Introduction
Acetabular dysplasia is a relatively common
abnormality of the anatomy of the acetabulum, whose prevalence in
adults varies across studies from 1–15% (1–4). The
disease is usually undiagnosed until the appearance of symptoms
during the second or third decade of a patient’s life. Dysfunction,
pain and limpness are the initial symptoms of acetabular dysplasia
in adults (5). In total, ~20–50%
of adults develop arthritis as a result of subluxation or dysplasia
of the hip (6). Adults with
acetabular dysplasia usually have a shallow or deformed acetabulum,
occasionally with luxation or subluxation of the hip (7). Patients with persistent acetabular
dysplasia and subluxation are at high risk of osteoarthritis (OA)
(8,9). The lack of early diagnosis and
treatment for acetabular dysplasia can lead to OA in adults
(10). At present, the imaging
diagnosis of acetabular dysplasia typically depends on radiographic
evaluation. Certain parameters, such as the center-edge (CE) and
Tönnis angles, are the most commonly used measurements of
acetabular dysplasia (7,11,12).
The Tönnis angle measures the weight-bearing surface
of the acetabulum, otherwise known as the acetabular sourcil. More
precisely, the acetabular sourcil represents an area of subchondral
osseous condensation in the acetabular roof (7). The Tönnis angle is formed between a
horizontal line and a tangential line extending from the medial
edge to the lateral edge of the acetabular sourcil; however, in
clinical practice, the medial edges of certain acetabular sourcils
on hip radiographs are not distinct (13), resulting in the inaccuracy or
impossibility of Tönnis angle measurement. In addition, the
relative positions of the medial edges of the acetabular sourcils
may have a number of individual differences, which may affect the
accuracy of the Tönnis angle measurement. The aim of the present
study was to evaluate the clarity and relative position of the
medial edge of the acetabular sourcil on hip radiographs and to
attempt to improve the Tönnis angle.
Materials and methods
Patients
Conventional anterior-posterior pelvic radiographs
of patients, obtained between December 2012 and February 2013, were
extracted from the picture-archiving communication system in The
Second Hospital of Shandong University (Jinan, China). The
exclusion criteria comprised narrowing of the hip joint space,
subluxation and luxation of the hip joint, osteonecrosis of the
femoral head, acetabular and femoral fracture, hip tumor and total
hip arthroplasty. According to the criteria of Siebenrock et
