Introduction
Clinical imaging uses a variety of methods for the
evaluation of coronary arteries and ventricular function; these
techniques are categorized as either invasive or non-invasive and
include X-ray cardioangiography, transesophageal echocardiography
(ECHO), transthoracic ECHO, cardiac magnetic resonance imaging,
cardiovascular radionuclide imaging and cardiovascular computed
tomography (CT) imaging. Compared with the traditional
single-source multi-slice spiral CT, dual-source CT (DSCT) has a
faster scanning rate and a higher time resolution of 83 msec.
Therefore, coronary imaging using DSCT is less susceptible to
interference from the heart rate and expands the clinical
applications of CT in coronary imaging. DSCT is relatively
consistent in terms of accurately diagnosing coronary lesions when
used with coronary arteriography (also known as coronary
angiography, CAG). The imaging quality is susceptible to multiple
factors, including heart rate irregularities such as tachycardia
and arrhythmia, artifacts due to respiration and body movement,
parameters in scanning and reconstruction, selected trigger points
in the monitored layer, chosen reconstruction phases, adopted
injection velocity, dosage of the contrast and options of pitch
(1–4). Studies on the applications of DSCT
for evaluating cardiac morphology and function have been considered
noteworthy. Despite the possibility of overestimation or
underestimation, the left heart function evaluated by DSCT appears
to be reliable regardless of its inability to prove significant
differences in comparative studies, as compared with ultrasound or
MRI as the controls (5–7). Coronary stenosis leads to myocardial
ischemia or infarction, thereby negatively influencing cardiac
motor function. Different degrees of coronary stenoses differ in
the extent of their effect on cardiac function. The evaluation of
altered cardiac function based on the extent of coronary stenosis
is of great importance in clinical diagnosis, treatment, and
prognosis. Only a few studies on this topic have been conducted or
are currently ongoing. The present study aimed to determine the
accuracy of DSCT for evaluating coronary stenosis and cardiac
function (without the intake of heart rate-reducing agents).
Selective CAG and transthoracic ECHO were used as controls to
determine the correlation between various degrees of stenosis and
the altered left ventricular (LV) function, as well as the
significance of DSCT in clinical applications.
Materials and methods
Clinical data
Data were collected from 66 patients with coronary
heart disease, which included 40 males and 26 females aged 41 to 88
years old (mean, 62.7), with heart rates between 65 and 120 bpm as
well as normal rhythm. The patients enrolled in the study underwent
DSCT CAG between January 2012 and January 2013. A diagnosis was
established for every patient based on their history, physical
examination, electrocardiography (ECG), serum biochemistry and
myocardial enzyme levels. Patients with diseases such as rheumatic
heart disease were excluded. The patients underwent CAG and ECHO
within one week. This study was conducted in accordance with the
Declaration of Helsinki. This study was conducted with approval
from the Ethics Committee of the First Affiliated Hospital of
Nanjing Medical University, Nanjing, China. Written informed
consent was obtained from all participants.
The control group included 36 healthy volunteers who
underwent DSCT CAG. This group included 21 males and 15 females
aged 16 to 74 years-old (mean, 49.3), with heart rates of 60 to 110
bpm and normal rhythm. The volunteers were healthy; those with a
predisposition to any organic diseases were excluded. No
abnormalities were observed during the detailed inquiry of patient
history, physical examination, ECG, ECHO, serum biochemistry or
results of the examination of hepatic or renal function.
Scanning methods and data collection
Retrospective ECG-gated scanning was performed using
a DSCT machine (Somatom Definition; Siemens, Munich, Germany).
Prior to the scanning, the participants were prohibited from taking
heart rate-reducing agents, such as Betaloc. A scout view was
obtained for a patient holding his breath in a supine position,
while scanning from 1 cm inferior to the tracheal carina to 1.5 cm
inferior to the inferior border of the heart. A plain scan was
initially generated prior to the injection of the nonionic contrast
agent iohexol (350 mg I/ml) via the ulnar vein at a dosage of
80–100 ml at a rate of 4.5–5.5 ml/s. A contrast-triggered enhanced
scanning was then performed with the tracing level at the root of
the ascending aorta and the trigger threshold at 90–100 HU. The
scan was launched with a 6 sec delay and performed for 5 to 12 sec.
Following injection of the contrast agent, 30 ml 0.9% normal saline
was injected at the same rate. The following scanning parameters
were used: detector dimensions, 2×32×0.6 mm; layer thickness,
2×64×0.6 mm; rack rotation time, 330 msec; heart rate-dependent
pitch, 0.2–0.5; tube current time, 400 mAsec/cycle; and tube
voltage, 120 kV.
