Introduction
Acute type A aortic dissection (AD) can sometimes
involve the ostium of the coronary artery, leading to acute
myocardial infarction (AMI). It is possible for the clinical
symptoms of acute AD and AMI to be similar, which makes an accurate
diagnosis of AD difficult. Furthermore, once the exact diagnosis is
validated, management of the condition is controversial, as there
are only a few reports in the literature and no current guidelines
for treatment. The present report describes a case of acute AD with
the typical presentation of acute inferior MI and cardiogenic shock
that was diagnosed by inserting the catheter into a false lumen
during coronary angioplasty and was successfully treated with right
coronary ostial occlusion stenting as a bridge for surgery. To
date, there are few reports that have described AD in combination
with AMI treated by stenting (1–8). Among
these reports, only one described a case of acute AD complicated by
AMI that was similarly diagnosed by accidentally inserting the
catheter into a false lumen during catheterization (9).
Case report
A 51-year-old man with a history of hypertension was
transferred to the Emergency Department following the sudden onset
severe chest pain, which lasted 7 h. The patient had been diagnosed
with AMI and accepted thrombolytic therapy with urokinase in the
local hospital and was then transferred to the First Affiliated
Hospital of Jilin University (Changchun, China) in order to undergo
a primary percutaneous coronary intervention (PCI). The blood
pressure of the patient was at 86/60 mmHg with continuous dopamine
administration (5 µg/kg/min) and his heart rate was 82 bpm. Other
physical examination findings appeared normal, with the pulse
within the normal range and no aortic regurgitation; however, the
electrocardiograms (ECGs) showed a marked ST-segment elevation in
leads II, III, aVF, V3R-V5R and a reciprocal
ST-segment depression in lead V4-V6 (Fig. 1). The levels of cardiac troponin I
and D-dimers were also elevated. The personnel of the Emergency
Department considered the diagnosis of AMI and therefore referred
the patient directly to the catheterization laboratory.
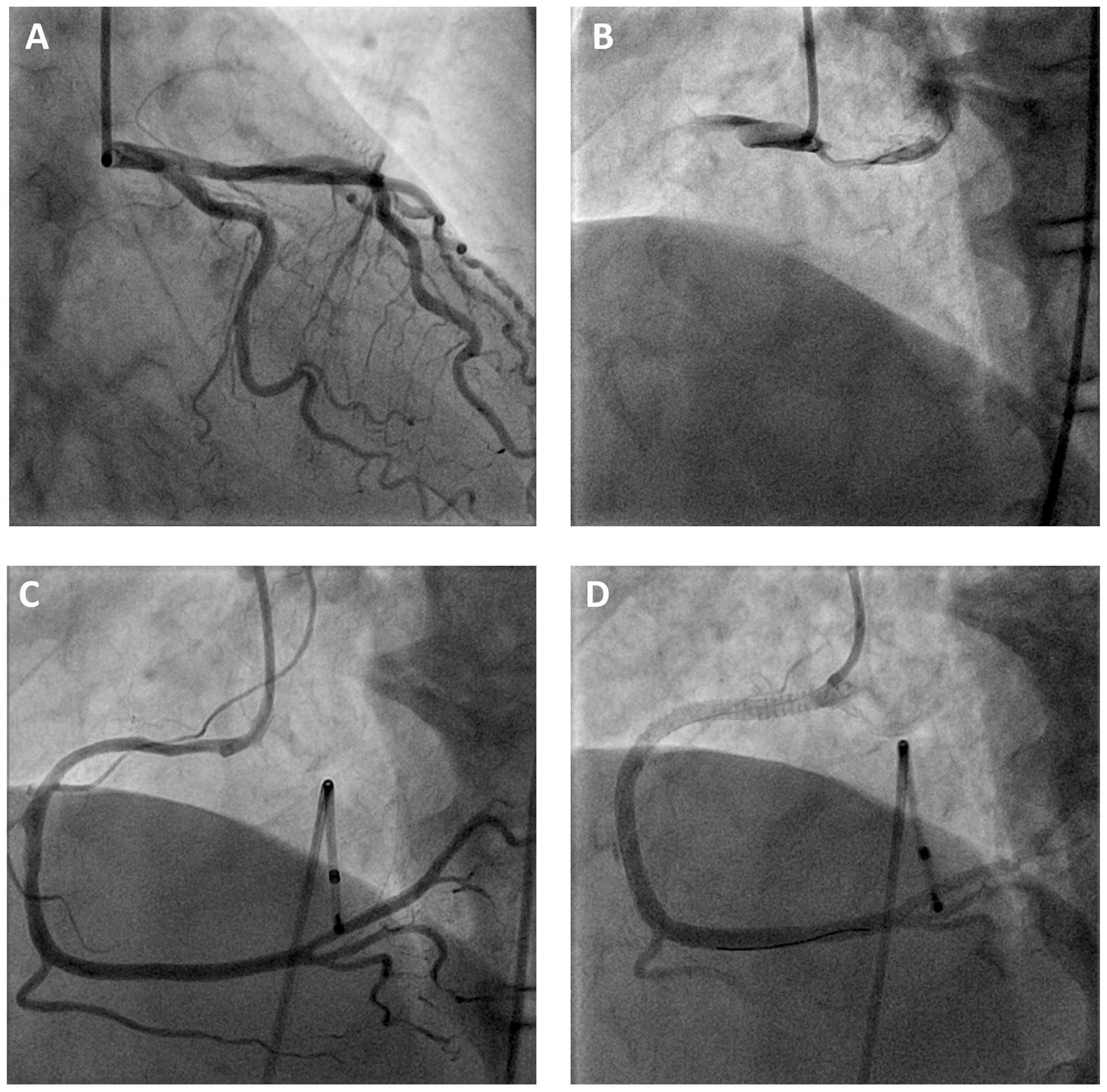
During primary coronary angioplasty, the left
coronary arteries were found to be normal (Fig. 2A), while the right coronary artery
(RCA) was completely occluded (as found later, the catheter was in
the wrong lumen) (Fig. 2B). Stent
implantation was subsequently attempted by placing a guiding
catheter into the true lumen (Fig.
