Introduction
Triple-negative breast cancer is a subtype of the
disease, in which estrogen receptor (ER), progesterone receptor
(PR) and human epidermal growth factor receptor-2 (Her-2) are not
expressed. Triple-negative breast cancer accounts for 10–17% of
total breast cancer cases (1). This
form of breast cancer is highly invasive and is associated with a
short survival time and poor patient prognosis (1). Conversely, triple-positive breast
cancer tissue expresses ER, PR and Her-2. Traditionally, breast
cancer ER refers to the estrogen receptor α (ERα), which is the
most important subtype of the ER. Traditional endocrine therapy is
targeted primarily against ERα and PR; however, only 40–70% of
breast tissue expresses ERα (2,3). In
1996, Kuiper et al observed that the estrogen receptor
subtype, estrogen receptor β (ERβ) was present in breast cancer
cells (4). Numerous studies
(5–7), including in vitro cell cultures,
animal models and immunohistochemical studies, have indicated that
ERβ is closely associated with breast cancer cell proliferation and
invasion. Thus, it may be possible to develop novel therapeutic
approaches for triple-negative breast cancer that traditionally do
not respond to endocrine therapy. Furthermore, previous studies
have indicated that ERα and ERβ expression levels vary among
different forms of breast cancer (8,9).
Patients with negative ERα expression also exhibit positive ERβ
expression (10).
In the present study, the expression levels of ERβ
were detected in 107 patients with triple-negative breast cancer
and 127 patients with triple-positive breast cancer in order to
determine the association between ERβ expression and the prognosis
of patients with triple-negative and triple-positive breast cancer.
In addition, the effect of ERβ expression on the survival rates of
breast cancer patients was analyzed.
Materials and methods
Clinical data
Primary cancer tissue samples were collected from
107 patients with triple-negative breast cancer and 127 patients
with triple-positive breast cancer, who had been hospitalized at
the First Affiliated Hospital of Xinjiang Medical University
(Ürümqi, China) between January 2000 and December 2010. The tissue
samples were paraffin-embedded, and complete follow-up data of the
patients were available. All the patients received standard
comprehensive cancer treatment, which included surgery,
anthracycline/taxane-based chemotherapy and radiotherapy. Patient
follow-up was conducted for 2–12 years, with a median follow-up
period of 3.5 years. During the follow-up period, nine patients
exhibited cancer recurrence and metastasis, while 26 patients
succumbed to the disease. All patients were female, with an age
range of 32–72 years and a median age of 49 years. Clinical data
were obtained via telephone or from the medical records of patients
who were regularly admitted to the hospital for review. The disease
progression-free survival (DFS) of the patients was defined as the
period between the date of cancer diagnosis to the first occurrence
of metastasis or cancer-associated mortality. During the follow-up
period, 10 patients with triple-negative breast cancer and 14
patients with triple-positive breast cancer were excluded. These
patients had succumbed to causes other than breast cancer, or had
been lost to follow-up at the time of last contact or prior to the
study cut-off point.
Prior written and informed consent was obtained from
each patient, and the study was approved by the Ethics Review Board
of Xinjiang Medical University (ürümqi, China).
Immunohistochemical analysis
Breast cancer tissue specimens were fixed in 10%
formaldehyde for 24 h, embedded in paraffin, sliced into 3-µm
sections and incubated overnight at 70°C. The sections were
subsequently dewaxed in xylene for 20 min and rehydrated in graded
alcohols. Endogenous peroxidase activity was blocked with 3%
hydrogen peroxide for 10 min. For antigen retrieval, the sections
were boiled in EDTA antigen retrieval solution for 20 min. After
cooling to room temperature and washing with phosphate-buffered
saline (PBS), the sections were incubated with a polyclonal rabbit
anti-human ERβ primary antibody (#BY-02101; Shanghai Yueyan
Biological Technology, Co., Ltd., Shanghai, China) at 37°C for 1 h
in the dark. Subsequently, the sections were incubated with a
horseradish peroxidase-conjugated anti-rabbit IgG secondary
antibody (Shanghai Gene Biological Technology Co., Ltd., Shanghai,
China) at 37°C for 30 min in the dark. Following incubation with
the antibodies, the sections were developed with
3,3-diaminobenzidine chromogenic reagent (Tianjin East Tengen Fine
Chemical Reagent, Tianjin, China) for 5 min and counterstained with
hematoxylin. Following hydrochloric acid differentiation and
dehydration in graded alcohols, the sections were mounted with
neutral gum (Tianjin East Tengen Fine Chemical Reagent). Positive
samples were used as the positive controls, while for the negative
control, the secondary antibody was replaced with PBS.
