Introduction
Viral encephalitis is an inflammation of the central
nervous system caused by a specific virus. The prognosis is often
good if treated early. Acute retinal necrosis syndrome (ARN) is a
viral infection characterized by retinal focal necrosis (1). A previous study reported an incidence
of 1 case of ARN per 1.6–2.0 million population (2). ARN is a viral inflammatory condition
that manifests with vitreitis, severe retinal vasculitis and
progressive peripheral retinal necrosis (3). Previous studies have shown that ARN may
exist concurrently with viral encephalitis (4,5). The
present study describes the case of a patient with viral
encephalitis complicated by bilateral ARN. Written informed consent
was obtained from the patient. The case report and a review of the
literature were subsequently utilized to investigate the possible
pathogenesis of this disease.
Case report
A 44-year-old male patient was admitted to the
Department of Neurology in the Affiliated Yantai Yuhuangding
Hospital of Qingdao University Medical College (Yantai, China) on
June 2, 2012 with a fever and headache that had persisted for 12
days, and confusion and divagation that had lasted for 1 day. The
patient had no remarkable clinical or family history and had no
history of drug allergies. Physical examination revealed that the
patient was restless, irritable, had neck stiffness and was
positive for Kernig's sign. The patient's deep tendon reflexes were
normal and no paresis was present. Blood chemistry and urinalysis
tests were normal. The results from the cerebrospinal fluid (CSF)
analysis were as follows: leucocytes, 805.3 mg/l; monocytes (90%),
130×106/l; and herpes simplex virus I (HSV-I)
immunoglobulin M, positive. Polymerase chain reaction analysis
revealed positive results for HSV in the CSF and blood, while tests
for cytomegalovirus (CWV) allotype, human immunodeficiency virus
and hepatitis C were negative. The culture of CSF produced no
acid-fast bacilli, common bacteria or Cryptococci. Based on
these results, the patient was diagnosed with viral encephalitis
and administered antiviral therapy (500 mg acyclovir intravenously
every 8 h, dropwise).
Following antiviral therapy, the general condition
of the patient improved; however, on June 6, 2012 he presented with
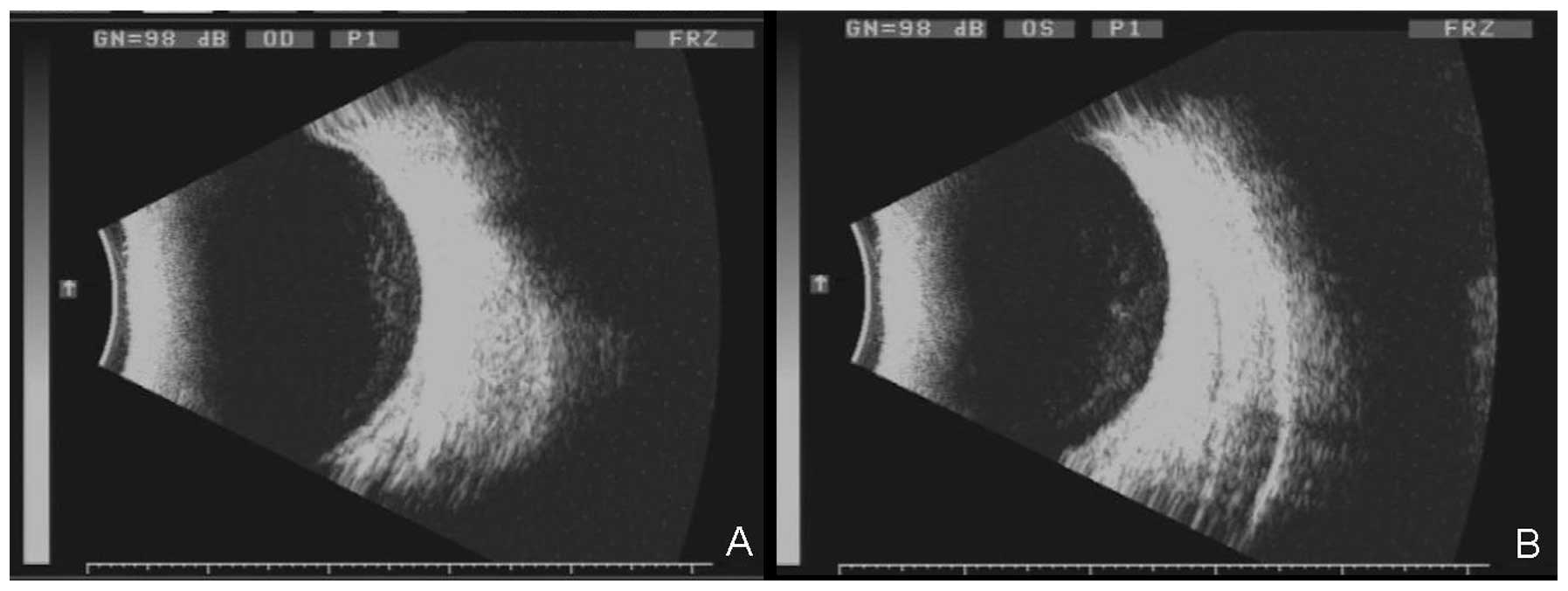
blurred vision. Ophthalmological examinations revealed mild
opacification of the lenses and moderate opacification of the
vitreous body. The fundus appeared hazy and had blurred disc
margins. Ophthalmic ultrasound showed a dense hypoechoic focal
lesion (Fig. 1). The mean visual
evoked potential amplitude was slightly decreased and the
time-to-peak was substantially prolonged. Methylprednisolone pulse
therapy (1.0 g/day) was administered for three days, followed by
orally administered prednisone. A second ophthalmological
examination (June 16, 2012) revealed that vitreous opacification
was present in both eyes. The majority of the retinal artery was
occluded, particularly in the left eye. Retinal necrotic lesions
with mild bleeding were visible.
