Introduction
Bipolar disorder (BD) is a chronic and disabling
psychiatric disorder, with patients spending up to half of their
time in a state of depression (1,2).
Thus, pharmacological approaches in BD have focused primarily on
the treatment of bipolar depressive episodes. Despite recent
advances, only a few agents have proven efficacy in treating
bipolar depression, with a wide range of controversial options
being tested. Lithium is a primary agent for the treatment of BD in
multiple phases worldwide (3).
Furthermore, lithium has significant neuroprotective effects
(3) and may also, at low doses,
decrease the risk of dementia in BD (4).
Current guidelines recommend the use of lithium as a
treatment for acute bipolar depression (5,6).
Data from the European drug surveillance program reveal that
lithium is the most commonly prescribed agent for bipolar
depression in combined therapy (33%) (5). Early studies suggested that blood
lithium levels >0.8 mEq/l are necessary in maintenance therapy
for BD (7). More recently, it was
observed that lower plasma lithium levels (0.4–0.6 mEq/l) were
associated with higher relapse rates in maintenance therapy
(8). However, a recent large
study, involving a 24-week follow-up, revealed no association
between an improvement in depression or mania ratings in patients
with BD and their blood lithium levels [low (<0.4 mEq/l) vs.
high (0.4–0.9 mEq/l)] (9).
Furthermore, a reanalysis of the study by Gelenberg et al
(7) demonstrated that patients
treated with low levels of lithium during the pre- and
post-randomization phases remained stable during the study period
(10). These results may encourage
a more limited use of higher lithium doses, even in acute mood
episodes in BD.
Furthermore, studies investigating the use of
lithium in BD treatment have revealed high drop-out rates and
morbidity due to side-effects (11) In these studies, the minimum lithium
levels were 0.5–0.6 mEq/l (12–14),
with drop-out rates reaching 61% (13). In the current six-week, open-label,
proof-of-concept study, the efficacy and tolerability of lithium
monotherapy with flexible doses in bipolar disorder I (BDI) and II
(BDII) depressive episodes were evaluated.
Materials and methods
Study design
In the present study, individuals were required to
have a DSM-IV-TR diagnosis of BDI or BDII in a current depressive
episode, according to the structured clinical interview for DSM-IV
axis I disorders (SCID-I) (15).
Patients began the lithium treatment on a dose of 450 mg/day and
subsequent dosage adjustments were permitted in a flexible manner
to a dose of ≤900 mg/day, based on the clinical efficacy
(response/remission rate) of individual patients and the level of
lithium in their plasma. Measurements for the plasma lithium levels
were obtained on days 7 and 14, and at the endpoint. Short-term use
of benzodiazepines/hypnotics for a maximum of five consecutive days
(once per day) was permitted during the follow-up period. Subjects
with BDII had not taken any psychopharmacological treatment for at
least six weeks prior to the study while subjects with BDI may have
been treated with a maximum of one mood stabilizer or one
antipsychotic agent. All patients had not been previously treated
with lithium. Lithium was obtained from Eurofarma (São Paulo,
Brazil). The current study was a single center study conducted at
the Institute of Psychiatry of the University of São Paulo (São
Paulo, Brazil), clinical trial number NCT01919892.
Subjects and outcome measures
Male and female outpatients, aged between 18–45
years were eligible to participate in the study. All subjects were
recruited and followed up at the Mood Disorders Program, Laboratory
of Neuroscience LIM27, Institute of Psychiatry of the University of
São Paulo (São Paulo, Brazil) between August 2010 and June 2012.
Clinical assessments included: the score for the 21-item Hamilton
Rating Scale for Depression (HAM-D) as the primary outcome, and the
Young Mania Rating Scale (YMRS) and the Clinical Global Impression
(CGI) scale scores as secondary outcomes. A HAM-D score of ≥18 was
also required for inclusion. All adverse effects were recorded
using the Udvalg for Kliniske Undersogelse (UKU) side-effects
rating scale. Early improvement was defined as ≥20% improvement
from the baseline HAM-D score following one week of lithium
treatment. The response rate was defined as a reduction of ≥50% in
the HAM-D score at endpoint and the remission rate was
characterized as a HAM-D score of <8 at endpoint. There was no
run-in period. At the onset of the study, all subjects had <3
mood episodes in their lifetime and an illness duration of ≤5
years. Exclusion criteria included: rapid cycling in the past 12
months, previous head trauma, a current Axis I psychiatric disorder
other than BD, subjects submitted to electroconvulsive therapy,
significantly abnormal laboratory test results and any chronic
medical condition. The diagnosis was determined by experienced
psychiatrists who held an inter-rater reliability score of >0.9
for HAM-D and YMRS. The first assessment was carried out at
baseline [visit (V)1] and subsequent visits for clinical
assessment, dose adjustment and monitoring of the levels of lithium
were performed at the end of weeks 1 (V2), 2 (V3), 4 (V4) and 6
(V5). The present study was approved by the local institutional
ethics committee of the Clinics Hospital (São Paulo, Brazil) and
all patients provided written consent prior to participation in the
study.