al (14), further assessments
were made of the anterior-posterior pelvic radiographs showing the
alignment of the tip of the coccyges with the middle of the
symphysis pubis and the distance between the sacrococcygeal joint
and the symphysis pubis (<32 mm in males and <47 mm in
females). With these criteria, 224 patients (120 females and 104
males) with 448 hips, aged between 15 and 83 years (median, 45.0
years), were selected for this study. All procedures were approved
by the Ethics Committee of The Second Hospital of Shandong
University. Informed consent was obtained from all patients or
their families.
Measurements on radiographs
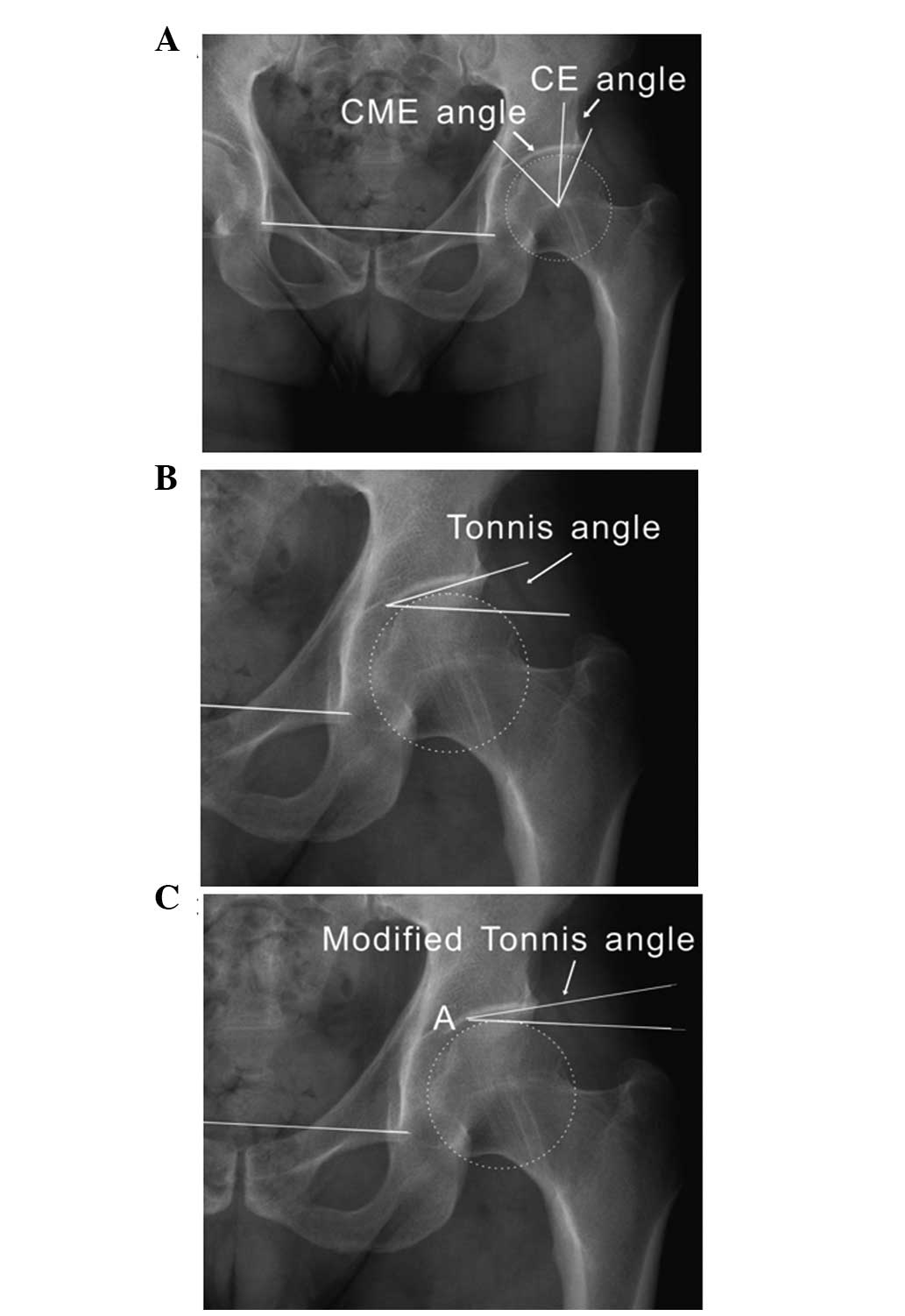
To measure the CE angle, the horizontal plane of the
pelvis was firstly determined by drawing a horizontal line along
the inferior boundaries of the two teardrops. A vertical line
perpendicular to the horizontal plane of the pelvis was then drawn
as described above (teardrop to teardrop), crossing the center of
the femoral head. Finally, an oblique line from the center of the
femoral head was drawn out to the lateral margin of the acetabulum.
The angle between the vertical line and the oblique line showed
Wiberg’s CE angle (Fig. 1A).
The Tönnis angle was formed by a line parallel to
the horizontal plane of the pelvis (teardrop to teardrop) touching
the medial edge of the weight-bearing portion of the acetabulum
(the ‘sourcil’) and a tangential line extending from the medial
edge to the lateral edge of the acetabular sourcil (Fig. 1B).
To evaluate the relative position of the medial edge
of the acetabular sourcil, a new parameter known as the
center-medial-edge (CME) angle was designed. The CME angle was the
angle between the vertical line through the femoral head center, as
described above, and the line that was tangential to the femoral
head center and the medial margin of the acetabular sourcil
(Fig. 1A).
As an improvement of the Tönnis angle, a new angle,
preliminarily termed the modified Tönnis angle, was created. The
measure this angle, a line parallel to the horizontal plane of the
pelvis was drawn as described above (teardrop to teardrop),
touching the vertex of the femoral head. This line intersected with
the acetabular sourcil at a point marked ‘A’. A line originating
from point A was then drawn out to the lateral extent of the
weight-bearing portion of the acetabulum. The angle between these
two lines indicated the modified Tönnis angle (Fig. 1C). If the lateral edge of the
acetabular sourcil was below the parallel line, the value of the
modified Tönnis angle was negative.