The examination results confirmed the patient had
viral encephalitis with bilateral ARN, and retinal laser treatment
was administered. Two days after retinal laser treatment, visual
acuity had improved. The CSF tests (June 18, 2012) were found to be
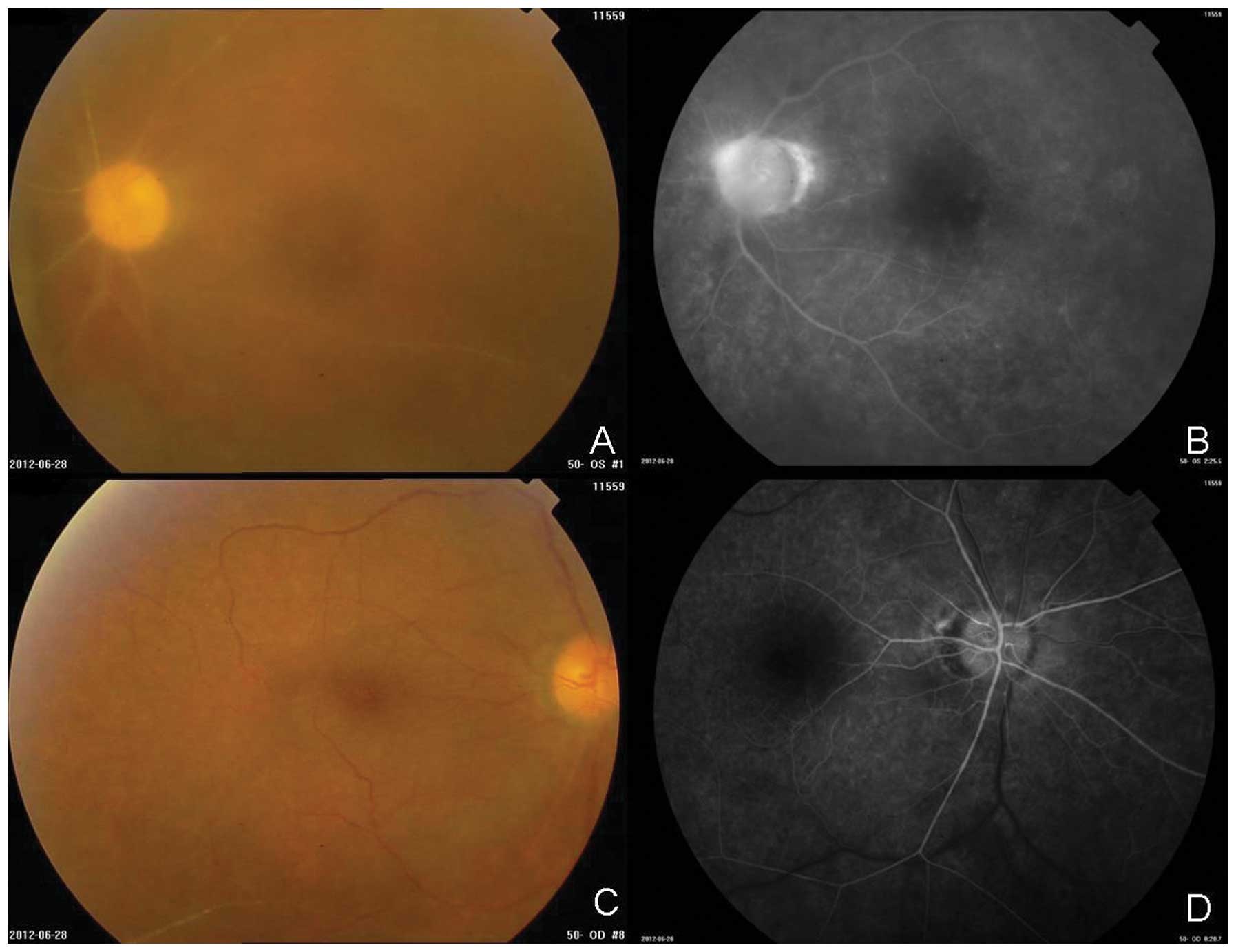
normal. Fluorescein fundus angiography revealed that the majority
of the retinal artery, shown as a white line, was occluded,
particularly in the left eye (Fig.
