Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE)
causes high infant mortality and long-term morbidity rates
(1–3). HIE occurs in ~1–3 per 1,000 full-term
infants and in almost 60% of premature newborns. Approximately
15–20% of affected newborns succumb within the postnatal period
(4) and an additional 25% develop
severe and permanent neuropsychological handicaps (5), including cerebral palsy, seizures,
visual impairment, mental retardation, learning disabilities and
epilepsy. Following the infiltration of circulating monocytes,
neutrophils and T-cells in neonates, cerebral ischemia initiates an
immediate innate immune response that may occur minutes following
insult. This in turn exacerbates damage to the brain with a large
accumulation of inflammatory cytokines (6–8).
However, interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α),
two inflammatory cytokines that are accumulated during cerebral
ischemia, play a protective role in the incidence of HIE (9,10).
Secreted by T cells, B cells and macrophages, IL-6 and TNF-α may be
enriched during the progression of stress (11,12).
High-sensitivity C-reactive protein (Hs-CRP), an acute-phase
protein, is secreted by the liver in response to factors released
by macrophages and fat cells. It is a sensitive marker of
inflammatory reactions, since its levels rise in response to
inflammation (13,14).
To date, several studies have revealed the
association of inflammatory cytokines with the process of HIE
(11–13); however, it remains unclear as to
whether these cytokines play a role in the progression and
prognosis of the disease. The current study analyzed the levels of
IL-6, TNF-α and Hs-CRP among the different clinical gradings of HIE
and further investigated the correlation between the changes in the
levels of these inflammatory cytokines and the clinical prognosis
of the disease.
Subjects and methods
Patients
A total of 74 patients with HIE, admitted to The
First Affiliated Hospital of Xinxiang Medical University (Weihui,
China) hospital between June 2010 and June 2013, were involved in
the current study. All patients had been previously diagnosed and
clinically graded based on encephalic computed tomography scans and
the clinical determination criteria for HIE (15) (Table
I). The control group comprised 74 healthy newborns. There were
no statistically significant differences between the HIE and
control groups in terms of gender, gestational age and weight
(P>0.05). All patients with HIE were classified by clinical
grading and comprised 31 individuals with mild, 26 with moderate
and 17 with severe HIE. There was no statistically significant
difference among the different gradings in terms of gender,
gestational age and weight (P>0.05). Furthermore, the patients
with HIE were divided into good and poor prognosis groups with 32
and 42 individuals in each group, respectively. Once again, there
was no statistically significant difference between the groups in
terms of gender, gestational age and weight (P>0.05). The
present study was conducted in accordance with the Declaration of
Helsinki and with approval from the Ethics Committee of The First
Affiliated Hospital of Xinxiang Medical University. Written
informed consent was provided by the legal guardians of all
participants.
 | Table IClinical information of the
patients. |
Table I
Clinical information of the
patients.
| Group | Cases | Gender | Gestational age,
weeks (mean±SD) | Weight, g
(mean±SD) |
|---|
|
|---|
| Male | Female |
|---|
| Control | 74 | 44 | 30 | 39.5±2.9 | 3418±524 |
| HIE | 74 | 42 | 32 | 39.6±2.7 | 3591±619 |
Treatment methods
All patients were administered narcotic,
anti-acidosis, encephalic hypotensive and antioxidant drugs.
Hyperbaric oxygen therapy was also performed daily on all
patients.
Enzyme-linked immunosorbent assay (ELISA)
and radioimmunometric assay (RIA)
The serum levels of IL-6 and TNF-α were evaluated by
ELISA using commercially-available kits (R&D Systems,
Minneapolis, MN, USA). A RIA was carried out to detect the serum
levels of Hs-CRP using a commercially-available kit (Jokoh Co.,
Ltd., Tokyo, Japan). The assays were performed following the
manufacturers’ instructions.
Statistical analysis
Computerized statistical analyses were performed
using SPSS software version 13.0 (SPSS, Inc., Chicago, IL, USA).