Statistical analyses
The primary outcome was the degree of change in
depressive symptoms (HAM-D scores) analyzed using mixed-effects
random regression. The mixed-effects regression was used to analyze
changes in HAM-D assessments over the 6 weeks of follow-up and
their association with time and clinical variables that were
potentially associated with response to lithium treatment
including: age, gender, duration of illness, history of psychosis,
BD subtype and plasma lithium levels at week 6. Inter-group
comparisons of continuous variables with a Gaussian distribution
were performed using the Student’s t-test. The analyses of
continuous variables with a non-parametric distribution were
conducted using the Mann-Whitney U Test (the Kolmogorov-Smirnov
test was used to verify the normality of the data within each study
group). The chi-square test was used for the comparison of
categorical factors. The Pearson coefficient was used to evaluate
the correlation between the relative change in HAM-D scores over
time and other demographic and clinical variables. Statistical
significance was set at P<0.05 (two-tailed) and data are
presented as means ± standard deviations. All statistical analyses
were carried out using SPSS software, version 16.0 (SPSS, Inc.,
Chicago, IL, USA).
Results
Patient characteristics
A total of 42 patients were accessed for eligibility
to participate in the current study following a telephone screening
at the Mood Disorders Program, LIM27, University of São Paulo. Of
these, 31 patients were included in the present study. Two
drop-outs were observed: one patient left due to personal problems
unrelated to the study and the other patient was excluded due to
noncompliance to the treatment (undetectable blood lithium levels).
Thus, the final sample at endpoint comprised of 29 acutely
depressed bipolar patients.
Table I summarizes
the clinical and demographic data for the subgroups of patients
with BDI and BDII. The final study group comprised 21 females
(72.4%). The patients had a mean age of 28.4±5.4 years and a
diagnosis of BDI (n=11; 37.9%) or BDII (n=18; 62.1%). At baseline,
the patients had a mean duration of illness of 36.1±19.6 months and
presented mean HAM-D and YMRS scores of 22.5±3.5 and 6.1±5.6,
respectively. Out of the 29 patients that completed the current
study, 21 were naïve to lithium treatment (72.4%) and 25 (86.2%)
had been medication-free for at least six weeks prior to
participating in the study. Three of the patients had YMRS scores
>8. Furthermore, only four (13.8%) patients had a previous
history of psychotic symptoms.
 | Table IDemographic and clinical information
of subjects with bipolar I and II disorders. |
Table I
Demographic and clinical information
of subjects with bipolar I and II disorders.
| Characteristics | Bipolar I (n=11) | Bipolar II
(n=18) | P-value |
|---|
| Age (years) | 29.1±6.3 | 27.9±5. | 0.592 |
| Female gender | 9 (81.8) | 12 (66.7) | 0.376 |
| Duration of illness
(months) | 43.3±20.3 | 31.6±18.3 | 0.121 |
| History of
psychosis | 4 (36.4) | 0 (0%) | 0.006 |
| Naïve to treatment at
week 0 | 6 (54.5) | 15 (83.3) | 0.092 |
| Medication-free at
week 0 | 8 (72.7) | 17 (94.4) | 0.100 |
| HAM-D score at
baseline | 22.2±4.5 | 22.8±2.9 | 0.669 |
| Ham-D score at week
6 | 7.5±5.7 | 7.1±6.1 | 0.852 |
| YMRS score at
baseline | 6.4±6.3 | 5.9±5.3 | 0.982 |
| YMRS score at week
6 | 5.2±13.2 | 2.9±4.0 | 0.912 |
| Response rate at week
6 | 8 (72.7) | 17 (94.4) | 0.100 |
| Remission rate at
week 6 | 7 (63.6) | 11 (61.1) | 0.892 |
| Levels of lithium at
week 6 (mmol/l) | 0.51±0.21 | 0.48±0.19 | 0.729 |
The 29 patients who completed the study were
followed-up with lithium monotherapy (n=25) or lithium therapy
associated with another mood stabilizer or antipsychotics (n=4).
