Introduction
Malignant bone tumors are the eighth most common
type of tumor in children, accounting for 2.4% (1) of all childhood cancers. According to
a review conducted by the National Cancer Institute of America, the
age-adjusted incidence rate for all bone and joint cancers for all
ages and races is 0.9/100,000 individuals per year, and the
mortality rate is 0.4/100,000 individuals (2). Osteosarcoma and Ewing’s sarcoma are
the two most predominant malignant bone tumors in children and
adolescents (3).
Osteosarcoma is derived from primitive bone-forming
mesenchymal cells and is the most common primary bone malignancy,
accounting for 56% of bone tumors (3). The incidence rate of osteosarcoma for
all races and both genders is 4.0 (3.5–4.6 95% confidence interval)
for the age range of 0–14 years (per year, per million
individuals), and the 10–14-year-old age group has the highest
incidence of osteosarcoma, coinciding with the pubertal growth
spurt (1).
A total of 75% of malignant bone tumors in children
and adolescents occur in the distal femur, near the metaphyseal
growth plates (1). The most common
strategy for the removal of malignant metaphyseal bone tumors is
tumor resection with epiphysis preservation by preoperative physeal
distraction, transepiphyseal resection, knee arthroplasty (knee
joint resection) and amputation (4–8).
Epiphysis preservation with preoperative physeal distraction was
first described by Cañadell et al (9) in 1994, and may be performed when the
tumor has not transgressed the physis and ≥5 mm of normal bone is
preserved above the physis on the sagittal section, as determined
using magnetic resonance imaging (MRI) (10). Under these conditions, physeal
distraction allows separation of the epiphysis from the
tumor-bearing metaphysis. However, when the tumor has crossed the
physis, it is necessary to perform knee joint resection combined
with metal prosthesis transfer, known as knee arthroplasty
(11).
In the present study, the effects of metaphyseal
bone tumor removal with epiphysis preservation and knee
arthroplasty were analyzed by assessing tumor control, limb growth
capacity, range of movement of the knee and functional outcomes of
the lower limb.
Patients and methods
Patients
Between 2007 and 2012, 15 patients with malignant
metaphyseal bone tumors underwent tumor resection. Six of these
procedures involved physeal distraction and subsequent
joint-preserving tumor excision and tumor prosthesis for all
patients with knee joint reconstruction, which were transplanted
with an allograft or autograft bone. This group was termed the
physeal distraction (PD) group; patient information for the PD
group is listed in Table I. Nine
patients underwent resection of the knee joint combined with metal
prosthesis transfer and were labeled the knee arthroplasty (KA)
group (Table II). The tumor was
located in the distal femur in all 15 patients in the PD and KA
groups. The histological diagnosis was osteosarcoma in all patients
in the PD group and osteosarcoma in seven and Ewing’s sarcoma in
two patients in the KA group.
 | Table IClinical data of patients in the
physeal distraction group. |
Table I
Clinical data of patients in the
physeal distraction group.
| Patient | Age (years) | Gender | Limb with tumor | Tumor location | Distance of tumor
physeal line (mm) | Histological
diagnosis | Clinical stage | Duration of
distraction (days) |
|---|
| 1 | 12 | Male | Left | Distal femur | 10 | Osteosarcoma | IIB | 7 |
| 2 | 14 | Male | Left | Distal femur | 7 | Osteosarcoma | IIB | 4 |
| 3 | 13 | Female | Right | Distal femur | 12 | Osteosarcoma | IIB | 5 |
| 4 | 9 | Male | Left | Distal femur | 5 | Osteosarcoma | IIA | 5 |
| 5 | 11 | Male | Right | Distal femur | 10 | Osteosarcoma | IIB | 7 |
| 6 | 13 | Female | left | Distal femur | 15 | Osteosarcoma | IIB | 6 |
| Table IIClinical data of patients in the knee
arthroplasty group. |
Table II
Clinical data of patients in the knee
arthroplasty group.
