the antrum. The
risks are also greater for resection of a tumor in the fundus than
for those in other locations. Iatrogenic perforation and its
inadequate closure are reported to be the major complications of
this procedure (13,14). New techniques, such as the use of
the Resolution clip, have been developed that enable secure closure
of iatrogenic perforations and have already been successfully used
in clinical practice in Shandong Provincial Hospital (Jinan,
China), Taian Central Hospital (Taian, China) and Dezhou People’s
Hospital (Dezhou, China).
The aim of this study was to evaluate the
feasibility of resection of small gastric SETs using the ESD
technique followed by closure of the gastric wall using Resolution
clips.
Patients and methods
Study design and study population
The study protocol was approved by the Ethics
Committees of Shandong Provincial Hospital, Taian Central Hospital
and Dezhou People’s Hospital. In this retrospective single-center
analysis, 11 consecutive patients (5 men, 6 women; median age 59.3
years, range 33–78) with gastric SETs were enrolled between October
2011 and December 2012 in Shandong Provincial Hospital, Jinan,
China. At first, EUS was performed with a radial-scanning echo
endoscope (GIF-T140; Olympus Optical Co. Ltd., Tokyo, Japan) to
determine the size, layer of origin, margin and growth pattern of
the SETs. The included patients met the following criteria: i) age
>18 years; ii) maximum size was measured by the EUS examination
before ESD between 1 and 3 cm as determined by EUS; iii) intramural
growth assessed by EUS; iv) tumors originated from the muscularis
propria; v) tumors located at the gastric fundus. Written informed
consent to undergo ESD was obtained from all included patients
after detailed spoken and written explanations were provided
concerning the ESD procedure and other possible treatment options.
Exclusion criteria, as used in a previous study, were as follows:
i) no consent from the patient; ii) American Society of
Anesthesiologists’ (ASA) class IV or V; iii) pregnancy; iv)
disorders of blood coagulation; v) contraindications for endoscopy;
vi) intramural or extramural large blood vessels within the
resection area detected by EUS (15).
Study apparatus
The main apparatuses used include an GIF-T140
endoscope, a double-channel upper GI endoscope (GIF-H260), a
double-bending double-channel upper GI endoscope (GIF-2T260M), a
transparent hood (D-201-11802), an insulated-tip knife 2 (IT-knife
2, KD-611L), a dural knife (KD-650L), Coagrasper hemostatic forceps
(FD-410LR), an injection needle (NM-4L-1) and a snare (SD-9L-1) all
from Olympus Optical Co. Ltd., Resolution clips (Boston Scientific,
Natick, MA, USA), endoclips (HX-600-135; Olympus Optical Co. Ltd.),
a high-frequency generator (ICC200; Erbe Elektromedizin GmbH,
Tübingen, Germany), an argon plasma coagulation (APC) unit (APC300;
Erbe Elektromedizin GmbH) and an auxiliary water jet (GIF-Q260J;
Olympus Optical Co. Ltd.).
Study procedures
The surgery was performed in the operating theater
with the patient under mechanically ventilated general anesthesia
and electrocardiographic monitoring.