Data are presented as mean ± standard deviation. The variances in
the levels of the inflammatory cytokines between the controls and
patients were analyzed using the Student’s t-test. The comparisons
of these parameters among the different grading groups were
calculated using analysis of variance (ANOVA) and multiple
comparison tests. The correlation between the change in the levels
of the inflammatory cytokines and the clinical grading and
prognosis of the disease was examined by Spearman’s correlation
analysis. In all statistical analyses, a two-tailed P-value ≤0.05
was considered to indicate a statistically significant
difference.
Results
Serum concentrations of IL-6, TNF-α and
Hs-CRP
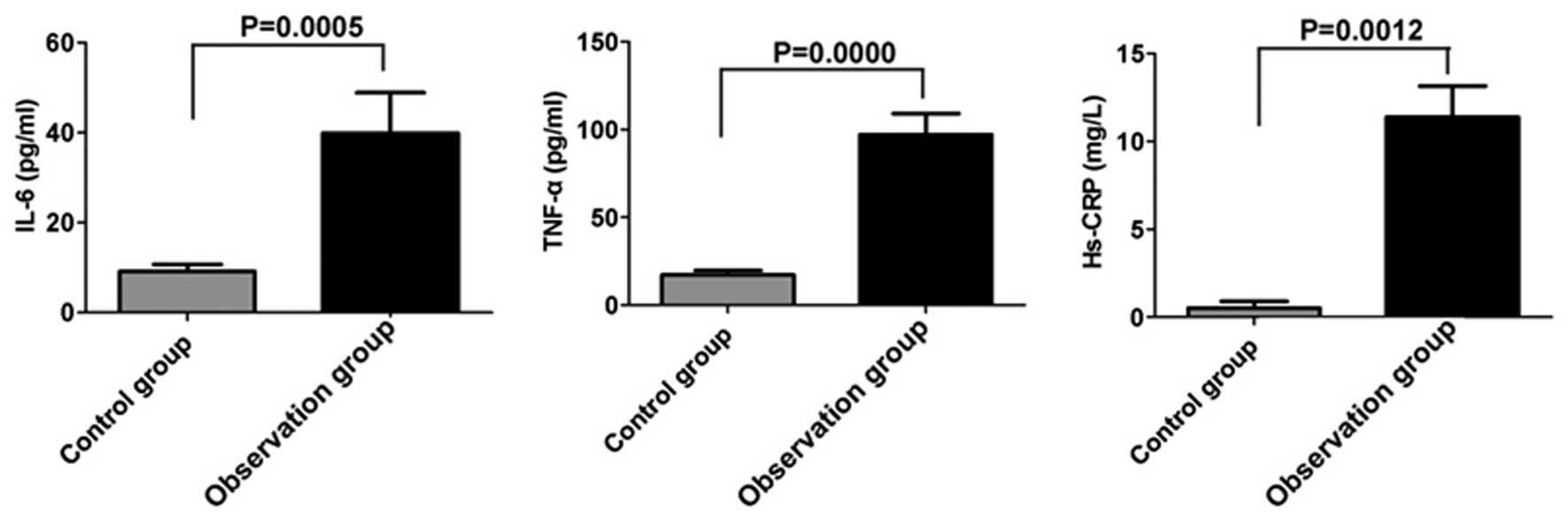
The serum levels of IL-6, TNF-α and Hs-CRP were
detected. The levels of IL-6 (39.94±4.46 pg/ml; P<0.05), TNF-α
(97.00±5.97 pg/ml; P<0.05) and Hs-CRP (11.93±1.91 mg/l;
P<0.05) were significantly higher in the patients with HIE
compared with the respective values in the control group, IL6
(9.18±1.27 pg/ml), TNF α (17.20±1.26 pg/ml) and Hs CRP (0.51±0.18
mg/l) (Fig. 1).
