Introduction
The rise in the prevalence of coronary arterial
obstructive disease and the increase in indicators of percutaneous
coronary arterial stent implantation, have made the accurate
detection of coronary arterial in-stent restenosis (ISR) using
non-invasive techniques a focal point of research, and a positive
conclusion has been drawn that multi-slice spiral computed
tomography (MSCT) can be used to follow up the occurrence of
coronary arterial ISR (1–7). From 2003 onwards, 64-MSCT has been used
to detect coronary arterial ISR in assessable stents, and a
relatively high specificity (88–100%) and negative predictive value
(NPV; 90–100%) have been obtained (6,8–14), due to its higher spatial and temporal
resolution, compared with previous generations of MSCT. More
recently, 320-MSCT systems able to achieve up to 16-cm volumetric
coverage in a single gantry rotation have become available
(15). These systems simultaneously
acquire 320 slices per rotation, and use a volumetric computed
tomography (CT) data acquisition approach, thereby reducing
contrast load, time of breath-hold and radiation (15). The high diagnostic performance of
320-slice CT coronary angiography (CTCA) in the assessment of
coronary artery disease has been previously reported (16–18);
however, the comparative analysis of the effectiveness of 64- and
320-MSCT in the detection of coronary artery stents and diagnosis
of in-stent restenosis is lacking.
In the present study, data collected from the 64-
and 320-MSCT coronary angiography of 93 patients following coronary
artery stent implantation at the First Affiliated Hospital of
Xinxiang Medical University (Weihui, China) between December 2008
and June 2013 were analyzed. The patients included 30 cases with 51
stents that were subjected to 64-MSCT, and 63 cases with 99 stents
that were subjected to 320-MSCT. The aim of the study was to
compare the diagnostic value of 64- and 320-MSCT in the display of
coronary artery stents and the diagnosis of in-stent
restenosis.
Materials and methods
Ethical approval and patient
consent
The present retrospective study was approved by the
Institutional Review Board of the First Affiliated Hospital of
Xinxiang Medical University, and informed consent was waived by the
institutional review board.
Patient data
A total of 93 patients who had coronary stents that
had been in place for 30 days to 12 years were subjected to 64- or
320-slice CTCA. Of the 93 patients, 30 underwent 64-slice CTCA
[64-MSCT group; 27 men and 3 women (age range, 39–82 years; mean
age, 58.30±14.35 years; body mass index (BMI), 23.40±1.56
kg/m2)] and 63 underwent 320-slice CTCA [320-MSCT group;
60 men and 3 women (age range, 45–86 years; mean age, 59.40±14.00
years; BMI, 24.10±1.53 kg/m2).
Clinical data
The 64-MSCT group received 51 stents (1 stent in 15
cases, 2 stents in 9 cases and 3 stents in 6 cases). The 51 stents
comprised 20 stainless steel coronary and 31 nitinol coronary
stents. The 320-MSCT group received 99 stents (1 stent in 33 cases,
2 stents in 24 cases and 3 stents in 6 cases). The 99 stents
comprised 21 stainless steel coronary and 78 nitinol coronary
stents. No hypersensitivity to iodinated contrast media, renal
insufficiency or any other contraindications were observed in any
of the cases. No cases of arrhythmia or atrial fibrillation (AF)
were observed in the 64-MSCT group; however, in the 320-MSCT group,
15 cases of arrhythmia or AF were identified.