| Patient | Age (years) | Gender | Limb with tumor | Tumor location | Distance of tumor
physeal line (mm) | Histological
diagnosis | Clinical stage |
|---|
| 1 | 10 | Male | Right | Distal femur | 2 | Osteosarcoma | IIB |
| 2 | 13 | Female | Left | Distal femur | 3 | Osteosarcoma | IIA |
| 3 | 12 | Male | Left | Distal femur | 3 | Ewing’s sarcoma | IIB |
| 4 | 12 | Male | Right | Distal femur | 0 | Osteosarcoma | IIB |
| 5 | 14 | Male | Right | Distal femur | 1 | Osteosarcoma | IIB |
| 6 | 11 | Female | Left | Distal femur | 3 | Ewing’s sarcoma | IIA |
| 7 | 9 | Male | Right | Distal femur | 1 | Osteosarcoma | IIB |
| 8 | 16 | Female | Left | Distal femur | 2 | Osteosarcoma | IIB |
| 9 | 12 | Male | Left | Distal femur | 3 | Osteosarcoma | IIA |
All patients were administered two cycles of
neoadjuvant chemotherapy prior to tumor resection, as per National
Comprehensive Cancer Center Network guidelines (12). The protocol included a high dose of
methotrexate (8–12 g/m2), Adriamycin (60–90
g/m2), ifosfamide (2 g/m2) and cisplatin (120
g/m2) for osteosarcomas.
Written informed consent was obtained from the
guardians on the behalf of the participants involved in this study.
The Life Sciences Institutional Review Board of Zhengzhou
University and The Ethics Committee of Henan Cancer Hospital
approved the consent procedures and this study.
Surgery
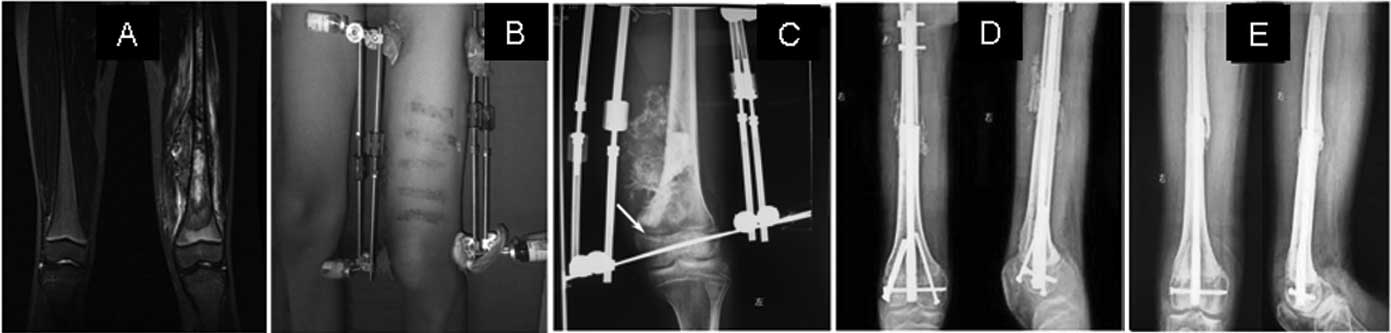
PD group
The indications for physeal distraction were as
follows: i) histological examination was used to confirm the
presence of a primary bone sarcoma; ii) the tumor was situated in
the metaphyseal region and had not metastasized to other organs;
iii) the physeal cartilage was intact; iv) the tumor had not
transgressed the physis and ≥5 mm of normal bone above the physis
was preserved on the sagittal section, as determined using MRI,
undertaken prior to treatment (Fig.
1A).
The procedure consisted of three phases. i) Physeal
distraction: Two pins were inserted into the epiphysis and another
two into the diaphysis, 8–10 cm beyond the tumor. An external
monolateral fixator with a T-shaped piece for the epiphysis pins
was attached (Fig. 1B).
