Introduction
Acinetobacter baumannii (A.
baumannii), a non-fermenting bacteria, is the known conditioned
pathogen leading to noso-comial infection, which exists widely in
nature and the hospital environment and is the only Gram-negative
bacillus which can survive for weeks on human skin (1). With the wide use of immunosuppressive
drugs, the increase in invasion surgeries and the development of
intensive care technology (2), an
increasing number of A. baumannii infections have been
detected. Multi-drug resistance and the amplification of resistance
to A. baumannii have increased the mortality rate in the
clinic (3). Resistance to
antibiotics against A. baumannii mostly occurs due to the
loss of membrane proteins, active efflux mechanisms, changes in
penicillin-binding proteins (PBPs) and the production of various
enzymes, amongst which the production of β-lactamases plays an
important role in the resistance to β-lactam antibiotics (5). Both domestic and foreign studies have
suggested the severe drug resistance to A. baumannii
(4). The aim of the present study
was to perform a genetic test and drug resistance analysis for the
AmpC enzyme in A. baumannii isolated from tertiary-level
hospitals in the Xuzhou region, China by polymerase chain reaction
(PCR), to strengthen the study of drug resistance genes, which is
of great significance ot understand the distribution of gene type
to control and treat infections caused by A. baumannii. The
findings of our study may facilitate and provide guidelines for the
rational clinical use of antibiotics and the prevention and
epidemic control of the drug-resistant bacterium, A.
baumannii.
Materials and methods
Materials
A total of 134 clinical isolates of non-repetitive
A. baumannii were collected from patients at the First
People's Hospital, Affiliated to Xuzhou Medical College, Central
Hospital in Xuzhou, China, from August 2012 to November 2012. The
Escherichia coli ATCC 25922 strain was employed as a
negative quality control, while Enterobacter cloacae was
employed as a positive quality control. The VITEK® 2 Compact system
was obtained from bioMérieux, Inc., Craponne, France; the Gel
Imaging System was from Tianneng, Shanghai, China; the GeneAmp PCR
System was purchased from Biometra GmbH, Goettingen, Germany; the
Electrophoresis System was from Beijing Liuyi Instrument Plant,
Beijing, China; the Mueller-Hinton (MH) was from Oxoid,
Basingstoke, UK; the Ex Taq enzyme, dNTPs and the DNA Marker 1200
were from Tiangen Biotech, Beijing, China (http://www.tiangen.com/); and agarose and ethidium
bromide were from Sigma, St. Louis, MO, USA.
Methods
Clinical samples were cultured in blood agar culture
medium at 35°C for 18–24 h. The identification of the bacteria was
carried out according to the ‘National Clinical Laboratory
procedures’. All strains were tested for drug sensitivity analysis
with the Gram-negative bacteria GN and AST GN-13 identification of
the French Merieux automatic bacteria Vitek-2 identification
system.
According to the instructions provided with the
bacteria DNA extracting kit (Tiangen Biochemical Technology Co.,
Ltd., Beijing, China), DNA samples of the clinical strains were
extracted as a PCR template. The primers used for PCR amplification
(7 pairs created by Shenggong Corp., Shanghai, China) were as
previously reported (6,7) and are presented in Table I. PCR was performed with a final
volume of 25 µl. The PCR program consisted of an initial
denaturation step at 94°C for 3 min, followed by 28 cycles of DNA
denaturation at 94°C for 30 sec, primer annealing at 56°C for 30
sec, and primer extension at 72°C for 1 min. After the final cycle,
a final extension step at 72°C for 7 min was added. The PCR product
was analyzed by gel electrophoresis on 1.5% agarose gels. The gels
were stained with ethidium bromide at 0.5 µg/ml and visualized
using a UV transillumination imaging system (Furi Technology Co.,
Ltd., Shanghai, China).
 | Table I.PCR primer sequences and target
genes. |
Table I.
