Introduction
Infantile myofibromatosis (IM), a rare benign
neoplasm with an incidence of 1 in 400,000 (1), can occur at any organ, particularly
the skin or subcutaneous tissues or muscles (2,3). IM
is the most common fibrocellular tumor in infancy and childhood
(4–6). The features of the disease are
painless, solitary and congenital lesions (3). The diagnoses of IM by prenatal
ultrasound have been reported in seven previous studies (7–13);
however, its diagnosis by prenatal magnetic resonance imaging (MRI)
has been described in only one previous report (11). In addition, IM with ulcerated
plaque has been described in three case reports (2,14,15).
The present case report describes a case of IM with a
pseudo-ulcerated plaque that, to the best of our knowledge, has
never been reported before.
Case report
A 30-year-old female, gravida 1 para 1, was examined
conventionally by prenatal ultrasound in the 38th week of
gestation. The study was approved by the Medical Ethics Board of
The Second Hospital of Shandong University (Jinan, China). The
patient’s parents signed a statement of informed consent. A mass
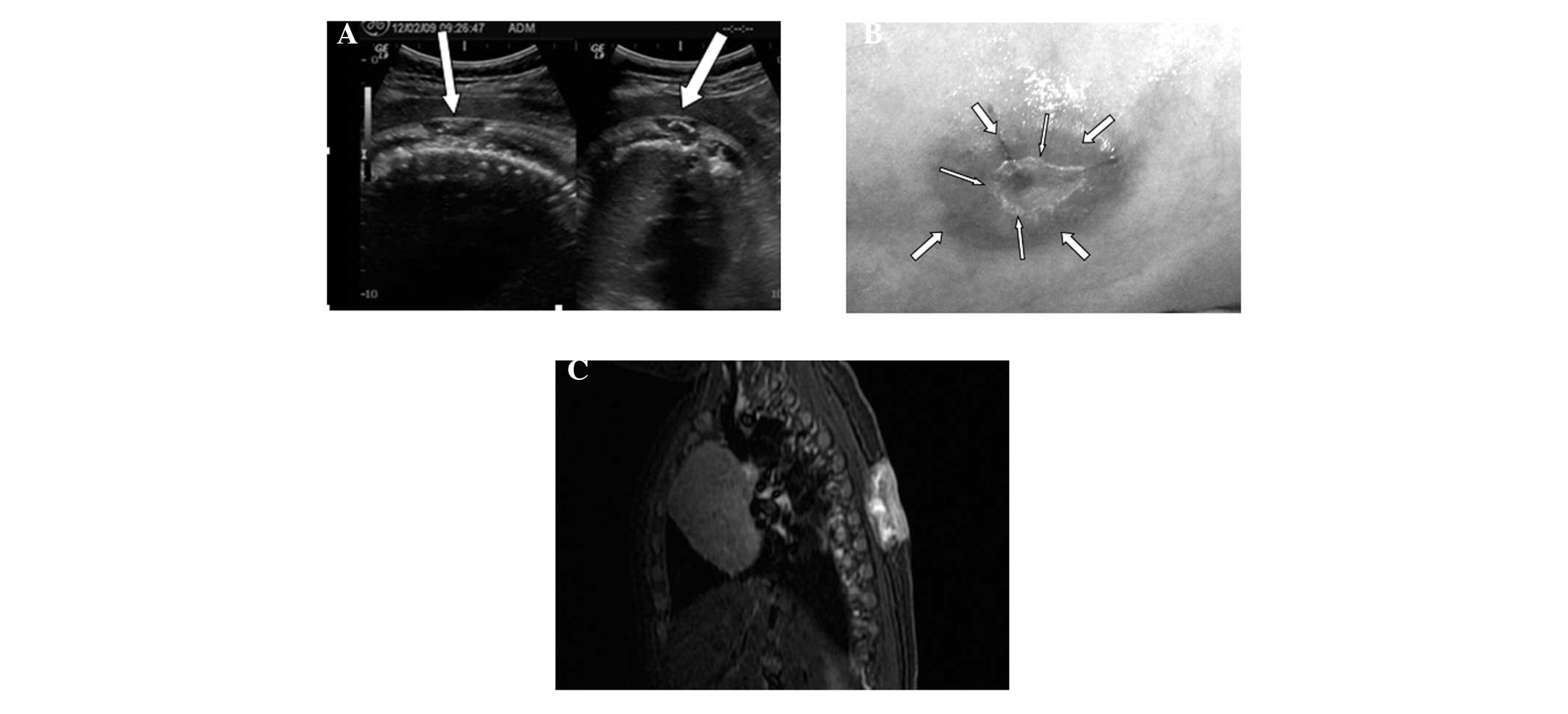
(2.4×2.2×1.1 cm in size) was discovered on the fetal right back
(T3-8), which was hypoechoic with sporadic hyperecho (Fig. 1A). Color Doppler flow imaging
(CDFI) showed intermittent blood flow inside and around the mass.
