Introduction
Acquired immune deficiency syndrome (AIDS) is a
serious disease that spread rapidly in the world since 1984. AIDS
has spread rapidly in China as well as numerous other developing
countries. During the end of the last decade, AIDS spread rapidly
through serum sampling in Henan Province, China. Chronic heart
disease contributes to the mortality of individuals with AIDS
(1,2). Although studies of left ventricular
function in patients with AIDS have been conducted (3–6),
studies of right ventricular function are rare, thus, the
phenomenon remains unclear. For this reason, the present study
investigated the characteristics of tricuspid annulus movement and
evaluated right ventricular function in patients with AIDS by
Doppler tissue imaging (DTI), which is a quantitative method that
evaluates ventricular myocardial function, to explore whether the
right ventricular function was damaged in patients with AIDS.
Materials and methods
Patients
In total, 106 patients with AIDS were enrolled in
the study, comprising 46 males (43.40%) and 60 females (56.60%),
aged 20–59 years, with a mean age of 41.26±7.47 years. The CD4
counts ranged between 1 and 390 cells/μl, with a mean of
185.09±118.12/μl. All cases were infected by serum sample and were
confirmed to be infected with the testing of plasma samples (GE
Medical Systems, Horton, Norway) . The infection period was between
4 and 27 years, with a mean of 11.69±4.04 years. The AIDS group was
compared with an age- and gender-matched population of 64 normal
subjects. No abnormal observations in the control group were
observed by physical examination, X-ray, electrocardiography (ECG)
and echocardiography. None of the enrollees had a medical history
of cardiovascular abnormalities and none of the patients with AIDS
had undergone highly active antiretroviral therapy. The study was
conducted in accordance with the Declaration of Helsinki and with
approval from the Ethics Committee of the People’s Hospital of
Zhengzhou University (Zhengzhou, China). Written informed consent
was obtained from all participants.
Methods
Echocardiography was performed in all enrollees
using American GE Vivid 3 or 7 ultrasound systems (GE Healthcare,
Little Chalfont, UK), with transducer frequencies of 1.7–3.5 and
1.5–4.0 MHz, respectively. Enrollees were positioned in the
left-lateral position and had normal respiration. Doppler tissue
velocity mode was used and focused at the tricuspid annulus level,
