Introduction
The stump of the carotid artery has been shown to be
a source of emboli for ischemic stroke (1). The occurrence of ischemic stroke
following carotid artery occlusion can be attributed to an embolism
from the contralateral carotid artery via the circle of Willis, the
distal limit of thrombus propagation, or to an embolism from the
carotid stump via the external carotid artery (2). It is believed that microemboli
originating from the stump of the occluded internal carotid artery
(ICA) can pass into the middle cerebral artery circulation and the
ophthalmic artery as a consequence of patent external
carotid-internal carotid anastomosis; however, the occluded ICA is
traditionally only assumed to be responsible for the symptoms once
all other possible sources of emboli, such cardiac sources and
atheromatous lesions in the aortic arch or ipsilateral common
carotid artery, have been excluded. Following the exclusion of
these sources, a diagnosis of carotid stump syndrome (CSS) can be
made. The present study describes the case of a patient who
presented with a central retinal artery embolism following
ipsilateral ICA occlusion. The possible pathophysiological causes
and the treatment of this case are discussed.
Case report
The present study was conducted in accordance with
the Declaration of Helsinki and with approval from the Ethics
Committee of Qingdao University (Qingdao, China). Written informed
consent was obtained from the patient.
A 50-year-old male patient was hospitalized at 13:40
on November 21, 2013 due to a sudden weakness on the right side
associated with alalia for 3 days. The cranial magnetic resonance
imaging (MRI; GE Healthcare Bio-Sciences, Pittsburgh, PA, USA)
revealed multiple infarctions in the left basal ganglia region and
left temporal lobe. The cranial magnetic resonance angiography
(MRA) indicated occlusion of the left ICA and the middle cerebral
artery, and cerebral infarction was diagnosed. The symptoms did not
improve significantly upon antithrombotic treatment so the patient
was admitted to The Affiliated Hospital of Qingdao University
(Qingdao, China).
The patient had suffered from hypertension for 17
years and smoked for >30 years. Physical examination upon
hospitalization showed clear consciousness, incomplete motor
aphasia, a 3-mm pupil diameter on both sides, reflex sensitivity to
direct/indirect light, shallow right nasolabial fold, right
deflection of the tongue, decreased muscular tension of the
right-hand side of the body, grade 0 muscular strength and a
positive Babinski sign for the right side. The findings of the
cranial MRI on November 22, 2013 (Fig.
1) were consistent with the occurrence of cerebral infarction
(radial-basal ganglia region, insular lobe and temporal lobe). A
low-molecular-weight heparin injection (Pfizer, New York, NY, USA)
was administered for anticoagulation, aspirin tablets (Bayer
Schering Pharma AG, Beijing, China) were used as an antiplatelet
therapy, atorvastatin calcium tablets (Pfizer) were used to
regulate lipids and a hetastarch-130/0.4 NaCl injection (Beijing
Fresenius Kabi Pharmaceutical Co., Ltd., Beijing, China) was used
to improve infusion.
