Introduction
The occurrence and development of colorectal cancer
is a complicated multi-step process, which involves numerous
factors and genes. A number of tumor-related events are involved in
this process, including oncogene activation, tumor suppressor gene
inactivation, mismatch repair (MMR) gene mutations and gene
promoter hypermethylation (1,2).
Since the identification of MMR genes, studies have investigated
the association between the aberrant expression of MMR genes and
hereditary nonpolyposis colorectal cancer (HNPCC) or sporadic
colorectal cancer (3–5). A number of studies have found that
aberrant MMR gene expression plays an important role in the
occurrence of colorectal cancer (6,7). At
present, numerous genes are known to be involved in the MMR
process, including human mutL homolog 1 (hMLH1), human mutS homolog
(hMSH) 2, hMSH6, human postmeiotic segregation increased (hPSM) 1,
hPSM2, hMSH3 and hMSH5. The protein products of MMR expression are
enzymes that can repair mismatched base groups in the DNA
replication process in order to maintain the fidelity of DNA
replication.
At present, there are numerous studies investigating
the pathogenesis of HNPCC (8,9);
however, fewer studies have investigated the role of MMR gene
mutations in sporadic colorectal cancer and microsatellite
instability (MSI). A previous study found that ~15% of sporadic
colorectal cancer cases exhibit a similar pathogenesis to HNPCC
(10). However, the contribution
of MMR gene mutation to the pathogenesis of these two types of
colorectal cancer is considered to be different.
It has been indicated in a number of previous
studies (11,12) that MMR gene mutations can result in
tumorigenesis through two mechanisms. Firstly, simple sequence
repeats can cause homologous genetic recombination in the DNA
replication process. Consequently, variations in the sequence
containing the simple sequence repeats increase DNA MSI in tumor
cells. Secondly, aberrant MMR gene expression can result in the
accelerated accumulation of gene mutations in proto-oncogenes and
cancer suppressor genes. Consequently, this can affect the
proliferation regulation of normal cells. In recent years, studies
have focused on four types of MMR genes, MLH1, MSH2, MSH6 and PSM2
(13–15).
In excess of 90% of patients with HNPCC have DNA
with high MSI (MSI-H), suggesting that the occurrence of HNPCC is
associated with the functional loss of cell MMR. Therefore, DNA MSI
can be regarded as a reliable indicator to measure the function of
cell MMR (16). A typical
characteristic of MMR gene mutation is MSI expression. The
microsatellite sequence mutation rate due to MMR of tumor cells is
100–1,000 fold higher than that of normal cells. Furthermore, the
MSI in colorectal tumors caused by aberrant MMR gene expression is
~15% (17). Therefore, detecting
MSI is of high value. MSI may be used as a positive prognostic
factor for sporadic colorectal cancer (18), but also as a negative forecasting
sign for fluorouracil (5-FU)-based chemotherapy (19,20).
At present, there are there are few studies
investigating MMR genes in sporadic colorectal cancer. Therefore,
in the present study, clinicopathological data and 404
postoperative samples from patients with sporadic colorectal cancer
were collected from the Tumor Hospital of Xinjiang Medical
University (Urumqi, China). The aims of the study were to detect
MMR protein (MMRP) expression using immunohistochemistry, in order
to elucidate how aberrant MMRP expression was distributed in
Chinese patients with sporadic colorectal cancer, and to analyze
the association between aberrant MMRP expression and
clinicopathological features, in order to investigate their
prognostic effect.
Materials and methods
Patients and clinicopathological
parameters
Clinicopathological data and postoperative samples
from 404 patients with sporadic colorectal cancer were collected
between May 2009 and June 2012 from the Tumor Hospital of Xinjiang
Medical University. Parameters involved age at diagnosis, gender,
nationality, body mass index (BMI) at diagnosis, anemia, tumor
size, histological type, degree of differentiation, general type,
TNM stage, tumor location, family history of cancer and
histopathology report (shown in Table
I). The diagnostic criteria were as follows: Anemia, male
hemoglobin (Hb) <120 g/l or female Hb <115 g/l; BMI, lean
<18.5 kg/m2, normal 18.5–23.9 kg/m2,
overweight 24–27.9 kg/m2 and obese ≥28 kg/m2;
HNPCC, diagnosis according to the Amsterdam II criteria (21). Cases were excluded due to HNPCC
diagnosis, preoperative chemoradiotherapy or lack of data. Informed
consent was obtained from all the patients prior to inclusion in
the study and this study was approved by the Medical Ethics
Committee of the Affiliated Tumor Hospital of Xinjiang Medical
University (no. W201302).
 | Table IUnivariate analysis between MMRP
expression and clinicopathological parameters. |
Table I
Univariate analysis between MMRP
expression and clinicopathological parameters.