with a sample volume between 4 and 5 mm. Care was taken in
directing the transducer beam as close as possible to the DTI beam
at <20° in selected planes. Tricuspid annulus movements in all
subjects were detected from the apical four-chamber view and the
apical right heart two-chamber view. The peak diastolic early
period velocity (Ve), peak diastolic later period velocity (Va) and
peak systolic velocity (Vs) were measured at four sites (anterior,
posterior, lateral wall and interventricular septum) and the mean
value of these variables, including ‘s’, ‘e’ and ‘a’, were
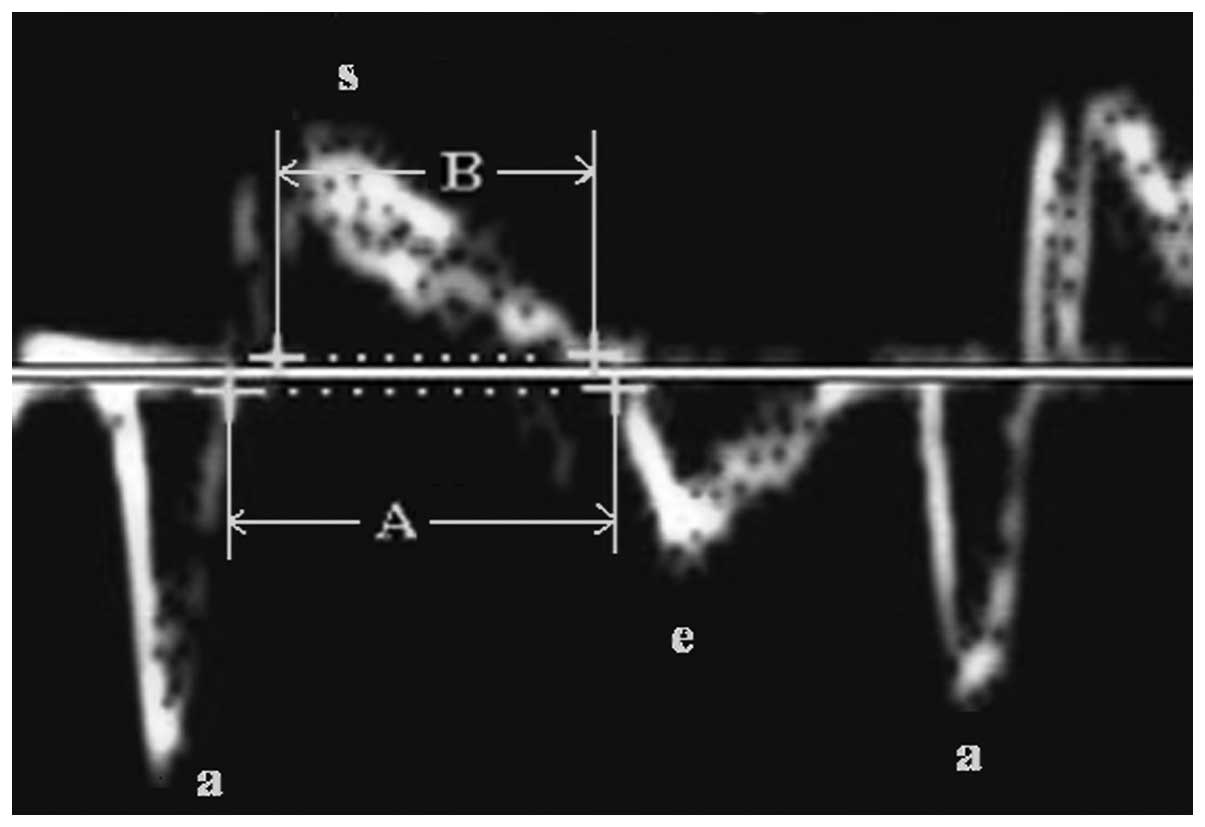
calculated. The DTI spectrum of tricuspid annulus movements
includes three waves: ‘s’, movement towards the apical during
systole; ‘e’, quick movement towards the roof of the atrium during
early diastole; and ‘a’, movement caused by atrium systole during
late diastole. At the lateral site of the tricuspid annulus, the
interval from the end of the ‘a’ wave to the beginning of the next
‘e’ wave, was recorded as line A and the interval from the
beginning to the end of the ‘s’ wave was recorded as line B. The
Tei index was calculated using the following formula: (A – B)/B.
All parameters were measured three times and mean values were
obtained.
Statistical analysis
Data were analyzed using SPSS version 11.5 (SPSS,
Inc., Chicago, IL, USA) and are expressed as mean ± SD. A Student’s
t-test was used to compare the mean values between the two groups.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Fig. 1 shows the
‘s’, ‘e’ and ‘a’ movement waves of the tricuspid annulus in a
patient with AIDS. Compared with the values in the control group,
the Vs and Va of the AIDS group decreased in all sites with the
exception of the lateral wall and the Ve decreased in all sites of
the tricuspid annulus (P<0.05). The mean values of Vs, Ve and Va
at the four sites of the tricuspid annulus showed a marked
reduction in the AIDS group (P<0.05). The Tei index increased
significantly in the patients with AIDS (P<0.05). All values are
shown in Table I. These results
show that the systole and diastole functions of the right ventricle
were decreased in the patients with HIV/AIDS, indicating that these
individuals are susceptible to right ventricular dysfunction.
 | Table IContrast between the DTI parameters of
the AIDS and control groups. |
Table I
Contrast between the DTI parameters of
the AIDS and control groups.