The mean plasma level of lithium at V5 was 0.49±0.20 mEq/l.
Clinical assessment scores
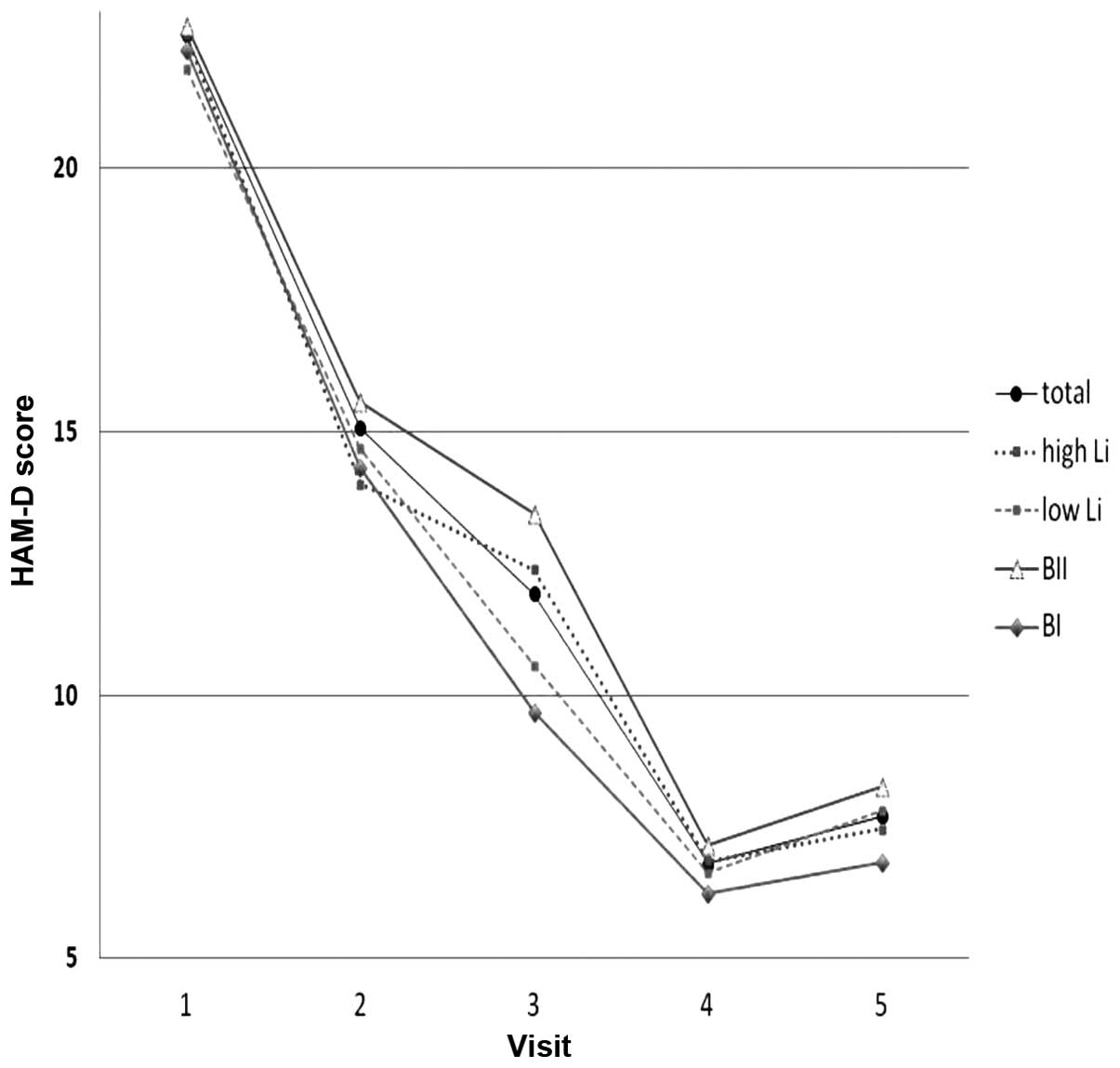
A significant reduction in HAM-D scores was observed
over the six weeks of follow-up in the whole group of BD patients
(P<0.001). Following six weeks of lithium treatment, the
response and remission rates in the total study population were
86.2% and 62.0%, respectively. The mean HAM-D and YMRS scores
following six weeks of lithium treatment were 7.3±5.9 and 3.8±8.6,
respectively. When comparing BDI and BDII, similar remission rates
were observed at endpoint; 63.6 vs. 61.1%, respectively (Fig. 1). The CGI scores, which were
4.21±0.55 pretreatment, were significantly decreased at endpoint
(2.14±0.99; P<0.001) with no significant difference identified
between the patients with BI and those with BII (P=0.86). None of
the patients experienced a switch to (hypo)mania during the
follow-up period.