CTCA data acquisition
In the 64-MSCT group, CTCA investigations were
performed using 64-MSCT (Aquilion; Toshiba Medical Systems,
Otawara, Japan) with 64 detector rows, each 0.5-mm wide, and a
gantry rotation time of 0.40 sec. If the heart rate of the patient
exceeded 65 beats/min, oral β-blocking medication (25–75 mg
propranolol hydrochloride tablets) was administered 1 h before
examination, unless contraindicated. A triphasic protocol was used
for the intravenous administration of the contrast medium. The
total volume of the nonionic contrast agent (Ultravist® 370
injection; Bayer Schering Pharma AG, Leverkusen, Germany) injected
into the median cubital vein was 60–85 ml (volume based on body
weight: ≤50 kg, 60 ml; 50–60 kg, 70 ml; 60–70 kg, 80 ml; and >
70 kg, 85 ml) at a flow rate of 5.0–5.5 ml/sec, followed by 40 ml
normal saline (NS). Following the 6-sec injection of the contrast
agent, an automated peak enhancement detection technique was used
to record the arrival of the contrast agent in the ascending aorta,
in order to synchronize the arrival of the contrast media and the
CT data acquisition, using a threshold of +180 Hounsfield units.
CTCA images were acquired during an inspiratory breath-hold of ~8
sec covering an entire R-R interval of the retrospective
electrocardiogram (ECG)-gating.
In the 320-MSCT group, CTCA investigations were
performed using 320-MSCT (Aquilion ONE; Toshiba Medical Systems)
with 320 detector rows, each 0.5-mm wide, and a gantry rotation
time of 0.35 sec. If the heart rate of the patient exceeded 70
beats/min, oral β-blocking medication (25–75 mg propranolol
hydrochloride tablets) was administered 1 h before examination,
unless contraindicated. A triphasic protocol was used for the
intravenous administration of the contrast medium. The total volume
of the nonionic contrast agent (Ultravist® 370 injection; Bayer
Schering Pharma AG) injected into the median cubital vein was 50–70
ml (volume based on BMI: ≤20, 50 ml; 20–25, 50–60 ml; 25–30, 60–70
ml; and >30, 70 ml) at a flow rate of 5.0–5.5 ml/sec, followed
by 40 ml NS. Following the 6-sec injection of the contrast agent,
an automated peak enhancement detection technique was used to
determine the arrival of the contrast agent in the thoracic aorta,
in order to synchronize the arrival of the contrast media and the
CT data acquisition, using a threshold of +350 Hounsfield units. An
inspiratory breath-hold following the 12-sec injection of the
contrast agent was required for the acquisition of the CT data.
During the CT data acquisition, the ECG was registered
simultaneously for prospective triggering of data acquisition. The
phase window was set at 30–80% of the R-R interval in patients with
a stable heart rate (≤70 beats/min). In the patients with a heart
rate >70 beats/min, CTCA data acquisition was performed during
multiple heart beats (typically two).
In both groups, the entire heart was examined. Tube
voltage and current were adapted to the BMI of the patient (tube
voltage range, 110–140 kV; maximal tube current, 400–580 mA).
An initial data set was reconstructed at the optimal
phase of the R-R interval (typically 75%). A slice thickness of
0.50 mm was obtained and the reconstruction interval was set to
0.25 mm. If multiple phases were obtained, the cardiac phase with
the least motion artifacts was selected (19). With regard to processing and
assessment, images were transferred to a remote workstation with
dedicated CTCA analysis software (Vitrea 2.0 or FX 3.1.1.0; Vital
Images, Minnetonka, MN, USA). During the CTCA examination the
highest heart rates recorded were 73 beats/min in the 64-MSCT group
and 88 beats/min in the 320-MSCT group.
CTCA data analysis
CTCA image analysis was performed by two observers
in consensus, experienced in the evaluation of CTCA and blinded to
the results of invasive coronary angiography (ICA). First,
three-dimensional volume-rendered reconstructions were used to
gather information regarding the anatomy and status of the coronary
arteries. Secondly, axial slices were visually examined for
significant narrowing, which was achieved by determining the
presence of ≥50% reduction of the luminal diameter and vessel
occlusion (20). Thirdly, the
analysis was assisted by curved multiplanar reconstructions of all
vessels.