Off-line reconstruction was performed for the raw
material after the scanning was finished, with a 1 mm-thick
reconstruction layer, a 1 mm interval, a 10% R-R interval, and a
convolution function value of B26f. All-phase reconstruction at 0
to 95% was adopted to obtain images of the 20 cardiac cycles, which
were transferred to the workstation for analysis by Syngo
Circulation (Siemens). The short-axis, four-chamber, and
two-chamber views in each cycle were observed in cineloop to define
the ends of the diastole and systole. The LVA software (Siemens)
was used to analyze the cardiac function and delineate the
endocardium and epicardium, by covering the entire area from the
outflow tract to the left ventricle; the papillary muscles were
irregular and small, and therefore ignored. The end-diastolic
volume (EDV), endsystolic volume (ESV), stroke volume (SV),
ejection fraction (EF) and myocardial mass (MM) of the left
ventricle were automatically calculated based on the Simpson’s rule
for numerical integration. The mean of triplicate measurements was
recorded. The data included in this study were obtained by one
physician proficient in the use of the software.
Analysis of coronary stenosis shown by
angiography
The degree of stenosis was qualitatively evaluated
using the area method. The stenoses were categorized into three
groups based on the routine standards commonly used in clinical
practice, namely, the mild group with <50% stenosis, the
moderate group stenosis with between 50 and 75% stenosis, and the
severe group with ≥75% stenosis (8). The stenoses in multiple branches were
categorized according to the narrowest branch.
ECHO analysis
Two-dimensional ECHO was performed using a Color
Doppler intelligent diagnostic system (Philips IE 33, Amsterdam,
The Netherlands). The examinations were performed by one senior
physician.
Statistical analysis
The data were expressed as mean ± standard
deviation. A paired χ2 test was performed to compare the
coronary stenosis evaluated by CAG and DSCT CAG. The two-sample
Student’s t-test and the Pearson correlation analysis were used to
correlate the cardiac function based on DSCT against the ECHO
findings. The two-sample Student’s t-test and q-test were used to
analyze the effect of different degrees of coronary stenosis on
cardiac function. P<0.05 was considered to indicate a
statistically significant result.
Results
Coronary stenosis evaluated by DSCT
Out of the 330 assessable arteries, 211 exhibited
stenosis based on the DSCT results [right coronary artery (RCA),
left anterior descending artery (LAD), diagonal branch (Diag), left
circumflex coronary artery (LCX), left obtuse marginal branch
(LOM)] of 66 patients, out of which 196 were confirmed by selective
CAG. Only 12 instances of selective CAG-identified stenoses were
