Introduction
Eosinophilia is typically associated with allergic
reactions, parasitic infestations, certain forms of vasculitis, the
use of medication and hematologic malignancies. However,
eosinophilia in solid malignancies is rarely reported. Severe
peripheral hypereosinophilia has been reported in solid tumors
including gastrointestinal tumors (1), lung cancer (2,3), and
thyroid carcinoma (4). However,
there have been a limited number of reports describing peripheral
hypereosinophilia in urologic tumors (5,6).
Todenhöfer et al (6)
presented the first and only case of severe paraneoplastic
hypereosinophilia in a patient with renal cell carcinoma. The
present study reports three cases of eosinophilia in patients with
chromophobe renal cell carcinoma (CRCC) and investigates the
association between excessive eosinophilia and the recurrence and
prognosis of renal carcinoma.
Case reports
Patient history
Between September 2010 and September 2013, three
patients (two males and one female) were admitted to The Second
Xiangya Hospital (Changsha, China). Two patients, one male and one
female, presented with lumbago. Another male patient complained of
weight loss of 5 kg in three months. All the patients were found to
have a kidney mass according to a computed tomography (CT) scan of
the abdomen and were diagnosed with a renal tumor (Table I). One patient complained of a
weight loss of 5 kg in three months. None of the patients exhibited
hematuria or a fever. Patient medical histories were negative for
specific drug use, food allergies, parasitic infestations and
exposure to tuberculosis. Informed consent was obtained from the
patient’s families.
 | Table IGeneral information of the three
patients diagnosed with chromophobe renal cell carcinoma with
eosinophilia. |
Table I
General information of the three
patients diagnosed with chromophobe renal cell carcinoma with
eosinophilia.
| | | Tumor | Mean percentage of
eosinophils |
|---|
| | |
|
|
|---|
| Patient | Gender | Age (years) | Position | Size (cm) | TNM | Recurrence | Metastasis | Pre-surgery | Month 1 after
surgery | Months 2–12 after
surgery |
|---|
| 1 | Male | 53 | Right kidney | 7.0 | T1bN0M0 | No | No | 17.53 | 2.86 | 2.54 |
| 2 | Male | 56 | Left kidney | 6.2 | T1bN0M0 | No | No | 12.35 | 2.77 | 2.63 |
| 3 | Female | 48 | Right kidney | 7.5 | T2aN0M0 | Yes | Yes | 19.08 | 3.37 | 16.98 |
Patient examination
Physical examination revealed that each patient had
a soft and flat abdomen. No masses were located in the abdominal
region and the superficial lymph nodes were not palpable. Stools
were negative for ova and parasites. Rheumatoid immune factors
including C-reactive protein, procalcitonnin, antinuclear antibody
and anti-neutrophil cytoplasmic antibody were all negative in the
blood. Tuberculosis tests were negative. Tumor markers and alkaline
phosphatase were negative in the blood. A bone marrow biopsy was
performed and demonstrated no evidence of leukemia. The chest X-ray
demonstrated no positive signs of pulmonary and metastatic lesions.