Image quality assessments
Adequately reconstructed CTCA images of stented
segments were visually classified into 4 grades as follows: Grade
1, visible stent and stent lumen without metal artifacts; grade 2,
visible stent and stent lumen with slight metal artifacts; grade 3,
visible stent but invisible stent lumen with significant metal
artifacts; grade 4, invisible stent and stent lumen with severe
metal artifacts.
Significant ISR was diagnosed from the CTCA results
if intraluminal low-attenuation filling defects narrowed the stent
lumen diameter or the vessel lumen within 5 mm away from the stent
by >50%.
Quantification of radiation dose
Radiation effective dose (ED) was quantified by a
dose-length product conversion factor of 0.017 mSv/(mGy.cm).
Following the examination, the CT machines (Aquilion and Aquilion
ONE) provided a dose-length product automatically.
Statistical analysis
The results of ICA as a gold standard, and the
sensitivity, specificity, positive predictive value (PPV), negative
predictive value (NPV) and accuracy of the two MSCT methods for the
detection of significant ISR in CTCA were calculated for assessable
stents. Continuous data are expressed as mean ± standard deviation.
The χ2, Fisher's exact and rank-sum tests were used to
compare differences between the two groups. P<0.05 was
considered to indicate a statistically significant difference and
all reported P-values were two-sided. Statistical analyses were
performed using SPSS software, version 13 (SPSS, Inc., Chicago, IL,
USA).
Results
Results of image quality
assessment
In the 64-MSCT group, the images of the 20 stainless