not detected by DSCT CAG (Table
I). The paired χ2 test (McNemar test) with P=0.701
(P>0.05) and κ coefficient test (kappa test) with κ=0.824
(κ≥0.7; P=0.000) suggested a high level of consistency between the
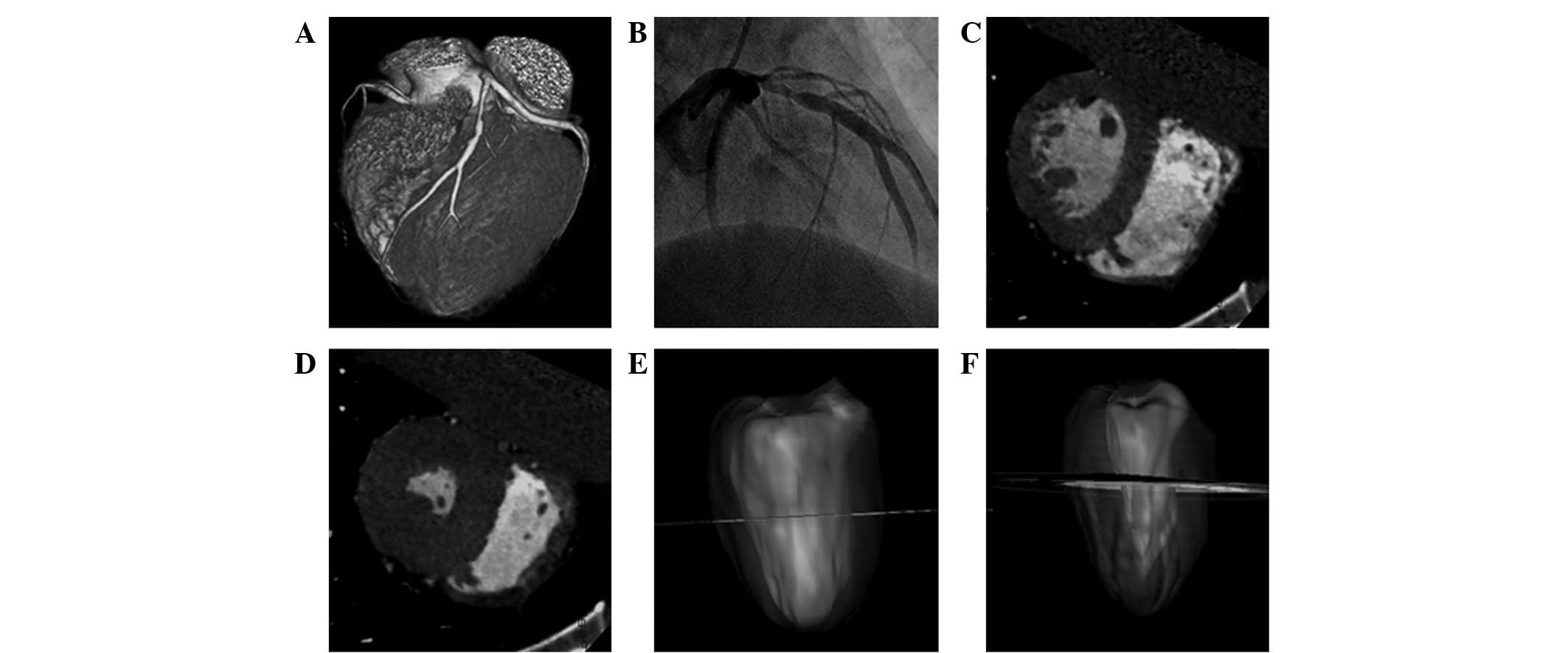
DSCT CAG and selective CAG results. No significant differences in
the capacity to diagnose coronary stenosis were observed between
the two approaches (Fig. 1A and
B).
 | Table I.Comparative analysis between coronary
artery DSCT-CTA and the selective CAG control. |
Table I.
Comparative analysis between coronary
artery DSCT-CTA and the selective CAG control.
| Coronary artery
DSCT-CTA | CAG
| Total (segment) |
|---|
| Positive
(segment) | Negative
(segment) |
|---|
| Positive
(segment) | 196 | 15 | 211 |
| Negative
(segment) | 12 | 107 | 119 |
| Total (segment) | 208 | 122 | 330 |
Comparison of LV function as evaluated by
DSCT and ECHO
The results showed that the EDV, SV and EF of the
left ventricle in the disease and control groups were slightly
higher, while ESV was slightly lower when measured by DSCT, as
compared with those measured by ECHO. However, no significant
differences were observed between the parameters of cardiac
function measured by the two methods (P>0.05; Tables II and III).
| Table II.Comparison of left ventricular
function between DSCT and ECHO in the control group. |
Table II.
Comparison of left ventricular
function between DSCT and ECHO in the control group.
| Parameters of left
ventricular function | DSCT | ECHO | r-value | P-value |
|---|
| EDV (ml) | 100.78±13.78 | 97.61±13.32 | 0.81 | 0.92 |
| ESV (ml) | 31.56±7.44 | 31.61±6.99 | 0.90 | 0.91 |
| SV (ml) | 69.22±10.96 | 66.00±9.88 | 0.71 | 0.96 |
| EF (%) | 68.67±5.88 | 67.69±5.19 | 0.83 | 0.65 |
| Table III.Comparison of determined parameters of
left heart function by DSCT with those by ECHO in the stenosis
group. |
Table III.
Comparison of determined parameters of
left heart function by DSCT with those by ECHO in the stenosis
group.
| Parameters of left
ventricular function | DSCT | ECHO | r-value | P-value |
|---|
| EDV (ml) | 124.85±50.81 | 121.20±48.15 | 0.76 | 0.91 |
| ESV (ml) | 51.91±38.96 | 52.25±36.02 | 0.91 | 0.88 |
| SV (ml) | 72.02±25.87 | 68.95±24.43 | 0.72 | 0.89 |
| EF (%) | 59.72±13.68 | 58.45±11.81 | 0.83 | 0.69 |
Association between the degree of
coronary stenosis and the parameters of LV function
There were 36 individuals in the control group, and
8, 22 and 36 patients in the mild, moderate and severe stenosis
groups, respectively. The q-test of paired comparisons revealed
significant differences in the ESV, EF and SV in the severe group,
as compared with those of the mild or the moderate groups (both
P<0.05). However, these parameters were not significantly
different between the mild and the moderate groups (P>0.05).