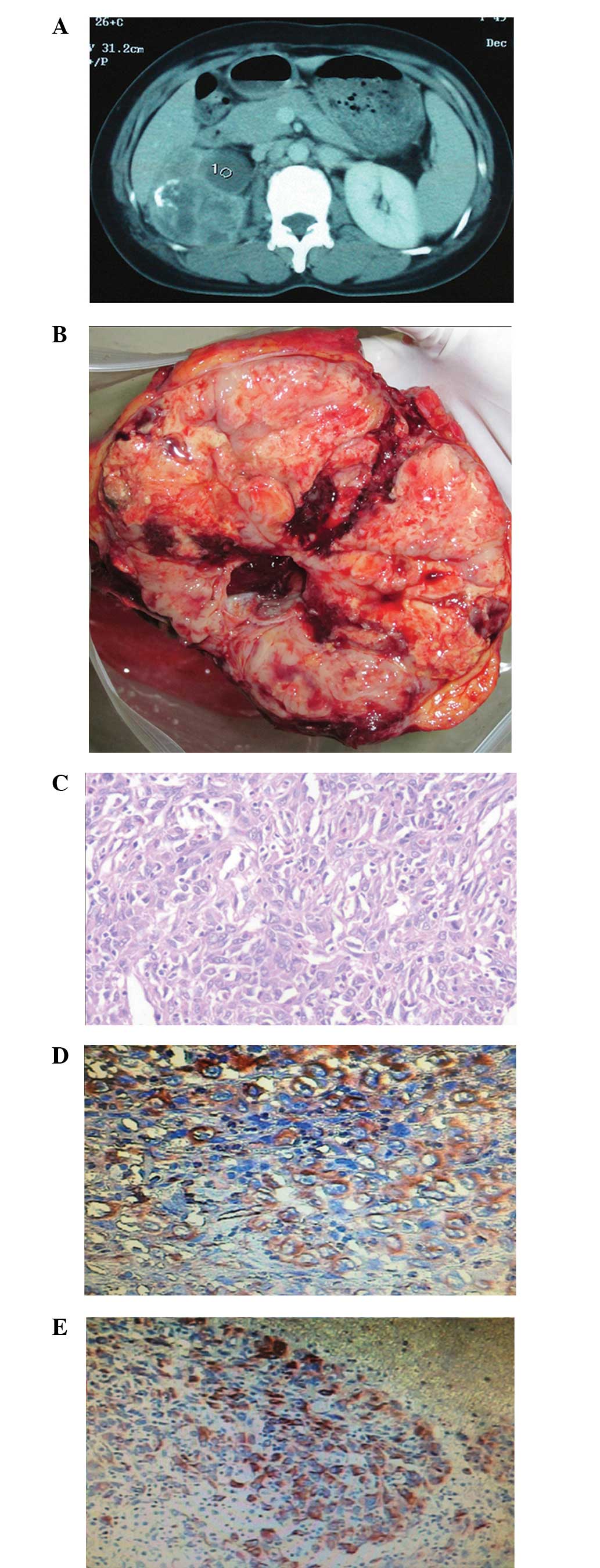
A CT scan of the abdomen and pelvis of the female patient revealed
a kidney tumor without venous tumor thrombus and distant metastasis
(Fig. 1). One retroperitoneoscopic
radical nephrectomy and two open surgeries were performed without
any complications. Swollen lymph nodes were not observed between
surgeries. Histological and pathological examinations revealed
CRCC. Eosinophilic variant CRCC with sarcomatoid components was
observed in the female patient (Fig.
1).
Outcomes
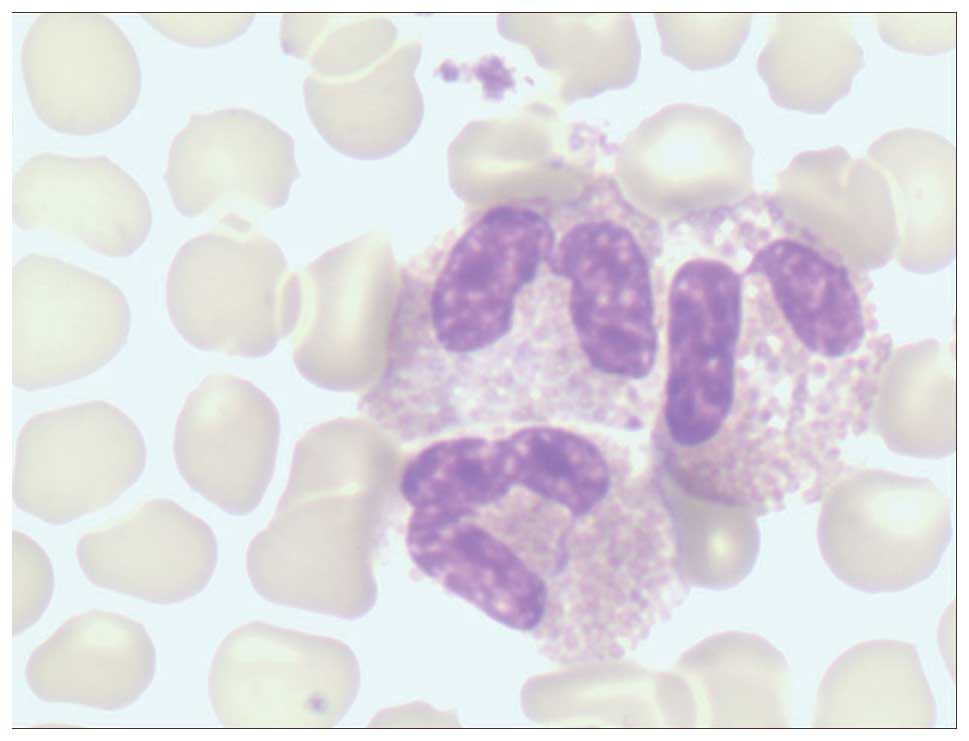
Prior to surgery, routine blood tests revealed that
all patients had persistent leukocytosis (11,360–22,230/μl, normal
range: 4,000–100,000/μl) and eosinophilia (1,120–5,060/μl, normal
range: 0–800/μl; Fig. 2). A
routine blood test was administered during the perioperative period
and at the one-year follow-up following discharge. Eosinophilia