Immunohistochemical staining results were evaluated
by an experienced pathologist. Cells that exhibited brown staining
were considered to be ERβ-positive. Five fields were randomly
selected and observed under high magnification (DM LB2; Leica
Camera AG, Wetzlar, Germany). The ERβ expression rate was defined
as the ratio of the number of ERβ positive cells to the total
number of cells in each field. An ERβ rate <1% was defined as
ERβ negative [ERβ (-)] and an ERβ rate ≥1% was defined as ERβ
positive [ERβ (+)].
Statistical analysis
SPSS statistical software, version 17.0 (SPSS, Inc.,
Chicago, IL, USA) was used to analyze the data. Differences between
groups were compared using the χ2 test. The Kaplan-Meier
method was used for survival analysis, while the log-rank test was
performed to compare the differences in the survival rates. All
statistical tests were two-sided, and P<0.05 was considered to
indicate a statistically significant difference.
Results
Expression levels of ERβ in breast
cancer tissues
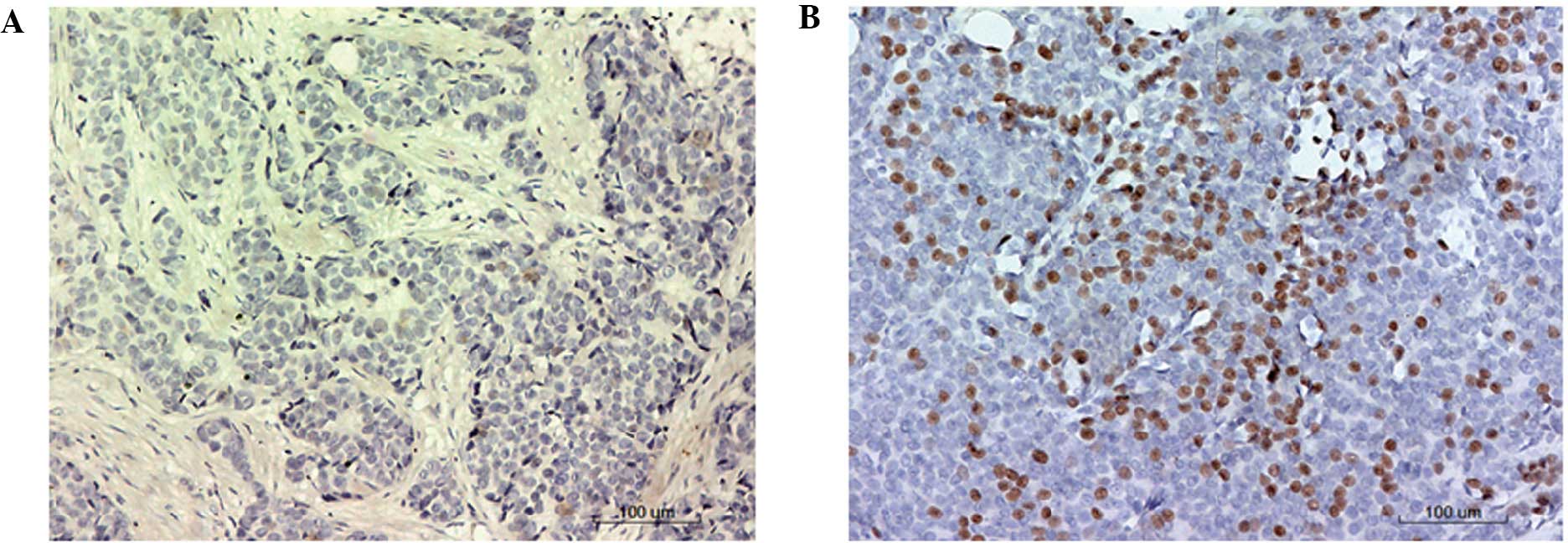
Immunohistochemical analysis was performed to
determine the levels of ERβ expression in the breast cancer tissue
samples. Representative immunohistochemical staining results are
presented in Fig. 1. Cells with
brown particles in the nucleus were considered to be ERβ-positive.