Distraction was performed at a rate of 1–2 mm/day until the physis
was disconnected from the epiphysis, as determined by X-ray
examination (Fig. 1C). The mean
time over which distraction was applied was 12 days. It was
possible to carry out this phase while the patient was finishing
the course of neoadjuvant chemotherapy. ii) Epiphysis preservation
surgery: En-bloc resection was performed, leaving a wide margin,
without exposing the metaphyseal surface of the physis. The
resected tumor was immediately sent for histological examination.
iii) Prosthetic reconstruction with allograft or autograft bone
graft: Reconstruction of the bone defect was undertaken as soon as
the pathologist reported the absence of tumor at the edges of the
resected segment. A bone allograft or autograft was then inserted
(Fig. 1D and E).
If tumor cells were found at the physeal edge of the
resection, the epiphysis was excised, and the limb was
reconstructed using other means (prosthesis or knee
arthroplasty).
KA group
A total of 9 patients, in which the metaphyseal bone
tumor crossed the physis, as seen on the MRI (Fig. 2A and B) and X-ray (Fig. 2C) images, underwent resection of
the knee joint and were outfitted with a metal prosthesis (Fig. 2D and E), a procedure known as knee
arthroplasty.
Postoperative treatment
All patients were intravenously administrated
neoadjuvant chemotherapy for four to six cycles following the
surgery, depending on the patient response. Patients were allowed
to do rehabilitation exercises of active extension and flexion
following wound healing.
Follow-up
Postoperative results of all patients in the two
groups were evaluated at a follow-up appointment using knee range
of movement (ROM), the Musculoskeletal Tumor Society (MSTS)
(13) score and the Toronto
extremity salvage score (TESS) (14). In addition, tumor prognosis, length
of lower limb and complications, including delayed wound healing,
delayed bone union (>12 months with little new bone formation,
post-operatively) or non-union (>1 year without new bone
formation, post-operatively) were recorded.
Statistical analysis
Data are expressed as the mean ± the standard error
of the mean. GraphPad Software (San Diego, CA, USA) was used for
statistical analysis. Significant difference between the two groups
with one variant was determined using a Student’s t-test. P<0.05
was considered to indicate a statistically significant
difference.
Results
Duration of the follow-up time
The follow-up in the PD group was 1–5 years, with a
mean duration of 2.5 years, whilst the follow-up time in the KA
group was 1–6 years, with a mean duration time of 2.6 years. There
was no significant difference in follow-up time between the PD
group and the KA group (P>0.05).
Postoperative results
Five patients in the PD group were alive and
disease-free at the last follow-up and one patient succumbed two
years following the surgery from lung tumor metastasis. No local
tumor recurrence was found, although delayed union occurred in one
patient following surgery.
In the KA group, there was local tumor recurrence in
one patient, five months following the operation, whereupon the
lower limb with the tumor was amputated. Two patients exhibited
lung tumor metastasis six months following the surgery. One of the
two patients succumbed 27 months following the surgery; however,
the other patient was still alive with the tumor at the final
follow-up 36 months following the surgery. The metal prosthesis
became exposed outside the leg in one patient four months following
the procedure, whereupon the lower limb was amputated.