| Site | Parameter | AIDS | Control | P-values |
|---|
| Anterior wall | Vs (mm/sec) | 11.35±2.20 | 13.19±2.69 | <0.001a |
| Ve (mm/sec) | 12.72±3.06 | 15.44±3.20 | <0.001a |
| Va (mm/sec) | 10.95±3.68 | 13.16±3.54 | 0.001a |
| Posterior wall | Vs (mm/sec) | 11.23±2.18 | 12.21±2.50 | 0.018a |
| Ve (mm/sec) | 12.45±3.43 | 14.84±3.87 | <0.001a |
| Va (mm/sec) | 10.71±3.39 | 12.34±4.78 | 0.026a |
| Interventricular
septum | Vs (mm/sec) | 9.05±1.60 | 11.45±2.42 | <0.001a |
| Ve (mm/sec) | 10.71±1.83 | 14.85±3.62 | <0.001a |
| Va (mm/sec) | 8.26±1.88 | 10.64±3.11 | <0.001a |
| Lateral wall | Vs (mm/sec) | 14.11±2.83 | 14.14±2.64 | 0.095 |
| Ve (mm/sec) | 12.97±2.38 | 15.53±3.62 | <0.001a |
| Va (mm/sec) | 13.86±4.30 | 14.70±4.13 | 0.284 |
| Mean of four
sites | S (mm/sec) | 11.44±1.45 | 12.74±2.09 | <0.001a |
| E (mm/sec) | 12.21±1.93 | 15.17±3.05 | <0.001a |
| A (mm/sec) | 10.97±2.45 | 12.71±3.18 | 0.001a |
| Lateral wall | Tei index | 0.41±0.11 | 0.30±0.16 | <0.001a |
Discussion
Recently, the improved control of opportunistic
infection has resulted in a greater awareness of cardiovascular
complications in individuals who are HIV positive or have AIDS
(7–9). Generally, cardiac complications are
asymptomatic and may be masked by symptoms of other complications,
which leads to negative results for X-ray and ECG examinations
(10,11). This highlights the importance of
echocardiography in HIV-associated cardiac dysfunction. Studies on
cardiac dysfunction in HIV/AIDS patients frequently investigate the
left ventricle (12–15). The ultrasound results included
M-mode, pulsed Doppler or strain. DTI is a technique that may be
employed to quantitatively study right ventricular function. The
technique measures the movements of the tricuspid annulus or right
ventricle myocardia, which reflect right ventricular function. In
addition, DTI is not affected by morphology, pre-load, respiration,
valve area or regurgitant (16).
Similarly, the technique is more direct and accurate than pulsed
Doppler or the M-mode in assessing right ventricular function by
the flow of the tricuspid and pulmonary valves or by the change of
right ventricle volume. At present, there are a limited number of
studies on the determination of right ventricular function in
HIV-positive individuals using DTI (17).
The Tei index is a parameter that reflects the
systolic and diastolic function of the heart (18). The results of the present study
showed that the DTI values of the tricuspid annulus decreased,
while the Tei index increased in patients with AIDS. This indicated
that the function of the right ventricle in the AIDS patients was
damaged; however, the mechanism is not clear. Left ventricular
dysfunction in patients with HIV/AIDS may be caused by a number of
factors, including HIV infection, opportunistic infection,
autoimmunity, malnutrition, long-term immunodepression, neoplasm
and pharmaceuticals (19–23). Right ventricular dysfunction may
also be caused by the combined effect of pulmonary diseases,
including pulmonary infection and pulmonary microvascular embolism
due to embolus formation or drug injection. These diseases increase
pulmonary vascular resistance, pulmonary artery hypertension and
right ventricular dysfunction. In addition, HIV itself may play a
role in the development of right ventricular dysfunction. However,
the effects of other factors, including the pathogeny of
opportunistic infection, immunomechanisms, pharmaceutical toxicity
and neoplasms are unclear and the development of right ventricular
dysfunction may be due to multifactorial effects. The present study
demonstrated that the right ventricular function of patients with
AIDS was damaged, but the mechanism was unclear, and further study
is required.
Acknowledgements
The authors thank Dr Weixia Chen of Shangcai County
People’s Hospital, Henan for support during this study.
References
|
1
|
Lekakis J and Ikonomidis I: Cardiovascular
complications of AIDS. Curr Opin Crit Care. 16:408–412. 2010.