Significant differences were observed in EDV and MM among the three
stenosis groups (P<0.05). No significant differences were
demonstrated among the parameters of the control group, as compared
with those of the mild stenosis group (P>0.05; Table IV).
| Table IV.Correlation between the degree of
coronary stenosis and parameters of left ventricular function. |
Table IV.
Correlation between the degree of
coronary stenosis and parameters of left ventricular function.
| Parameters of left
ventricular function | Control | Mild stenosis | Moderate
stenosis | Severe stenosis | P-value |
|---|
| EDV (ml) | 100.78±13.78 | 104.56±20.21 | 115.43±23.66 | 138.34±36.14 | <0.05 |
| ESV (ml) | 31.56±7.44 | 35.42±20.53 | 38.54±21.64 | 59.21±43.56 | >0.05a |
| SV (ml) | 69.22±10.96 | 72.75±10.44 | 66.84±15.76 | 41.43±13.28 | >0.05a |
| EF (%) | 68.67±5.88 | 67.29±11.34 | 66.37±12.98 | 31.76±8.97 | >0.05a |
| MM (g) | 97.60±17.64 | 107.45±12.74 | 136.86±8.32 | 155.46±34.07 | <0.05 |
Discussion
The use of CAG with spiral CT has become an
important invasive approach for coronary imaging. In addition, the
parameters of ventricular function may be obtained while
angiography is conducted and thus provide more informative data for
clinical practice. The dosage of heart rate-reducing agents prior
to the examination may interfere with the results (9) Therefore, the results of the DSCT CAG
performed without artificial control of the heart rate may
overestimate the actual values. The extent of coronary stenosis
similarly influences the alteration of LV function to a certain
degree.
Previous studies (10,11)
have revealed the high sensitivity, specificity and accuracy of
DSCT performed under stable heart rate conditions without obvious
variability or arrhythmia, in diagnosing significant stenosis in
coronary arteries. Similarly, our results from patients who did not
take heart rate-reducing agents suggested that DSCT CAG is capable
of consistently diagnosing coronary stenosis without significant
differences. However, multiple factors may affect CAG. Incorrect or
incomplete diagnoses of the patients may be correlated with the
flowing velocity of the contrast, twisted courses of blood vessels
and the calcification in the vascular wall. Certain studies
(12–14) have suggested that the tendency of
multi-slice spiral CT to overestimate coronary stenosis is
correlated with the spatial resolution being used, particularly the
effect of the partial volume effect on the calcified vessel wall.
Despite its inability to provide hemodynamic information, CT may
rule out the presence of obvious coronary stenosis, therefore, this
method has important applications in clinical practice. Therefore,
a close-up view from multiple angles with numerous aspects should
be used while analyzing CAG to minimize errors or missed
diagnoses.
By distinguishing the defined borders of the
endocardium and epicardium, DSCT may reveal the anatomical
structure of the heart more clearly than ultrasound scan. Due to
its large capacity for raw data and a powerful post-processing
software, DSCT is capable of semi-automatically delineating the
ventricular contours and enabling the repeated playback of
three-dimensional movies that simultaneously show multiple
positions of the heart (Fig.
1C–F), thereby indicating its high reproducibility (15). ECHO is the most frequently used
approach for clinically evaluating cardiac function and it was used
as the control. The results of DSCT and ECHO were highly
consistent; their values for EDV, ESV, SV and EF were not
significantly different. However, the parameters evaluated by DSCT
(with the exception of ESV) were slightly higher than those by
ECHO. Previous studies suggested that overestimation or
underestimation exists in both MDCT and DSCT when ECHO is adopted
as the control (6,16,17).
These inconsistencies are due to the lack of similar temporal
resolution among the different techniques. However, the differences
have no statistical significance, which shows that these techniques
are of great clinical importance. Systematic underestimation exists
in various parameters of cardiac function evaluated by MRI, while
the underestimation or overestimation occurs in results evaluated
by the 64-layer spiral CT due to its dependence upon the heart
rate. A comparison of the two approaches indicated that DSCT
appeared to have the least number of errors (18). In addition, no heart rate-reducing
agent was required by DSCT, thereby eliminating the influence of
artificial factors on cardiac function and making the results more
accurate.