2C), which, instead of showing RCA stenosis, revealed
dissection over the ostium of the RCA, indicating the diagnosis of
AD. In order to promote rapid recovery from the cardiogenic shock,
primary angioplasty was performed using the implantation of three
drug-eluting stents in the RCA that reached the ostium. Following
treatment by direct stenting, the anterograde coronary blood flow
was completely restored and myocardial perfusion improved (Fig. 2D). Following the procedure, the
cardiac hemodynamics of the patient were also stabilized. As a
result, the dose of dopamine was gradually reduced, as the patient
had a blood pressure of 110/70 mmHg while on continuous dopamine at
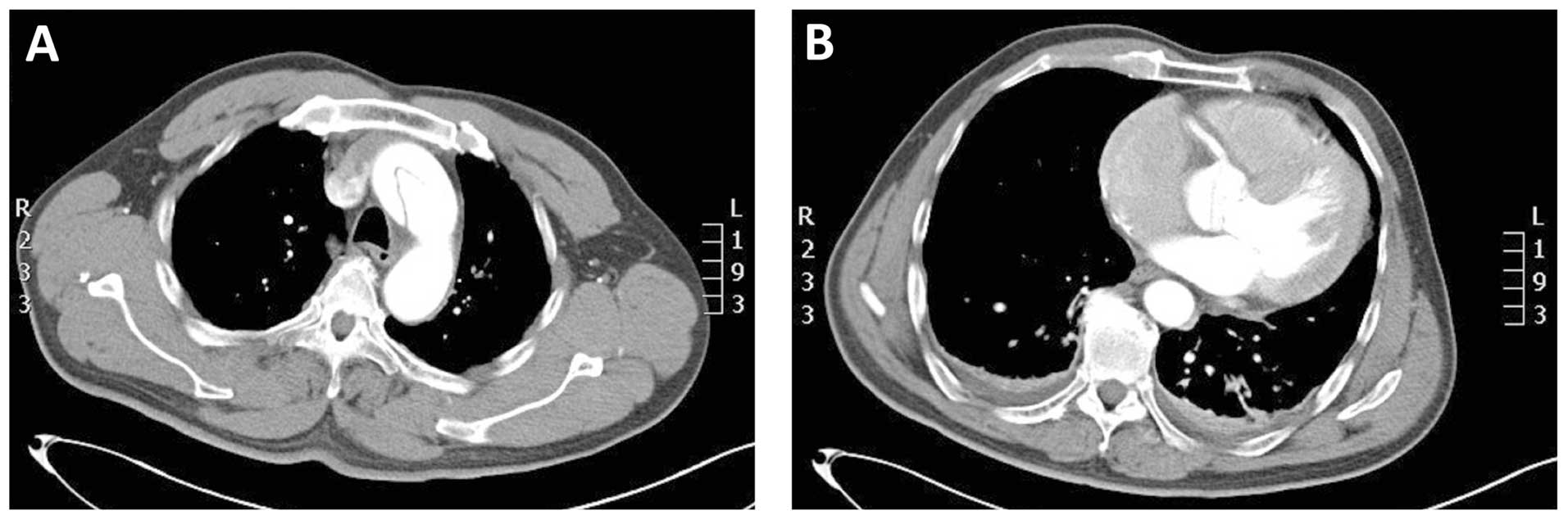
a dose of 3 µg/kg/min. Aortic computed tomography angiography
revealed Stanford type A AD (Fig. 3A and
B). The patient was then immediately transferred to the
Department of Cardiac Surgery, which confirmed the diagnosis of
dissection of the ascending aorta with involvement of the RCA. A
tetrafurcated graft with stented elephant trunk implantation (Sun's
procedure) was used, followed by surgical replacement of the
partial ascending aorta and aortic arch under stable hemodynamic
conditions. Following surgery, the patient was stabilized and
shortly admitted to the Intensive Care Unit.