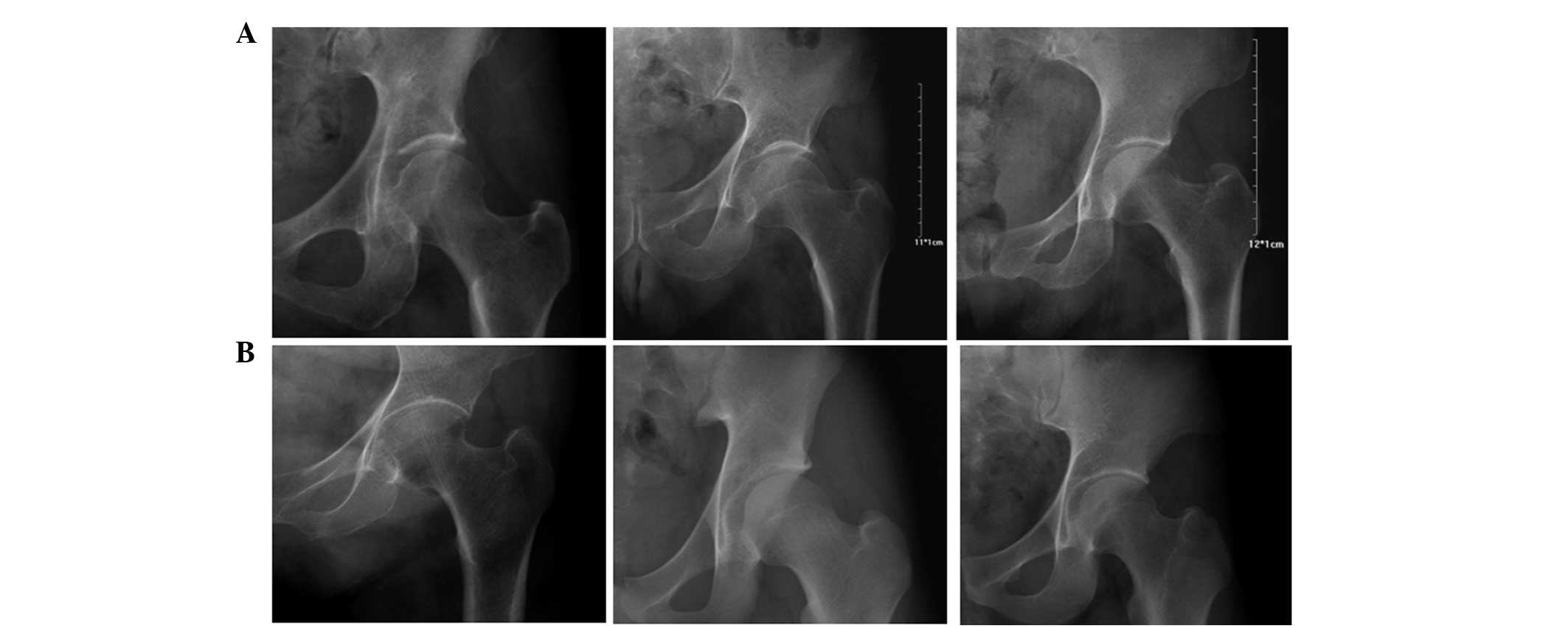
According to the clarity degree of the medial edge
of the acetabular sourcil on radiograph, the hips were divided into
the clear-edge (Fig. 2A) and
blurred-edge (Fig. 2B) groups. The
hips belonging to the blurred-edge group could not be used for
Tönnis angle measurements. All measurements were performed
digitally using the Huahai MedPACS picture-archiving communication
system (Huahai Medical Info-Tech Co., Ltd., Xi’an, China).
Statistical analysis
All statistical analyses were performed using SPSS
18.0 for Windows (SPSS, Inc., Chicago, IL, USA). Statistical
analysis of the type of acetabular sourcil based on the medial edge
clarity was made. The Gaussianity of various parameters was
graphically revealed using frequency polygons. Associations between
any two of the CE angle, the Tönnis angle and the modified Tönnis
angle were evaluated using Pearson’s coefficient of correlation.