steel coronary stents comprised 9 images classified as grade 3 and
11 as grade 2, and for the 31 nitinol coronary stents, 29 of the
images were classified as grade 1, and 2 as grade 2. In the
320-MSCT group, the images of the 21 stainless steel coronary
stents comprised 10 images classified as grade 3 and 11 classified
as grade 2, and for the 78 nitinol coronary stents, 74 were
classified as grade 1, and 4 as grade 2. No statistically
significant differences were observed in the image quality
assessments between the 64- and 320-MSCT groups for stainless steel
(χ2=0.028) and nitinol coronary (χ2=0.075)
stents (P>0.05).
Differences of sensitivity,
specificity, PPV, NPV and accuracy between 64-MSCT and 320-MSCT for
significant ISR
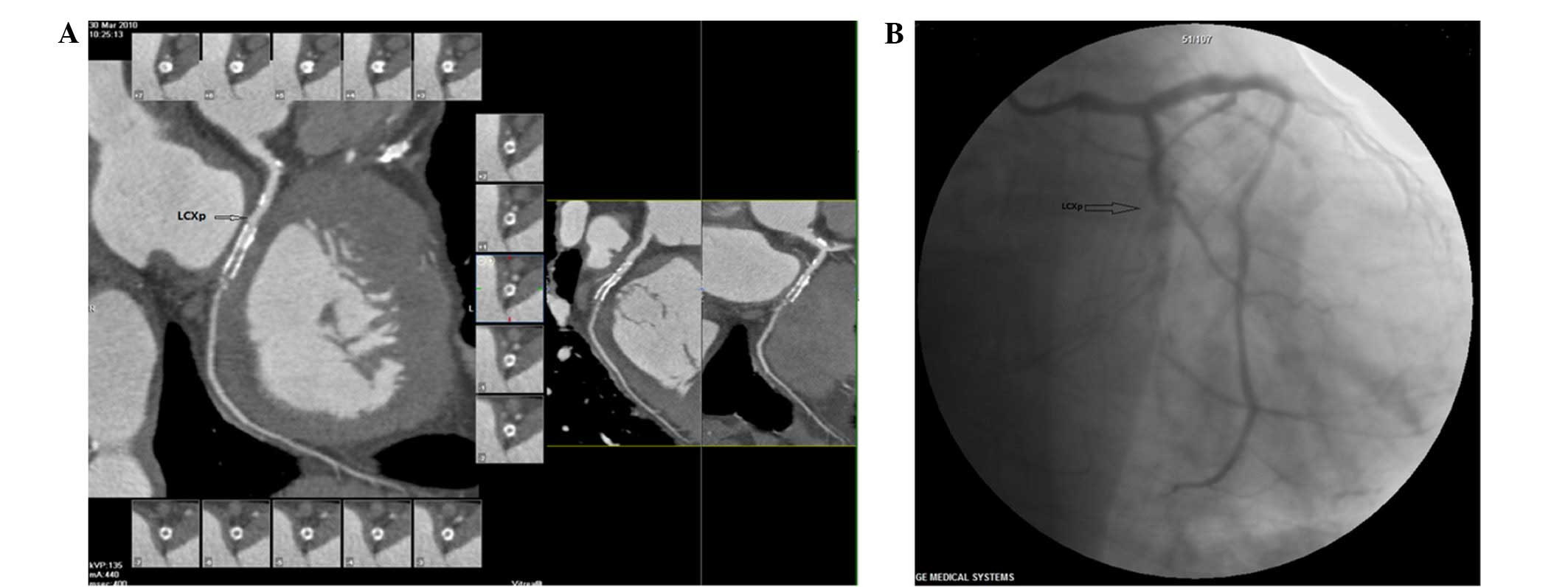
Images of stents classified as grade 3 or 4 were
excluded from the imaging quality assessments. In the 64-MSCT
group, 40 stents were classified as assessable, and 9 stents in 8
patients were diagnosed by CTCA to have significant ISR; however, 7
of 9 stents in 6 patients were found by ICA to have significant ISR
(Fig. 1). These stents had been in
place for 6 months to 4-years. The sensitivity, specificity, PPV,
NPV and accuracy of 64-MSCT for significant ISR in all assessable
stents were 100% (7/7), 93.94% (31/33), 77.78% (7/9), 100% (31/31)
and 95% (38/40), respectively (Table
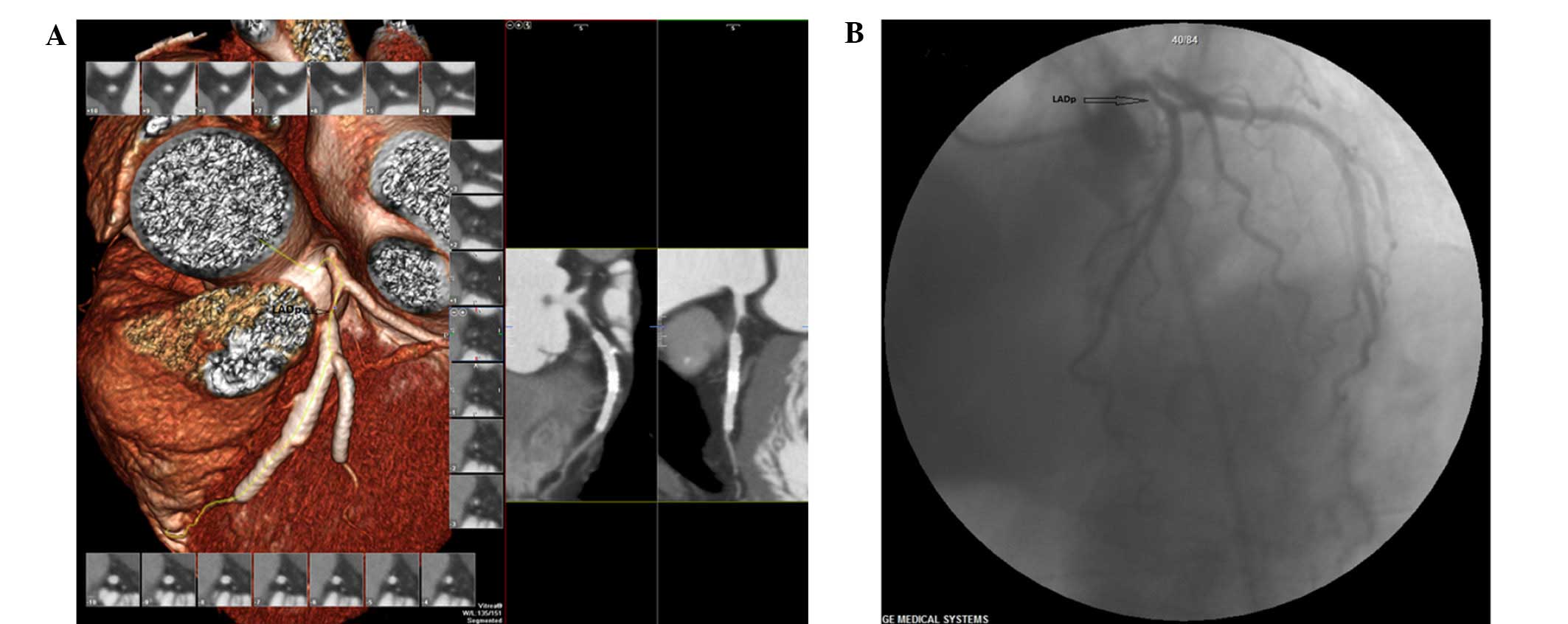
I). In the 320-MSCT group, 89 stents were classified as
assessable, and 19 stents in 88 patients were diagnosed by CTCA to
have significant ISR; however, 16 of 19 stents in 15 patients were
