Introduction
Axillary lymph node excision in breast cancer was
previously the standard optimal surgical procedure for breast
cancer. However, currently this procedure is not always essential
since the status of axillary lymph node metastasis can be predicted
by an intraoperative sentinel lymph node biopsy (SNB) (1). Despite this development, a number of
institutions in Japan perform lymph node excision for cases
demonstrated to be negative by intraoperative SNB. Thus, axillary
lymph node dissection tends to be unnecessary, particularly in a
number of patients with early stage breast cancer (2).
Axillary lymph node metastasis is a multifactorial
event, and several clinicopathological factors have been reported
as predictors of lymph node metastasis in breast cancer (3). However, since only a few methods
exist for precisely predicting the axillary lymph node metastasis
of an individual patient with breast cancer, a number of patients
may not receive appropriate treatment for such metastasis.
The development of diagnostic imaging systems has
facilitated the evaluation of axillary lymph node metastasis prior
to surgery for breast cancer (4).
Computed tomography (CT) is one of the representative modalities
that can be used to evaluate the lymph node status, and is commonly
used in hospitals due to its noninvasive and inexpensive
characteristics. However, the number of studies investigating the
clinical usefulness of CT in determining the axillary lymph node
status is limited (5).
Therefore, the aim of the present retrospective
study was to examine whether contrast CT imaging for the
preoperative evaluation of the axillary lymph node status was a
clinically useful modality.
Materials and methods
Patients
A total of 75 patients with primary breast cancer
that had undergone surgical treatment at the First Department of
Surgery of Sapporo Medical University (Sapporo, Japan) between 2009
and 2010 were recruited for the study. The clinical data from the
Medical Records Department were retrospectively obtained. Written
informed consent was required from all patients. All the patients
were Japanese females that had been pathologically diagnosed with
invasive ductal carcinoma without distant dissemination by whole
body CT and bone scintigraphy. In this department, preoperative
contrast CT is normally performed.
Data on clinical information were confirmed from the
medical records of the patients and are shown in Table I. Tumor status was classified
according to UCLA-integrated staging system classification with
tumor, node and metastasis categories (6). The expression of the estrogen
receptor or progesterone receptor was designated as positive when
positive staining was observed and a total Allred score of ≥3 was
achieved. Tumors that were immunohistochemically scored 2+ or 3+
and were fluorescence in situ hybridization-positive, were
regarded as HER2-positive (7).
Patients were classified into the following two groups: Group A
consisted of patients who had been diagnosed as negative by SNB,
while group B comprised patients who had been diagnosed as axillary
lymph node metastasis-positive.
 | Table IClinical characteristics of the 75
patients with breast cancer. |
Table I
Clinical characteristics of the 75
patients with breast cancer.
| Characteristics | Patients |
|---|
| Mean age, years
(range) |
| Total (n=75) | 56 (35–84) |
| Pre-menopause
(n=28) | 54 (32–60) |
| Post-menopause
(n=47) | 60 (40–82) |
| pTa, n (%) |
| pTis | 14 (18.7) |
| pT1 | 23 (30.6) |
| pT2 | 38 (50.7) |
| HR status, n (%) |
| ER(+), PgR(+) | 40 (53.4) |
| ER(+), PgR(−) | 19 (25.3) |
| ER(−), PgR(+) | 7 (9.3) |
| ER(−), PgR(−) | 9 (12.0) |
| HER2 status, n
(%) |
| Positive | 11 (14.7) |
| Negative | 64 (85.3) |
| pNa, n (%) |
| pN0 | 56 (74.7) |
| pN1 | 19 (25.3) |
| pN2 | 0 (0) |
| Surgery, n (%) |
|
Breast-conserving | 28 (37.3) |
| Mastectomy | 47 (62.7) |
Evaluation of axillary lymph nodes by
preoperative contrast CT
Although the axillary lymph nodes were not palpable
in any patient, enhanced whole body CT (Aquilion 64; Toshiba,
Tokyo, Japan) with contrast was preoperatively performed since this
is the standard procedure in Japan. A helical CT unit (64-slice CT
system; Light Speed VCT vision; GE Healthcare, Milwaukee, WI, USA)
was used for the evaluation of the axillary lymph nodes. The
patients were in a supine position and raised their arms during the
CT examination. CT images of the axillary lymph nodes were obtained
as 2-mm slices through the axilla. The most caudally located
enhanced lymph nodes were considered to be the sentinel lymph
nodes. Lymph node size and shape were evaluated, as well as the
Hounsfield units (HU) of the axillary lymph nodes in the CT images.