On the next day, MRI examination showed a normal result. The woman
gave birth to a boy in the 41st week of gestation. A scarlet mass
that was slightly elevated compared with the skin around it with a
cavity in the center, was observed on the right side of the back of
the newborn at birth. These characteristics suggested that the mass
was an ulcerated plaque; however, the mass was not actually an
ulcerated plaque according to the visual inspection. The surface of
the mass was white and intact, and was indicated to be a
pseudo-ulcerated plaque (Fig. 1B).
Physical examinations showed no abnormality. Considering that the
mass was congenital and might regress spontaneously, doctor
suggested that the parents should wait.
Three months later, the mass had increased in size,
and reached a size of 5.0×4.0×3.5 cm. It showed a clear boundary,
but no tenderness or activities. Ultrasound investigation showed a
subcutaneous hypoechoic tumor (3.8×3.2×2.4 cm) on the right side of
the back with a clear boundary and heterogeneous echogenicity
inside. In addition, calcification, an echoless region and invasion
of the erector spinae muscles were observed. CDFI showed
intermittent blood flow inside and around the tumor. MRI
demonstrated the presence of a mass under the subcutaneous soft
tissue on the right side of the back between T3-8 with a
heterogeneous or long T1 signal, equal or long T2 signal, and
heterogeneous high short time inversion recovery (STIR) signal,
implicating the right paraspinal muscle, but not canalis spinalis
(Fig. 1C). Three days later, the
mass was resected by surgery and sent for pathological study. The
surgery revealed that a tumor with a size of 5.0×4.0×3.0 cm was
present under the subcutaneous soft tissue, with a clear boundary
and invasion of erector spinae muscles. The mass was confirmed as
IM, with rare nuclear fission and unclear cell atypia. The results
of immunohistochemistry were as follows: smooth muscle actin (+)
and vimentin (+). Hematoxylin and eosin staining showed that the
myofibroblasts were arranged into a clustered or circinate
structure (Fig. 2). Two years
later, the patient was healthy with no recurrence of IM.
Discussion
IM is a type of rare mesenchymal tumor that
originates from myofibroblasts, with 88% IM patients being younger
than 2 years old (16). Male
patients account for 60.8% of all IM cases, while female patients
account for 39.2% (3). IM is
solitary or multicentric according to the number of lesions
(3). The solitary form of IM
usually occurs in the skin, subcutaneous tissues, muscles and the
skull, with good prognosis (3,16–19).
By contrast, the multicentric form of IM widely invades
subcutaneous muscles, bones and viscera (1,19,20).
Both solitary and multicentric forms of IM are associated with poor
prognosis if they affect viscera, particularly the heart, the lungs
and gastrointestinal tracts (9,13,18).
Ultrasound imaging characteristics of IM include stiffness,
encapsulation, calcification, liquefaction and signs of reduced
blood flow (4,21). To the best of our knowledge, a case
of IM with a pseudo-ulcerated plaque has never been reported in any
previous literature. The case of IM with pseudo-ulcerated plaque
sign discussed in the present report was solitary, and involved
skin, subcutaneous tissues and muscles. However, the patient
exhibited a good prognosis. The pathology of the white and
transparent surface was diagnosed as a cuticular layer. The imaging
features of the tumor shown by ultrasound, including a clear
boundary, calcification, liquefaction and two or three strips of
blood flow signals, were consistent with previous literature
(4). The infant was examined by
MRI prior to birth and surgery. MRI examination before birth did
not show the mass, probably because the tumor was too small to be
detected or the posture of the fetus was not appropriate for
examination. Although IM is congenital and the lesions usually
regress spontaneously in one or two years (18), the IM in the present case grew
larger after three months and thus surgery was performed. The
surgery may have been avoided if the newborn had been given a
long-term follow-up (3).
While IM can be diagnosed by prenatal ultrasound
(7–13), it is important to differentiate IM
from hemangioma, neurofibroma or desmoids (5). Although it is difficult to definitely
diagnose IM using prenatal ultrasound, it is possible to confirm
the location and numbers of IM lesions. If the tumor is single and
located in superficial organs, pregnancy can continue; if it is not
single and has infiltrated into other important viscera, the
pregnancy should be terminated. In summary, prenatal ultrasound can
be used to detect fetal lesions and to diagnose IM according to its
imaging features.
Acknowledgements
This study was supported by the Fourth People’s
Hospital of Jinan City and Shandong University.
References
|
1
|
Hausbrandt PA, Leithner A, Beham A, Bodo
K, Raith J and Windhager R: A rare case of infantile
myofibromatosis and review of literature. J Pediatr Orthop B.