The association between the CME and CE angles was also evaluated.
Differences were considered significant when P<0.01.
Results
Hips belonging to the blurred-edge group
cannot be used for Tönnis or CME angle measurements
To measure the values of the CE, CME, Tönnis and
modified Tönnis angles, 448 hips were analyzed. Among these hips,
142 (31.7%) were assigned to the blurred-edge group and 306 (68.3%)
had clear medial sourcil edges that were used to measure the Tönnis
and CME angles. All 448 hips were used for CE and modified Tönnis
angle measurement. The mean CME angle was 37.94° with a range of
21.76–63.99° [n=306; 95% confidence intervals (CI), 37.22–38.66°;
standard deviation, 6.41]. The mean modified Tönnis angle was 2.67°
(n=448; 95% CI, 2.24–3.10°; standard deviation, 4.62), with the 95%
prediction interval being estimated to be −6.39 to 11.73°. These
data demonstrated that hips in the blurred-edge group could not be
used for Tönnis or CME angle measurements, but the limitation did
not exist in the measurements of the CE and modified Tönnis
angles.
CME angle values vary across a large
range
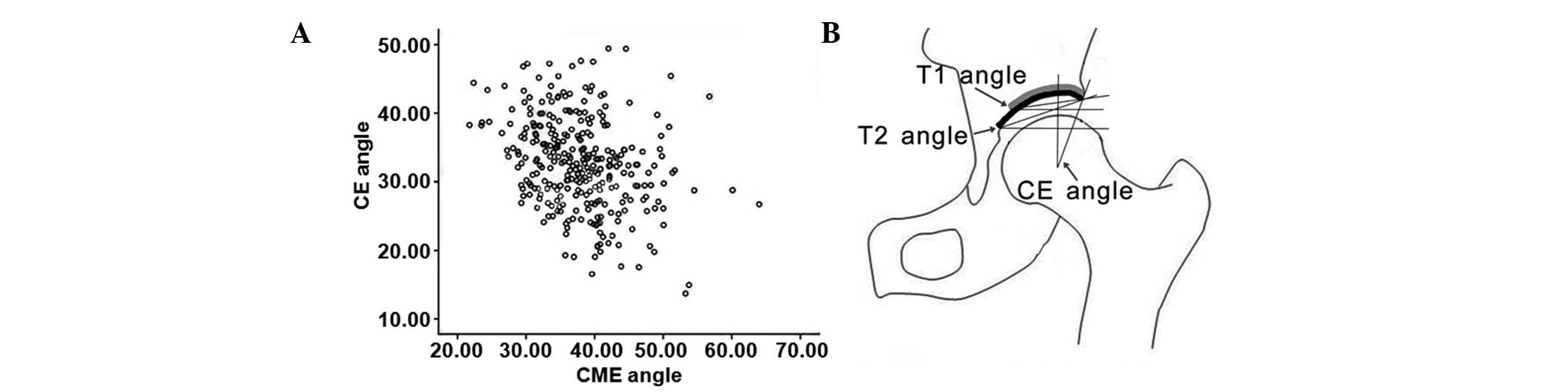
To evaluate the correlation between the CE and CME
angles, a scatter plot was drawn. According to the scatter plot,
the points representing the CE and CME angles were distributed in
the coordinate without any order, suggesting weak association
between the two angles (Fig. 3A).
It is possible that a situation could exist in which two hips with
the same CE angle value could have two acetabular sourcils with
marked differences between the relative medial edge positions; this
would generate two notably different Tönnis angles, thus affecting
the correlation between the CE and Tönnis angles (Fig. 3B). These data indicated that the
relative positions of the medial edges of the acetabular sourcils
in hips could vary across a large range, which could decrease the
correlation coefficient between the CE and Tönnis angles to a
certain degree.