Plasma lithium levels
At week 6, 15 patients had lower (Li<0.5 mEq/l)
and 14 presented higher (Li≥0.5 mEq/l) plasma lithium levels. The
plasma lithium levels did not differentially impact the number of
patients who responded (n=13 responders with lower levels vs. n=12
responders with higher levels; P=0.94). Furthermore, the use of
hypnotics (n=7), if necessary, was not observed to influence the
clinical outcome (HAM-D scores; P=0.37). No other significant
association was observed in the mixed-effects regression. No
significant differences were observed in patients in remission
(n=18) vs. those not in remission (n=11) at endpoint (a HAM-D score
<8) with regard to oral dosage, blood lithium levels, gender and
bipolar disorder subtype (data not shown). No association was
observed between HAM-D scores and lithium dose (P=0.99) or blood
levels (P=0.87) at endpoint.
Response rate and side-effects of lithium
treatment
With regard to the potential predictors of response
rate, only a previous history of psychosis was observed to be
significantly associated with a faster reduction in HAM-D scores in
response to lithium treatment (F=3.68, P=0.008). None of the
patients experienced a switch to (hypo)mania during the follow-up
period. Baseline YMRS scores did not influence the response rate
(data not shown). Common adverse effects observed were
polydipsia/polyuria (62.1%), cognitive complaints (41.4%), nausea
(31.0%), increased oniric activity (31.0%) and sedation (31.0%). In
subjects with higher lithium levels compared with those with lower
levels, an increased prevalence of nausea (50.0 vs. 13.3%; P=0.03),
restlessness (42.9 vs. 6.7%; P=0.02) and headaches (42.9 vs. 6.7%;
P=0.02) was observed. No patient drop-outs due to side-effects
occurred during the follow-up period.
Discussion
In the present six-week, open-label, single-arm
study, lithium revealed a significant antidepressant efficacy in
short-term BD. No differences in efficacy were observed with lower
levels (<0.5 mEq/l) vs. standard levels (0.5–1.2 mEq/l) of
lithium. However, the current study population comprised
predominantly young subjects with a shorter duration of illness and
included predominantly BDII cases, which may have had an influence
on the positive clinical outcome.
The similarity in the efficacy of standard vs.
‘sub-therapeutic’ lithium levels that was observed in the BD
treatment in the present study has been indirectly addressed by
recent studies on BD (9,16). The LiTMUS study evaluated
symptomatic BD; however, unlike the current study it was solely
based on the use of lithium monotherapy (9). A study by Perlis et al did not
identify a superior efficacy of using higher lithium levels (≥0.8
mm/l) in long-term maintenance therapy (10). Furthermore, a higher prevalence of
nausea, restlessness, headaches and cognitive complaints was
identified in BD subjects with higher blood lithium levels in the
present study. Other studies have experienced potential compliance
issues with patients with higher blood lithium levels. In a study
by Amsterdam and Shults, only 37.5% of subjects under higher
lithium doses completed a 12-week trial with lithium monotherapy in
bipolar depression compared with a completion rate of 79.1% for
patients treated with antidepressant (12). Similarly, a previous study on
bipolar depression described the early termination of 61% (30 out
of 49) of patients with expected lithium levels of 0.8–1.2 Meq/l
(13). The limitations of the
current study include the lack of a placebo group, the open-label
design and the relatively small sample size.
The current study aimed to define the optimal
lithium dose for BD treatment based on the clinical responses of
patients and their tolerance of lithium. The results revealed that
lower lithium doses demonstrated similar improvements to higher
doses; however, they were associated with lower drop-out rates due
to side-effects. In the context of personalized psychiatric
treatments, it is critical to evaluate the therapeutic action of
lithium with individual regimens in order to develop more effective
and tolerable approaches to BD treatment. Further studies are
required to investigate this.