In the negative control group, no cells exhibited positive staining
(Fig. 1A). Cells exhibiting positive
ERβ staining are shown in Fig.
1B.
Rate of positive ERβ expression is
reduced in patients with triple-negative breast cancer
Among the study population, 101/234 cases of breast
cancer exhibited positive expression of ERβ (Table I); thus, the positive expression rate
was 43.2%. With regard to the triple-negative breast cancer
patients, 38/107 (35.5%) cases exhibited positive ERβ expression.
Furthermore, among the triple-positive breast cancer patients,
positive ERβ expression was observed in 63/127 (49.6%) cases.
Statistically, the triple-negative breast cancer patients exhibited
significantly lower expression levels of ERβ compared with the
triple-positive breast cancer patients (χ2=4.701,
P=0.03).
 | Table I.Expression of ERβ in patients with
triple-negative and triple-positive breast cancer. |
Table I.
Expression of ERβ in patients with
triple-negative and triple-positive breast cancer.
| Patients | ERβ positive, n
(%) | ERβ negative, n
(%) | Total (n) |
|---|
| Triple-positive | 63 (49.6) | 64 (50.4) | 127 |
| Triple-negative | 38 (35.5) | 69 (64.5) | 107 |
| Total | 101 (43.2) | 133 (56.8) | 234 |
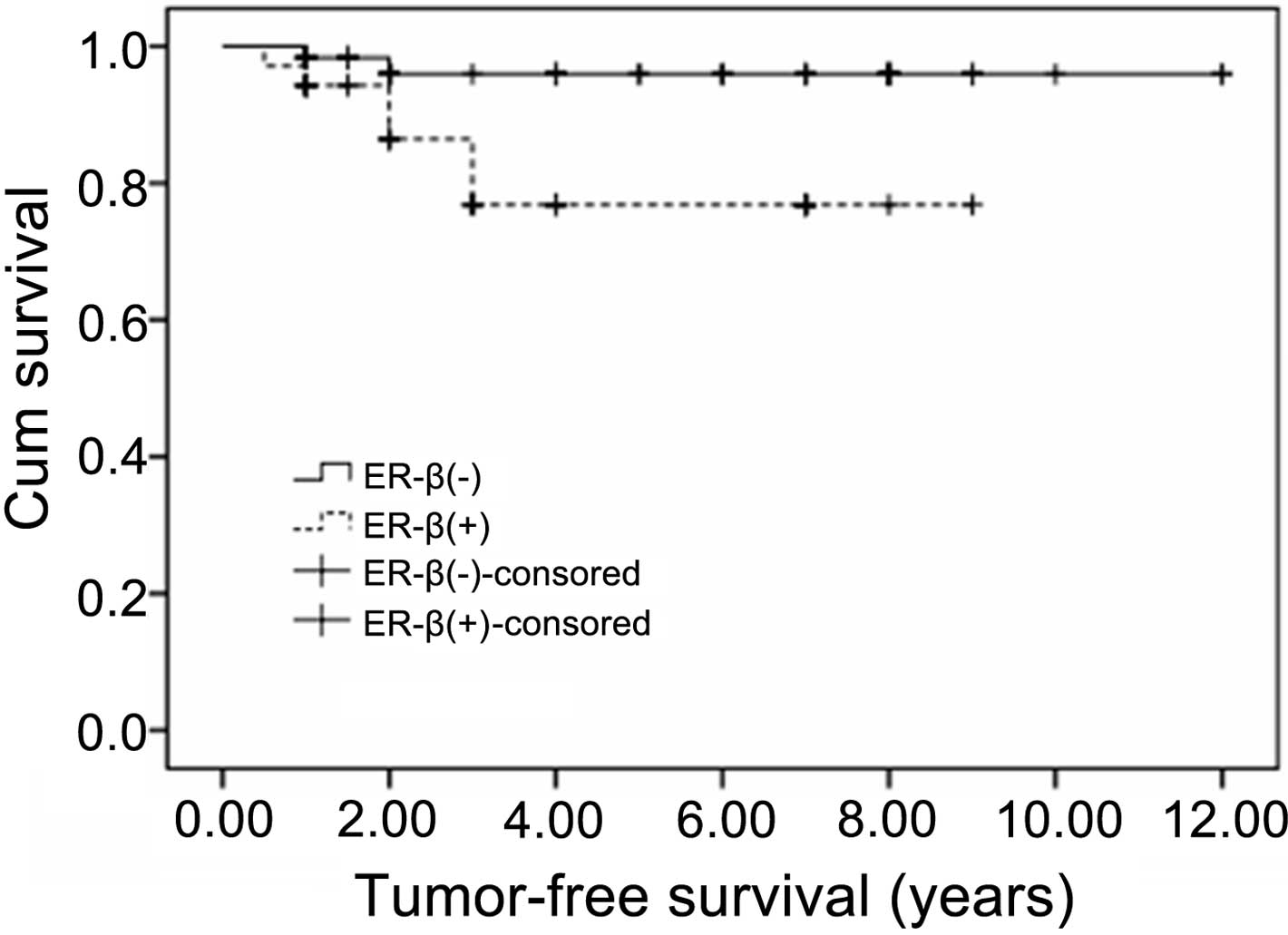
Triple-negative breast cancer patients
with positive ERβ expression exhibit reduced survival times
Survival analysis was performed using the
Kaplan-Meier method in order to investigate the association between
ERβ expression and survival times in the triple-negative breast
cancer patients. The Kaplan-Meier survival curve is shown in
Fig. 2. The survival rate of the
triple-negative breast cancer patients with negative ERβ expression
was higher compared with the triple-negative patients with positive
ERβ expression, and the difference was statistically significant
(χ2=5.330, P<0.05). In addition, at the end of the
follow-up period, the average DFS time for the triple-negative
breast cancer patients with negative ERβ expression was 10.620
years, which was significantly higher compared with the
triple-negative breast cancer patients with positive ERβ expression
(7.417 years; P<0.05). Thus, the prognosis of triple-negative
breast cancer patients with positive ERβ expression was
comparatively poor.