found by ICA to have significant ISR (Fig. 2). These stents had been in place for
2 months to 7 years. The sensitivity, specificity, PPV, NPV and
accuracy of 320-MSCT for significant ISR in all assessable stents
were 100% (16/16), 95.89% (70/73), 84.21% (16/19), 100% (70/70) and
96.63% (86/89), respectively (Table
II). No statistically significant difference was identified in
the sensitivity, specificity, PPV, NPV and accuracy between the
64-MSCT and 320-MSCT groups tested using Fisher's exact test
(P>0.05).
 | Table I.Validation of 64-slice CTCA compared
with ICA for in-stent restenosis. |
Table I.
Validation of 64-slice CTCA compared
with ICA for in-stent restenosis.
|
| 64-Slice CTCA
results |
|
|---|
|
|
|
|
|---|
| ICA results | Positive | Negative | Total |
|---|
| Positive | 7 | 2 | 9 |
| Negative | 0 | 31 | 31 |
| Total | 7 | 33 | 40 |
| Table II.Validation of 320-slice CTCA compared
with ICA for in-stent restenosis. |
Table II.
Validation of 320-slice CTCA compared
with ICA for in-stent restenosis.
|
| 320-Slice CTCA
results |
|
|---|
|
|
|
|
|---|
| ICA results | Positive | Negative | Total |
|---|
| Positive | 16 | 3 | 19 |
| Negative | 0 | 70 | 70 |
| Total | 16 | 73 | 89 |
Differences of heart rate and ED
between 64-MSCT and 320-MSCT
Statistically significant differences were observed
in the heart rate and ED of the patients between the 64-MSCT and
320-MSCT groups (P<0.05) (Table
III).
| Table III.Comparative analysis of heart rate,
BMI and ED between the two groups. |
Table III.
Comparative analysis of heart rate,
BMI and ED between the two groups.