Coronary stenosis leads to myocardial ischemia. The
blood flow reserve for coronary vessels gradually decreases with
the increasing severity of coronary stenosis, and resting
ventricular ataxia occurs at this stage. This proceeds to altered
cardiac functions, including weakened myocardial contractility,
enlarged heart and decreased compliance, as well as congestion in
the left ventricle and the left atria. The increased EDV and
decreased EF reflect the gradual loss of compensation on the left
side of the heart, as well as predict the onset of left-sided heart
failure and poor prognosis. Myocardial ischemia and anoxia may
cause myocardial hypertrophy and thickened ventricular walls,
thereby increasing MM but decreasing myocardial contractility. In
clinical practice, the evaluation of varying cardiac functions
according to the degree of coronary stenosis is of great
importance. Along with the increasing number of coronary branches
with lesions and the aggravating stenosis, cardiac function
gradually worsens. In this study, patients were categorized into
three groups by evaluating the coronary stenosis, which is
frequently used in clinical practice. No significant variation was
observed in the parameters in the mild group compared with those of
the controls. Similarly, no significant changes were observed in
the ESV, SV or EF in the moderate stenosis group. However,
significant changes were noted in the severe stenosis group.
Myocardial compensation continued to be achieved in certain cases
of mild or moderate stenosis of the coronary arteries. The enhanced
myocardial contractibility may aid maintenance of systemic
circulation and avoid a significant reduction of the EF, which may
occasionally undergo a compensatory increase. A significant
reduction in the EF occurred with the decompensation of cardiac
function in the severe stenosis group. The decreasing EF was
closely correlated with the incidence and mortality of acute
myocardial infarction. EDV and MM were significantly increased in
the moderate stenosis group, and increased further in the severe
group relative to the moderate group. Therefore, EDV and MM are
likely more sensitive than EF in terms of reflecting the variation
of cardiac function. Along with the increasing EDV that occurs with
ventricular wall tension, myocardial oxygen consumption was further
increased with aggravated myocardial ischemia. Simultaneously, the
MM may gradually increase and further aggravate cardiac
contractibility, thereby suggesting that severe myocardial ischemia
damages LV systolic functions.
This study is primarily limited by the use of only
the mild, moderate and severe categories in the interest of
simplification and pragmatism. Our results would have been more
meaningful if stenosis sites at the trunk or branch, as well as the
lesions in single or multiple branches were considered. Our study
is further limited by the size of the samples used. Therefore,
further studies are required to investigate patients with different
types of arrhythmias. Despite its high temporal and spatial
resolution, DSCT has a limited capacity to accurately identify
stenosis due to motion and halo artifacts induced by arrhythmias
and calcification, respectively. DSCT is similarly challenged by
controversies concerning ionizing radiation (19,20).
Thus, future studies are required to focus on the realization of
scanning with reduced radiation.
None of the previously available data indicate that
heart CT scans have been used to evaluate cardiac function alone.
However, data with regard to cardiac function may be utilized
during CAG to obtain additional information (12). Our results suggest that the degree
of coronary stenosis may be used to evaluate variations in cardiac
function. Significant changes to the EDV and MM in the left
ventricle of the moderate stenosis group, as well as those of all
the parameters in the severe group, may aid in the diagnosis, early
intervention and prognosis of stenosis. Therefore, acute coronary
events and heart failure may be prevented. DSCT during one
examination is able to accomplish the simultaneous observation of
two parameters, including the morphology of coronary vessels and
the biology of EFs. Therefore, DSCT is the fastest method for
non-invasive cardiovascular examination, with clinical applications
of great significance.
References
|
1.
|
Leber AW, Johnson T, Becker A, et al:
Diagnostic accuracy of dual-source multi-slice CT-coronary
angiography in patients with an intermediate pretest likelihood for
coronary artery disease. Eur Heart J. 28:2354–2360. 2007.PubMed/NCBI
|
|
2.
|
Alkadhi H, Scheffel H, Desbiolles L, et
al: Dual-source computed tomography coronary angiography: influence
of obesity, calcium load, and heart rate on diagnostic accuracy.
Eur Heart J. 29:766–776. 2008.PubMed/NCBI
|
|
3.
|
Weustink AC, Mollet NR, Pugliese F, et al:
Optimal electrocardiographic pulsing windows and heart rate: effect
on image quality and radiation exposure at dual-source coronary CT
angiography. Radiology. 248:792–798. 2008.
|
|
4.
|
Tsiflikas I, Drosch T, Brodoefel H, et al:
Diagnostic accuracy and image quality of cardiac dual-source
computed tomography in patients with arrhythmia. Int J Cardiol.