| Clinicopathological
index | Normal MMRP,
n=294 | Aberrant MMRP,
n=110 | Total, n=404 | χ2 | P-value |
|---|
| Age (years) | | | | 0.274 | 0.601 |
| <50 | 88 | 30 | 118 | | |
| ≥50 | 206 | 80 | 286 | | |
| Gender | | | | 0.335 | 0.563 |
| Male | 167 | 66 | 233 | | |
| Female | 127 | 44 | 171 | | |
| Nationality | | | | 3.907 | 0.272 |
| Han | 219 | 73 | 292 | | |
| Uyghur | 38 | 16 | 54 | | |
| Hui | 21 | 12 | 33 | | |
| Others | 14 | 9 | 25 | | |
| BMI
(kg/m2) | | | | 7.911 | 0.048 |
| <18.5 | 20 | 4 | 24 | | |
| 18.5–23.99 | 133 | 37 | 170 | | |
| 24–27.99 | 107 | 49 | 156 | | |
| ≥28 | 34 | 20 | 54 | | |
| Anemia | | | | 1.238 | 0.266 |
| Yes | 83 | 25 | 108 | | |
| No | 211 | 85 | 296 | | |
| Tumor size
(cm) | | | | 1.258 | 0.533 |
| <4 | 68 | 25 | 93 | | |
| 4–6 | 156 | 53 | 209 | | |
| ≥6 | 70 | 32 | 102 | | |
| Tissue type | | | | 7.226 | 0.007 |
| Glandular | 244 | 78 | 322 | | |
| Mucous
gland/signet cell | 50 | 32 | 82 | | |
| Differentiation
degree | | | | 8.119 | 0.004 |
|
Well/moderately | 200 | 58 | 258 | | |
| Poorly | 94 | 52 | 146 | | |
| Tumor general
type | | | | 0.257 | 0.880 |
| Ulcerative | 196 | 76 | 272 | | |
| Mass | 85 | 29 | 114 | | |
| Infiltrative | 13 | 5 | 18 | | |
| TNM staging | | | | 1.061 | 0.786 |
| I | 21 | 8 | 29 | | |
| II | 104 | 33 | 137 | | |
| III | 144 | 59 | 203 | | |
| IV | 25 | 10 | 35 | | |
| Tumor location | | | | 11.607 | 0.003 |
| Rectal | 159 | 46 | 203 | | |
| Left
hemicolon | 86 | 28 | 114 | | |
| Right
hemicolon | 51 | 36 | 87 | | |
| Familial cancer
history | | | | 7.510 | 0.023 |
| Colorectal
cancer | 20 | 16 | 36 | | |
| Others | 45 | 21 | 66 | | |
| No | 229 | 73 | 302 | | |
Immunohistochemistry
The neutral formalin-fixed (concentration, 40 g/l),
paraffin-embedded specimens were serially sectioned (5-μm
thickness), and a PV-9000 two-step method was performed using mouse
anti-human monoclonal antibodies against MLH1, MSH2, MSH6 and PSM2
(Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd., Beijing,
China) as primary antibodies with a working concentration of 1:150.
A universal two-step method (horseradish peroxidase) detection kit
(Fujian Maixin Biological Products Co., Ltd., Fuzhou, China) was
utilized. Phosphate-buffered saline was used instead of primary
antibodies as a negative control, while normal colorectal mucosa
and/or infiltrating lymphocytes were used as a positive control.
Positive expression of MLH1 and MSH2 was observed in the nucleus.
The results were analyzed in accordance with the method previously
described by Plevová et al (22), in which the number of microscopic
tumor cells showing positive nuclear staining was combined with the
staining intensity and percentage of positive cells to determine
the positive expression levels. A total of five high-power fields
were selected from each sample using a light microscope and 100
cells were counted in each field. The grading of staining intensity
was as follows: no staining, 0 points; light yellow, 1 point;
yellow, 2 points; and brown, 3 points. The grading of the
percentage of positive cells was as follows: No positive cells, 0
points; ≤10%, 1 point; 11–50%, 2 points; 51–75%, 3 points; and
>75%, 4 points. If the result obtained by multiplying the two
scores above was ≥2 points, the case was considered to have
positive expression; however, if the score was <2 points, the
case was considered to have negative expression. The positive
control was positive nuclei of normal colorectal mucosa and/or
infiltrating lymphocytes. However, a negative result was judged in
the case of positive nuclear expression in the positive control and
missing staining in the tumor cell nuclei.
Statistical analysis
Univariate analysis was performed using the
χ2 test. Multivariate correlation analysis was performed
using the logistic regression test. Disease-free survival (DFS) was
analyzed using the Kaplan-Meier method and the Log-rank test was
used for comparison between groups. The statistical analysis was
performed using SPSS for Windows version 18 (SPSS Inc., Chicago,
IL, USA). The Fisher’s exact test from the statistical package
STATA 9.0 (Stata Corp., College Station, TX, USA) was used for the
calculations. P<0.05 was considered to indicate a statistically
significant difference.