PCR primer sequences and target
genes.
| Genes | Primer sequences
(5′→3′) | Expected
amplification size (bp) |
|---|
|
blaADC | P1:
TAAACACCACATATGTTCCG | 663 |
|
| P2:
ACTTACTTCAACTCGCGACG |
|
|
blaMOX | P1: GCT GCT CAA GGA
GCA CAG GAT | 520 |
|
| P2: CAC ATT GAC ATA
GGT GTG GTG C |
|
|
blaCIT | P1: TGG CCA GAA CTG
ACA GGC AAA | 462 |
|
| P2: TTT CTC CTG AAC
GTG GCT GGC |
|
|
blaDHA | P1: AAC TTT CAC AGG
TGT GCT GGG T | 405 |
|
| P2: CCG TAC GCT TAC
TGG CTT TGC |
|
|
blaACC | P1: AAC AGC CTC AGC
AGC CGG TTA | 346 |
|
| P2: TTC GCC GCA ATC
ATC CCT AGC |
|
|
blaEBC | P1: TCG GTA AAG CCG
ATG TTG CGG | 302 |
|
| P2: CTT CCA CTG CGG
CTG CCA GTT |
|
|
blaFOX | P1: AAC ATG GGG TAT
CAG GGA GAT G | 190 |
|
| P2: CAA AGC GCG TAA
CCG GAT TGG |
|
Sequence analysis
Two strains with positive PCR amplication were
selected, and were bidirectionally sequenced (by Shenggong Corp.)
and searched using the BLAST program (http://blast.ncbi.nlm.nih.gov/Blast.cgi). The
sequencing results were compared with data on the GenBank
database.
Results
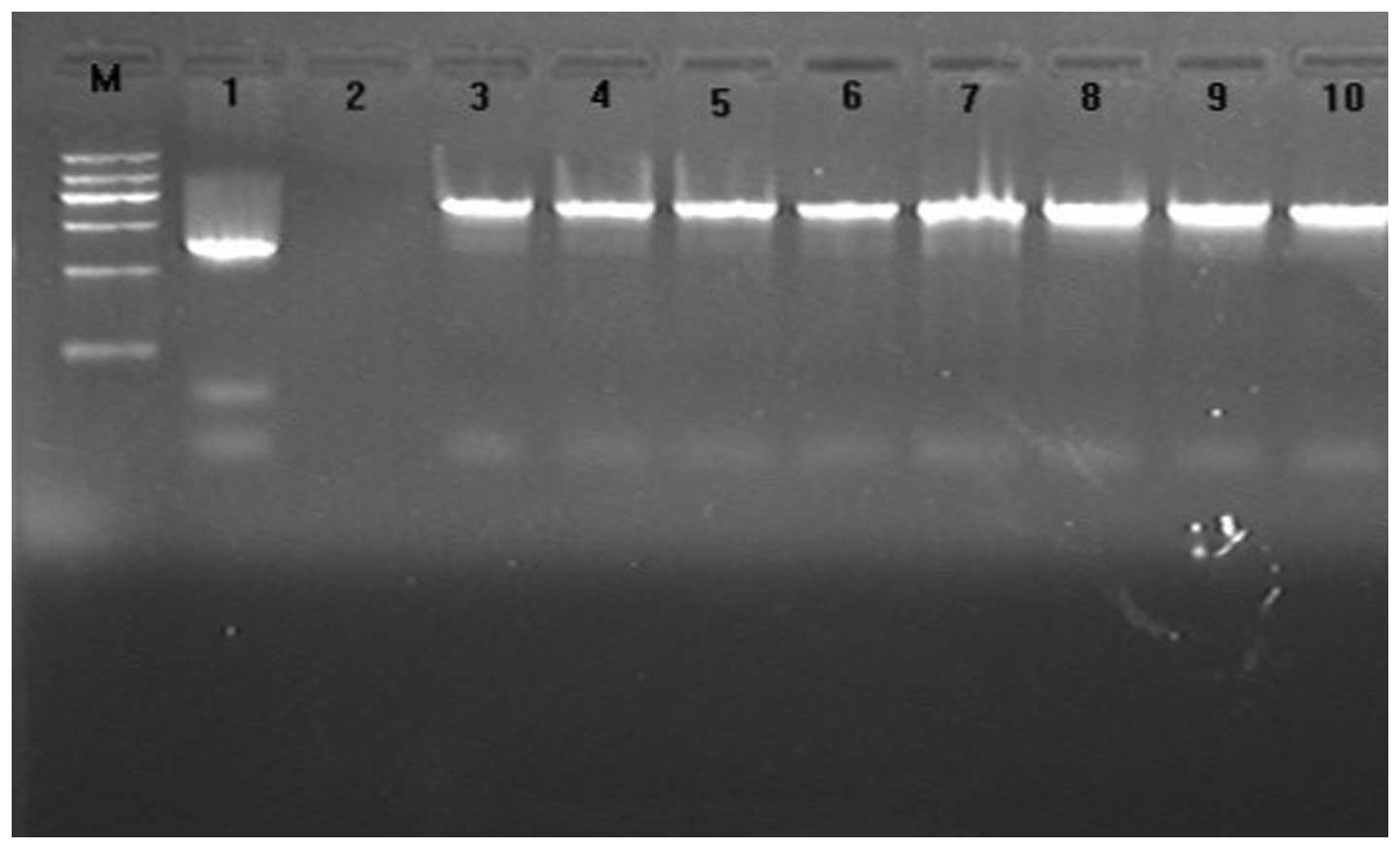
The results indicated that the majority of A.
baumannii bacteria were present in the ICU deparments of the
hospitals (Table II). The
amplification products from 96 strains were observed for each
template, and the size observed was consistent with the expected
size (663 bp). All A. baumannii isolates were of the
acinetobacter-derived cephalosporinase (ADC) type based on the size
of the fragments amplified by the primers. The positive rate was
72% (96/134) (Fig. 1).
| Table II.Distribution of the 134
Acinetobacter baumannii strains in distinct departments. |
Table II.
Distribution of the 134
Acinetobacter baumannii strains in distinct departments.