| Variable | Heart rate | BMI | ED |
|---|
| 64-MSCT group | 65.10±4.78 | 23.30±1.46 | 20.00±3.26 |
| 320-MSCT group | 71.24±7.91 | 24.06±1.51 | 12.26±1.81 |
| Z-score | 3.05 | 2.02 | 6.21 |
| P-value | 0.02 | 0.04 | 0.00 |
Discussion
ISR is a major long-term complication of
percutaneous coronary treatment and is mainly due to neointimal
proliferation, but also mechanical causes (6). Generally, if the vessel lumen on both
sides of the stent does not narrow and the density in the stent is
the same as the density of adjacent normal vessels, this is
considered a direct sign of lack of ISR. An indirect sign of an
absence of ISR is a well-filled distant vessel of the stent;
however, if the stent has been distorted, the vessel distant from
of the stent exhibits a filling defect, narrowing or intermittent
display (21). It has been shown
that 20–30% of patients develop ISR at ~6 months after coronary
stent implantation (22). Although
the results of the present study indicate that patients develop ISR
>6 months after the coronary stent implantation, that may be due
to the relatively small number of patients included in the
study.
The diagnosis of ISR has been a subject of
particular interest to cardiologists and radiologists (3,5,7,17,23–31).
The main finding of the present study was the lack of statistically
significant differences in the sensitivity, specificity, PPV, NPV
and accuracy between 64- and 320-MSCT in the diagnosis of
significant ISR (P>0.05), suggesting that, when the number of
detector rows of spiral CT reaches a certain value, if not to
improve the spatial resolution of CT, but only to increase the
number of detector rows, no further effective improvements in the
quality of CT imaging can be achieved., with any further increases
in the number of detector rows of spiral CT not causing any
improvement of the spatial resolution of CT. In addition, the
present results indicated that both 64- and 320-MSCT failed to
display the stainless steel coronary stents clearly, and that the
grade of image quality assessments for these stents was lower than
that of the nitinol coronary stents. This finding also suggests
that stent material plays a central role in the follow-up and
curative effect evaluation following stent implantation (2).
It may be concluded that 64-MSCT remains
underdeveloped and inferior to 320-MSCT in all aspects. First,
64-MSCT scanning is easily affected by the patient's condition and
requires a regular heartbeat, a low heart rate and lack of AF in
order for it to be successful. Obtaining an acceptable image when
the patient exhibits an irregular heartbeat, high heart rate and AF
can be challenging. The results demonstrated that the mean heart
rate of the 64-MSCT group was significantly lower than that of the
302-MSCT group (P=0.02). This indicates that there is a greater
restriction on the patient's heart rate in 64-slice CTCA than in
320-slice CTCA. Secondly, the ED received by the patients in the
64-MSCT group was higher than that in the 320-MSCT group. A
previous study has reported that the use of 320- instead of 64-MSCT
scanning could signify a considerable reduction in the ED received
by patients (17). The
aforementioned finding is not only associated with the differences
between 64- and 320-MSCT scans, but also with other factors that
affect the scanning procedure, such as the scan mode and
reconstruction methods used during the examination. The present
study also showed that the ED of the patients in the 320-MSCT group
was lower than that of the patients in the 64-MSCT group
(P<0.01), a finding that was fairly consistent with results
reported in the literature (15,17).
The present study did, however, have certain
limitations: First, the number of samples was small, and therefore
further studies with a larger sample should be conducted. Secondly,
the effect of the stent material on image quality could not be
observed and thirdly, the sign of ISR has not been described in
detail.
In conclusion, both 64- and 320-MSCT are suitable
for use in follow-up and curative effect evaluation following
coronary stent implantation; however, 320-MSCT is less restricted
by the patient's heart rate and uses a lower dose of radiation.
Acknowledgements
This study was supported by the Health Department of
Henan Province, by a grant to the research project entitled ‘The
applied research of 320-slice spiral CT used in coronary arterial
in-stent restenosis’ (no. 201003078). The authors would also like
to thank the doctors, technicians and nurses of the Departments of
DSA and Radiology of the Affiliated Hospital of Xinxiang Medical
University for their assistance in case collection.