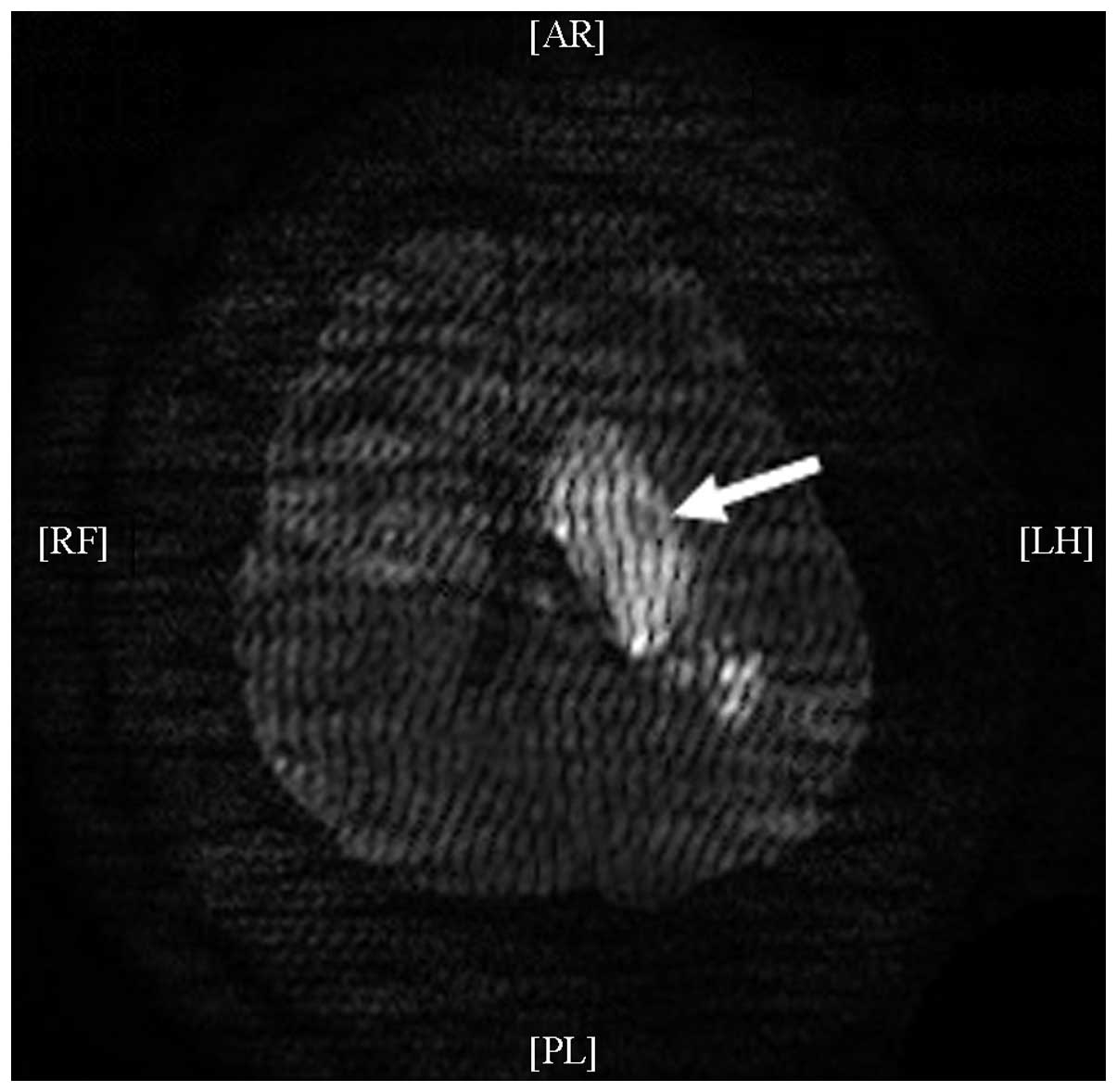
The sight of the left eye of the patient was lost at
10:10 on November 22, 2013. Physical examination showed
insignificant eyelid inflammation, normal sight of the right eye,
no light perception of the left eye, normal eye pressure, a
transparent cornea, a 5-mm-diameter left pupil, no reflex to direct
light and reflex sensitivity to indirect light. The diameter of the
pupil of the right eye was 3 mm. The right eye was sensitive to
direct light but did not sense indirect light. In terms of the
eyeground, the boundary of the optic disc of the right eye was
clear and reddish, and the cup/disc ratio was ~0.3; the boundary of
the optic disc of the left eye was clear and reddish, the blood
vessel of the retina was thin and the retina was pale. From the
ophthalmological consultation it was considered a strong
possibility that occlusion of the central retinal artery of the
left eye had occurred. The patient was administered oral 0.5-g
nitroglycerin tablets (Beijing Yimin Pharmaceutical Co., Ltd.,
Beijing, China) immediately and once a day for 2 days and was given
timolol maleate (Jiangsu Chengxin Pharmaceutical Co., Ltd., Jining,
China) and brimonidine D-tartrate (Allergan Pharmaceuticals Ireland
Ltd., County Mayo, Ireland) eye drops. In addition, the patient was
retrobulbarly injected with 10 mg raceanisodamine hydrochloride
(Suicheng Pharmaceutical Co., Ltd., Xinzheng, China) and
high-pressure oxygen treatment was applied.