Results
Immunohistochemical results of MMRP
expression
In 404 cases with sporadic colorectal cancer, 110
(27.23%) patients showed aberrant nuclear staining for MMRP. For
patients with only one type of aberrant expression, hMLH1
expression was absent in 17 cases, hMSH2 in 9 cases, hPSM2 in 7
cases and hMSH6 in 5 cases. In patients with more than one type of
aberrant MMRP expression, the protein expression of
hMLH1/hMSH2/hPSM2/hMSH6 was absent in 3 cases, hMLH1/hMSH2/hMSH6 in
3 cases, hMSH2/hPSM2/hMSH6 in 4 cases, hMLH1/hPSM2 in 29 cases,
hMSH2/hMSH6 in 17 cases, hMLH1/hMSH2 in 7 cases, hMLH1/hMSH6 in 5
cases and hMSH2/hPSM2 in 4 cases. The highest frequency of aberrant
MMRP expression was for hMLH1/hPSM2 (Fig. 1).
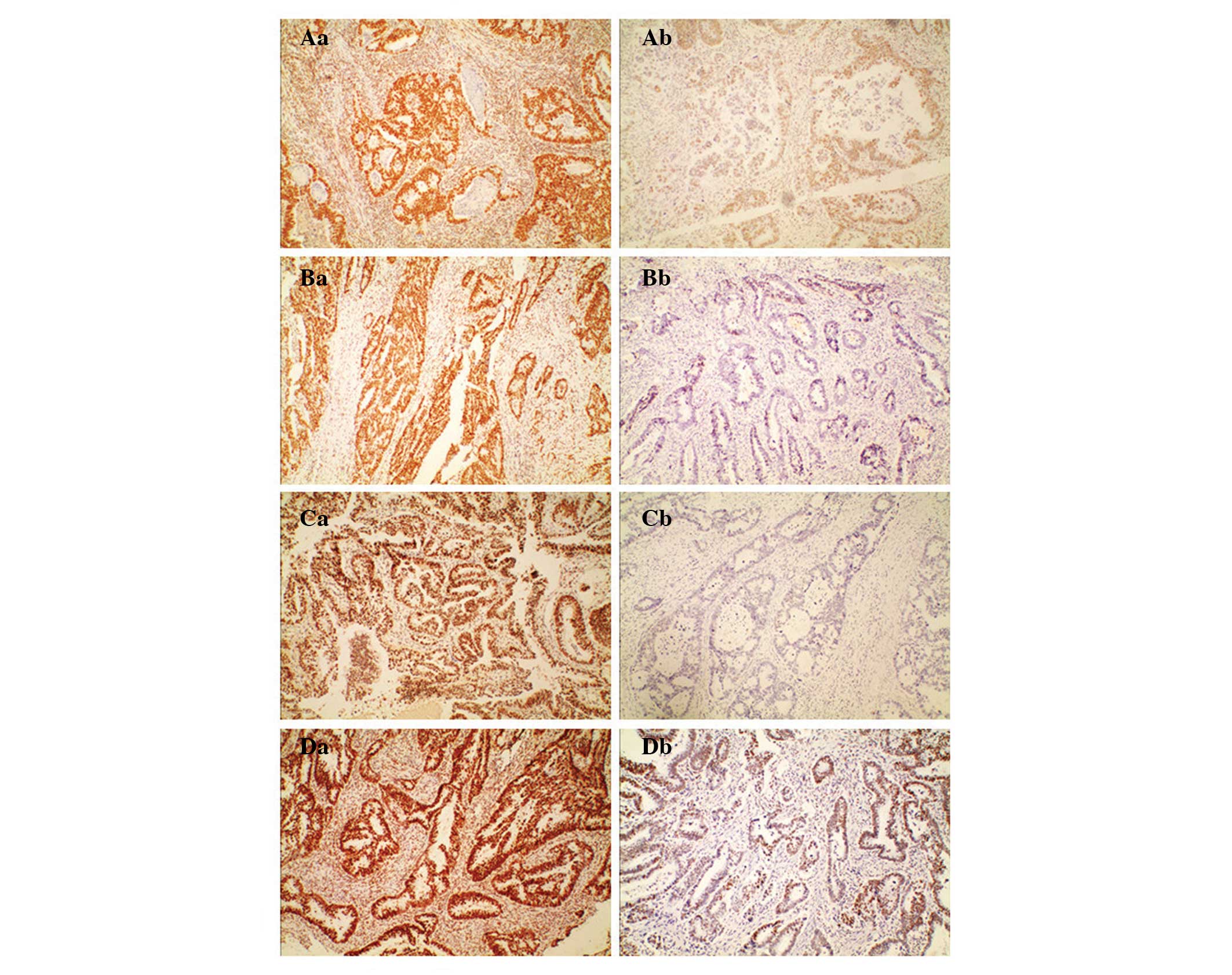 | Figure 1Immunohistochemical staining showing
normal and aberrant MMRP expression (magnification, ×100). (A)
hMLH1, (B) hMSH2, (C) hPMS2 and (D) hMSH6. (Aa-Da) Normal
immunohistochemical staining of (Aa) hMLH1, (Ba) hMSH2, (Ca) hPMS2
and (Da) hMSH6. Normal nuclear staining of the MMRPs can be
observed not only in stromal cells, but also in epithelial tumor
cells, showing a brownish accumulation of dye in the nucleus.