Acknowledgements
This study was sponsored by the State of São Paulo
Research Foundation (FAPESP, Brazil) grant 2009/14891–9. The
Laboratory of Neuroscience LIM27 is also supported by the
Associação Beneficente Alzira Denise Hertzog da Silva (ABADHS).
References
|
1
|
Judd LL, Akiskal HS, Schettler PJ, et al:
A prospective investigation of the natural history of the long-term
weekly symptomatic status of bipolar II disorder. Arch Gen
Psychiatry. 60:261–269. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Merikangas KR, Akiskal HS, Angst J, et al:
Lifetime and 12-month prevalence of bipolar spectrum disorder in
the National Comorbidity Survey replication. Arch Gen Psychiatry.
64:543–552. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Machado-Vieira R, Manji HK and Zarate CA
Jr: The role of lithium in the treatment of bipolar disorder:
convergent evidence for neurotrophic effects as a unifying
hypothesis. Bipolar Disord. 11(Suppl 2): 92–109. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Forlenza OV, de Paula VJ, Machado-Vieira
R, et al: Does lithium prevent Alzheimer’s disease? Drugs Aging.
29:335–342. 2012.
|
|
5
|
Haeberle A, Greil W, Russmann S and
Grohmann R: Mono- and combination drug therapies in hospitalized
patients with bipolar depression. Data from the European drug
surveillance program AMSP. BMC Psychiatry. 12:1532012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yatham LN, Kennedy SH, Parikh SV, et al:
Canadian Network for Mood and Anxiety Treatments (CANMAT) and
International Society for Bipolar Disorders (ISBD) collaborative
update of CANMAT guidelines for the management of patients with
bipolar disorder: update 2013. Bipolar Disord. 15:1–44. 2013.
View Article : Google Scholar
|
|
7
|
Gelenberg AJ, Kane JM, Keller MB, et al:
Comparison of standard and low serum levels of lithium for
maintenance treatment of bipolar disorder. N Engl J Med.
321:1489–1493. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Severus WE, Kleindienst N, Seemüller F, et
al: What is the optimal serum lithium level in the long-term
treatment of bipolar disorder - a review? Bipolar Disord.
10:231–237. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nierenberg AA, Friedman ES, Bowden CL, et
al: Lithium treatment moderate-dose use study (LiTMUS) for bipolar
disorder: a randomized comparative effectiveness trial of optimized
personalized treatment with and without lithium. Am J Psychiatry.
170:102–110. 2013. View Article : Google Scholar
|
|
10
|
Perlis RH, Sachs GS, Lafer B, et al:
Effect of abrupt change from standard to low serum levels of
lithium: a reanalysis of double-blind lithium maintenance data. Am
J Psychiatry. 159:1155–1159. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Coppen A, Abou-Saleh M, Milln P, et al:
Decreasing lithium dosage reduces morbidity and side-effects during
prophylaxis. J Affect Disord. 5:353–362. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Amsterdam JD and Shults J: Comparison of
short-term venlafaxine versus lithium monotherapy for bipolar II
major depressive episode: a randomized open-label study. J Clin
Psychopharmacol. 28:171–181. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Suppes T, Marangell LB, Bernstein IH, et
al: A single blind comparison of lithium and lamotrigine for the
treatment of bipolar II depression. J Affect Disord. 111:334–343.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Young AH, McElroy SL, Bauer M, et al: A
double-blind, placebo-controlled study of quetiapine and lithium
monotherapy in adults in the acute phase of bipolar depression
(EMBOLDEN I). J Clin Psychiatry. 71:150–162. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
First MB, Spitzer RL, Gibbon M and
Williams J: Structured Clinical Interview for DSM-IV Axis I
Disorders. Patient Edition (SCID-I/P). Biometrics Research, New
York State Psychiatry Institute; New York, NY: 1995
|
|
16
|
Nolen WA and Weisler RH: The association
of the effect of lithium in the maintenance treatment of bipolar
disorder with lithium plasma levels: a post hoc analysis of a
double-blind study comparing switching to lithium or placebo in
patients who responded to quetiapine (Trial 144). Bipolar Disord.
15:100–109. 2013. View Article : Google Scholar
|