A cranial-cervical computed tomography (CT)
angiography (GE Healthcare Bio-Sciences) was performed on November
26, 2013 (Fig. 2) and showed
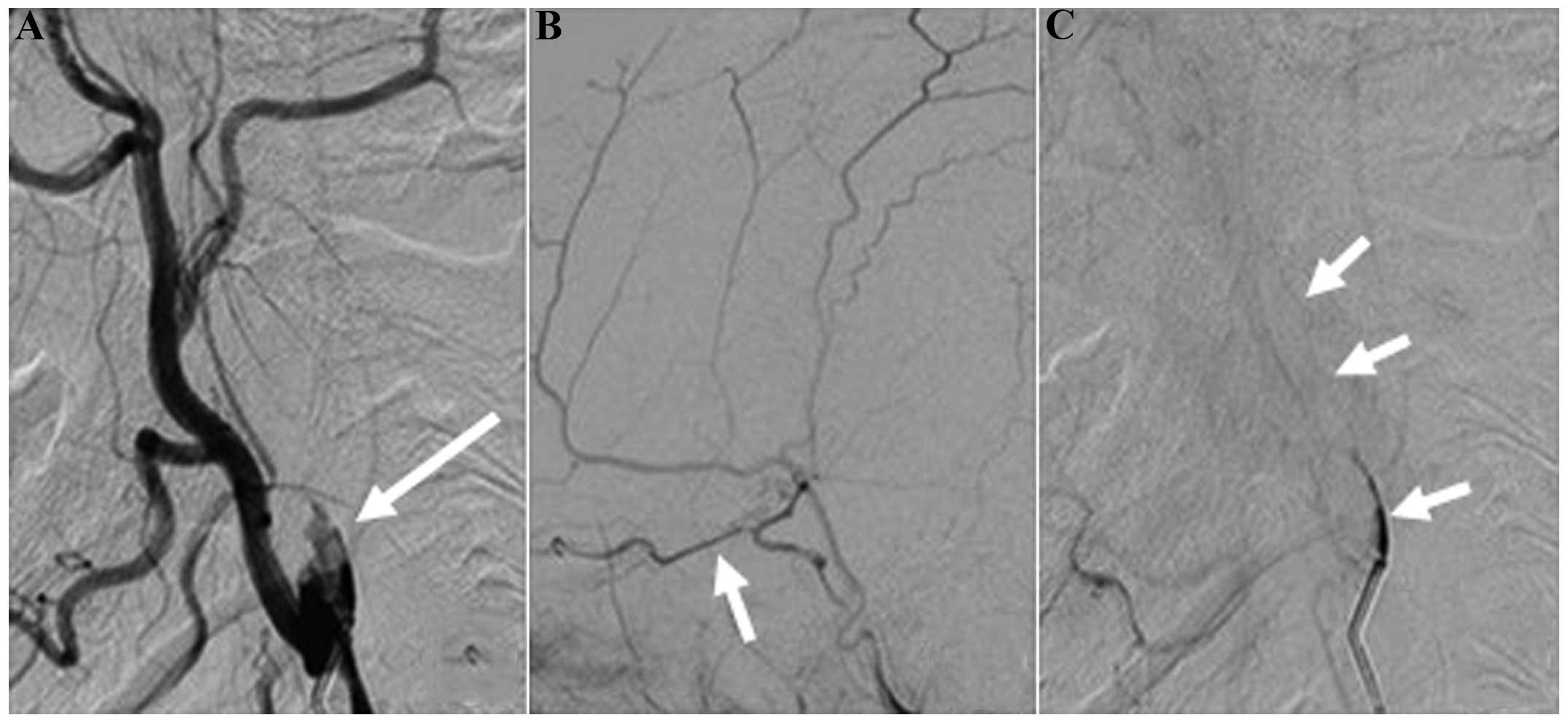
occlusion of the left ICA and left middle cerebral artery. Digital
subtraction angiography (DSA; Philips Electronics N.V., Amsterdam,
The Netherlands) was conducted on December 9, 2013 (Fig. 3) and showed a cervical occlusion of
the left ICA, defective filling and vortex blood flow in the stump
upon a local angiography of the left carotid artery, indicating a
new thrombus in the stump. During the venous phase, a trickle blood
flow was observed in the carotid artery but no flow was observed in
the left middle cerebral artery. The left external carotid artery
supplied blood to the brain to compensate via the deep cervical
artery branch, and the image of the siphonal section of the
cerebral cervical artery was weak. The anterior cerebral arteries
of both sides started from the right ICA. The right ICA branch
partially compensated for blood supply to the left middle cerebral
artery area through the soft membrane of the anterior cerebral
artery. The vertebral artery compensated partially for the left
anterior circulation through the poorly developed posterior
communicating artery and the soft membrane of the posterior
cerebral artery, but compensation was evidently insufficient. The
left ophthalmic artery showed forward blood flow.