The average of the region of interest (ROI) was used to evaluate
the HU as a CT score. Lymph node shapes were classified into three
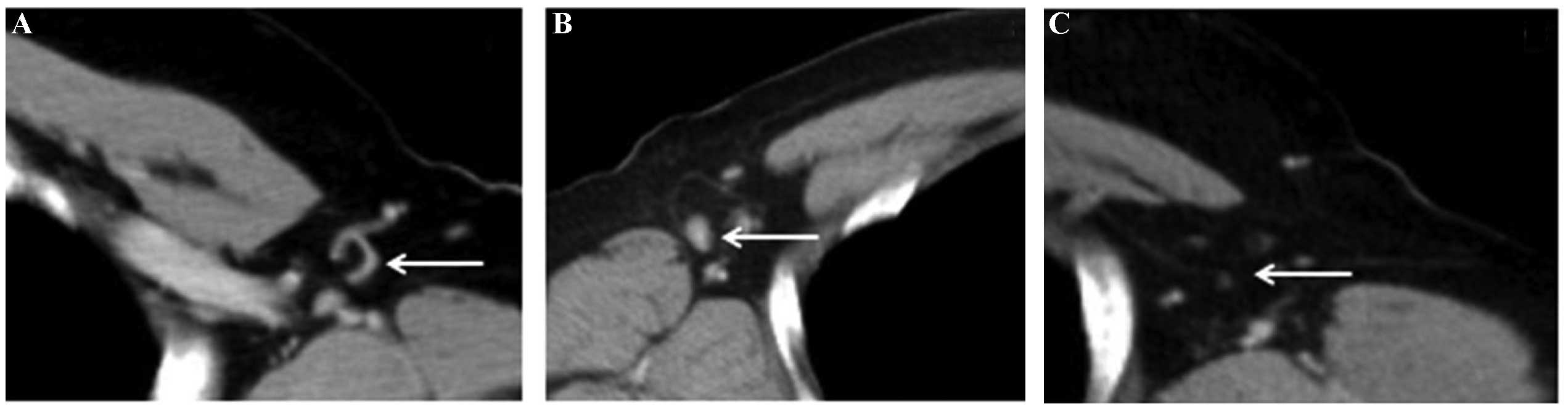
groups, according to a previous study (8). Nodes with an internal fat
concentration were classified as the fat-type (Fig. 1A), those with a size of ≥10 mm that
appeared as rounded nodes without any internal fat were classified
as the clear-type (Fig. 1B), while
the nodes with unclear borders were classified as the obscure-type
(Fig. 1C).
SNB
Prior to the initiation of surgery, 3–5 ml indigo
carmine was injected into the peritumor, as well as subcutaneous
and intradermal portions of the areola. Sentinel lymph nodes were
located following massaging the expected area for 2–3 min. All the
sentinel lymph nodes identified were sliced into 2-mm sections and
stained with hematoxylin and eosin. A surgeon conducted the SNB,
while a pathologist evaluated the specimens during the surgery.
Finally, SNB specimens were embedded in paraffin and evaluated.
Statistical analysis
Analysis of the continuous variables, including age,
tumor size, lymph node size and the CT score, was conducted with
the t-test, whereas the χ2 test was applied for the
categorical variables (Table I).
For the logistic regression analysis, odds ratios and 95%
confidence intervals (CIs) were calculated following adjustment for
age. All the statistical analyses and corresponding P-values were
two-sided, and P<0.05 was considered to indicate a statistically
significant difference. All statistical calculations were performed
using JMP version 9.0 software (SAS Institute, Cary, NC, USA).
Results
Characteristics of the patients
A total of 75 patients who had received adequate
treatment for primary breast cancer were analyzed in the study
(Table I). A mastectomy was
performed for 61% of the population.
Patients were classified into the following two
groups according to the histological diagnosis from the SNB. Group
A (n=56) patients were diagnosed as axillary lymph node
metastasis-negative by SNB, while group B (n=19) patients were
diagnosed as axillary lymph node metastasis-positive.