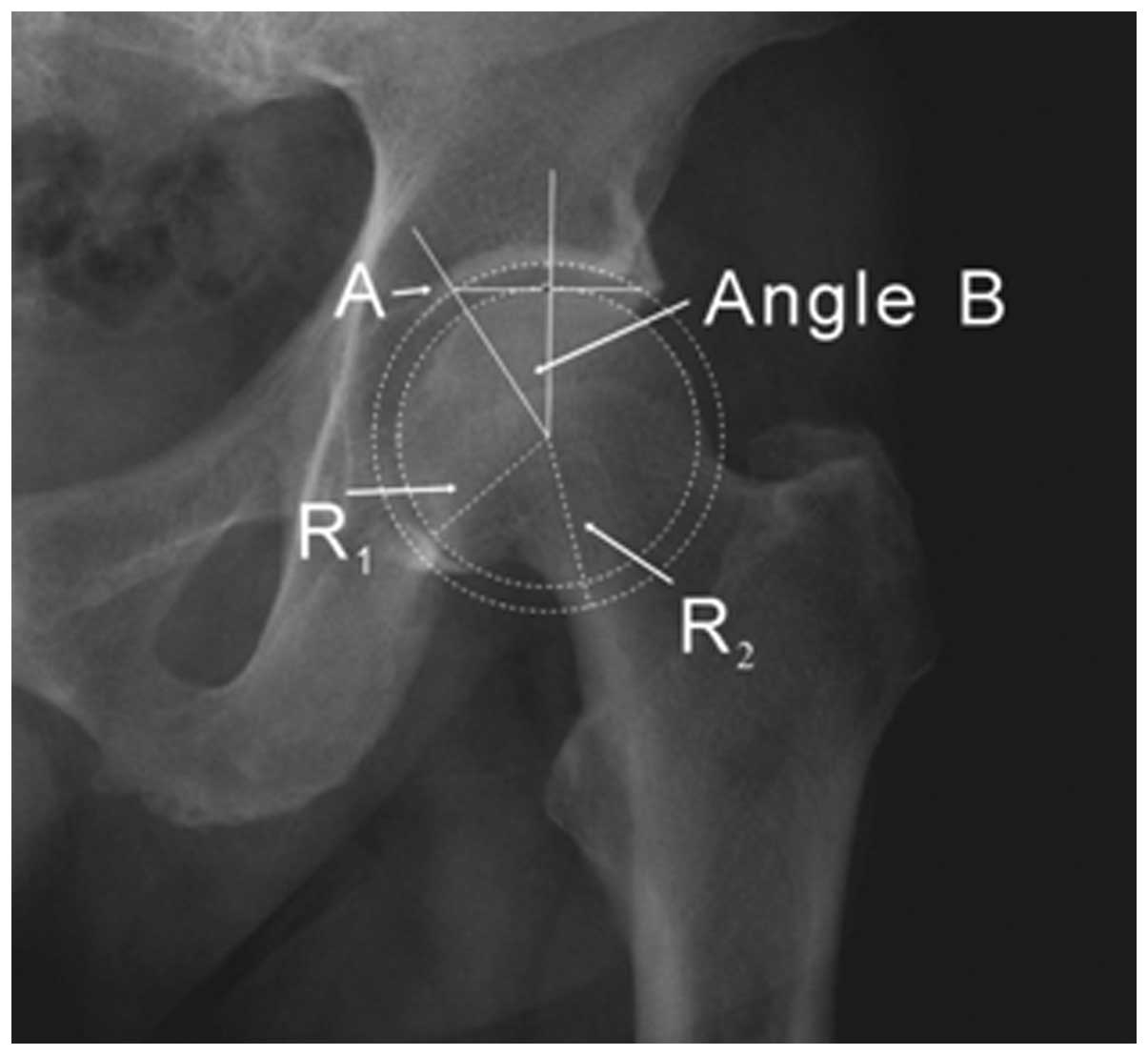
Theoretically, the value of angle B is
only affected by the radii of the femoral head and acetabulum
To improve the Tönnis angle, the modified Tönnis
angle was created, which was formed by two lines that intersected
at a point marked ‘A’ (Fig. 1C).