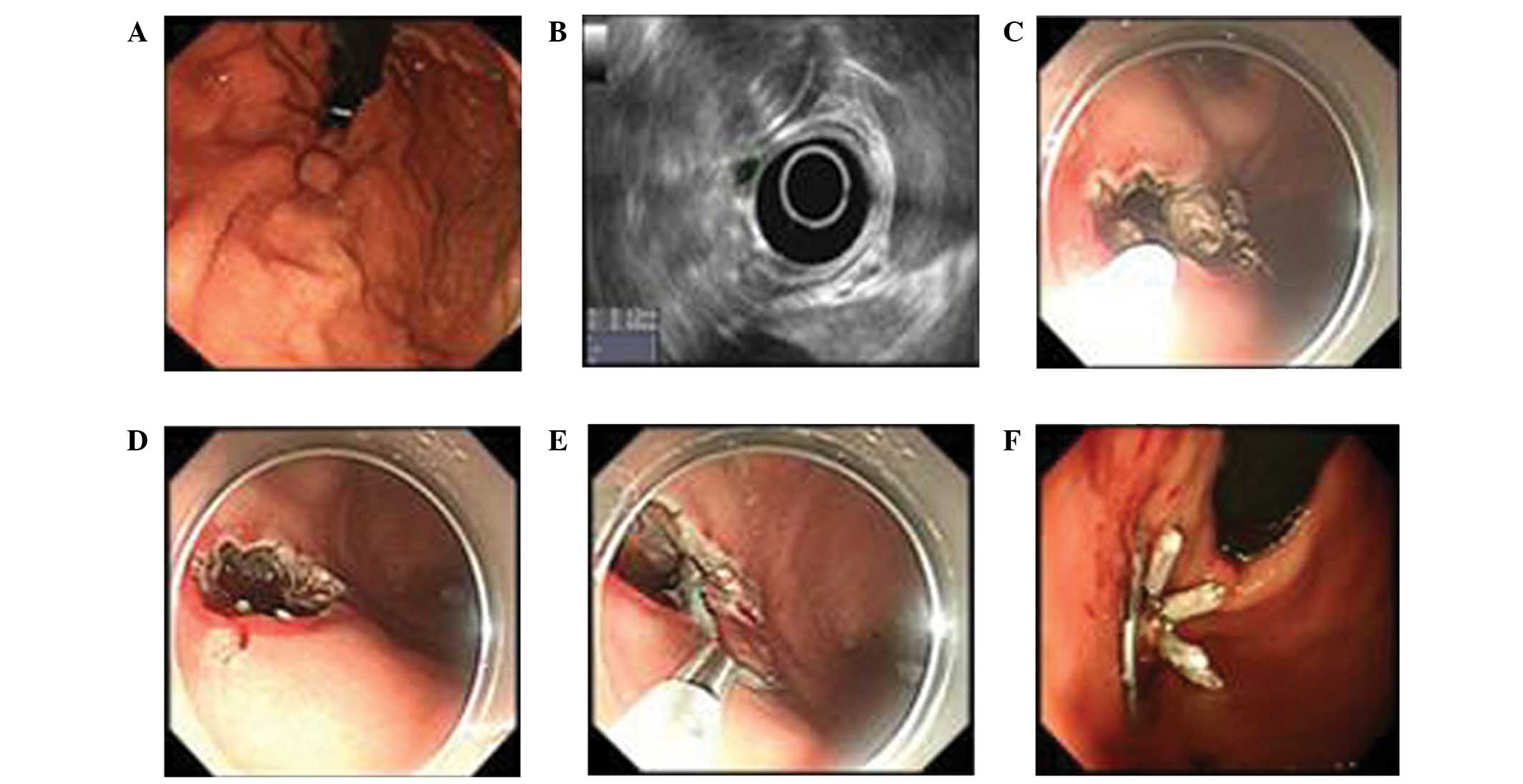
The procedure (Fig.
1) began by marking the lesion margins with APC. The tissue at
the proximal end of the subepithelial lesion was injected with 1–2
ml of a mixture prepared by diluting epinephrine (1 mg) and 0.8%
indigo carmine (2 ml) dye in 0.9% saline solution (500 ml) to
create a submucosal liquid pool. A precut of 3–5 mm was made at the
injection site using a dural knife with the electrosurgical
generator in the 30 W EndoCut mode. The IT-knife 2 was placed at
the initial incision to dissect the tissue and create a circular
incision around the lesion. When the submucosa was completely
separated from the tumor, the underlying muscularis propria was
dissected away to lift the tumor. During the dissection, it was
necessary to coagulate all visible vessels in the muscular and
submucosal layers and stop any bleeding using a forceps coagrasper
or by APC prior to the next step of the resection. Since the tumor
was located at the fundus, the final step of the dissection was
performed using the technique of polypectomy by employing an
electrocautery snare using blended electrosurgical current. All
tumors were retrieved by a net. The large defect of the gastric
wall following resection was closed completely with clips.
Resolution clips were used to close the defect or perforation first
in order to narrow the leaks. Endoclips were used for the closure
of the remaining small leaks. At the end of the procedure, a
leakage test was performed with methylene blue dye. Complete
resection was defined as the absence of any tumor remnant when
viewed endoscopically following resection. The patients were given
GI decompression and remained nil per os for three days with
parenteral alimentation and proton pump inhibitor treatment.
Pathological examination
The removed tumors were paraffin-embedded and
sectioned for histopathological and immunohistochemical analysis.
Staining was carried out with hematoxylin and eosin (H&E).