The recurrent strokes of the patient were considered
to be due to a thromboembolism originating from the left carotid
artery stump. Antiplatelet agent administration was ceased and
warfarin sodium tablets (2.5 mg/day; Shanghai Xinyi Pharmaceutical
Co., Ltd., Shanghai, China) were used for anticoagulation
treatment. Following hospitalization for 30 days, the symptoms of
the patient improved, including the incomplete motor aphasia. The
patient had a defective visual field at the nasal side of the left
eye, visual acuity at the level of finger count at 30 cm of the
temporal side, a 4-mm-diameter left pupil, a dulled reflex to
direct light, a sensitive reflex to indirect light and grade II
muscular strength in the right side of the body. Following the
patient's discharge from the hospital, atorvastatin calcium and
warfarin sodium tablets were administered orally for therapy (to
maintain the prothrombin time-international normalized ratio at
2.0–3.0), and rehabilitation training was performed.
A 6-month follow-up showed that the patient's
language ability, the eyesight of the left eye and the muscular
strength of the right side of the body had improved significantly,
and the patient could walk independently. The visual acuity was
finger count at 50 cm at the temporal side of the left eye, the
diameter of the left pupil was 3 mm, the reflex to direct light was
slightly dulled and the reflex to indirect light was sensitive. In
the right eye, the diameter of the pupil was 3 mm, the reflex to
direct light was sensitive and the reflex to indirect light was
slightly dulled. The patient had grade IV muscular strength on the
right side of the body.
Discussion
The annual incidence of mortality and stroke of
patients suffering from one-sided ICA occlusion has been shown to
be ~30%, and the risk of an ipsilateral stroke occurring in the
presence of an occluded ICA is 3–5% per year (3–5). The
occurrence of ischemic stroke following carotid artery occlusion
can be attributed to an embolism from the contralateral carotid
artery via the circle of Willis, the distal limit of thrombus
propagation, or to an embolism from the carotid bifurcation via the
external carotid artery (6). When
all other sources of emboli are excluded, the ipsilateral ischemic
stroke resulting from an emboli arising from the stump of the
occluded ICA is known as CSS. CSS was initially identified by
Fields and Lemak (7). It is
understood that microemboli originating from the stump of the
occluded ICA or the ipsilateral external carotid artery can enter
the middle cerebral artery circulation due to the existence of
patent external carotid-internal carotid anastomotic channels
(8).