disappeared in the first month following radical nephrectomy. The
two male patients presented with normal eosinophilic granulocytes
without tumor recurrence following surgery and at the one-year
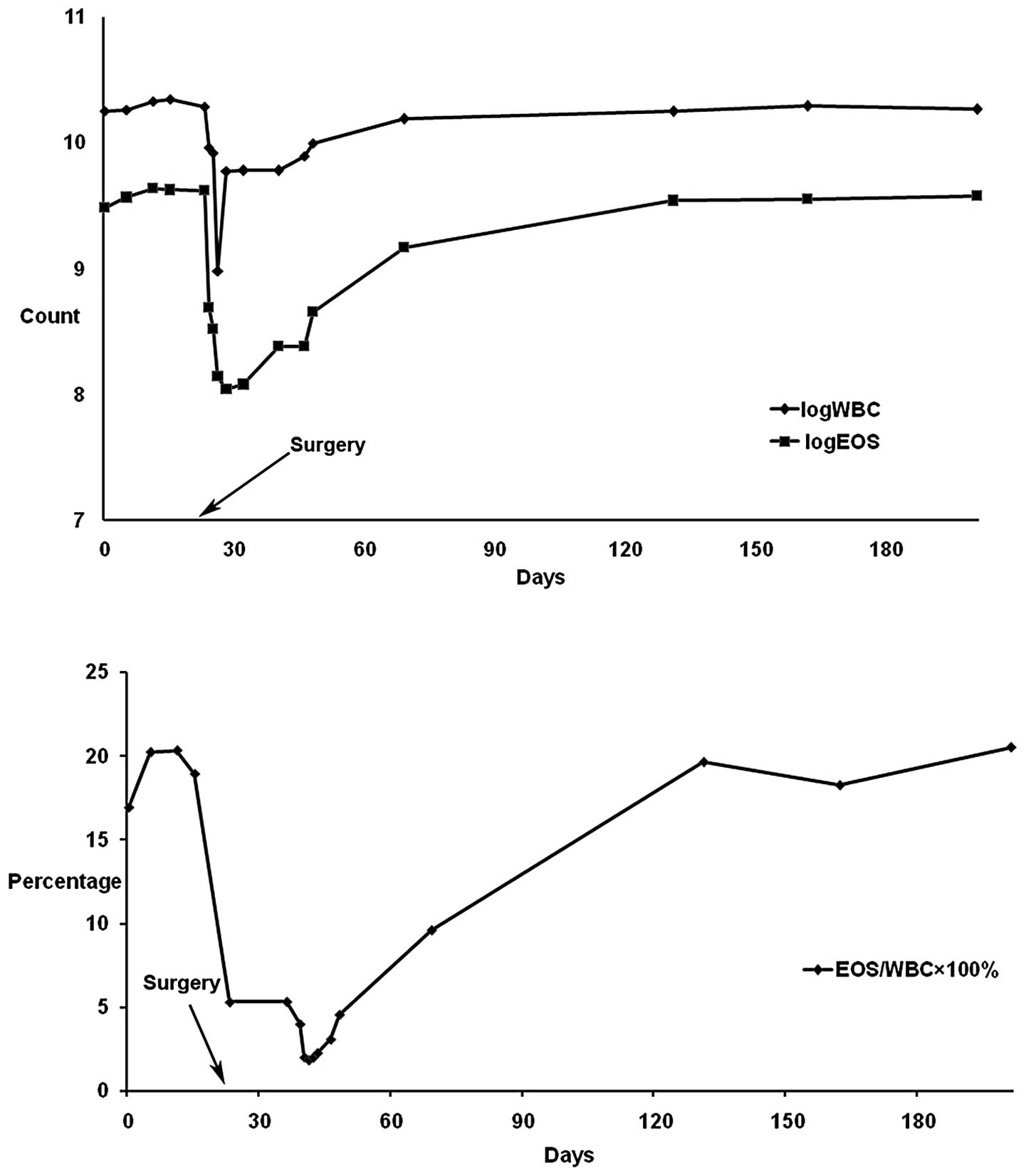
follow-up. However, blood analysis of the female patient revealed
that the leukocyte and eosinophilic granulocyte counts had
gradually increased and returned to the preoperative levels
(Fig. 3). Ultrasound examination
revealed renal carcinoma recurrence in the original renal region
involving the abdominal wall and intestine. Blood tests
demonstrated that the levels of eosinophilic granulocytes
continuously increased (19.61–20.49%, normal range: 0–5%). The
patient suffered from pain, fever and an abdominal mass. The female
patient succumbed to the disease six months following surgery due
to tumor recurrence.