Additionally, immunohistochemical staining was performed on
paraffin-embedded tissue sections. Positive reactions for DOG-1 or
CD34 were considered diagnostic of a gastrointestinal stromal tumor
(GIST) and in cases where a GIST was suspected, the analysis
included a mitotic count under a high-power field (HPF) in order to
determine the malignant potential according to the classification
of Miettinen and Lasota (5).
Immunohistochemical analysis of CD117, smooth muscle actin (SMA),
desmin, S-100 and Ki67 markers was also performed to classify the
tumor subtype. Resection of the tumor was regarded as complete when
dissection margins were negative for tumor tissue (R0 resection)
and regarded as incomplete when there were positive margins (R1
resection) (17). Achievement of
R0 resection for gastric SETs with subsequent adequate closure of
the gastric wall was the target of the surgery and study.
Patient follow-up
The included patients were scheduled for follow-up
by telephone interview or at an outpatient visit 2 weeks after the
procedure, and by standard upper GI endoscopy 8 weeks after the
procedure. The interval between surveillance examinations was
extended to 6 months for leiomyomas and 3 months for GISTs based on
the results of histopathological evaluation.
Results
The characteristics of the 11 patients included in
the current study and their treatment outcomes are summarized in
Table I and in Fig. 1. All lesions were located at the
fundus and originated from the muscularis propria. Complete
resection was achieved in 10 of 11 lesions (90.9%). A switch to
laparoscopic wedge resection was necessary in one patient in whom
the tumor was attached to surrounding tissue (Table I). The mean resected tumor size was
18.8×17.2 mm, and the mean operation time of the 10 patients with
ESD was 81 min (range 45–130 min).
 | Table I.Clinicopathologic characteristics of
patients in this study and treatment outcomes. |
Table I.
Clinicopathologic characteristics of
patients in this study and treatment outcomes.
| Patient no. | Age (years) | Gender | Tumor size (mm) | Procedure time
(min) | Complete
resection/complication | Pathology
findings | Follow up time
(weeks/recurrence) |
|---|
| 1 | 59 | F | 15×15 | 95 | Yes | Leiomyoma, SMA+,
Desmin+, CD117-, Dog-, S-100-, Ki67<1% | 45/no |
| 2 | 57 | F | 20×18 | 100 | Yes | GIST, SMA-, Desmin-,
CD117+, Dog+, S-100-, Ki67=2%, mitosis/HPF=5/50 HPF | 30/no |
| 3 | 67 | F | 12×10 | 78 | Yes | GIST, SMA-, Desmin-,
CD117+, Dog+, S-100-, Ki67=2%, mitosis/HPF=5/50 HPF | 35/no |
| 4 | 60 | M | 15×9 | 62 | Yes | Leiomyoma, SMA+,
Desmin+, CD117-, Dog-, S-100-, Ki67<1% | 25/no |
| 5 | 48 | M | 25×15 | 110 | Yes/perforation | GIST, SMA-, Desmin-,
CD117+, Dog+, S-100-, Ki67=2%, mitosis/HPF=5/50 HPF | 25/no |
| 6 | 58 | M | 12×12 | 65 | Yes | GIST, SMA-, Desmin-,
CD117+, Dog+, S-100-, Ki67=2%, mitosis/HPF=5/50 HPF | 30/no |
| 7 | 53 | M | 30×28 | 130 | Yes/perforation | GIST, SMA-, Desmin-,
CD117+, Dog+, S-100-, Ki67=2%, mitosis/HPF=5/50 HPF | 25/no |
| 8 | 48 | M | 15×15 | 55 | Yes/perforation,
EPEB | GIST, SMA-, Desmin+,
CD117+, Dog+, S-100-, Ki67=3%, mitosis/HPF=5/50 HPF | 20/no |
| 9 | 49 | F | 15×15 | 45 | Yes | Leiomyoma, SMA+,
Desmin+, CD117-, Dog-, S-100-, Ki67<1% | 10/no |
| 10 | 51 | F | 25×20 | 70 | Yes | GIST, SMA-, Desmin+,
CD117+, Dog+, S-100-, Ki67=3%, mitosis/HPF=5/50 HPF | 10/no |
| 11a | 51 | F | 30×25 | NA | NA | GIST, SMA-, Desmin+,
CD117+, Dog+, S-100-, Ki67=3%, mitosis/HPF=5/50 HPF | NA |
Gastric perforation occurred in 3/11 patients
(27.2%). All perforations and defects were closed successfully by
endoscopic techniques using clips without surgical treatment
(Table I; Fig. 1). Early post-ESD bleeding (EPEB)
occurred in one patient. Basic ferric sulfate solution was sprayed
during the upper GI endoscopy and the bleeding stopped (Table I).