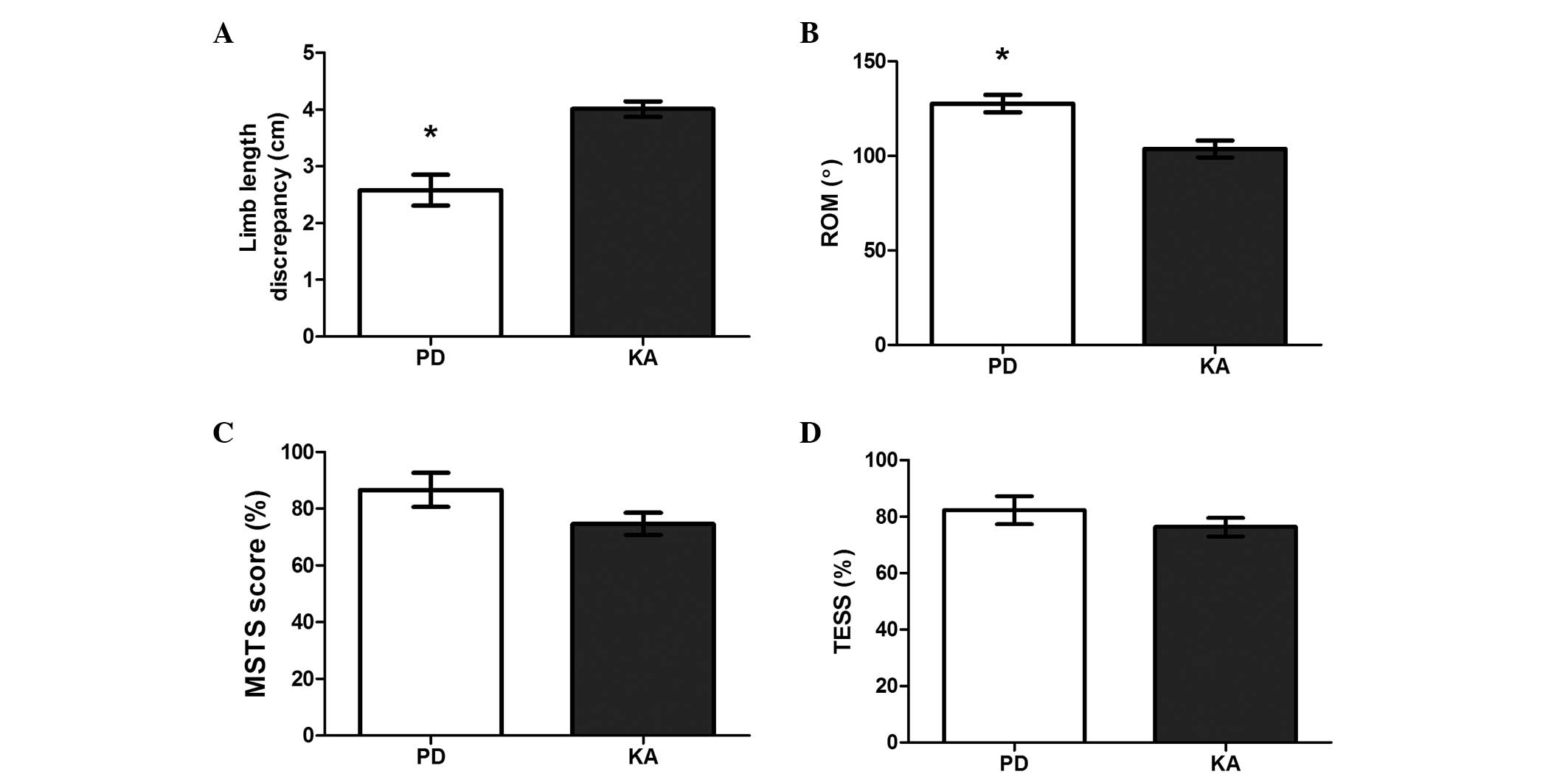
Growth capacity of the lower limb
The length of the lower limb is negatively
influenced by epiphysis when children reach adulthood. The length
discrepancy between the lower limb that received the surgery and
the other healthy lower limb in patients in the PD group was
2.58±0.27 cm, which was significantly smaller compared with the
length discrepancy of two lower limbs in patients in the KA group
(4.01±0.13 cm) (t=4.691; P=0.009; Fig.
3A).
Functional outcome of the knee
The knee ROM of the lower limb with tumor resection
in patients in the PD group was 127.70±14.63°, which showed an
increase compared with that in patients in the KA group
(105.70±15.48°) (t=3.723; P=0.020; Fig. 3B). The MSTS score and TESS results
of lower limb with tumor resection in patients in the PD group were
86.67±6.06% and 82.33±4.98%, respectively, and 74.67±4.84% and
76.33±3.82% in patients in the KA group, respectively. There was no
significant difference between the PD and KA groups with regard to
MSTS scores (t=1.671; P=0.170) or TESS (t=1.006; P=0.371) (Fig. 3C and D).