(Ab-Db) Aberrant staining of (Aa) hMLH1, (Ba) hMSH2, (Ca) hPMS2 and
(Da) hMSH6. Aberrant nuclear staining of the MMRPs can only be
observed in stromal cells, not in epithelial tumor cells. MMRP,
mismatch repair protein; hMLH1, human mutL homolog 1; hMSH, human
mutS homolog; hPMS2, human postmeiotic segregation increased 2. |
Univariate analysis between MMRP
expression and clinicopathological parameters
Using univariate analysis, aberrant MMRP expression
in colorectal cancer was found to be closely associated with tumor
location, histological type, BMI and family history of cancer, and
this was statistically significant (P<0.05; Table I).
Multivariate analysis between MMRP
expression and clinicopathological parameters
Using logistic regression analysis, independent risk
factors for aberrant MMR were identified; these included tumor
location, histological type, BMI and family history of cancer
(P<0.05; Table II).
| Table IIMultivariate analysis results between
MMRP expression and clinicopathological parameters. |
Table II
Multivariate analysis results between
MMRP expression and clinicopathological parameters.
| | | 95% confidence
interval | |
|---|
| | |
| |
|---|
| Variable | B-value | OR | Lower bound | Upper bound | P-value |
|---|
| BMI
(kg/m2) |
| ≤24 vs.
≥24 | 0.341 | 0.711 | 0.529 | 0.956 | 0.024 |
| Histological
type |
| Glandular
vs. mucous gland/signet cell | 0.609 | 1.838 | 1.072 | 3.152 | 0.027 |
| Tumor location |
| Left
hemicolon/rectal vs. right hemicolon | 0.761 | 0.467 | 0.278 | 0.784 | 0.004 |
| Family history of
cancer |
| Positive
vs. negative | 0.413 | 1.511 | 1.075 | 2.124 | 0.017 |
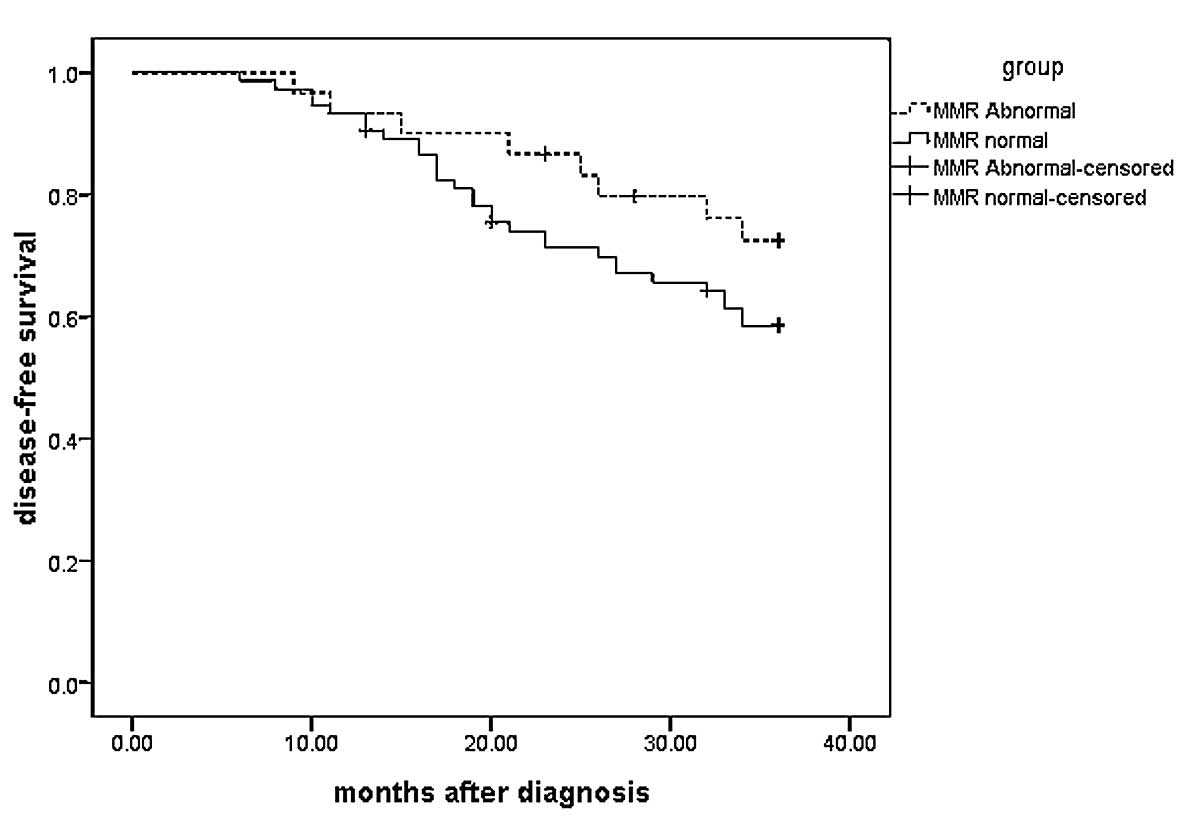
Survival analysis of normal and aberrant
MMRP expression groups
A total of 104 cases with stage III colorectal
cancer were randomly selected from 404 cases and followed up for
>3 years. A total of 5 cases were lost midway through the
follow-up: Three patients succumbed (two due to other diseases and
one due to a traffic accident), one patient moved abroad, leading
to a loss of contact, and one patient quit the study midway due to
mental disease. In total, 74 cases had normal MMRP expression,
while 30 cases exhibited aberrant MMR expression. The three-year
overall survival was 70.19%, and 31 cases succumbed from distant
metastasis or local recurrence. However, the three-year DFS rate
was 58.65%, of which 20 cases showed aberrant MMRP expression. The
Kaplan-Meier survival curve showed that the aberrant expression
group had a three-year DFS rate of 66.67%, which was higher than
the three-year DFS rate of the normal group (55.41%). However, no
statistical difference was found using the Log-Rank test
(P>0.05; Fig. 2).