19:122–126. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hocar O, Sab IA, Akhdari N, Amal S,
Ouladsiad M and Belaabidia B: Recurrent infantile myofibromatosis
in a 19-month-old boy presenting as ulcerated plaque. Skinmed.
11:371–373. 2013.PubMed/NCBI
|
|
3
|
Mashiah J, Hadj-Rabia S, Dompmartin A, et
al: Infantile myofibromatosis: a series of 28 cases. J Am Acad
Dermatol. 71:264–270. 2014. View Article : Google Scholar
|
|
4
|
Koujok K, Ruiz RE and Hernandez RJ:
Myofibromatosis: imaging characeristics. Pediatr Radiol.
35:374–380. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wiswell TE, Davis J, Cunningham BE,
Solenberger R and Thomas PJ: Infantile myofibromatosis: The most
common fibrous tumor of infancy. J Pediatr Surg. 23:315–318. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schurr P and Moulsdale W: Infantile
myofibroma: a case report and review of the literature. Adv
Neonatal Care. 8:13–20. 2008. View Article : Google Scholar
|
|
7
|
Arabin B, Hack K, Nooij L and Nikkels P:
Discrepant findings in a monoamniotic twin pregnancy affected by
infantile myofibromatosis. Ultrasound Obstet Gynecol. 33:488–490.
2009. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kubota A, Imano M, Yonekura T, Hirooka S,
Nose K, Oyanagi H and Nakayama M: Infantile myofibromatosis of the
triceps detected by prenatal sonography. J Clin Ultrasound.
27:147–150. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yeniel AO, Ergenoglu AM, Zeybek B, Kazandi
M, Akercan F, Ozcan C and Veral A: Prenatal diagnosis of infantile
myofibromatosis of the lung: a case report and review of the
literature. J Clin Ultrasound. 1:38–41. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guschmann M, Tönnies H, Bührer C, Mau H
and Vogel M: Myoid differentiation in mesoblastic nephroma:
clinicopathologic and cytogenetic findings of a rare case. J
Pediatr Surg. 37:E222002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Meizner I, Shalev J, Mashiach R, Vardimon
D and Ben-Raphael Z: Prenatal ultrasound diagnosis of infantile
myofibromatosis-a case report. Ultrasound Obstet Gynecol. 16:84–86.
2000. View Article : Google Scholar
|
|
12
|
Nishioka K, Seguchi T, Yamamura Y, et al:
Infantile myofibromatosis identified by fetal ultrasound. Br J
Dermatol. 140:539–541. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schurr P and Moulsdale W: Infantile
myofibroma: a case report and review of the literature. Adv
Neonatal Care. 8:13–20. 2008. View Article : Google Scholar
|
|
14
|
Delorme N, Doré MX, Croué A, Maillard H
and Verret JL: Unusual presentation of infantile myofibromatosis
with an ulcered plaque. Ann Dermatol Venereol. 132:338–341.
2005.PubMed/NCBI
|
|
15
|
Martí-Fajardo N, Ortega-Monzó C and
Navarro-Hervas M: Ulcerated congenital tumor. Solitary infantile
myofibromatosis. Actas Dermosifiliogr. 104:525–526. 2013.PubMed/NCBI
|
|
16
|
Enzinger FM and Weiss SW: Infantile
myofibromatosis. Soft Tissue Tumor. 1st edition. Mosby; St. Louis:
pp. 78–83. 1983
|
|
17
|
Engel M, Thiele O, Mechtersheimer G,
Hoffmann J, Freudlsperger C, Freier K and Castrillon-Oberndorfer G:
Solitary infantile myofibroma of the skull. J Craniofac Surg.
22:e66–e68. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Machan K, Bravo Bravo C, Martínez-León MI
and Affumicato L: Infantile myofibromatosis. Study of a case using
whole body ultrasound and MRI. Radiologia. 56:80–83. 2014.(In
Spanish).
|
|
19
|
Wu W, Chen J, Cao X, Yang M, Zhu J and
Zhao G: Solitary infantile myofibromatosis in the bones of the
upper extremities: Two rare cases and a review of the literature.
Oncol Lett. 6:1406–1408. 2013.PubMed/NCBI
|
|
20
|
Holzer-Fruehwald L, Blaser S, Rossi A,
Fruehwald-Pallamar J and Thurnher MM: Imaging findings in seven
cases of congenital infantile myofibromatosis with cerebral,
spinal, or head and neck involvement. Neuroradiology. 54:1389–1398.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dubois J, Garel L, David M and Powell J:
Vascular soft-tissue tumors in infancy: distinguishing features on
Doppler sonography. AJR Am J Roentgenol. 178:1541–1545. 2002.
View Article : Google Scholar : PubMed/NCBI
|