Difference in the distributions of the
possible predictors of axillary lymph node metastasis
Differences in the menopausal status, histological
type, tumor size, axillary lymph node size, axillary lymph node
shape in contrast CT and CT scores (the average of the ROI) were
analyzed between groups A and B (Table II). The menopausal status, tumor
size, axillary lymph node size, axillary lymph node shape and CT
score exhibited statistically significant differences when
comparing the two groups (Table
II). In addition, the ratio of the premenopausal group was
higher in group B compared with group A (P=0.034), and the primary
tumor size, axillary lymph node size and CT score (ROI) were larger
in group B compared with group A (P=0.034, P=0.0007 and
P<0.0001, respectively). Furthermore, of the 56 patients in
group A, fat-, clear- and obscure-type lymph nodes were observed in
17 (30.4%), 8 (14.3%) and 31 cases (55.3%), respectively. By
contrast, fat-, clear- and obscure-type lymph nodes were identified
in two (10.5%), 14 (73.7%) and three cases (15.8%) in group B,
respectively, indicating that there were statistically significant
differences (P<0.0001) in the distribution of the lymph node
shapes in preoperative contrast CT between the two groups (Table II).
| Table IIDifferences in the distributions of
possible predictors for positive SNB. |
Table II
Differences in the distributions of
possible predictors for positive SNB.
| Characteristics | Group A (n=56) | Group B (n=19) | P-value |
|---|
| Menopause (pre/post),
n | 17/39 | 11/08 | 0.034 |
| Tumor sizeb, cm | 1.55±0.15 | 2.19±0.26 | 0.034 |
| Axillary lymph node
sizeb, cm | 0.56±0.05 | 0.92±0.09 | 0.0007 |
| Axillary lymph node
shape in contrast CT (fat/clear/obscure), n | 17/08/31 | 2/14/3 | <0.0001 |
| CT score
(ROI)a,b | 0.16±21.6 | 31.4±31.9 | <0.0001 |
Identification of the predictors for
axillary lymph node metastasis
To identify the risk factors for axillary lymph node
metastasis, logistic regression analysis of the menopausal status,
tumor size, axillary lymph node size, axillary lymph node shape and
CT score was conducted since the aforementioned predictors
significantly differed between the groups (Table III). In univariate analysis, the
menopausal status, axillary lymph node size, obscure-type lymph
nodes, clear-type lymph nodes and the CT score were demonstrated to
be predictors of lymph node metastasis (P=0.036, P=0.01, P=0.006,
P<0.001 and P=0.013, respectively, with 95% CIs of 0.11–0.93,
0.0062–0.64, 0.04–0.58, 4.7–60 and 0.15–6.0, respectively). In
addition, with regard to the multivariate analysis, clear-type
axillary lymph nodes were shown to be significantly associated with
axillary lymph node metastasis following adjustment for the
menopausal status, axillary lymph node size, obscure-type lymph
nodes and the CT score (P=0.003; 95% CI, 2.5–89; Table III), indicating that the axillary
lymph node shape in preoperative contrast CT imaging was an
independent indicator of axillary lymph node metastasis
(SNB-positive).
| Table IIIUnivariate and multivariate analyses
of the predictors of SNB. |
Table III
Univariate and multivariate analyses
of the predictors of SNB.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Predictors | Odds ratio | 95% CI | P-value | Odds ratio | 95% CI | P-value |
|---|
| Tumor size (≥2 cm,
<2 cm) | 0.84 | 0.29–2.39 | 0.74 | 0.45 | 0.10–1.8 | 0.26 |
| Lymph node size
(≥0.5, <0.5) | 0.12 | 0.0062–0.64 | 0.01 | 0.16 | 0.0071–1.6 | 0.12 |
| Shape |
| Obscure | 0.15 | 0.040–0.58 | 0.006 | 0.30 | 0.056–1.6 | 0.15 |
| Clear | 17 | 4.7–60 | <0.001 | 15 | 2.5–89 | 0.003 |
| Fat | 0.27 | 0.56–1.3 | 0.102 | 0.16 | 0.025–1.1 | 0.06 |
| CT score (ROIa; ≥0, <0) | 0.22 | 0.047–0.74 | 0.013 | 0.95 | 0.15–6.0 | 0.95 |
Discussion
Lymph node metastasis is an important factor that
affects the prognosis and management of patients with breast cancer
(9). Although the axillary lymph
nodes should be dissected for patients who are considered to be
axillary lymph node-positive, lymph node dissection often causes
complications, including arm edema, motor disturbance of the arm
and axillary numbness (10–12).