2). Retinal necrotic lesions, together with mild bleeding, were
visible along the white line. Visual acuity was markedly improved
following treatment.
Discussion
Viral meningitis complicated by ARN is relatively
rare, and is most common in immunocompromised individuals.
Bilateral eye involvement occurs only in approximately one-third of
patients with ARN (6). The present
case study involved an adult male with viral encephalitis
complicated by bilateral ARN. The mechanism by which viruses induce
ARN has yet to be elucidated; however, it has been suggested that
the virus may be transmitted along the brain-optic nerve
axon-retina pathway (7,8).
Viral encephalitis may be an important risk factor
for ARN. ARN syndrome is known to occur occasionally alongside, or
shortly after, herpetic encephalitis (9). A review of the available literature
(10), as well as our own
observations, indicates that there is no universal guideline on how
long antiviral and anti-inflammatory treatment should be continued.
Early retinal laser treatment may prevent retinal detachment in
patients with ARN (11). At present,
a full course of antiviral therapy is essential to prevent the
development of ARN as a result of viral encephalitis, as well as to
prevent the progression of ARN from one eye to the other (12). Systemic glucocorticoids may alleviate
retinal inflammation, and have also been shown to protect the
retina and optic nerve. Prophylactic laser coagulation of retinal
defects and margins may also prevent retinal detachment (13).
In conclusion, if a patient with viral encephalitis
experiences decreased visual acuity or has vitreous opacification,
the possibility of ARN should be considered. Fundus fluorescein
angiography should be performed and early active treatment should
be applied.
References
|
1
|
Kanoff J and Sobrin L: New diagnosis and
treatment paradigms in acute retinal necrosis. Int Ophthalmol Clin.
51:25–31. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Muthiah MN, Michaelides M, Child CS and
Mitchell SM: Acute retinal necrosis: a national population-based
study to assess the incidence, methods of diagnosis, treatment
strategies and outcomes in the UK. Br J Ophthalmol. 91:1452–1455.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lau CH, Missotten T, Salzmann J and
Lightman SL: Acute retinal necrosis features, management, and
outcomes. Ophthalmology. 114:756–762. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vandercam T, Hintzen RQ, de Boer JH and
Van der Lelij A: Herpetic encephalitis is a risk factor for acute
retinal necrosis. Neurology. 71:1268–1274. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Klein A and Lefebvre P: Three consecutive
episodes of acute retinal necrosis due to herpes simplex-1 over
twelve years following herpetic encephalitis. Ocul Immunol Inflamm.
15:411–413. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gartry DS, Spalton DJ, Tilzey A and Hykin
PG: Acute retinal necrosis syndrome. Br J Ophthalmol. 75:292–297.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cardine S, Chaze PA, Bourcier F, et al:
Bilateral acute retinal necrosis syndrome associated with
meningoencephalitis caused by herpes simplex virus 2. A case
report. J Fr Ophtalmol. 27:795–800. 2004.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Arruti M, Aldazabal M, Blanco A, et al:
Acute herpes simplex virus type 1 retinal necrosis three years
after herpes simplex encephalitis. Rev Neurol. 58:45–46. 2014.(In
Spanish). PubMed/NCBI
|
|
9
|
Gaynor BD, Wade NK and Cunningham ET Jr:
Herpes simplex virus type 1 associated acute retinal necrosis
following encephalitis. Retina. 21:688–690. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Flaxel CJ, Yeh S and Lauer AK: Combination
systemic and intravitreal antiviral therapy in the management of
acute retinal necrosis syndrome (an American Ophthamological
Society thesis). Trans Am Ophthalmol Soc. 111:133–144.
2013.PubMed/NCBI
|
|
11
|
Kianersi F, Masjedi A and Ghanbari H:
Acute retinal necrosis after herpetic encephalitis. Case Rep
Ophthalmol. 1:85–89. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tibbetts MD, Shah CP, Young LH, et al:
Treatment of acute retinal necrosis. Ophthalmology. 117:818–824.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Verma L, Venkatesh P, Satpal G, Rathore K
and Tewari HK: Bilateral necrotizing herpetic retinopathy three
years after herpes simplex encephalitis following pulse
corticosteroid treatment. Retina. 19:464–467. 1999. View Article : Google Scholar : PubMed/NCBI
|