Discussion
Marked peripheral eosinophilia associated with
neoplasia is rare and is observed in ~0.5% of all documented
malignancies, most frequently in hematological malignancies
(1). Peripheral eosinophilia
associated with neoplasia is more common in patients with renal
carcinoma. To the best of our knowledge, this is the first report
of CRCC associated with excessive eosinophilia. Following the
exclusion of other causes, such as infections, allergies, collagen
disease, vascular diseases and concomitant malignant hematopoietic
diseases, it was considered to be a paraneoplastic manifestation.
The majority of reports have indicated that this phenomenon is
associated with a poor prognosis and rapid disease progression
(2,6).
Eosinophilia may disappear following tumor removal
and reappear with tumor relapse or dissemination. In the three
patients in the present report, leukocytosis and eosinophilia
normalized following radical nephrectomy. However, the levels of
eosinophilic granulocytes relapsed to preoperative levels and tumor
recurrence was observed in the female patient one month following
surgery. Since no other causes of peripheral eosinophilia were
identified, the authors conclude that renal carcinoma-associated
blood eosinophilia indicated a recurrence and poor prognosis of
CRCC.
CRCC is a distinctive subtype of renal cell
carcinoma and is classified into two variants, typical and
eosinophilic, where the prognosis is more favorable for patients
with the eosinophilic rather than the typical variant (7). Clinical evidence indicates that CRCC
is one of the less aggressive types of renal cell carcinoma, but it
has been accepted that sarcomatoid changes are an unfavorable sign
histologically (8). Several
previous studies have reported the phenomenon of tumor-associated
tissue eosinophilia (TATE) at the tumor site (9,10).
TATE may occur together with or separately from tumor-associated
blood eosinophilia (TABE). The association between TATE and TABE
remains unclear. Notably, tumors with TATE alone appear to have a
better prognosis compared with those without TATE, while TABE is
associated with tumor spread and a poor prognosis (11). The causes of this difference remain
unclear and require identification. In the present study, TABE was
present but TATE was not observed at the tumor site of the
patients. Consistent with numerous reports, the female patient with
sarcomatoid changes and TABE exhibited a poor prognosis and
succumbed to tumor recurrence (2,6,13).
The pathogenesis of TABE remains unclear. Numerous
mechanisms have been postulated, including bone marrow stimulation
via circulatory factors produced by the tumor itself, tumor
necrosis as the promoter of increasing eosinophils and stimulation
of eosinophil production resulting from the seeding of metastatic
neoplastic cells to bone marrow (12). The theory of bone marrow
stimulation via circulatory factors has been acknowledged (4,14). Cytokines including interleukin-3,
interleukin-5 and granulocyte-macrophage colony-stimulating factor
produced by the primary tumor have been considered to account for
increased eosinophilic granulocytes (1,3,4,13).
Although these cytokines were not measured in the three patients,
eosinophilia was considered to be associated with the increased
cytokine levels. However, there is no single mechanism for this
phenomenon as the correlation between disseminated carcinomas,
hypereosinophilia and cytokine production is complex and
unknown.