143:79–85. 2010.PubMed/NCBI
|
|
5.
|
Groen JM, van der Vleuten PA, Greuter MJ,
Zijlstra F and Oudkerk M: Comparison of MRl, 64-slice MDCT and DSCT
in assessing functional cardiac parameters of a moving heart
phantom. Eur Radiol. 19:577–583. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Stolzmann P, Scheffel H, Trindade PT, et
al: Left ventricular and left atrial dimensions and volumes:
comparison between dual-source CT and echocardiography. Invest
Radiol. 43:284–289. 2008.PubMed/NCBI
|
|
7.
|
Bastarrika G, Arraiza M, De Cecco CN,
Mastrobuoni S, Ubilla M and Rábago G: Quantification of left
ventricular function and mass in heart transplant recipients using
dual-source CT and MRI: initial clinical experience. Eur Radiol.
18:1784–1790. 2008.PubMed/NCBI
|
|
8.
|
Leber AW, Knez A, von Ziegler F, et al:
Quantification of obstructive and nonobstructive coronary lesions
by 64-slice computed tomography: a comparative study with
quantitative coronary angiography and intravascular ultrasound. J
Am Coll Cardiol. 46:147–154. 2005. View Article : Google Scholar
|
|
9.
|
Jensen CJ, Jochims M, Hunold P, et al:
Assessment of left ventricular function and mass in dual-source
computed tomography coronary angiography: influence of
beta-blockers on left ventricular function: comparison to magnetic
resonance imaging. Eur J Radiol. 74:484–491. 2010.
|
|
10.
|
Scheffel H, Alkadhi H, Plass A, et al:
Accuracy of dual-source CT coronary angiography: First experience
in a high pre-test probability population without heart rate
control. Eur Radiol. 16:2739–2747. 2006.PubMed/NCBI
|
|
11.
|
Feuchtner G, Loureiro R, Bezerra H, et al:
Quantification of coronary stenosis by dual source computed
tomography in patients: a comparative study with intravascular
ultrasound and invasive angiography. Eur J Radiol. 81:83–88.
2012.PubMed/NCBI
|
|
12.
|
Mahnken AH, Mühlenbruch G, Günther RW and
Wildberger JE: Cardiac CT: coronary arteries and beyond. Eur
Radiol. 17:994–1008. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Cury RC, Nieman K, Shapiro MD, Nasir K,
Cury RC and Brady TJ: Comprehensive cardiac CT study: evaluation of
coronary arteries, left ventricular function, and myocardial
perfusion - is it possible? J Nucl Cardiol. 14:229–243. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Leschka S, Scheffel H, Desbiolles L, et
al: Combining dual-source computed tomography coronary angiography
and calcium scoring: added value for the assessment of coronary
artery disease. Heart. 94:1154–1161. 2008.PubMed/NCBI
|
|
15.
|
Bak SH, Ko SM, Jeon HJ, Yang HS, Hwang HK
and Song MG: Assessment of global left ventricular function with
dual-source computed tomography in patients with valvular heart
disease. Acta Radiol. 53:270–277. 2012.PubMed/NCBI
|
|
16.
|
Ko SM, Kim YJ, Park JH and Choi NM:
Assessment of left ventricular ejection fraction and regional wall
motion with 64-slice multidetector CT: a comparison with
two-dimensional transthoracic echocardiography. Br J Radiol.
83:28–34. 2010. View Article : Google Scholar
|
|
17.
|
Bruners P, Knackstedt C, Mahnken AH, et
al: Global left ventricular function: assessment with dual-source
CT versus conventional ventriculography in a porcine model. Acta
Cardiol. 64:311–319. 2009.PubMed/NCBI
|
|
18.
|
Groen JM, van der Vleuten PA, Greuter MJ,
Zijlstra F and Oudkerk M: Comparison of MRI, 64-slice MDCT and DSCT
in assessing functional cardiac parameters of a moving heart
phantom. Eur Radiol. 19:577–583. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Mahnken AH, Bruners P, Schmidt B,
Bornikoel C, Flohr T and Günther RW: Left ventricular function can
reliably be assessed from dual-source CT using ECG-gated tube
current modulation. Invest Radiol. 44:384–389. 2009.PubMed/NCBI
|
|
20.
|
Earls JP, Berman EL, Urban BA, et al:
Prospectively gated transverse coronary CT angiography versus
retrospectively gated helical technique: improved image quality and
reduced radiation dose. Radiology. 246:742–753. 2008. View Article : Google Scholar
|