Cranial MRI was performed on the patient at the date
of the attack. Infarction was observed in the left middle cerebral
artery, and the flow void signal of the left ICA and middle
cerebral artery disappeared. Cranial-cerebral MRA showed left ICA
and middle cerebral artery occlusion. The right-sided weakness had
been attributed to the acute occlusion of the left ICA. Four days
after the acute occlusion of the left ICA, the ipsilateral eyesight
was lost. Once ophthalmological diseases were excluded, the loss of
eyesight was suggested to be a result of the occlusion of the
retinal central artery. Since the left carotid artery had been
occluded, it was unclear where the embolism was from. Furthermore,
no evident abnormality was observed on the patient's cardiac
ultrasound and dynamic cardiogram and no clear stenosis or plaque
were found on the CT angiography of the aortic arch, ipsilateral
common carotid artery, external carotid artery and contra-lateral
ICA. With regard to the possible mechanisms underlying the
recurrent ipsilateral ischemic stroke of the patient, heart-,
aortic arch-, ipsilateral common carotid artery- and external
carotid artery-born emboli and low fusion could, in principle, be
excluded. Cerebral angiography showed the cervical occlusion of the
left ICA, deficient filling and vortex blood flow in the left
carotid artery stump, and trickle flow in the ICA during the venous
phase. It was presumed that the embolism was from the thrombus of
the carotid artery stump. Cerebral angiography of the patient
showed that the anterior cerebral arteries of both sides started
from the right ICA. The terminal branch of the left ICA extends and
becomes an isolated middle cerebral artery, and the middle cerebral
artery had been occluded due to acute thrombus formation, which led
to aphasia and right hemiplegia; therefore, the emboli derived from
the ICA stump led only to ophthalmic artery ischemia.
Among the possible mechanisms of CSS, a central
retinal artery embolism caused by the emboli of the ICA stump via
the external carotid and ophthalmic arteries held the highest
possibility. The classical pathway involves the reversed blood flow
of the ophthalmic artery (ICA stump-external carotid
artery-ophthalmic artery-central retinal artery). DSA of the
patient showed vortex flow at the left ICA stump and a fresh
thrombus, but no reversed blood flow was observed at the
ipsilateral ophthalmic artery. The embolism of this patient was
therefore not caused by the classical pathway mentioned above.
DSA showed that the branch of the ipsilateral deep
carotid artery and the other external carotid artery opened and
supplied blood to the ophthalmic artery through the siphonal
section of the ICA. Emboli at the internal carotid stump could,
therefore, cause the embolism of the central retinal artery and
subsequent eyesight loss of the patient via the ipsilaterally open
deep carotid and ophthalmic arteries (internal carotid
stump-external carotid artery-deep carotid artery-siphonal section
of ICA-ophthalmic artery-central retinal artery). In addition to
this possible mechanism, Lakshminarayan et al (9) mentioned a mechanism of trickle flow,
which indicated that the persistent trickle flow in the occluded
ICA was a possible mechanism of CSS. DSA of the patient in the
present report showed a small trickle flow in the occluded ICA
during the venous phase; there was a weak image in the siphonal
section of the ICA and no image in the middle cerebral artery.
Although the small trickle flow in the occluded ICA could not meet
with the effective perfusion of the brain, stump emboli could be
transported to the ophthalmic artery. This is a possible reason why
no reversed flow was observed in the ophthalmic artery.
Additionally, during the venous phase, the DSA of the patient
showed a small trickle flow in the left ICA and the siphonal
section. Since the middle cerebral artery comprises a terminal
branch of the ICA, it is unclear whether a thromboembolism in the
trunk of the middle cerebral artery could, to a certain extent, be
considered to be another stump. Furthermore, it is unclear whether
the unstable hemodynamics in this region dispose embolus formation
at the corresponding site. Since no studies, to the best of our
knowledge, have investigated this mechanism, further research is
required. It was considered likely that the recurrent strokes of
this patient were caused by one of the aforementioned mechanisms or
perhaps by a combination of at least two mechanisms.
To date, CSS therapy includes conservative
medication, surgical treatment and intravascular intervention.
Surgical treatment involves a longitudinal incision in the common
and external carotid arteries. The inner membrane of the external
carotid artery is then peeled off and the opening of the ICA is
sealed so as to stop the source of emboli from the internal carotid
stump. Kumar et al (10)
studied 25 cases of CSS, analyzing retrospectively the clinical
traits and postoperative recovery, and reported the safety and
validity of surgical treatment of CSS. In a study including 40
cases of CSS, the risk of recurrent cerebral vascular events with
conservative medication treatment was compared with that with
surgical treatment (11). During the
4-year follow-up, only one cerebral vascular event occurred. Since
the risk of recurrent stroke was low following one-sided ICA
occlusion, the study did not prove the superiority of conservative
medication treatment over surgical treatment; however, the
prognosis of patients with CSS treated by conservative medication
or surgical treatment was good (11). Despite this, compensation for an
occluded ICA by the ipsilateral external carotid artery is
associated with certain risks in surgical treatment, as the
clamping and blocking of the external carotid artery during surgery
can lead to low infusion and an ischemic stroke event.