Discussion
Complications of acute AD in the setting of AMI are
relatively rare, with a reported incidence of 1–3% (10,11). The
present study reported a case of acute AD combined with AMI, which
was successfully treated by coronary artery stenting. The diagnosis
of acute inferior and right ventricular MI was determined based on
the clinical symptoms of the patient, the ST-segment elevation
observed via ECG and the elevated serum levels of troponin. Τhe
guiding catheter was accidentally placed in a false lumen and the
dissection was noted, since stenosis was absent in the RCA when the
catheter was inserted into the true lumen and dissection over the
ostium of the RCA was revealed. In this case, the possibility of
iatrogenic coronary dissection was ruled out. To promote rapid
recovery from the cardiogenic shock, a direct PCI was performed as
a bridge to further surgical interventions. In cases such as the
present one, in which the patient exhibits shock, a correct
diagnosis may be even more difficult to make, and direct stenting
may be required to save the patient's life during angioplasty.
In previous years, a limited number of cases of
Stanford type A AD in combination with MI that were treated with
coronary stenting have been reported (1–8).
Furthermore, only one case was diagnosed in a similar manner to the
patient described in the present study (9). Physicians should therefore be aware of
primary and secondary ischemic heart diseases that are complicated
by AD. Thorough physical examinations along with transthoracic
echocardiograms should be performed before catheterization to
exclude Stanford type A AD with AMI. Once the correct diagnosis is
validated, a treatment strategy should be determined. Surgery has
been recommended as the treatment of choice for patients with
typical acute type A AD (12);
however in cases of hemodynamic instability due to the complication
of AMI, as is in the present case, a primary PCI should be
considered as a bridge approach to not only stabilize the cardiac
hemodynamics of the patient but also gain some time before surgery
can be performed.
Acknowledgements
The authors would like to thank Medjaden Bioscience
Limited (Hong Kong SAR, China) for their assistance in the
preparation of this manuscript.
References
|
1
|
Cardozo C, Riadh R and Mazen M: Acute
myocardial infarction due to left main compression aortic
dissection treated by direct stenting. J Invasive Cardiol.
16:89–91. 2004.PubMed/NCBI
|
|
2
|
Barabas M, Gosselin G, Crépeau J,
Petitclerc R, Cartier R and Théroux P: Left main stenting - as a
bridge to surgery - for acute type A aortic dissection and anterior
myocardial infarction. Catheter Cardiovasc Interv. 51:74–77. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yunoki K, Naruko T, Itoh A, et al:
Stenting of right coronary ostial occlusion due to thrombosed type
A aortic dissection: One-year follow-up results. J Cardiol.
1:e166–e170. 2010.
|
|
4
|
Shimamura J, Kubota H, Tonari K, et al:
Acute aortic dissection with left main coronary malperfusion
treated with precedent stenting followed by a definitive surgery.
Kyobu Geka. 63:537–541. 2010.(In Japanese). PubMed/NCBI
|
|
5
|
Ohara Y, Hiasa Y and Hosokawa S:
Successful treatment in a case of acute aortic dissection
complicated with acute myocardial infarction due to occlusion of
the left main coronary artery. J Invasive Cardiol. 15:660–662.
2003.PubMed/NCBI
|
|
6
|
Lentini S, Specchia L, Cricco A, et al:
Hybrid management of acute type A aortic dissection presenting as
acute coronary syndrome. Int J Cardiol. 167:e85–e87. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ravandi A and Penny WF: Percutaneous
intervention of an acute left main coronary occlusion due to
dissection of the aortic root. JACC Cardiovasc Interv. 4:713–715.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Camaro C, Wouters NT, Gin MT and Bosker
HA: Acute myocardial infarction with cardiogenic shock in a patient
with acute aortic dissection. Am J Emerg Med. 27:8992009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chan KC, Wu DJ, Ueng KC, et al: Acute
aortic dissection developing acute myocardial infarction diagnosed
by accidentally inserting the catheters into the false lumen during
catheterization: A pitfall and rare image. Jpn Heart J. 44:583–585.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
DeSanctis RW, Doroghazi RM, Austen WG and
Buckley MJ: Aortic dissection. N Engl J Med. 317:1060–1067. 1987.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Neri E, Toscano T, Papalia U, et al:
Proximal aortic dissection with coronary malperfusion:
Presentation, management, and outcome. J Thorac Cardiovasc Surg.
121:552–560. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Prêtre R and Von Segesser LK: Aortic
dissection. Lancet. 349:1461–1464. 1997. View Article : Google Scholar : PubMed/NCBI
|