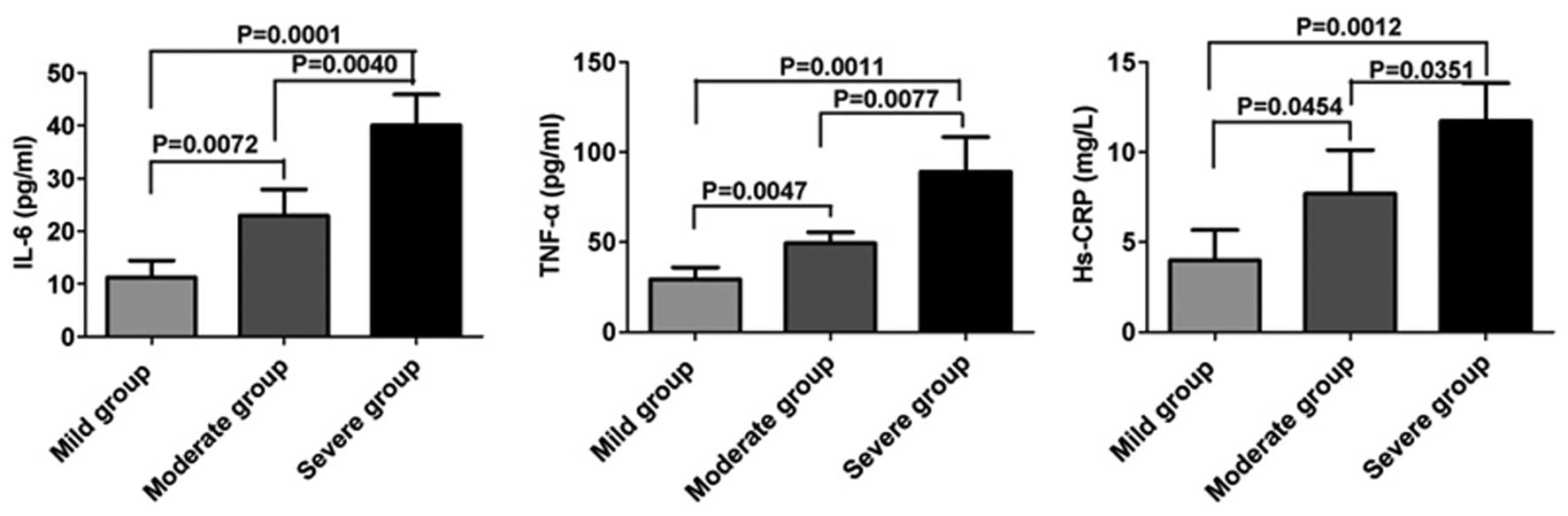
Comparison of the serum levels of IL-6,
TNF-α and Hs-CRP in patients with different clinical gradings
The present investigation revealed that the
upregulation of inflammatory cytokines was accompanied by
deterioration of the disease. As shown in Fig. 2, the levels of IL-6, TNF-α and
Hs-CRP in the moderate and severe patient groups were significantly
higher compared with those in the mild group (P<0.05).
Furthermore, there was a significant upregulation of the cytokines
in the severe group compared with those in the moderate group
(P<0.05).