Vascular intervention has become a new option for
patients with CSS. Naylor et al (12) reported the first case of vascular
intervention for patients with CSS in 2003. Stents were placed in
the common carotid and external carotid arteries to block the blood
flow of the internal carotid stump and to eradicate the source of
the embolism. Nano et al (13) also conducted case reports concerning
the intravascular intervention treatment of CSS.
In the present case, the diagnosis of CSS following
a recurrent ischemic stroke was correct. There was a high
possibility of a recurrent embolism; therefore, warfarin sodium was
used for anticoagulation treatment. During the 6-month follow up
the eyesight and physical activity of the patient improved and
further strokes did not occur.
In conclusion, the occlusion of the ICA is common
but reports concerning CSS cases are not. It is, therefore,
necessary to enhance the understanding of CSS. For recurrent
ipsilateral stroke events that occur shortly after the occlusion of
an acute ICA, the possibility of CSS should be considered. The
specific mechanism of CSS should be analyzed and corresponding
treatment given. Anticoagulation therapy can be effective and
achieve a good prognosis.
References
|
1
|
Barnett HJ, Peerless SJ and Kaufmann JC:
‘Stump’ on internal carotid artery - a source for further cerebral
embolic ischemia. Stroke. 9:448–456. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Quill DS, Colgan MP and Sumner DS: Carotid
stump syndrome: A colour-coded Doppler flow study. Eur J Vasc Surg.
3:79–83. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eikelboom BC and Ackerstaff RG:
Preoperative prediction of cerebral ischaemia due to carotid
occlusion. Eur J Vasc Surg. 7(Suppl A): 21–24. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Irvine CD: The significance of one
occluded internal carotid artery. Eur J Vasc Endovasc Surg.
16:91–93. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nicholls SC, Kohler TR, Bergelin RO,
Primozich JF, Lawrence RL and Strandness DE Jr: Carotid artery
occlusion: Natural history. J Vasc Surg. 4:479–485. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kawano H, Inatomi Y, Hirano T, Yonehara T
and Uchino M: Anticoagulation therapy for vertebral artery stump
syndrome. J Neurol Sci. 295:125–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fields WS and Lemak NA: Joint study of
extracranial arterial occlusion: X. Internal carotid artery
occlusion. JAMA. 235:2734–2738. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kawano H, Inatomi Y, Hirano T and Yonehara
T: Vertebral artery stump syndrome in acute ischemic stroke. J
Neurol Sci. 324:74–79. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lakshminarayan R, Scott PM, Robinson GJ
and Ettles DF: Carotid stump syndrome: Pathophysiology and
endovascular treatment options. Cardiovasc Intervent Radiol.
34(Suppl 2): S48–S52. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kumar SM, Wang JC, Barry MC, Farrell L,
Kelly CJ, Fitzgerald PH, Leahy A and Hayes DB: Carotid stump
syndrome: Outcome from surgical management. Eur J Vasc Endovasc
Surg. 21:214–219. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hrbáč T, Beneš V, Širůček P, Jonszta T,
Herzig R, Procházka V and Skoloudík D: Safety and efficacy of
surgical treatment of carotid stump syndrome: Pilot study. Ann Vasc
Surg. 26:797–801. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Naylor AR, Bell PR and Bolia A:
Endovascular treatment of carotid stump syndrome. J Vasc Surg.
38:593–595. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nano G, Dalainas I, Casana R, Malacrida G
and Tealdi DG: Endovascular treatment of the carotid stump
syndrome. Cardiovasc Intervent Radiol. 29:140–142. 2006. View Article : Google Scholar : PubMed/NCBI
|