Discussion
Conservation surgery for malignant bone tumors of
the limb is becoming increasingly common due to improvements in
diagnostic imaging, the efficacy of chemotherapy and radiotherapy
and advances in the reconstruction of bone defects (15). Epiphyseal preservation surgery,
knee arthroplasty (knee joint resection) and transepiphyseal
resection are common techniques used in malignant bone tumor
conservation.
There are a number of advantages of epiphyseal
preservation in the removal of malignant bone tumors. Firstly,
epiphysis preservation with preoperative physeal distraction may
provide a safe margin of resection to prevent tumor reoccurrence.
When resecting a tumor, all the malignant tissue must be removed;
therefore, in this study, the presence of ≥5 mm of normal bone
above the physis was one of the most important indications in
determining whether or not to perform physeal distraction. If the
tumor is in contact with part of the physis, physeal distraction
may only be attempted, and intraoperative histology is recommended
(9). If tumor cells are found in
the physeal margin of the resection, transepiphyseal resection or
knee arthroplasty is the best method of surgical treatment, instead
of physeal distraction. When the tumor has crossed the physis,
resection requires the loss of the adjacent joint, and knee
arthroplasty must be performed as a conservative surgery. In this
way, safety is ensured, since all malignant tissue is excised.
However, San-Julian et al (16) reported promising results of physeal
distraction, even if the tumor was in close contact with the
physis.
In the present study, five out of six patients in
the PD group were alive and disease-free, and there was no local
tumor recurrence at last follow-up. The postoperative results
demonstrated that the safety margin produced by physeal distraction
may ensure complete resection of tumor tissue. In the KA group, the
local tumor recurred in one patient, five months following the
surgery. This may be as a result of malignant cells in the muscle
tissue or fascia around the tumor prior to the knee arthroplasty,
which is why it is necessary to make MRI images of tumors and the
adjacent tissue and carefully observe them to exclude nearby tumor
metastasis. One patient in the PD group and two patients in the KA
group were found to have lung metastases, which suggests that these
two conservation surgery techniques do not completely prevent
metastasis. It is possible that a number of malignant cells had
already migrated into the blood or lymph, which were not detected
by diagnostic methods prior to tumor resection.
Physeal distraction is safer than transepiphyseal
resection since transepiphyseal resection is more difficult to
perform on a super complex growth plate with irregular surfaces,
and may result in incomplete tumor excision (17). Physeal distraction is performed
preoperatively as the first stage of the surgery, with the
separation of the growth plate and tumor. Therefore, the tumor may
be resected completely by a diaphyseal osteotomy.
In addition, physeal distraction allows for
preservation of the epiphysis for limb lengthening in the growing
bone of children and adolescents. The epiphysis, the rounded end of
a long bone where it joins with the adjacent bone, is responsible
for bone lengthening, which is indispensable in growing children.
Progressive limb length discrepancies are likely to occur following
removal of the growth cartilage. In the present study, the leg
length discrepancy in the PD group was significantly decreased
compared with that in the KA group (Fig. 3A). This is due to the fact that
Cañadell’s technique of preoperative physeal distraction leaves
behind a widened boundary of newly formed bone, and the epiphysis
is preserved with its regenerative ability, to allow the cells of
the germinal layer to grow. Thus, this novel technique of ‘organic’
reconstruction may decrease limb length discrepancies compared with
biological reconstruction or reconstruction with metal prosthesis.
Langlois and Laville (18)
investigated limb lengthening and angular deformations in 15
patients who had undergone physeal distraction surgery, and found
that limb length discrepancy and angular deformation may be
simultaneously corrected with this novel technique. The authors
concluded that physeal distraction does not require osteotomy and
respects the vascular supply to the regenerative tissue. In the
present study, however, there was still a limb length discrepancy
of 2–3 cm in patients in the PD group, even though the discrepancy
was smaller compared with that observed with other techniques.