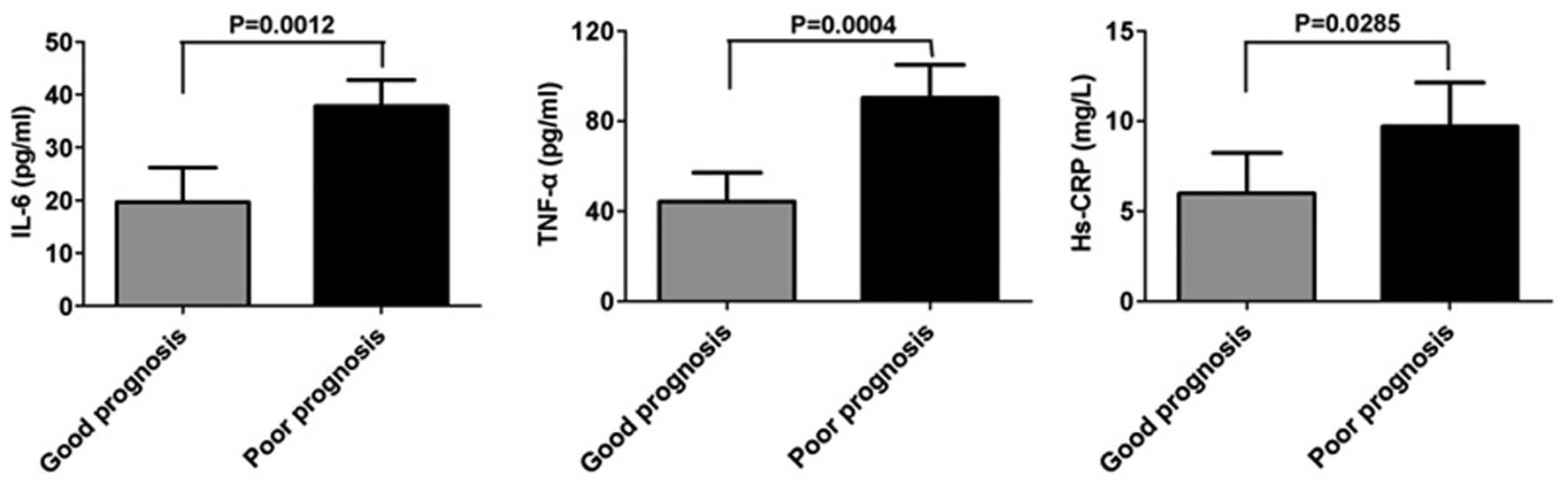
Comparison of the serum levels of IL-6,
TNF-α and Hs-CRP in patients with different prognoses
The levels of IL-6, TNF-α and Hs-CRP in patients
with either a poor or good prognosis were further analyzed.
Significant upregulation of the levels of IL-6 (37.75±4.24 pg/ml;
P<0.05), TNF-α (90.23±7.37 pg/ml; P<0.05) and Hs-CRP
(9.71±2.14 mg/l; P<0.05) were observed in patients who had a
poor prognosis compared with those in the patients who had a good
prognosis, IL 6 (19.59±2.94 pg/ml), TNF α (44.32±4.84 pg/ml) and Hs
CRP (5.99±0.99 mg/l) (Fig. 3).
Correlation between the changes in the
levels of inflammatory cytokines and the clinical grading and
prognosis of the disease
Based on the variations in the levels of IL-6, TNF-α
and Hs-CRP in patients with HIE, it is hypothesized that they may
play a role in the progression and prognosis of the disease. A
correlation analysis between these changes and the disease
progression and prognosis was carried out. Notably, positive
correlations were identified between the levels of IL-6, TNF-α and
Hs-CRP and the clinical grading (r=1.071, 0.811, 0.704,
respectively; P<0.05) and prognosis (r=1.071, 0.811, 0.704,
respectively; P<0.05) of the disease.
Discussion
HIE occurring in fetuses and neonates is a major
cause of acute mortality and chronic neurological disability in
surviving individuals (16). An
increasing number of studies have indicated that there is a
complicated correlation between HIE and the immune system (17,18).
Cytokines are activated in glial cells and astrocytes in the
central nervous system (CNS) and are released in response to brain
damage. In return, the activated cytokines regulate the activity of
the immune system. Thus, inflammatory cytokines play an important
role in brain inflammation caused by the occurrence of HIE. IL-6 is
a multifunctional immune mediator that regulates cellular immunity
and the inflammatory response. Being a pro- and anti-inflammatory
factor, IL-6 has caused controversy in studies investigating its
role in HIE in previous years. The ambiguous effects of IL-6 on the
CNS have been observed not only in animal models, but also in human
studies. The overexpression of IL-6 in animals or its increased
release in the brain has neurotoxic effects and may trigger an
inflammatory response cascade. By contrast, IL-6 deficient mice
demonstrate neuroprotective and anticonvulsive characteristics
(19,20). Furthermore, higher levels of IL-6
have been observed in infants with HIE than in normal infants and
the concentration of IL-6 has been found to be significantly
associated with the severity of HIE and the neurodevelopmental
outcome at two years of age (21).