All 10 tumors that were removed endoscopically
showed macroscopically complete resection; R0 resection was
achieved with basal tumor-free margins microscopically. Eight
patients (72.7%) had GISTs. The HPF mitotic counts of all resected
tumors were low (<5 mitosis/50 HPFs). All GISTs were completely
resected. During follow-up, peritonitis and abdominal abscess were
not observed in the patients.
Discussion
Upper-GI SETs are often discovered incidentally
during routine upper GI endoscopic examination in the clinic. The
recommended management strategy includes periodic follow-up
endoscopy and EUS (18). However,
the optimum method and interval of follow-up of SETs have not yet
been precisely established. Indefinite follow-up examinations
without definite diagnosis may cause an enormous emotional strain
on patients (19). In addition,
accurate diagnosis is essential since a subset of these lesions do
have malignant potential, particularly GISTs originating from the
muscularis propria (20). ESDs are
performed to remove the whole tumor, which may be analyzed
histopathologically. Despite the development and modification of
endoscopic resection by ESD, recent studies have reported that
gastric SETs originating from the muscularis propria layer may be
successfully enucleated by endoscopy (13,21).
However, the complete endoscopic resection of gastric fundus SETs
that originate from the muscularis propria is more challenging than
that of tumors from other locations and layers in the stomach
(13,21,22).
The reasons may be as follows: i) The gastric fundus is in the
upper portion of the stomach and the operation requires
retroflexion of the endoscope. ii) The muscularis propria is a deep
layer of gastric wall and adjacent to the serosal layer. For this
reason, endoscopic resection has a higher rate of perforation than
the same procedure when used for the treatment of lesions located
in other gastric areas.
In addition to a double-channel upper GI endoscope
(GIF-H260; Olympus), a double-bending double-channel upper GI
endoscope (GIF-2T260M; Olympus) was used in our ESD procedure. By
using GIF-2T260M, we were able to focus on the lesion more
accurately and avoid misjudgment and mishandling. In the present
study, we performed ESD in 11 patients and complete endoscopic
resection of 10 upper-GI SETs that originated from the muscularis
propria. The unsuccessful case was a patient who had a tumor
severely adhering to surrounding tissue. The complete resection
rate was higher than reported by Shim and Jung (16) and similar to that in a study by Liu
et al (13). However, in
the study conducted by Liu et al, only two lesions were
located at the fundus.
The perforation rate (27.2%) was higher in the
current study than that in a previous study on ESD by Tanaka et
al (23). This may due to the
location and origin of the lesions. Several methods for the closure
of gastric endoscopic full-thickness resection have been described
in a preclinical and clinical setting (24–27),
but thus far the majority of these methods are technically
challenging, require specialized equipment and are thus limited
with respect to reproducibility and widespread applicability
(15,24,25).
In the present study, the perforations were closed by clips. The
defects following surgery were also closed by clips to prevent
delayed perforation. The two types of clips used were Resolution
clips from Boston Scientific and endoclips from Olympus Optical Co.
Ltd. The diameter of the Resolution clip is ∼13 mm, which is larger
than that of the endoclip. To handle the defect or perforation, we
first used the larger clip to minimize the leakage and then used
the endoclip to make a complete closure. All the defects and
perforations were closed successfully.
EPEB occurred in one patient. The patient had a
reduction in hemoglobin level of 3 g/dl within 16 h after surgery.
Basic ferric sulfate solution was sprayed during the upper GI
endoscopy and the bleeding stopped. EPEB is a common ESD-associated
complication with the occurrence of clinical symptoms and
laboratory changes (hemoglobin reduction >2 g/dl) that indicates
GI bleeding within 48 h of the ESD (28). In a large-scale study, the rates of
bleeding differed significantly in relation to the location of the
lesion, origin of the lesions, presence of a scar, histological
type and ESD time (29).
In the current study the majority of the resected
SETs were GISTs with very low risk and the others were leiomyomas.