Therefore, axillary lymph node dissection should be performed only
following consideration of whether the procedure is essential in
each patient with breast cancer. In the present study, to identify
preoperative predictors for axillary lymph node metastasis, the
association of possible predictors and preoperative contrast CT
observations were investigated with axillary lymph node metastasis.
Axillary lymph node shape in preoperative contrast CT imaging was
found to be an independent predictor of metastasis. As shown in
Table III, multivariate analysis
indicated that clear-type axillary lymph nodes in contrast CT were
likely to be a predictor of metastasis (odds ratio, 15; P=0.003;
95% CI, 2.5–89). Although soybean-shaped lymph nodes have been
reported to be significantly metastatic and ‘C’-shaped and
ring-like lymph nodes are more likely to be nonmetastatic in
contrast-enhanced CT imaging (8),
the clear- and fat-type lymph nodes defined in the present study
were demonstrated to correspond to the former and latter,
respectively. The pathological association between the lymph node
shape in contrast CT and the localization of cancer cells in lymph
nodes has not yet been established. Thus, further
clinicopathological investigations may clarify how the localization
of cancer cells in lymph nodes influences their imaging or shape in
contrast CT.
Tumor size has been reported to be one of the main
predictors of axillary lymph node metastasis in several studies
(13–16). Although statistically significant
differences were observed in the distribution of tumor size between
groups A and B (Table II), tumor
size was not found to be an independent predictor for axillary
lymph node metastasis in the present study (Table III). However, future studies with
larger sample sizes are required to validate the association
between tumor size and lymph node metastasis, since 50% of the
tumors in the present study were small (<20 mm). SNB has become
a standard procedure, and preoperative evaluation of the axillary
lymph nodes based on imaging modalities is considered to be
important for selecting appropriate breast cancer treatment
(16,17). Several diagnostic imaging
modalities have been used for the preoperative diagnosis of the
sentinel lymph node status. Ultrasonography, magnetic resonance
imaging and multidetector CT have been reported to be useful
imaging systems to preoperatively evaluate the lymph node status
(18–20).
Lymph node size was also shown to be associated with
lymph node metastasis through univariate analysis; however, lymph
node size is unlikely to be an independent predictor according to
the results from the multivariate analysis (Table III). In the present study,
univariate analysis demonstrated that the CT score (ROI) was a
predictor of lymph node metastasis, indicating that high contrast
lymph nodes on CT images, which may be a consequence of vessel
development in the lymph nodes, may be associated with metastasis
(Table III). These observations
indicate that the evaluation of the lymph node status by
preoperative contrast CT may support the intraoperative diagnosis
by SNB.
In Japan, CT examinations are indispensable for the
preoperative metastatic search, and are conducted in all
institutions. CT is also considered to be very important for
preoperative sentinel lymph node examination. The results of the
present study indicate that preoperative CT examinations are useful
in predicting axillary lymph node metastasis, and can provide
supportive information for intraoperative sentinel lymph node
diagnosis. Although further large-scale studies are required to
validate these results, the observations of the present study
provide useful information for identifying predictors of axillary
lymph node metastasis, and may aid surgeons to determine
appropriate surgical strategies for individual patients with breast
cancer.
Acknowledgements
The study was supported by a grant from the Yuasa
Memorial Foundation. The authors thank all the study
participants.
References
|
1
|
Krag DN, Anderson SJ, Julian TB, Brown AM,
Harlow SP, Costantino JP, et al: Sentinel-lymph-node resection
compared with conventional axillary-lymph-node dissection in
clinically node-negative patients with breast cancer: overall
survival findings from the NSABP B-32 randomised phase 3 trial.