| Wards | Strain | Percentage (%) |
|---|
| ICU | 80 | 59.70 |
| Department of
Respiratory Care | 6 | 4.48 |
| Department of
Neurology | 4 | 11.19 |
| Department of
Geriatrics | 3 | 2.24 |
| Department of
Surgery | 15 | 19.40 |
| Others | 26 | 2.99 |
Results of sequencing analysis
Based on the GenBank database (http://www.ncbi.nlm.nih.gov/Entrez/), the
purification sequencing results revealed that the positive products
of PCR amplication were the ampC gene of the ADC type.
Partial sequencing results were shown in Fig. 2.
Results of the drug sensitivity
test
AmpC of A. baumannii was found to be
significantly resistant to cephalosporin, quinolone, a synthetic
compound combined with sulbactam and carbapenem antibiotics, but
were sensitive to polymyxin (Table
III).
| Table III.Results of the drug sensivity test of
the 96 Acinetobacter baumannii strains positive for
AmpC. |
Table III.
Results of the drug sensivity test of
the 96 Acinetobacter baumannii strains positive for
AmpC.
|
| Sensivity | Medium sensivity | Resistance |
|---|
|
|
|
|---|
| Strain | Rate | Strain | Rate | Strain | Rate |
|---|
| Cefoxitin | 0 | 0 | 0 | 0 | 96 | 100 |
| Ceftazidime | 0 | 0 | 0 | 0 | 96 | 100 |
| Cefepime | 0 | 0 | 0 | 0 | 96 | 100 |
| Levofloxacin | 0 | 0 | 0 | 0 | 96 | 100 |
| Gentamicin | 0 | 0 | 2 | 2.1 | 94 | 97.9 |
|
Ampicillin/sulbactam | 1 | 1.0 | 7 | 7.3 | 88 | 91.7 |
|
Piperacillin/tazobactam | 1 | 1.0 | 8 | 8.3 | 87 | 90.6 |
| Tienam | 7 | 7.3 | 1 | 1.0 | 88 | 91.7 |
| Polymyxin | 96 | 100 | 0 | 0 | 0 | 0 |
Discussion
A. baumannii is a clinically opportunistic
pathogen, particularly for hospital-acquired pneumonia (8), and infections are associated with
invasive medical procedures (9).