Previous studies have demonstrated that there is a close
association between the rate of physeal distraction and limb
lengthening. De Bastiani et al (19) compared the effects of two rates of
distraction of the epiphyseal plate and noted that, with rapid
distraction at a rate of 1 mm/day for seven days, almost complete
ossification of the cartilage was observed after 70 days. By
contrast, slow distraction was performed at 0.25 mm every 12 h (0.5
mm/day) for 28 days, whereupon the epiphyseal plate returned to a
normal thickness with normal cellular morphology after 70 days,
which meant that the epiphyseal plate was able to maintain a normal
growth rate. In addition, Pereira et al (20) distracted the proximal tibial physis
of a rabbit with a rate of distraction of 0.5 mm/day for four
weeks, and demonstrated that the proximal tibial growth plate
maintained a normal growth rate following slow physeal distraction.
In the present study, the physis was distracted at the rate of 1–2
mm/day for seven days. This suggests that rapid distraction may
damage the integrity of the growth plate or damage some cells in
the germinal layer. In future studies, the rate of distraction
should be reduced, in order to explore the implicated mechanism and
possibly prevent limb length discrepancies.
Epiphyseal preservation, as a type of limb-saving
surgery, is advantageous in terms of preserving knee function. In
the present study, the ROM of the knees of patients in the PD group
increased, compared with that in patients of the KA group (Fig. 3B), the knee joint in the epiphysis
preservation surgery was preserved, allowing the knee to flex at a
larger angle. This result is consistent with that of Fang et
al (21). Other functional
results from the present study included a mean MSTS score of 86.67%
and a mean TESS of 82.33% in patients in the PD group, which failed
to show a significant difference when compared with the scores of
patients in the KA group (Fig. 3C and
D). In accordance with the results from the present study,
previous studies have demonstrated that the functional outcomes of
epiphysis preservation surgery are similar to those of other
limb-saving techniques (22,23).
Despite these promising results, postoperative
complications remain a significant problem with this novel
technique. These complications may include delayed union or
non-union at the allograft-host junction. To solve this problem,
locked plating systems or stronger interlocking intramedullary
nails were used in the present study to improve fixation of the
allograft to the host bone. Additionally, joint contractures and
prosthetic loosening are the main complications of knee
arthroplasty; therefore, continued improvements of prostheses are
very important.
In conclusion, epiphyseal preservation surgery is an
effective limb-saving technique to treat malignant metaphyseal bone
tumors in children and adolescents when strict indications are
satisfied. The epiphyseal preservation surgery should be considered
firstly in this situation, since it results in a smaller limb
length discrepancy, larger range of movement of the knee and good
functional outcomes of lower limbs. However, when the indications
are not satisfied, knee arthroplasty should be performed as a
limb-saving surgery in order to completely remove the tumor.
Acknowledgements
The authors would like to acknowledge contributions
from colleagues.
References
|
1
|
Ottaviani G and Jaffe N: The epidemiology
of osteosarcoma. Cancer Treat Res. 152:3–13. 2009. View Article : Google Scholar
|
|
2
|
Ries LAG, Melbert D and Krapcho M: SEER
Cancer Statistics Review, 1975–2004. Bethesda, MD: National Cancer
Institute; 2006, http://seer.cancer.gov/csr/1975_2004/uri.
Accessed September 30, 2013
|
|
3
|
Gurney JG, Swensen AR and Bulterys M:
Malignant bone tumors. Cancer Incidence and Survival Among Children
and Adolescents: United States SEER Program 1975–1995 Bethesda, MD:
National Cancer Institute; 1999, http://seer.cancer.gov/publications/childhood/bone.pdfuri.
Accessed September 30, 2013
|
|
4
|
Betz M, Dumont CE, Fuchs B and Exner GU:
Physeal distraction for joint preservation in malignant metaphyseal
bone tumors in children. Clin Orthop Relat Res. 470:1749–1754.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Abudu A, Grimer R, Tillman R and Carter S:
The use of prostheses in skeletally immature patients. Orthop Clin
North Am. 37:75–84. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Campanacci L, Manfrini M, Colangeli M, Ali
N and Mercuri M: Long-term results in children with massive bone
osteoarticular allografts of the knee for high-grade osteosarcoma.