Discussion
To date, a number of previous studies have confirmed
that immunohistochemistry is a reliable method for MMR gene
analysis (23–26). The method has been utilized in the
majority of hospitals and research institutions, and has been shown
to be cost effective, stable and with a high sensitivity (77–100%)
and specificity (98–100%) (23,24).
As a result, the immunohistochemical method has been suggested as
the preferred method for MMR gene mutation analysis (25,26).
The immunohistochemistry PV-9000 two-step method is an enzymatic
biotin method. Monovalent Fab fragments of second antibody
molecules polymerize with enzymes instead of the traditional method
of secondary and tertiary antibodies. Consequently, the
antigen-antibody binding signal is directly amplified. Compared
with the traditional streptavidin-peroxidase three-step method, the
PV-9000 two-step method is simple, fast and sensitive. In addition,
it avoids background staining due to a lack of biotin. Thus, the
immunohistochemistry PV-9000 two-step method is often used in
clinical practice. In the present study, the immunohistochemistry
PV-9000 two-step method was performed to measure the expression
levels of hMLH1 hMSH2, hPMS2 and hMSH6 in 404 postoperative
pathological specimens.
Numerous studies have investigated MLH1 and MSH2
expression (27,28); however, fewer studies have
investigated MSH6 and PSM2. It has been shown that the rate of
aberrant MLH1 expression is higher than that of MSH2 (23). This may be due to the inactivation
of the MLH1 gene in somatic cells (29). CpG islands within the MLH1 gene
promoter region are hypermethylated. This methylation causes
barriers against gene transcription and translation, resulting in
aberrant MLH1 expression. Aberrant MLH1/PSM2 expression is the most
common type of aberrant MMR gene expression due to the high
frequency of MLH1 methylation and easy heterodimer formation.
Correspondingly, aberrant PSM2 expression becomes relatively higher
(30,31). In the present study, only one type
of aberrant MMRP expression was observed in 38 cases (9.4%).
Aberrant expression of hMLH1/hPSM2 showed the highest rate
(26.36%), while the rate of aberrant hMSH2/hMSH6 expression was the
second highest (15.45%). The results from this study were
consistent with those from a previous study by Molaei et al
(32).
A number of previous studies (33,34)
have demonstrated that aberrant MMR is associated with certain
clinicopathological features. This association has an important
role in the clinical diagnosis and treatment of colorectal cancer.
In the present study, cases where the tumor was in the right
hemicolon or the tissue type was mucus gland or signet ring cell
carcinoma were found to have a higher incidence of aberrant MMRP
expression, which is consistent with the results from previous
studies (23,35). This may be due to the fact that
aberrant MMRP expression is closely associated with MSI-H. The
clinicopathological features of right hemicolon tumors or mucinous
adenocarcinomas include MSI-H (36–38).
In the present study, no difference was observed between rectal and
left hemicolon tumors with regard to MMRP expression, suggesting
that the aberrant MMR expression pathways exhibit consistency.
However, a statistical difference was observed between left and
right hemicolon carcinomas, suggesting that a higher incidence of
gene promoter hypermethylation may occur in the right hemicolon
tissues, leading to the occurrence of MSI.
In the present study it was demonstrated that the
rate of aberrant MMRP expression was not associated with age at
diagnosis, gender, nationality, anemia, tumor size or TNM staging
(P>0.05). The association between anemia and MMRP expression
has, to this date, been unclear. The rate of aberrant MMRP
expression in the anemia group (23.15%) was lower than that in the
normal hemoglobin group (28.72%); however, this difference was not
statistically significant (P>0.05). Tumors with aberrant MMRP
expression were mostly located in right hemicolon, the clinical
manifestations of which showed a higher risk of anemia. Further
studies are required to elucidate the specific association between
these factors.