According to the monitoring data of nosocomial infection in 2003 in
the USA, the prevalence of A. baumannii infection, ranks
fourth in nosocomial infection. With the widespread application of
extended-spectrum antibiotics, the contribution of the multidrug
and pandrug resistance pattern of A. baumannii has increased
over the years, making the treatment of clinical infections more
difficult (10). For Gram-negative
bacteria, the production of β-lactamases plays an important role in
the resistance to β-lactam antibiotics (5).
AmpC β-lactamases (AmpC enzymes) are produced by
some bacteria and their production is mediated either by
chromosomes or by plasmids of Gram-negative bacteria (5). As a ‘serine’ cephalosporinase, AmpC
β-lactamases cannot be inhibited by clavulanic acid, but can be
inhibited by cloxacillin (11). The
enzymes belong to the functional group I [according to the
Bush-Jacoby-Medeiros (B-J-M) classification] and the molecular
class C. The A. baumannii bacterium is equipped with the
chromosome encoded enzyme of class C, and ampC genes from
heterogeneous A. baumannii strains highly correlate with
each other, but differ from those from other types of strains.
Thus, these enzymes are termed as the ADC family (7).
In this study, we genotyped A. baumannii
isolates by PCR. Amplification products from 96 strains were
observed for each template, with the expected size (663 bp). All
A. baumannii isolates were of the ADC type based on the size
of the fragments amplified by the primers. The absence of amplified
products for the other 6 pairs of primers suggested that the
assoication of the ampC gene with plasmid-mediated
phenomenon did not occur in A. baumannii and in the other
strains in this study. Two strains with positive PCR amplification
were selected, the products of which were bidirectionally sequenced
and searched using the BLAST program. The results revealed 100%
homology with ADC-1. In accordance with previous literature
(12), our results demonstrated a
total positive rate of 72% for AmpC β-lactamases in A.
baumannii in tertiary-level hospitals in the Xuzhou region in
China.
In this study, 134 strains of A. baumannii
were found to be extensively distributed in a range of departments,
amongst which the ICU departmet was found to be the major source.
The results of the drug sensitivity test revealed a multidrug, and
even a pandrug resistance pattern of AmpC A. baumannii.
Carbapenem is the priority drug used for the treatment of
infections with AmpC G-bacillus. In this study, the resistance rate
of ADC type AmpC A. baumannii to Tienam was as high as
91.7%, which is possibly associated with the spread of carbapenem
of OXA type in Acinetobacter (13). Some lines of evidence indicate that
sulbactam can irreversibly bind Acinetobacter PBP, which
contributes to its inherent antimicrobial activity (14). However, this study demonstrated a
drug resistance rate of approximately 90% to ampicillin-salbactam,
complicating its drug-resistant mechanisms. We did not identify any
drug-resistant strains for polymyxin, which can be a priority drug
for treatment. It has been reported that aztreonam in combination
with polymyxin may improve the therapeutic effect (14). Nonetheless, a kidney function test is
necessary before the combined application of these two drugs, given
that polymyxin may induce ototoxicity and renal toxicity. It has
also been suggested that antibacterial peptides and vaccination may
also be potential choices for therapeutic strategies (15).
In conclusion, the drug resistance condition of AmpC
A. baumannii in tertiary-level hospitals in the Xuzhou
region is relatively severe and warrants intensive monitoring.
References
|
1
|
Bayuga S, Zeana C, Sahni J, Della-Latta P,
el-Sadr W and Larson E: Prevalence and antimicrobial patterns of
Acinetobacter baumannii on hands and nares of hospital
personnel and patients: the iceberg phenomenon again. Heart Lung.