Secreted by macrophages, TNF-α is accumulated under stress and
manipulates tissue injury. In the CNS, TNF-α is secreted by
microglia and astrocytes. Previous studies have indicated that
TNF-α may act in a concentration-dependent manner. TNF-α has been
reported to play an immunoprotective role in HIE at a low
concentration, but exert a proinflammatory effect at a high
concentration (22,23). Hs-CRP is an acute-phase protein
secreted at a low level by the liver under normal circumstances. It
is a sensitive marker of inflammatory reactions since its levels
increase in response to inflammation when the body is under stress
(24,25).
The present study revealed that the serum levels of
IL-6, TNF-α and Hs-CRP in patients with HIE were upregulated when
compared with those in the normal controls. The increased levels of
Hs-CRP indicate the presence of an acute inflammatory response in
the patients; furthermore, the high levels of IL-6 and TNF-α may
have evoked an inflammatory response cascade and caused further
damage in the brain.
In order to detect the potential correlation between
the inflammatory factors and the different clinical gradings of the
disease, the serum levels of IL-6, TNF-α and Hs-CRP in patients
with different clinical gradings were analyzed. The results
demonstrated a correlation between the upregulation of these
cytokines and the severity of the disease. Notably, a positive
correlation between the grading severity and the different
cytokines was identified. Thus, patients with greater inflammatory
responses suffered from a severe progression of the disease.
Since a quarter of the patients who survive with HIE
suffer from a variety of neuropsychological disabilities, the
possible correlation between these mediators and the prognosis of
the disease was investigated. Notably, a positive correlation
between the different inflammatory factors and the prognosis of the
disease was identified.
In conclusion, the current study highlighted the
presence of high levels of IL-6, TNF-α and Hs-CRP in patients with
HIE and the potential role of these inflammatory mediators in the
progression and prognosis of the disease. HIE not only induces the
expression of cytokines in the brain but also changes the levels of
the peripheral cytokines, which in turn exacerbates the disease in
the brain and other tissues.
References
|
1
|
Zhang P and Cheng GQ: Research progress in
mild hypothermia treatment of neonatal hypoxic-ischemic
encephalopathy. Zhongguo Dang Dai Er Ke Za Zhi. 15:918–922.
2013.(In Chinese).
|
|
2
|
Filippi L, Fiorini P, Daniotti M, et al:
Safety and efficacy of topiramate in neonates with hypoxic ischemic
encephalopathy treated with hypothermia (NeoNATI). BMC Pediatr.
12:1442012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jacobs SE, Berg M, Hunt R, et al: Cooling
for newborns with hypoxic ischaemic encephalopathy. Cochrane
Database Syst Rev. 1:CD0033112013.
|
|
4
|
Lai MC and Yang SN: Perinatal
hypoxic-ischemic encephalopathy. J Biomed Biotechnol.
2011:6098132011.PubMed/NCBI
|
|
5
|
Vannucci RC and Perlman JM: Interventions
for perinatal hypoxic-ischemic encephalopathy. Pediatrics.
100:1004–1014. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu F and McCullough LD: Inflammatory
responses in hypoxic ischemic encephalopathy. Acta Pharmacol Sin.
34:1121–1130. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bonestroo HJ, Nijboer CH, van Velthoven
CT, et al: Cerebral and hepatic inflammatory response after
neonatal hypoxia-ischemia in newborn rats. Dev Neurosci.
35:197–211. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pimentel VC, Gomes JL, Zanini D, et al:
Evaluation of acetylcholinesterase and adenosine deaminase
activities in brain and erythrocytes and proinflammatory cytokine
levels in rats submitted to neonatal hypoxia-ischemia model. Mol
Cell Biochem. 378:247–255. 2013. View Article : Google Scholar
|
|
9
|
Loddick SA, Turnbull AV and Rothwell NJ:
Cerebral interleukin-6 is neuroprotective during permanent focal
cerebral ischemia in the rat. J Cereb Blood Flow Metab. 18:176–179.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Girard S, Sébire H, Brochu ME, et al:
Postnatal administration of IL-1Ra exerts neuroprotective effects
following perinatal inflammation and/or hypoxic-ischemic injuries.