View Article : Google Scholar
|
|
2
|
Barbaro G and Silva EF: Cardiovascular
complications in the acquired immunodeficiency syndrome. Rev Assoc
Med Bras. 55:621–630. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Montgomery DE, Puthumana JJ, Fox JM and
Ogunyankin KO: Global longitudinal strain aids the detection of
non-obstructive coronary artery disease in the resting
echocardiogram. Eur Heart J Cardiovasc Imaging. 13:579–587. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ho JN, Yoon HG, Park CS, Kim S, Jun W,
Choue R and Lee J: Isothiocyanates ameliorate the symptom of heart
dysfunction and mortality in a murine AIDS model by inhibiting
apoptosis in the left ventricle. J Med Food. 15:781–787. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen F, Bhardwaj R and Finkel MS:
Diastolic dysfunction following HIV infection. AIDS. 26:885–886.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mondy KE, Gottdiener J, Overton ET, et al;
SUN Study Investigators. High prevalence of echocardiographic
abnormalities among HIV-infected persons in the era of highly
active antiretroviral therapy. Clin Infect Dis. 52:378–386. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fisher SD, Kanda BS, Miller TL and
Lipshultz SE: Cardiovascular disease and therapeutic drug-related
cardiovascular consequences in HIV-infected patients. Am J
Cardiovasc Drugs. 11:383–394. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ogalha C, Luz E, Sampaio E, et al: A
randomized, clinical trial to evaluate the impact of regular
physical activity on the quality of life, body morphology and
metabolic parameters of patients with AIDS in Salvador, Brazil. J
Acquir Immune Defic Syndr. 57(Suppl 3): S179–S185. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sims A and Hadigan C: Cardiovascular
complications in children with HIV infection. Curr HIV/AIDS Rep.
8:209–214. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Miller LH and Coppola JT: Noninvasive
assessment of HIV-related coronary artery disease. Curr HIV/AIDS
Rep. 8:114–121. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baker JV and Lundgren JD: Cardiovascular
implications from untreated human immunodeficiency virus infection.
Eur Heart J. 32:945–951. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lipshultz SE, Williams PL, Wilkinson JD,
et al; Pedeatric HIV/AIDS Cohort Study (PHACS). Cardiac status of
children infected with human immunodeficiency virus who are
receiving long-term combination antiretroviral therapy: results
from the Adolescent Master Protocol of the Multicenter Pediatric
HIV/AIDS Cohort Study. JAMA Pediatr. 167:520–527. 2013. View Article : Google Scholar
|
|
13
|
Bajwa AA, Cury JD, Jones L, Shujaat A and
Usman F: Echocardiographic findings and their impact on outcomes of
critically ill patients with AIDS in the era of HAART. Pulm Med.
2012:5757932012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Reinsch N, Kahlert P, Esser S, et al:
Echocardiographic findings and abnormalities in HIV-infected
patients: results from a large, prospective, multicenter HIV-heart
study. Am J Cardiovasc Dis. 1:176–184. 2011.PubMed/NCBI
|
|
15
|
Blaylock JM, Byers DK, Gibbs BT, et al:
Longitudinal assessment of cardiac diastolic function in
HIV-infected patients. Int J STD AIDS. 23:105–110. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jones DK and Leemans A: Diffusion tensor
imaging. Methods Mol Biol. 711:127–144. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rocha MO, Barbosa FB, Martins MA and do
Nunes MC: Patient with chronic Chagas heart disease, hepatosplenic
schistosomiasis and acquired immunodeficency syndrome: possible
spontaneous resolution of thrombus in the right ventricle. Rev Soc
Bras Med Trop. 45:263–265. 2012.(In Portuguese).
|
|
18
|
Tei C, Ling LH, Hodge DO, et al: New index
of combined systolic and diastolic myocardial performance: a simple
and reproducible measure of cardiac function - a study in normals
and dilated cardiomyopathy. J Cardiol. 26:357–366. 1995.PubMed/NCBI
|
|
19
|
Fedele F, Bruno N and Mancone M:
Cardiovascular risk factors and HIV disease. AIDS Rev. 13:119–129.
2011.PubMed/NCBI
|
|
20
|
Choi AI, Vittinghoff E, Deeks SG, Weekley
CC, Li Y and Shlipak MG: Cardiovascular risks associated with
abacavir and tenofovir exposure in HIV-infected persons. AIDS.
25:1289–1298. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Reinsch N, Neuhaus K, Esser S, et al;
German Competence Network Heart Failure; German Competence Network
for HIV/AIDS. Are HIV patients undertreated? Cardiovascular risk
factors in HIV: results of the HIV-HEART study. Eur J Prev Cardiol.
19:267–274. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vernon LT, Babineau DC, Demko CA, et al: A
prospective cohort study of periodotal disease measures and
cardiovascular disease markers in HIV-infected adults. AIDS Res Hum
Retroviruses. 27:1157–1166. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Farinatti PT, Borges JP, Gomes RD, Lima D
and Fleck SJ: Effects of supervised exercise program on the
physical fitness and immunological function of HIV-infected
patients. J Sports Med Phys Fitness. 50:511–518. 2010.PubMed/NCBI
|