31:382–390. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kumar A, Randhawa VS, Nirupam N, Rai Y and
Saili A: Risk factors for carbapenem-resistant Acinetobacter
baumanii blood stream infections in a neonatal intensive care
unit, Delhi, India. J Infect Dev Ctries. 8:1049–1054. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chopra T, Marchaim D, Awali RA, Krishna A,
Johnson P, Tansek R, Chaudary K, Lephart P, Slim J, Hothi J, et al:
Epidemiology of bloodstream infections caused by Acinetobacter
baumannii and impact of drug resistance to both carbapenems and
ampicillin-sulbactam on clinical outcomes. Antimicrob Agents
Chemother. 57:6270–6275. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dettori M, Piana A, Deriu MG, Lo Curto P,
Cossu A, Musumeci R, Cocuzza C, Astone V, Contu MA and Sotgiu G:
Outbreak of multidrug-resistant Acinetobacter baumannii in
an intensive care unit. New Microbiol. 37:185–191. 2014.PubMed/NCBI
|
|
5
|
Poirel L, Lebessi E, Castro M, Fèvre C,
Foustoukou M and Nordmann P: Nosocomial outbreak of
extended-spectrum beta-lactamase SHV-5-producing isolates of
Pseudomonas aeruginosa in Athens, Greece. Antimicrob Agents
Chemother. 48:2277–2279. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pérez-Pérez FJ and Hanson ND: Detection of
plasmid-mediated AmpC beta-lactamase genes in clinical isolates by
using multiplex PCR. J Clin Microbiol. 40:2153–2162. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bou G and Martínez-Beltrán J: Cloning,
nucleotide sequencing, and analysis of the gene encoding an AmpC
beta-lactamase in Acinetobacter baumannii. Antimicrob Agents
Chemother. 44:428–432. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu YN, Cao B, Wang H, Chen LA, She DY,
Zhao TM, Liang ZX, Sun TY, Li YM, Tong ZH, et al: Adult hospital
acquired pneumonia: A multicenter study on microbiology and
clinical characteristics of patients from 9 Chinese cities.
Zhonghua Jie He He Hu Xi Za Zhi. 35:739–746. 2012.(In Chinese).
PubMed/NCBI
|
|
9
|
Trottier V, Namias N, Pust DG, Nuwayhid Z,
Manning R, Marttos AC Jr, Dunham MB, Schulman CI and McKenney MG:
Outcomes of Acinetobacter baumannii infection in critically
ill surgical patients. Surg Infect (Larchmt). 8:437–443. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee YL, Chen YS, Toh HS, Huang CC, Liu YM,
Ho CM, Lu PL, Ko WC, Chen YH, Wang JH, et al: Antimicrobial
susceptibility of pathogens isolated from patients with complicated
intra-abdominal infections at five medical centers in Taiwan that
continuously participated in the Study for Monitoring Antimicrobial
Resistance Trends (SMART) from 2006 to 2010. Int J Antimicrob
Agents. 40 (Suppl):S29–S36. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Seral C, Gude MJ and Castillo FJ:
Emergence of plasmid mediated AmpC β-lactamasas: Origin,
importance, detection and therapeutical options. Rev Esp Quimioter.
25:89–99. 2012.(In Spanish). PubMed/NCBI
|
|
12
|
Zhu JM, Jiang RJ, Wu JL, Wu KL, Wang JM
and Kong HS: Study on the AmpC gene of Multiple drug resistant
Acinetobacter baumannii type ADC. Chin J Clin Infect Dis.
1:222–226. 2008.(In Chinese).
|
|
13
|
Niumsup PR, Boonkerd N, Tansawai U and
Tiloklurs M: Carbapenem-resistant Acinetobacter baumannii
producing OXA-23 in Thailand. Jpn J Infect Dis. 62:152–154.
2009.PubMed/NCBI
|
|
14
|
Malone L and Kwon DH:
Carbapenem-associated multidrug-resistant Acinetobacter
baumannii are sensitised by aztreonam in combination with
polyamines. Int J Antimicrob Agents. 41:70–74. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
García-Quintanilla M, Pulido MR,
López-Rojas R, Pachón J and McConnell MJ: Emerging therapies for
multidrug resistant Acinetobacter baumannii. Trends
Microbiol. 21:157–163. 2013. View Article : Google Scholar : PubMed/NCBI
|