However, the malignant potential of a GIST may not be reliably
determined in advance by either endoscopic or endosonographic
techniques (29). Alternative
endosonographic surveillance may delay the diagnosis of malignancy
and cause strain in many patients. Therefore, endoscopic resection
appears an advisable, less invasive therapeutic option, although
over-treatment of benign lesions may occur. We observed that 72.7%
of the resected SETs were GISTs, which was similar to the findings
of a previous study (30). Current
guidelines of the National Comprehensive Cancer Network recommend
that all GISTs >2 cm should be resected and that incidentally
encountered GISTs <2 cm may be either followed up or resected
(31). However, there remain
certain contradictions concerning the guideline (32). R0 resection of all suspected
lesions appears advisable. Local resection with gross negative
margins and without lymph node resection is considered a curative
approach since GISTs rarely have lymph node metastasis. As the
defects and perforations may be closed completely by clips, we
achieved R0 resection of all GISTs.
Our study has certain limitations. Firstly, certain
new techniques, such as submucosal tunneling, may be evaluated for
SETs located at the fundus next to the cardia. Secondly, more
patients are required for further studies.
In our opinion, a classic ESD technique using clips
for the dissection of small gastric fundus SETs from the deep
muscularis propria layer is feasible and easy to conduct.
Perforations that occur following full-thickness resection may be
adequately managed by clips.
References
|
1.
|
Hedenbro JL, Ekelund M and Wetterberg P:
Endoscopic diagnosis of submucosal gastric lesions: The results
after routine endoscopy. Surg Endosc. 5:20–23. 1991.PubMed/NCBI
|
|
2.
|
Connolly EM, Gaffney E and Reynolds JV:
Gastrointestinal stromal tumours. Br J Surg. 90:1178–1186. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Humphris JL and Jones DB: Subepithelial
mass lesions in the upper gastrointestinal tract. J Gastroenterol
Hepatol. 23:556–566. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4.
|
Hwang JH, Rulyak SD and Kimmey MB;
American Gastroenterological Association Institute: American
Gastroenterological Association Institute technical review on the
management of gastric subepithelial masses. Gastroenterology.
130:2217–2228. 2006. View Article : Google Scholar
|
|
5.
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: pathology and prognosis at different sites. Semin
Diagn Pathol. 23:70–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Hwang JH, Saunders MD, Rulyak SJ, et al: A
prospective study comparing endoscopy and EUS in the evaluation of
GI subepithelial masses. Gastroinest Endosc. 62:202–208. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Oka S, Tanaka S, Kaneko I, et al:
Advantage of endoscopic submucosal dissection compared with EMR for
early gastric cancer. Gastrointest Endosc. 64:877–883. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Mekky MA, Yamao K, Sawaki A, et al:
Diagnostic utility of EUS-guided FNA in patients with gastric
submucosal tumors. Gastrointest Endosc. 71:913–919. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Philipper M, Hollerbach S, Gabbert HE, et
al: Prospective comparison of endoscopic ultrasound-guided
fine-needle aspiration and surgical histology in upper
gastrointestinal submucosal tumors. Endoscopy. 42:300–305. 2010.
View Article : Google Scholar
|
|
10.
|
Sugimoto T, Okamoto M, Mitsuno Y, et al:
Endoscopic submucosal dissection is an effective and safe therapy
for early gastric neoplasms: a multicenter feasible study. J Clin
Gastroenterol. 46:124–129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Nishida T, Hirota S, Yanagisawa A, et al:
GIST Guideline Subcommittee: Clinical practice guidelines for
gastrointestinal stromal tumor (GIST) in Japan: English version.
Int J Clin Oncol. 13:416–430. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Białek A, Wiechowska-Kozłowska A and Huk
J: Endoscopic submucosal dissection of large gastric stromal tumor
arising from muscularis propria. Clin Gastroenterol Hepatol.
8:e119–e120. 2010.PubMed/NCBI
|
|
13.
|
Liu BR, Song JT, Qu B, et al: Endoscopic
muscularis dissection for upper gastrointestinal subepithelial
tumors originating from the muscularis propria. Surg Endosc.
26:3141–3148. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Demetri GD, von Mehren M, Antonescu CR, et
al: NCCN Task Force report: update on the management of patients
with gastrointestinal stromal tumors. J Natl Compr Canc Netw.
8(Suppl 2): S1–S41. 2010.PubMed/NCBI
|
|
15.
|
Schlag C, Wilhelm D, von Delius S, et al:
EndoResect study: endoscopic full-thickness resection of gastric
subepithelial tumors. Endoscopy. 45:4–11. 2013.PubMed/NCBI
|
|
16.
|
Shim CS and Jung IS: Endoscopic removal of
submucosal tumors: preprocedure diagnosis, technical options, and
results. Endoscopy. 37:646–654. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Hwang JC, Kim JH, Kim JH, et al:
Endoscopic resection for the treatment of gastric subepithelial
tumors originated from the muscularis propria layer.