Point A was used to measure the modified Tönnis angle, and the
relative position of point A was determined by angle B (Fig. 4). R1 and R2
represented the radii of the femoral head and acetabulum,
respectively. Theoretically, cosB is equal to
R1/R2; therefore, the relative position of
point A can only be affected by the radii of the femoral head and
acetabulum. Compared with the medial edge of the acetabular
sourcil, point A was clear in all patients, and its relative
position was more stable. These data suggested that point A could
rarely negatively affect the measurement of the modified Tönnis
angle.
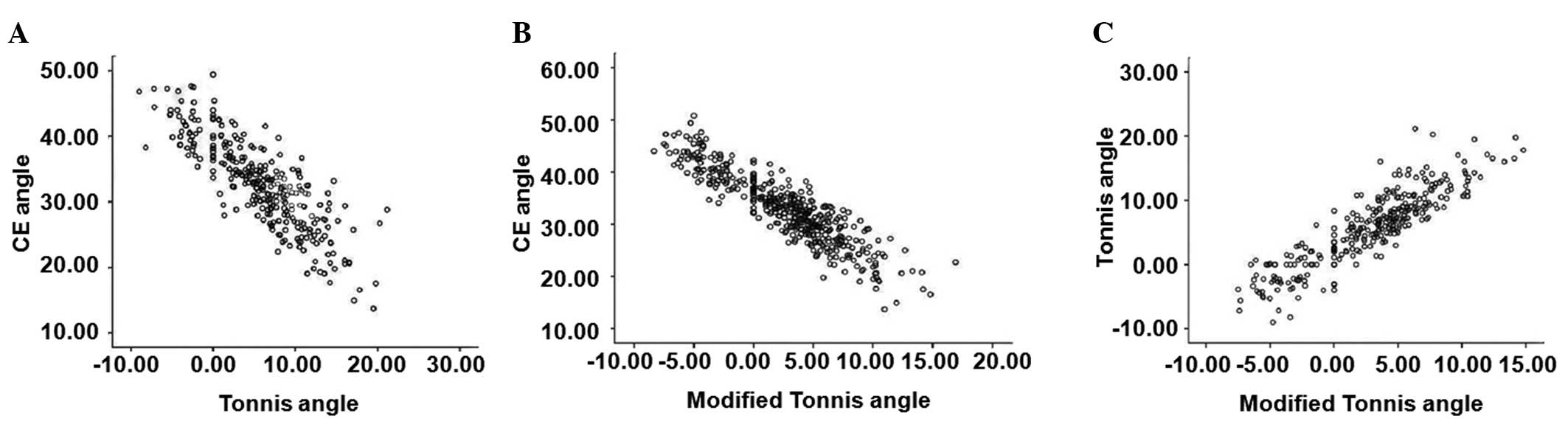
Positive or negative correlations exist
between any two of the CE, Tönnis and modified Tönnis angles
To evaluate whether correlations existed between any
two of the CE, Tönnis and modified Tönnis angles, three scatter
plots were drawn. The correlation coefficients were −0.838 between
the CE and Tönnis angles (n=306, P<0.01), 0.889 between the
Tönnis and modified Tönnis angles (n=306, P<0.01), and −0.905
between the CE and modified Tönnis angles (n=448, P<0.01)
(Table I and Fig. 5). These data demonstrated that
strong negative or positive correlations existed between any two of
the CE, Tönnis and modified Tönnis angles, and the correlation
between the CE and modified Tönnis angles was the strongest.
 | Table ICorrelation coefficients between any
two of the CE, Tönnis, modified Tönnis and CME angles. |
Table I
Correlation coefficients between any
two of the CE, Tönnis, modified Tönnis and CME angles.