With improvements in living standards, dietary
structure has also been changing. The dietary habit of consuming
more meat and less fiber has caused an increasing incidence of
overweight and obese individuals. An increasing number of studies
are focusing on the association between BMI and colorectal cancer.
Several studies have shown a close correlation between increasing
BMI and risk factors of colorectal cancer (39,40).
However, with the exception of the study by van Duijnhoven et
al (41), which described
certain aspects of the association between BMI and MMR gene
expression, studies focusing on the association between BMI and MMR
gene expression are relatively rare. In the present study,
increasing BMI was significantly correlated with aberrant MMRP
expression. In the study by Botma et al (42), it was revealed that BMI had a close
correlation with colorectal adenomas; however, the study subjects
were all male. In the study by Win et al (43), manifested BMI was reported to be a
potential risk factor for individuals in early adulthood carrying
MMR gene mutations. Therefore, previous study results suggest that
MMR gene mutation occurs in the early pathogenetic stage of
colorectal cancer. Being overweight or obese may be independent
risk factors of aberrant MMR gene expression. However, further
studies are required to investigate the underlying mechanism, as
this has yet to be elucidated.
Studies investigating whether the pathogenesis of
sporadic colorectal cancer in patients with a tumor familial
history is the same as that of HNPCC are rare. Germline MMR gene
mutations have been identified as the molecular genetic basis
underlying HNPCC. By contrast, mutations in the adenomatous
polyposis coli gene are believed to comprise the molecular genetic
basis underlying familial adenomatous polyposis and the majority of
sporadic colorectal cancer cases. Sporadic colorectal cancer
additionally exhibits a polygenic and multi-stage process of tumor
formation, which includes activating mutations in adenoma-carcinoma
sequences in oncogenes and inactivating mutations in tumor
suppressor genes (44,45). In the present study, the rate of
aberrant MMRP expression in the group with a family history of
cancer (36.27%) was higher than that in the group without a family
history of cancer (24.17%), with a statistically significant
difference (P<0.05). Therefore, cancer family history was
correlated with aberrant MMR expression.
A number of studies have revealed that patients with
a positive MSI in colorectal cancer show a more favorable prognosis
(46,47); however, the mechanism associated
with this remains unclear. Popat et al (18) reported that, although colorectal
cancer with MSI-H had numerous features associated with a poor
prognosis, MSI-H was also associated with a relatively good
prognosis due to increased inflammatory cell infiltration. In
addition, Sargent et al (20) revealed that cancer with MSI-H was
not sensitive to 5-FU-based chemotherapy. However, as to whether it
is associated with MMR gene mutations, a number of studies
(48,49) have produced affirmative results. In
the present study, 104 patients with stage III colorectal cancer
were followed up for >3 years. Survival analysis showed that the
three-year DFS of the aberrant MMRP expression group was higher
than that of the normal expression group. However, no statistically
significant difference was identified between the groups
(P>0.05). This may be due to the fact that patients with
aberrant MMRP expression had a higher MSI, which, according to the
above studies, was a good prognostic factor.
In conclusion, the immunohistochemistry PV-9000
two-step method can be feasibly used to detect the MMRP expression
level in sporadic colorectal cancer. MMRP expression is closely
associated with tumor location, histological type, differentiation
degree, BMI and a family history of cancer, respectively. MMRP
expression level may be a promising prognostic factor. Therefore,
MMR plays a significant role in the occurrence and development of
colorectal cancer; further studies are required to explore its
detailed mechanism.
Acknowledgements
This study was supported by the National 11th
Five-Year Science and Technology Support Program of China (no.
2006BAI02A06) and the Science and Technology Innovation Fund of
Xinjiang Medical University (no. XJC201267).
References
|
1
|
Adib SM, Tabbal N, Hamadeh R and Ammar W:
Geographic epidemiology in a small area: cancer incidence in
Baakline, Lebanon, 2000–2008. East Mediterr Health J. 19:320–326.
2013.PubMed/NCBI
|
|
2
|
Van Engeland M, Derks S, Smits KM, et al:
Colorectal cancer epigenetics: complex simplicity. J Clin Oncol.
29:1382–1391. 2011.PubMed/NCBI
|
|
3
|
Blokhuis MM, Pietersen GE, Goldberg PA, et
al: Lynch syndrome: the influence of environmental factors on
extracolonic cancer risk in hMLH1 c. C1528T mutation carriers and
their mutation-negative sisters. Fam Cancer. 9:357–363. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fishel R, Lescoe MK, Rao MR, et al: The
human mutator gene homolog MSH2 and its association with hereditary
nonpolyposis colon cancer. Cell. 75:1027–1038. 1993. View Article : Google Scholar
|
|
5
|
Aaltonen LA, Salovaara R, Kristo P, et al:
Incidence of hereditary nonpolyposis colorectal cancer and the
feasibility of molecular screening for the disease. N Engl J Med.