J Pediatr Orthop. 30:919–927. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Muscolo DL, Ayerza MA, Aponte-Tinao LA and
Ranalletta M: Partial epiphyseal preservation and intercalary
allograft reconstruction in high-grade metaphyseal osteosarcoma of
the knee. J Bone Joint Surg Am. 87(1 Suppl 2): 226–236. 2005.
|
|
8
|
Muscolo DL, Ayerza MA, Aponte-Tinao LA and
Ranalletta M: Use of distal femoral osteoarticular allografts in
limb salvage surgery. Surgical technique. J Bone Joint Surg Am.
88(1 Suppl 2): 305–321. 2006.PubMed/NCBI
|
|
9
|
Cañadell J, Forriol F and Cara JA: Removal
of metaphyseal bone tumours with preservation of the epiphysis.
Physeal distraction before excision. J Bone Joint Surg Br.
76:127–132. 1994.PubMed/NCBI
|
|
10
|
Weitao Y, Qiqing C, Songtao G and Jiaqiang
W: Epiphysis preserving operations for the treatment of lower limb
malignant bone tumors. Eur J Surg Oncol. 38:1165–1170. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
El-Gammal TA, El-Sayed A, Kotb MM, Saleh
WR and Ragheb YF: Knee joint reconstruction after hemiarticular
resection using pedicled patella and vascularized fibular graft.
Microsurgery. 30:603–607. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
D‘Adamo DR: Appraising the current role of
chemotherapy for the treatment of sarcoma. Semin Oncol. 38(Suppl
3): S19–S29. 2011.PubMed/NCBI
|
|
13
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 241–246.
1993.
|
|
14
|
Davis AM, Wright JG, Williams JI,
Bombardier C, Griffin A and Bell RS: Development of a measure of
physical function for patients with bone and soft tissue sarcoma.
Qual Life Res. 5:508–516. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
El Mesbahi O, Arifi S, Benbrahim Z, et al:
A rare case of locally advanced fibrosarcoma of diaphysal humerus
managed successfully with limb-sparing procedures after neoadjuvant
chemotherapy. World J Surg Oncol. 8:772010.PubMed/NCBI
|
|
16
|
San-Julian M, Aquerreta JD, Benito A and
Cañadell J: Indications for epiphyseal preservation in metaphyseal
malignant bone tumors of children: relationship between image
methods and histological findings. J Pediatr Orthop. 19:543–548.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bou Sleiman H, Ritacco LE, Aponte-Tinao L,
Muscolo DL, Nolte LP and Reyes M: Allograft selection for
transepiphyseal tumor resection around the knee using
three-dimensional surface registration. Ann Biomed Eng.
39:1720–1727. 2011.PubMed/NCBI
|
|
18
|
Langlois V and Laville JM: Physeal
distraction for limb length discrepancy and angular deformity. Rev
Chir Orthop Reparatrice Appar Mot. 91:199–207. 2005.(In
French).
|
|
19
|
De Bastiani G, Aldegheri R, Renzi Brivio L
and Trivella G: Limb lengthening by distraction of the epiphyseal
plate. A comparison of two techniques in the rabbit. J Bone Joint
Surg Br. 68:545–549. 1986.PubMed/NCBI
|
|
20
|
Pereira BP, Cavanagh SP and Pho RW:
Longitudinal growth rate following slow physeal distraction. The
proximal tibial growth plate studied in rabbits. Acta Orthop Scand.
68:262–268. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fang B, Yi C, Zhang H, et al: Combined
epiphyseal preservation and autograft bone transfer in treatment of
children osteosarcoma. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi.
27:45–49. 2013.(In Chinese).
|
|
22
|
Aksnes LH, Bauer HC, Jebsen NL, et al:
Limb-sparing surgery preserves more function than amputation: a
Scandinavian sarcoma group study of 118 patients. J Bone Joint Surg
Br. 90:786–794. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Niimi R, Matsumine A, Hamaguchi T,
Nakamura T, Uchida A and Sudo A: Prosthetic limb salvage surgery
for bone and soft tissue tumors around the knee. Oncol Rep.
28:1984–1990. 2012.PubMed/NCBI
|