Hepatogastroenterology. 56:1281–1286. 2009.PubMed/NCBI
|
|
18.
|
Polkowski M, Gerke W, Jarosz D, et al:
Diagnostic yield and safety of endoscopicult resound-guided trucut
[corrected] biopsy in patients with gastric submucosal tumors: a
prospective study. Endoscopy. 41:329–334. 2009.
|
|
19.
|
Yahagi N, Fujishiro M, Kakushima N, et al:
Endoscopic submucosal dissection for early gastric cancer using the
tip of an electrosurgical snare (thin type). Dig Endosc. 16:34–38.
2004. View Article : Google Scholar
|
|
20.
|
Polkowski M: Endoscopic ultrasound and
endoscopic ultrasound-guided fine-needle biopsy for the diagnosis
of malignant submucosal tumors. Endoscopy. 37:635–645. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
21.
|
Chung IK, Lee JH, Lee SH, et al:
Therapeutic outcomes in 1000 cases of endoscopic submucosal
dissection for early gastric neoplasms: Korean ESD Study Group
multicenter study. Gastrointest Endosc. 69:1228–1235. 2009.
View Article : Google Scholar
|
|
22.
|
Sugimoto T, Okamoto M, Mitsuno Y, et al:
Endoscopic submucosal dissection is an effective and safe therapy
for early gastric neoplasms: a multicenter feasible study. J Clin
Gastroenterol. 46:124–129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Tanaka M, Ono H, Hasuike N and Takizawa K:
Endoscopic submucosal dissection of early gastric cancer.
Digestion. 77(Suppl 1): S23–S28. 2008. View Article : Google Scholar
|
|
24.
|
Ikeda K, Fritscher-Ravens A, Mosse CA, et
al: Endoscopic full-thickness resection with sutured closure in a
porcine model. Gastrointest Endosc. 62:122–129. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Kaehler G, Grobholz R, Langner C, et al: A
new technique of endoscopic full-thickness resection using a
flexible stapler. Endoscopy. 38:86–89. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Arezzo A, Kratt T, Schurr MO and Morino M:
Laparoscopic-assisted transgastric cholecystectomy and secure
endoscopic closure of the transgastric defect in a survival porcine
model. Endoscopy. 41:767–772. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Zhou PH, Yao LQ, Qin XY, et al: Endoscopic
full-thickness resection without laparoscopic assistance for
gastric submucosal tumors originated from the muscularis propria.
Surg Endosc. 25:2926–2931. 2011. View Article : Google Scholar
|
|
28.
|
Takizawa K, Oda I, Gotoda T, et al:
Routine coagulation of visible vessels may prevent delayed bleeding
after endoscopic submucosal dissection - an analysis of risk
factors. Endoscopy. 40:179–183. 2008. View Article : Google Scholar
|
|
29.
|
Higashiyama M, Oka S, Tanaka S, et al:
Risk factors for bleeding after endoscopic submucosal dissection of
gastric epithelial neoplasm. Dig Endosc. 23:290–295. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Trupiano JK, Stewart RE, Misick C, et al:
Gastric stromal tumors: a clinicopathologic study of 77 cases with
correlation of features with nonaggressive and aggressive clinical
behaviors. Am J Surg Pathol. 26:705–714. 2002. View Article : Google Scholar
|
|
31.
|
Białek A, Wiechowska-Kozłowska A,
Pertkiewicz J, et al: Endoscopic submucosal dissection for
treatment of gastric subepithelial tumors (with video).
Gastrointest Endosc. 75:276–286. 2012.PubMed/NCBI
|
|
32.
|
Hoteya S, Iizuka T, Kikuchi D and Yahagi
N: Endoscopic submucosal dissection for gastric submucosal tumor,
endoscopic sub-tumoral dissection. Dig Endosc. 21:266–269. 2009.
View Article : Google Scholar
|
|
33.
|
Miettinen M, Sobin LH and Lasota J:
Gastrointestinal stromal tumors of the stomach: a
clinicopathologic, immunohistochemical, and molecular genetic study
of 1765 cases with long-term follow-up. Am J Surg Pathol. 29:52–68.
2005. View Article : Google Scholar : PubMed/NCBI
|