338:1481–1487. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mureşan F, Simescu R, Domşa I, et al:
Immunohistochemical screening of hMLH1 and hMSH2 gene mutations in
patients diagnosed with colorectal cancer and microsatellite
instability suspicion. Chirurgia (Bucur). 106:775–780. 2011.(In
Romanian).
|
|
7
|
Wei W, Liu F, Liu L, et al: Distinct
mutations in MLH1 and MSH2 genes in hereditary non-polyposis
colorectal cancer (HNPCC) families from China. BMB Rep. 44:317–322.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rodriguez-Bigas MA, Boland CR, Hamilton
SR, et al: A National Cancer Institute Workshop on Hereditary
Nonpolyposis Colorectal Cancer Syndrome: meeting highlights and
Bethesda guidelines. J Natl Cancer Inst. 89:1758–1762
|
|
9
|
Lynch HT and Smyrk T: Hereditary
nonpolyposis colorectal cancer (Lynch syndrome). An updated review.
Cancer. 78:1149–1167. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Win Aung Ko, Young Joanne P, et al:
Colorectal and other cancer risks for carriers and noncarriers from
families with a DNA mismatch repair gene mutation: a prospective
cohort study. J Clin Oncol. 30:958–964. 2012.PubMed/NCBI
|
|
11
|
Wada-Hiraike O, Yano T, Nei T, et al: The
DNA mismatch repair gene hMSH2 is a potent coactivator of oestrogen
receptor alpha. Br J Cancer. 92:2286–2291. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Park IJ, Kim HC, Kim JS, et al:
Correlation between hhMLH1/hhMSH2 and p53 protein expression in
sporadic colorectal cancer. Hepatogastroenterology. 52:450–454.
2005.PubMed/NCBI
|
|
13
|
Vreeswijk MP and van der Klift HM:
Analysis and interpretation of RNA splicing alterations in genes
involved in genetic disorders. Methods Mol Biol. 867:49–63. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sun ZQ, Yu XB, Wang HJ, et al:
Relationship between Aberrant Expression of hMSH2 and prognosis in
patients with sporadic colorectal cancer. Canc Cell Rec. 2:e47–e54.
2014.
|
|
15
|
Belcheva A, Irrazabal T, Robertson SJ, et
al: Gut microbial metabolism drives transformation of
msh2-deficient colon epithelial cells. Cell. 158:288–299. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cunningham JM, Kim CY, Chirstensen ER, et
al: The frequency of hereditary defective mismatch repair in a
prospective series of unselected colorectal carcinomas. Am J Hum
Genet. 69:780–790. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ionov Y, Peinado MA, Malkhosyan S, et al:
Ubiquitous somatic mutations in simple repeated sequences reveal a
new mechanism for colonic carcinogenesis. Nature. 363:558–561.
1993. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Popat S, Hubner R and Houlston RS:
Systematic review of microsatellite instability and colorectal
cancer prognosis. J Clin Oncol. 23:609–618. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ribic CM, Sargent DJ, Moore MJ, et al:
Tumor microsatellite-instability status as a predictor of benefit
from fluorouracil-based adjuvant chemotherapy for colon cancer. N
Engl J Med. 349:247–257. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sargent DJ, Marsoni S, Monges G, et al:
Defective mismatch repair as a predictive marker for lack of
efficacy of fluorouracil-based adjuvant therapy in colon cancer. J
Clin Oncol. 28:3219–3226. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Holzhüter J, Rösch T, Block A, et al: A
44-year-old woman with hereditary nonpolyposis colon carcinoma:
screening examinations for non-colonic tumors. Internist (Berl).
54:353–358. 2013.(In German).
|
|
22
|
Plevová P, Krepelová A, Papezová M, et al:
Immunohistochemical detection of the hMLH1 and hMSH2 proteins in
hereditary non-polyposis colon cancer and sporadic colon cancer.
Neoplasma. 51:275–284. 2004.PubMed/NCBI
|
|
23
|
Lindor NM, Burgart LJ, Leontovich O, et
al: Immunohistochemistry versus microsatellite instability testing
in phenotyping colorectal tumors. J Clin Oncol. 20:1043–1048. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ruszkiewicz A, Bennett G, Moore J, et al:
Correlation of mismatch repair genes immunohistochemistry and
microsatellite instability status in HNPCC-associated tumours.
Pathology. 34:541–547. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shia J, Klimstra DS, Nafa K, et al: Value
of immunohistochemical detection of DNA mismatch repair proteins in
predicting germline mutation in hereditary colorectal neoplasms. Am
J Surg Pathol. 29:96–104. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Marcus VA, Madlensky L, Gryfe R, et al:
Immunohistochemistry for hMLH1 and hMSH2: a practical test for DNA
mismatch repair-deficient tumors. Am J Surg Pathol. 23:1248–1255.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Joost P, Veurink N, Holck S, et al:
Heterogenous mismatch-repair status in colorectal cancer. Diagn
Pathol. 9:1262014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Haghighi MM, Aghagolzadeh P, Zadeh SM, et
al: Telomere shortening: a biological marker of sporadic colorectal
cancer with normal expression of p53 and mismatch repair proteins.