Brain Behav Immun. 26:1331–1339. 2012. View Article : Google Scholar
|
|
11
|
Aly H, Khashaba MT, El-Ayouty M, El-Sayed
O and Hasanein BM: IL-1beta, IL-6 and TNF-alpha and outcomes of
neonatal hypoxic ischemic encephalopathy. Brain Dev. 28:178–182.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Silveira RC and Procianoy RS:
Interleukin-6 and tumor necrosis factor-alpha levels in plasma and
cerebrospinal fluid of term newborn infants with hypoxic-ischemic
encephalopathy. J Pediatr. 143:625–629. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Windgassen EB, Funtowicz L, Lunsford TN,
Harris LA and Mulvagh SL: C-reactive protein and high-sensitivity
C-reactive protein: an update for clinicians. Postgrad Med.
123:114–119. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yousuf O, Mohanty BD, Martin SS, et al:
High-sensitivity C-reactive protein and cardiovascular disease: a
resolute belief or an elusive link? J Am Coll Cardiol. 62:397–408.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li XH: Diagnosis and therapy of
hypoxic-ischemic encephalopathy in newborn infants in China. J Appl
Clin Pediatr. 25:1037–1039. 2010.
|
|
16
|
van Laerhoven H, de Haan TR, Offringa M,
Post B and van der Lee JH: Prognostic tests in term neonates with
hypoxic-ischemic encephalopathy: a systematic review. Pediatrics.
131:88–98. 2013.PubMed/NCBI
|
|
17
|
Liu F and McCullough LD: Inflammatory
responses in hypoxic ischemic encephalopathy. Acta Pharmacol Sin.
34:1121–1130. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jenkins DD, Lee T, Chiuzan C, et al:
Altered circulating leukocytes and their chemokines in a clinical
trial of therapeutic hypothermia for neonatal hypoxic ischemic
encephalopathy. Pediatr Crit Care Med. 14:786–795. 2013. View Article : Google Scholar
|
|
19
|
Ali C, Nicole O, Docagne F, et al:
Ischemia-induced interleukin-6 as a potential endogenous
neuroprotective cytokine against NMDA receptor-mediated
excitotoxicity in the brain. J Cereb Blood Flow Metab. 20:956–966.
2000. View Article : Google Scholar
|
|
20
|
Westberg JA, Serlachius M, Lankila P, et
al: Hypoxic preconditioning induces neuroprotective stanniocalcin-1
in brain via IL-6 signaling. Stroke. 38:1025–1030. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chiesa C, Pellegrini G, Panero A, et al:
Umbilical cord interleukin-6 levels are elevated in term neonates
with perinatal asphyxia. Eur J Clin Invest. 33:352–358. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang Y, Cao M, Liu A, et al: Changes of
inflammatory cytokines and neurotrophins emphasized their roles in
hypoxic-ischemic brain damage. Int J Neurosci. 123:191–195. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Oygür N, Sönmez O, Saka O and Yeğin O:
Predictive value of plasma and cerebrospinal fluid tumour necrosis
factor-alpha and interleukin-1 beta concentrations on outcome of
full term infants with hypoxic-ischaemic encephalopathy. Arch Dis
Child Fetal Neonatal Ed. 79:F190–F193. 1998.PubMed/NCBI
|
|
24
|
Guo AS, Li AH, Chen X, Chen WG and Sun L:
Effect of acupoint catgut embedding on motor function and serum
high sensitivity C-reactive protein and IL-6 levels in patients
with acute cerebral infarction. Zhen Ci Yan Jiu. 38:224–228.
2013.(In Chinese).
|
|
25
|
Chen S, Martens-Lobenhoffer J, Weissenborn
K, et al: Association of dimethylarginines and mediators of
inflammation after acute ischemic stroke. J Neuroinflammation.
9:2512012. View Article : Google Scholar : PubMed/NCBI
|