| Angle | Statistical
analysis | CE angle | Tönnis angle | Modified Tönnis
angle | CME angle |
|---|
| CE angle | Pearson
correlation | 1 | −0.838a | −0.905a | −0.309a |
| P-value
(two-tailed) | | <0.001 | <0.001 | <0.001 |
| N | 448 | 306 | 448 | 306 |
| Tönnis angle | Pearson
correlation | −0.838a | 1 | 0.889a | 0.635a |
| P-value
(two-tailed) | <0.001 | | <0.001 | <0.001 |
| N | 306 | 306 | 306 | 306 |
| Modified Tönnis
angle | Pearson
correlation | −0.905a | 0.889a | 1 | 0.316a |
| P-value
(two-tailed) | <0.001 | <0.001 | | <0.001 |
| N | 448 | 306 | 448 | 306 |
| CME angle | Pearson
correlation | −0.309a | 0.635a | 0.316a | 1 |
| P-value
(two-tailed) | <0.001 | <0.001 | <0.001 | |
| N | 306 | 306 | 306 | 306 |
Discussion
Wiberg’s CE angle and the Tönnis angle are commonly
used to measure hip dysplasia. A CE angle value of <20°
indicates hip dysplasia. Values of 20–25° are considered borderline
dysplasia, representing hips that are at the lower normal limits in
terms of femoral head coverage, but not quite considered to have
uncovering (15). The Tönnis angle
is also known as the acetabular roof angle of Tönnis, the
weight-bearing acetabular index, Lequesne’s acetabular index, the
acetabular roof obliquity and the horizontal toit externe angle
(7,16,17).
This angle measures the weight-bearing surface of the acetabulum or
sourcil. A Tönnis angle >13° is considered to indicate hip
dysplasia (18). The intra- and
interobserver reproducibility of the Tönnis and CE angles are
reported to be satisfactory (19–21),
indicating that they are reliable measurements in clinical
practice.
The obliquity of the acetabular sourcil is directly
indicated by the Tönnis angle, and the clarity and relative
position of the medial edge of the acetabular sourcil on
radiographs can affect the measurement of the Tönnis angle. In this
study, 142 sourcils had blurred medial edges, accounting for ~31.7%
of all sourcils; these could not be used for Tönnis angle
measurements. One reason is that boney confluens may exist between
a thickened medial wall caused by heterotopic bone in the cotyloid
fossa and the medial margin of the acetabular sourcil (13). Another reason is that osteopenia in
acetabular subchondral bone was present on plain radiographs, due
to bone marrow edema (22).
Evidently, the measurement of the Tönnis angle occasionally became
impossible on account of the blurred medial edge of the sourcil,
and could be influenced by the relative position of the sourcil’s
medial edge; these could be considered to be limitations of the
Tönnis angle in the diagnosis of acetabular dysplasia.
In this study, all 448 hips, including 142 hips that
had blurred medial edges of the acetabular sourcils, were
successfully evaluated by the modified Tönnis angles. The upper
limit of the 95% reference range for the modified Tönnis angle was
11.73°, and the diagnosis of acetabular dysplasia could be made
when a modified Tönnis angle was >12°. Additionally, strong
negative or positive correlations existed between any two of the
CE, Tönnis and modified Tönnis angles, and the correlation between
the CE and modified Tönnis angles was the strongest. It is,
however, noteworthy that there are certain adverse factors,
including joint space narrowing (JSN) and subluxation of the hip,
which can lead to inaccurate measurement of the modified Tönnis
angle. The existence of JSN can cause a decrease in the value of
the modified Tönnis angle. In addition, subluxation of the hip can
increase the modified Tönnis angle or make the measurement of the
modified Tönnis angle impossible.
In conclusion, this study demonstrated that the
modified Tönnis angle was a feasible and available parameter for
radiographic evaluation of acetabular dysplasia, and could
substitute for the Tönnis angle without JSN or subluxation of the
hip, particularly when the Tönnis angle could not be measured due
to a blurred medial edge of the acetabular sourcil on pelvic
radiograph. Further studies are necessary to determine the
reliability of the modified Tönnis angle as a diagnostic parameter
of acetabular dysplasia.
Acknowledgements
The authors would like to thank Dr Feixue Zhang and
Dr Suhong Zhao for their assistance in the course of this
study.
References
|
1
|
Croft P, Cooper C, Wickham C and Coggon D:
Osteoarthritis of the hip and acetabular dysplasia. Ann Rheum Dis.
50:308–310. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jacobsen S and Sonne-Holm S: Hip
dysplasia: a significant risk factor for the development of hip
osteoarthritis. A cross-sectional survey. Rheumatology (Oxford).
44:211–218. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lau EM, Lin F, Lam D, Silman A and Croft
P: Hip osteoarthritis and dysplasia in Chinese men. Ann Rheum Dis.