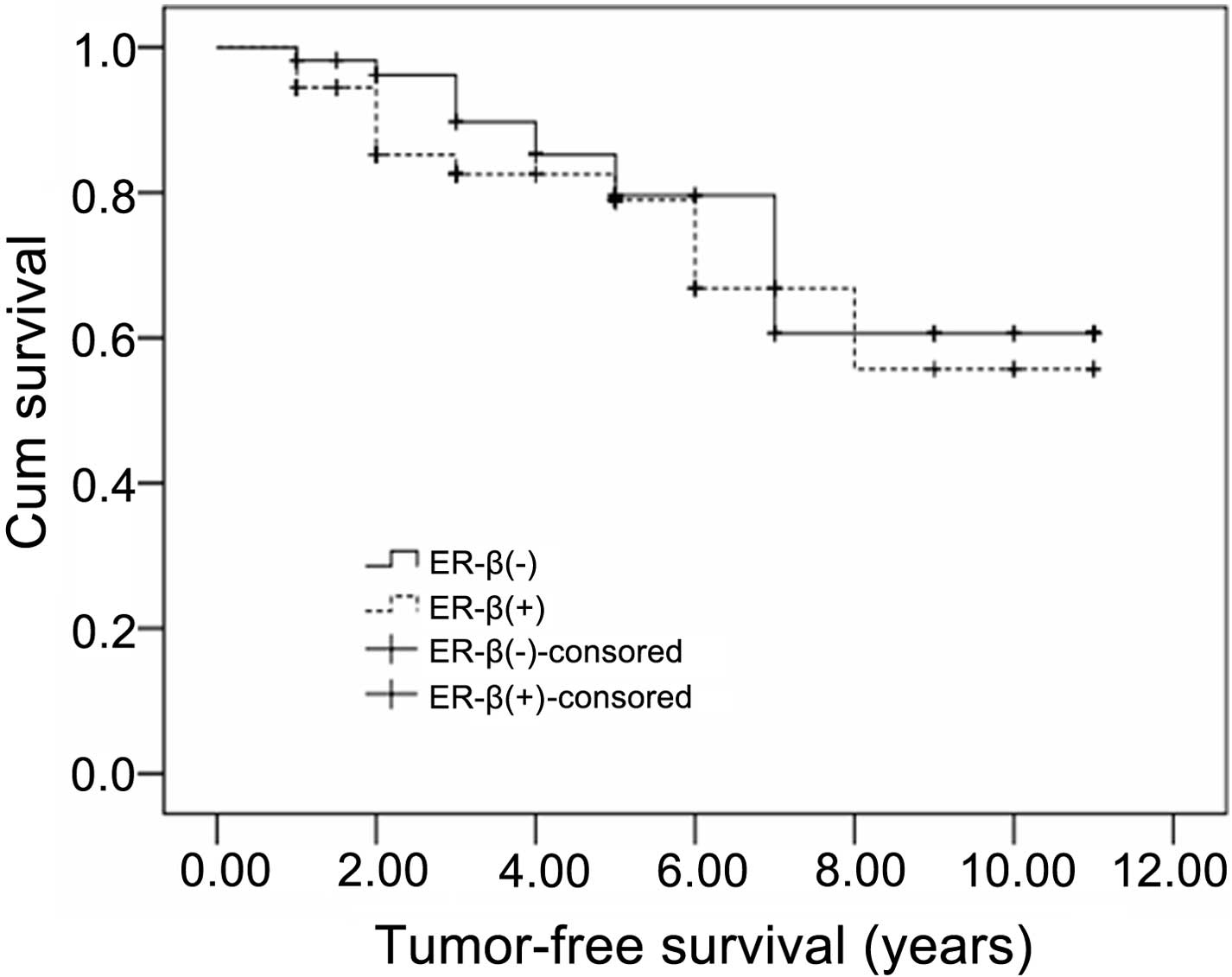
Survival rate of patients with
triple-positive breast cancer is not affected by ERβ
expression
Survival analysis was also conducted to determine
the association between ERβ expression and the survival rate in
triple-positive breast cancer patients. The Kaplan-Meier survival
curve for these patients is presented in Fig. 3. The expression of ERβ was
demonstrated to exert no effect on the survival times of the
triple-positive breast cancer patients. No statistically
significant difference was observed in the survival rate between
the triple-positive breast cancer patients with negative ERβ
expression and those with positive ERβ expression
(χ2=0.446, P>0.05). Therefore, the prognosis of
triple-positive breast cancer patients was not found to be
associated with ERβ expression.
Discussion
Triple-negative and triple-positive forms of breast
cancer are specific molecular subtypes of the disease of which the
triple-negative breast cancer subtype is more malignant.
Triple-negative breast cancer is associated with an increased rate
of malignancy due to the higher rates of local recurrence and
visceral metastasis (11,12). The ER belongs to the nuclear receptor
superfamily (8). The expression of
the ER subtype, ERα, in breast cancer is associated with
tumorigenesis and prognosis evaluation in breast cancer (9). In addition to ERα, an additional
primary ER subtype is ERβ. A previous study indicated that ERβ
expression is reduced in ductal carcinoma in situ and
invasive ductal carcinoma, which suggests that ERβ expression may
be associated with tumorigenesis and the degree of malignancy of
breast cancer (13). Furthermore, a
prior study indicated that the expression of ERβ is unaffected by
ERα expression (14).