The role of eosinophils in tumors requires further
investigation. The presence of eosinophils has been associated with
favorable prognosis in certain studies but poor prognosis in other
studies (9). The authors speculate
that the role of eosinophils associated with solid tumors may alter
with time and location. Initially, TATE is a particularly specific
reaction in certain tumors and the reactive eosinophils provide
protection against tumor cells. As the infiltration and
invasiveness of the tumor cells increase, eosinophils lose their
protective role and move to the peripheral blood. As a result,
tissue eosinophilia shifts to blood eosinophilia, indicating an
advanced stage of the neoplasm. The difference between tissue
eosinophilia and blood eosinophilia, in addition to the
hypothetical shifting process, remains unidentified. The underlying
mechanism requires validation through additional studies.
In conclusion, this is the first report of CRCC
associated with excessive eosinophilia. Eosinophilia following
tumor resection may indicate a poor patient prognosis, tumor
recurrence and rapid disease progression. The role of the
eosinophil in renal tumors and the mechanism of tumor-associated
blood eosinophilia require further elucidation.
Acknowledgements
The study was supported by the Fundamental Research
Funds for the Central Universities of Central South University in
2013 (no. 2013zzts095).
References
|
1
|
Anagnostopoulos GK, Sakorafas GH,
Kostopoulos P, et al: Disseminated colon cancer with severe
peripheral blood eosinophilia and elevated serum levels of
interleukine-2, interleukine-3, interleukine-5, and GM-CSF. J Surg
Oncol. 89:273–275. 2005. View Article : Google Scholar
|
|
2
|
El-Osta H, El-Haddad P and Nabbout N: Lung
carcinoma associated with excessive eosinophilia. J Clin Oncol.
26:3456–3457. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pandit R, Scholnik A, Wulfekuhler L and
Dimitrov N: Non-small-cell lung cancer associated with excessive
eosinophilia and secretion of interleukin-5 as a paraneoplastic
syndrome. Am J Hematol. 82:234–237. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vassilatou E, Fisfis M, Morphopoulos G, et
al: Papillary thyroid carcinoma producing granulocyte-macrophage
colony-stimulating factor is associated with neutrophilia and
eosinophilia. Hormones (Athens). 5:303–309. 2006. View Article : Google Scholar
|
|
5
|
Rojas GJ, Castro DM, Vigo-Guevara GL,
Ferrua M, Barriga-Maldonado V and Rotta-Escalante R:
Hypereosinophilic encephalopathy with multiple cerebral infarctions
in neighbouring vascular territories associated with prostate
cancer. Rev Neurol. 43:762–764. 2006.(In Spanish).
|
|
6
|
Todenhöfer T, Wirths S, von Weyhern CH, et
al: Severe paraneoplastic hypereosinophilia in metastatic renal
cell carcinoma. BMC Urol. 12:72012.PubMed/NCBI
|
|
7
|
Crotty TB, Farrow GM and Lieber MM:
Chromophobe cell renal carcinoma: clinicopathological features of
50 cases. J Urol. 154:964–967. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Onishi T, Oishi Y, Yanada S, Abe K,
Hasegawa T and Maeda S: Prognostic implications of histological
features in patients with chromophobe cell renal carcinoma. BJU
Int. 90:529–532. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pereira MC, Oliveira DT and Kowalski LP:
The role of eosinophils and eosinophil cationic protein in oral
cancer: a review. Arch Oral Biol. 56:353–358. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dorta RG, Landman G, Kowalski LP, Lauris
JR, Latorre MR and Oliveira DT: Tumour-associated tissue
eosinophilia as a prognostic factor in oral squamous cell
carcinomas. Histopathology. 41:152–157. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lowe D, Jorizzo J and Hutt MS:
Tumour-associated eosinophilia: a review. J Clin Pathol.
34:1343–1348. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lammel V, Stoeckle C, Padberg B, Zweifel
R, Kienle DL, Reinhart WH and Simon HU: Hypereosinophilia driven by
GM-CSF in large-cell carcinoma of the lung. Lung Cancer.
76:493–495. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rothenberg ME: Eosinophilia. N Engl J Med.
338:1592–1600. 1998. View Article : Google Scholar : PubMed/NCBI
|