54:965–969. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lequesne M, Malghem J and Dion E: The
normal hip joint space: variations in width, shape, and
architecture on 223 pelvic radiographs. Ann Rheum Dis.
63:1145–1151. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hartofilakidis G, Karachalios T and Stamos
KG: Epidemiology, demographics, and natural history of congenital
hip disease in adults. Orthopedics. 23:823–827. 2000.PubMed/NCBI
|
|
6
|
Weinstein SL: Natural history of
congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop
Relat Res. 225:62–76. 1987.PubMed/NCBI
|
|
7
|
Beltran LS, Rosenberg ZS, Mayo JD, et al:
Imaging evaluation of developmental hip dysplasia in the young
adult. AJR Am J Roentgenol. 200:1077–1088. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Angliss R, Fujii G, Pickvance E,
Wainwright AM and Benson MK: Surgical treatment of late
developmental displacement of the hip. Results after 33 years. J
Bone Joint Surg Br. 87:384–394. 2005.PubMed/NCBI
|
|
9
|
Terjesen T: Residual hip dysplasia as a
risk factor for osteoarthritis in 45 years follow-up of
late-detected hip dislocation. J Child Orthop. 5:425–431.
2011.PubMed/NCBI
|
|
10
|
Murphy SB, Ganz R and Müller ME: The
prognosis in untreated dysplasia of the hip. A study of
radiographic factors that predict the outcome. J Bone Joint Surg
Am. 77:985–989. 1995.PubMed/NCBI
|
|
11
|
Pereira F, Giles A, Wood G and Board TN:
Recognition of minor adult hip dysplasia: which anatomical indices
are important? Hip Int. 24:175–179. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Anderson LA, Gililland J, Pelt C, et al:
Center edge angle measurement for hip preservation surgery:
technique and caveats. Orthopedics. 34:862011.PubMed/NCBI
|
|
13
|
Brannon JK: Hip arthroscopy:
intra-articular saucerization of the acetabular cotyloid fossa.
Orthopedics. 35:e262–e266. 2012.PubMed/NCBI
|
|
14
|
Siebenrock KA, Kalbermatten DF and Ganz R:
Effect of pelvic tilt on acetabular retroversion: a study of pelves
from cadavers. Clin Orthop Relat Res. 407:241–248. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wiberg G: Studies on dysplastic acetabula
and congenital subluxation of the hip joint: With special reference
to the complication of osteo-arthritis. Acta Chir Scand. 83(Suppl
58): 5–135. 1939.PubMed/NCBI
|
|
16
|
Laborie LB, Engesæter IØ, Lehmann TG, et
al: Radiographic measurements of hip dysplasia at skeletal maturity
- new reference intervals based on 2,038 19-year-old Norwegians.
Skeletal Radiol. 42:925–935. 2013.PubMed/NCBI
|
|
17
|
Werner CM, Copeland CE, Ruckstuhl T, et
al: Relationship between Wiberg’s lateral center edge angle,
Lequesne’s acetabular index, and medial acetabular bone stock.
Skeletal Radiol. 40:1435–1439. 2011.
|
|
18
|
Lequesne M: Coxometry. Measurement of the
basic angles of the adult radiographic hip by a combined
protractor. Rev Rhum Mal Osteoartic. 30:479–485. 1963.(In
French).
|
|
19
|
Carlisle JC, Zebala LP, Shia DS, et al:
Reliability of various observers in determining common radiographic
parameters of adult hip structural anatomy. Iowa Orthop J.
31:52–58. 2011.PubMed/NCBI
|
|
20
|
Terjesen T and Gunderson RB: Reliability
of radiographic parameters in adults with hip dysplasia. Skeletal
Radiol. 41:811–816. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bouttier R, Morvan J, Mazieres B, et al:
Reproducibility of radiographic hip measurements in adults. Joint
Bone Spine. 80:52–56. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Malizos KN, Zibis AH, Dailiana Z, et al:
MR imaging findings in transient osteoporosis of the hip. Eur J
Radiol. 50:238–244. 2004. View Article : Google Scholar : PubMed/NCBI
|