In the present study, positive ERβ expression was
identified in 38/107 (35.5%) cases of triple-negative breast
cancer. By contrast, among the triple-positive breast cancer
patients, 63/127 (49.6%) cases were identified to express ERβ.
These results demonstrate that the rate of positive ERβ expression
in triple-negative breast cancer patients is significantly
decreased when compared with triple-positive breast cancer patients
(P<0.05).
Triple-negative breast cancer reportedly accounts
for 10–17% of all cases of breast cancer (15). At present, the function of ERβ in the
prognosis of breast cancer is contested (15,16). In
addition, there are few studies that have investigated the
association between the expression of ERβ and the prognosis of
patients with triple-negative breast cancer. In the present study,
the survival analysis indicated that there was no statistically
significant difference in the DFS time between the triple-positive
breast cancer patients with positive ERβ expression and those with
negative ERβ expression. This result suggests that the expression
of ERβ may not be a relevant prognostic factor for triple-positive
breast cancer patients. However, with regard to the triple-negative
breast cancer patients, those who exhibited positive ERβ expression
had significantly reduced DFS times when compared with those with
negative ERβ expression (P=0.021). This observation indicates that
ERβ expression may predict a poor prognostic outcome for patients
with triple-negative breast cancer. Previous studies demonstrated
that ERβ serves a crucial function in the regulation of tumor
angiogenesis, cell proliferation and lymphatic metastasis in breast
cancer (17–19). Jensen et al (20) detected the expression of ERβ and
tumor proliferation markers in breast cancer tissue using
immunohistochemistry. The authors observed that the expression of
the tumor proliferation markers was associated with the expression
of ERβ, indicating that ERβ expression is correlated with high
proliferative activity of tumor cells. This finding further
indicates that ERβ is a poor prognosis factor for breast cancer.
However, the role of ERβ as an indicator of poor prognosis in
patients with triple-negative breast cancer requires further
investigation.
In summary, ERβ expression levels in patients with
triple-negative breast cancer were lower compared with those in
patients with triple-positive breast cancer. The DFS time was
significantly reduced in the ERβ-positive patients with
triple-negative breast cancer, as compared with the ERβ-negative
patients. Thus, positive ERβ expression in triple-negative breast
cancer patients may indicate a poor prognosis. Therefore, ERβ may
be useful as a novel prognostic indicator for patients with
triple-negative breast cancer. However, further studies
investigating ERβ expression are required to improve understanding
of the progression of triple-negative breast cancer and to aid the
development of effective targets for the treatment of this
disease.
Acknowledgements
This study was supported by grants from the Natural
Science Foundation of Xinjiang Uygur Autonomous Region (no.
2011211A069) and the National Clinical Key Subject General Surgery
Construction Project.
References
|
1
|
Bauer KR, Brown M, Cress RD, Parise CA and
Caggiano V: Descriptive analysis of estrogen receptor
(ER)-negative, progesterone receptor (PR)-negative, and
HER2-negative invasive breast cancer, the so-called triple-negative
phenotype: A population-based study from the California cancer
Registry. Cancer. 109:1721–1728. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Arpino G, Weiss H, Lee AV, Schiff R, De
Placido S, Osborne CK and Elledge RM: Estrogen receptor-positive,
progesterone receptor-negative breast cancer: Association with
growth factor receptor expression and tamoxifen resistance. J Natl
Cancer Inst. 97:1254–1261. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shi X, Lin XY, Huang Y, Zhang ZF, Wang RX
and Zeng WC: Expressions of ER, PR, Her-2 in breast cancer. Zhong
Liu Yan Jiu Yu Lin Chuang. 21:461–462,465. 2009.[(In Chinese)].