Lancet Oncol. 11:927–933. 2010. View Article : Google Scholar
|
|
2
|
Macaskill EJ, Dewar S, Purdie CA, Brauer
K, Baker L and Brown DC: Sentinel node biopsy in breast cancer has
a greater node positivity rate than axillary node sample: results
from a retrospective analysis. Eur J Surg Oncol. 38:662–669. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Callejo IP, Brito JA, Bivar JW, Fernandes
FJ, Faria JL, André MS, et al: Predictors of positive axillary
lymph nodes in breast cancer patients with metastatic sentinel
lymph node. Clin Transl Oncol. 7:18–22. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Garami Z, Hascsi Z, Varga J, Dinya T,
Tanyi M, Garai I, et al: The value of 18-FDG PET/CT in early-stage
breast cancer compared to traditional diagnostic modalities with an
emphasis on changes in disease stage designation and treatment
plan. Eur J Surg Oncol. 38:31–37. 2012. View Article : Google Scholar
|
|
5
|
Shien T, Akashi-Tanaka S, Yoshida M, Hojo
T, Iwamoto E, Miyakawa K and Kinoshita T: Evaluation of axillary
status in patients with breast cancer using thin-section CT. Int J
Clin Oncol. 13:314–319. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
International Union Against Cancer. Sobin
LH and Wittekind C: TNM Classification of Malignant Tumours. 6th
edition. Wiley-Liss; New York, NY: 2002
|
|
7
|
Jacobs TW, Gown AM, Yaziji H, Barnes MJ
and Schnitt SJ: Specificity of HercepTest in determining HER-2/neu
status of breast cancers using the United States Food and Drug
Administration-approved scoring system. J Clin Oncol. 17:1983–1987.
1999.
|
|
8
|
Nasu Y, Shikishima H, Miyasaka Y, Nakakubo
Y, Ichinokawa K and Kaneko T: A study of the assessment of axillary
lymph nodes before surgery for breast cancer using
multidetector-row computed tomography. Surg Today. 40:1023–1026.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fisher B, Wolmark N, Bauer M, Redmond C
and Gebhardt M: The accuracy of clinical nodal staging and of
limited axillary dissection as a determinant of histologic nodal
status in carcinoma of the breast. Surg Gynecol Obstet.
152:765–772. 1981.PubMed/NCBI
|
|
10
|
No authors listed. NIH consensus
conference: Treatment of early-stage breast cancer. JAMA.
265:391–395. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Assa J: The intercostobrachial nerve in
radical mastectomy. J Surg Oncol. 6:123–126. 1974. View Article : Google Scholar
|
|
12
|
Kissin MW, Querci della Rovere G, Easton D
and Westbury G: Risk of lymphoedema following the treatment of
breast cancer. Br J Surg. 73:580–584. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Patani NR, Dwek MV and Douek M: Predictors
of axillary lymph node metastasis in breast cancer: a systematic
review. Eur J Surg Oncol. 33:409–419. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Murakami S: Examination of axillary lymph
node metastasis using the multi-detector row CT in breast cancer.
Nihon Gazō Igaku Zasshi. 22:9–20. 2003.(In Japanese).
|
|
15
|
Hata Y, Ogawa Y, Nishioka A, Inomata T and
Yoshida S: Thin section computed tomography in the prone position
for detection of axillary lymph node metastases in breast cancer.
Oncol Rep. 5:1403–1406. 1998.PubMed/NCBI
|
|
16
|
Schwartz GF, Giuliano AE and Veronesi U;
Consensus Conference Committee. Proceedings of the consensus
conference on the role of sentinel lymph node biopsy in carcinoma
of the breast, April 19–22, 2001, Philadelphia, Pennsylvania.
Cancer. 94:2542–2551. 2002.
|
|
17
|
Lyman GH, Giuliano AE, Somerfield MR,
Benson AB 3rd, Bodurka DC, Burstein HJ, et al; American Society of
Clinical Oncology. American Society of Clinical Oncology guideline
recommendations for sentinel lymph node biopsy in early-stage
breast cancer. J Clin Oncol. 23:7703–7720. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ogasawara Y, Doihara H, Shiraiwa M and
Ishihara S: Multidetector-row computed tomography for the
preoperative evaluation of axillary nodal status in patients with
breast cancer. Surg Today. 38:104–8. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yoshimura G, Sakurai T, Oura S, Suzuma T,
Tamaki T, Umemura T, et al: Evaluation of axillary lymph node
status in breast cancer with MRI. Breast Cancer. 6:249–258. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang WT, Ahuja A, Tang A, Suen M, King W
and Metreweli C: High resolution sonographic detection of axillary
lymph node metastases in breast cancer. J Ultrasound Med.
15:241–246. 1996.PubMed/NCBI
|