Genet Test Mol Biomarkers. 18:236–244. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hawkins NJ and Ward RL: Sporadic
colorectal cancers with microsatellite instability and their
possible origin in hyperplastic polyps and serrated adenomas. J
Natl Cancer Inst. 93:1307–1313. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kupčinskaitė-Noreikienė R, Skiecevičienė
J, Jonaitis L, et al: CpG island methylation of the MLH1, MGMT,
DAPK, and CASP8 genes in cancerous and adjacent noncancerous
stomach tissues. Medicina (Kaunas). 49:361–366. 2013.PubMed/NCBI
|
|
31
|
Gomes A, Reis-Silva M, Alarcão A, et al:
Promoter hypermethylation of DNA repair genes MLH1 and MSH2 in
adenocarcinomas and squamous cell carcinomas of the lung. Rev Port
Pneumol. 20:20–30. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Molaei M, Mansoori BK, Ghiasi S, et al:
Colorectal cancer in Iran: immunohistochemical profiles of four
mismatch repair proteins. Int J Colorectal Dis. 25:63–69. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bellizzi AM and Frankel WL: Colorectal
cancer due to deficiency in DNA mismatch repair function: a review.
Adv Anat Pathol. 16:405–417. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Valle L, Perea J, Carbonell P, et al:
Clinicopathologic and pedigree differences in amsterdam I-positive
hereditary nonpolyposis colorectal cancer families according to
tumor microsatellite instability status. J Clin Oncol. 25:781–786.
2007. View Article : Google Scholar
|
|
35
|
Jass JR: HNPCC and sporadic MSI-H
colorectal cancer: a review of the morphological similarities and
differences. Fam Cancer. 3:93–100. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Raskin GA, Ianus GA, Kornilov AV, et al:
Immunohistochemical examination of MSH2, PMS2, MLH1, MSH6 compared
with the analysis of microsatellite instability in colon
adenocarcinoma. Vopr Onkol. 60:47–50. 2014.(In Russian).
|
|
37
|
Kim JH and Kang GH: Molecular and
prognostic heterogeneity of microsatellite-unstable colorectal
cancer. World J Gastroenterol. 20:4230–4243. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Goldstein J, Tran B, Ensor J, et al:
Multicenter retrospective analysis of metastatic colorectal cancer
(CRC) with high-level microsatellite instability (MSI-H). Ann
Oncol. 25:1032–1038. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Slattery ML, Levin TR, Ma K, et al: Family
history and colorectal cancer: predictors of risk. Cancer Causes
Control. 14:879–887. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Campbell PT, Cotterchio M, Dicks E, et al:
Excess body weight and colorectal cancer risk in Canada:
associations in subgroups of clinically defined familial risk of
cancer. Cancer Epidemiol Biomarkers Prev. 16:1735–1744. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
van Duijnhoven FJ, Botma A, Winkels R, et
al: Do lifestyle factors influence colorectal cancer risk in Lynch
syndrome? Fam Cancer. 12:285–293. 2013.PubMed/NCBI
|
|
42
|
Botma A, Nagengast FM, Braem MG, et al:
Body mass index increases risk of colorectal adenomas in men with
Lynch syndrome: the GEOLynch cohort study. J Clin Oncol.
28:4346–4353. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Win AK, Dowty JG, English DR, et al: Body
mass index in early adulthood and colorectal cancer risk for
carriers and non-carriers of germline mutations in DNA mismatch
repair genes. Br J Cancer. 105:162–169. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Sánchez-de-Abajo A, de la Hoya M, van
Puijenbroek M, et al: Molecular analysis of colorectal cancer
tumors from patients with mismatch repair proficient hereditary
nonpolyposis colorectal cancer suggests novel carcinogenic
pathways. Clin Cancer Res. 13:5729–5735. 2007.
|
|
45
|
Karoui M, Tresallet C, Brouquet A, et al:
Colorectal carcinogenesis. 1. Hereditary predisposition and
colorectal cancer. J Chir (Paris). 144:13–18. 2007.(In French).
|
|
46
|
Bubb VJ, Curtis LJ, Cunningham C, et al:
Microsatellite instability and the role of hhMSH2 in sporadic
colorectal cancer. Oncogene. 12:2641–2649. 1996.PubMed/NCBI
|
|
47
|
Gryfe R, Kim H, Hsieh ET, et al: Tumor
microsatellite instability and clinical outcome in young patients
with colorectal cancer. N Engl J Med. 342:69–77. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Sankila R, Aaltonen LA, Järvinen HJ and
Mecklin JP: Better survival rates in patients with hMLH1-associated
hereditary colorectal cancer. Gastroenterology. 110:682–687. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Heinimann K, Scott RJ, Buerstedde JM, et
al: Influence of selection criteria on mutation detection in
patients with hereditary nonpolyposis colorectal cancer. Cancer.
85:2512–2518. 1999. View Article : Google Scholar : PubMed/NCBI
|