|
|
4
|
Kuiper GG, Enmark E, Pelto-Huikko M,
Nilsson S and Gustafsson JA: Cloning of a novel receptor expressed
in rat prostate and ovary. Proc Natl Acad Sci USA. 93:5925–5930.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chang HG, Kim SJ, Chung KW, Noh DY, Kwon
Y, Lee ES and Kang HS: Tamoxifen-resistant breast cancers show less
frequent methylation of the estrogen receptor β but not the
estrogen receptor α gene. J Mol Med (Berl). 83:132–139. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cappelletti V, Celio L, Bajetta E, Allevi
A, Longarini R, Miodini P, Villa R, et al: Prospective evaluation
of estrogen receptor-β in predicting response to neoadjuvant
antiestrogen therapy in elderly breast cancer patients. Endocr
Relat Cancer. 11:761–770. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Esslimani-Sahla M, Kramar A,
Simony-Lafontaine J, Warner M, Gustafsson JA and Rochefort H:
Increased estrogen receptor betacx expression during mammary
carcinogenesis. Clin Cancer Res. 11:3170–3174. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Thomas C and Gustafsson JÅ: The different
roles of ER subtypes in cancer biology and therapy. Nat Rev Cancer.
11:597–608. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yager JD and Davidson NE: Estrogen
carcinogenesis in breast cancer. N Engl J Med. 354:270–282. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dotzlaw H, Leygue E, Watson PH and Murphy
LC: Expression of estrogen receptor-β in human breast tumors. J
Clin Endocrinol Metab. 82:2371–2374. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Young SR, Pilarski RT, Donenberg T,
Shapiro C, Hammond LS, Miller J, Brooks KA, Cohen S, Tenenholz B,
Desai D, et al: The prevalence of BRCA1 mutations among young women
with triple-negative breast cancer. BMC Cancer. 9:862009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dent R, Hanna WM, Trudeau M, Rawlinson E,
Sun P and Narod SA: Pattern of metastatic spread in triple-negative
breast cancer. Breast Cancer Res Treat. 115:423–428. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sengupta S, Sharma CG and Jordan VC:
Estrogen regulation of X-box binding protein-1 and its role in
estrogen induced growth of breast and endometrial cancer cells.
Horm Mol Biol Clin Investig. 2:235–243. 2010.PubMed/NCBI
|
|
14
|
Speirs V, Adams IP, Walton DS and Atkin
SL: Identification of wild-type and exon 5 deletion variants of
estrogen receptor beta in normal human mammary gland. J Clin
Endocrinol Metab. 85:1601–1605. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Reis-Filho JS and Tutt AN: Triple negative
tumours: A critical review. Histopathology. 52:108–118. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vinayagam R, Sibson DR, Holcombe C, Aachi
V and Davies MP: Association of oestrogen receptor beta 2 (ER beta
2/ER beta cx) with outcome of adjuvant endocrine treatment for
primary breast cancer - a retrospective study. BMC Cancer.
7:1312007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Järvinen TA, Pelto-Huikko M, Holli K and
Isola J: Estrogen receptor β is coexpressed with ERα and PR and
associated with nodal status, grade, and proliferation rate in
breast cancer. Am J Pathol. 156:29–35. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hou YF, Yuan ST, Li HC, Wu J, Lu JS, Liu
G, Lu LJ, Shen ZZ, Ding J and Shao ZM: ERβ exerts multiple
stimulative effects on human breast carcinoma cells. Oncogene.
23:5799–5806. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Knowlden JM, Gee JM, Robertson JF, Ellis
IO and Nicholson RI: A possible divergent role for the oestrogen
receptor α and β subtypes in clinical breast cancer. Int J Cancer.
89:209–212. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jensen EV, Cheng G, Palmieri C, Saji S,
Mäkelä S, Van Noorden S, Wahlström T, Warner M, Coombes RC and
Gustafsson JA: Estrogen receptors and proliferation markers in
primary and recurrent breast cancer. Proc Natl Acad Sci USA.
98:15197–15202. 2001. View Article : Google Scholar : PubMed/NCBI
|