References
|
1
|
Ehara M, Kawai M, Surmely JF, Matsubara T,
Terashima M, Tsuchikane E, Kinoshita Y, Ito T, Takeda Y, Nasu K, et
al: Diagnostic accuracy of coronary in-stent restenosis using
64-slice computed tomography: Comparison with invasive coronary
angiography. J Am Coll Cardiol. 49:951–959. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chung SH, Kim YJ, Hur J, Lee HJ, Choe KO,
Kim TH and Choi BW: Evaluation of coronary artery in-stent
restenosis by 64-section computed tomography: Factors affecting
assessment and accurate diagnosis. J Thorac Imaging. 25:57–63.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hong C, Chrysant GS, Woodard PK and Bae
KT: Coronary artery stent patency assessed with in-stent contrast
enhancement measured at multi-detector row CT angiography: Initial
experience. Radiology. 233:286–291. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gaspar T, Halon DA, Lewis BS, Adawi S,
Schliamser JE, Rubinshtein R, Flugelman MY and Peled N: Diagnosis
of coronary in-stent restenosis with multidetector row spiral
computed tomography. J Am Coll Cardiol. 46:1573–1579. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gilard M, Cornily JC, Pennec PY, Le Gal G,
Nonent M, Mansourati J, Blanc JJ and Boschat J: Assessment of
coronary artery stents by 16 slice computed tomography. Heart.
92:58–61. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ehara M, Surmely JF, Kawai M, Katoh O,
Matsubara T, Terashima M, Tsuchikane E, Kinoshita Y, Suzuki T, Ito
T, et al: Diagnostic accuracy of 64-slice computed tomography for
detecting angiographically significant coronary artery stenosis in
an unselected consecutive patient population: Comparison with
conventional invasive angiography. Circ J. 70:564–571. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Seifarth H, Ozgün M, Raupach R, Flohr T,
Heindel W, Fischbach R and Maintz D: 64-Versus 16-slice CT
angiography for coronary artery stent assessment: In vitro
experience. Invest Radiol. 41:22–27. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rist C, von Ziegler F, Nikolaou K, Kirchin
MA, Wintersperger BJ, Johnson TR, Knez A, Leber AW, Reiser MF and
Becker CR: Assessment of coronary artery stent patency and
restenosis using 64-slice computed tomography. Acad Radiol.
13:1465–1473. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rixe J, Achenbach S, Ropers D, Baum U,
Kuettner A, Ropers U, Bautz W, Daniel WG and Anders K: Assessment
of coronary artery stent restenosis by 64-slice multi-detector
computed tomography. Eur Heart J. 27:2567–2572. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Oncel D, Oncel G and Karaca M: Coronary
stent patency and in-stent restenosis: Determination with
64-section multidetector CT coronary angiography-initial
experience. Radiology. 242:403–409. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Carrabba N, Bamoshmoosh M, Carusi LM,
Parodi G, Valenti R, Migliorini A, Fanfani F and Antoniucci D:
Usefulness of 64-slice multidetector computed tomography for
detecting drug eluting in-stent restenosis. Am J Cardiol.
100:1754–1758. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Das KM, El-Menyar AA, Salam AM, Singh R,
Dabdoob WA, Albinali HA and Al Suwaidi J: Contrast-enhanced
64-section coronary multidetector CT angiography versus
conventional coronary angiography for stent assessment. Radiology.
245:424–432. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schuijf JD, Pundziute G, Jukema JW, Lamb
HJ, Tuinenburg JC, van der Hoeven BL, de Roos A, Reiber JH, van der
Wall EE, Schalij MJ and Bax JJ: Evaluation of patients with
previous coronary stent implantation with 64-section CT. Radiology.
245:416–423. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tedeschi C, Ratti G, De Rosa R, Sacco M,
Borrelli F, Tammaro P, Covino G, Montemarano E, Cademartiri F,
Runza G, et al: Usefulness of multislice computed tomography to
assess patency of coronary artery stents versus conventional
coronary angiography. J Cardiovasc Med (Hagerstown). 9:485–492.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hein PA, May J, Rogalla P, Butler C, Hamm
B and Lembcke A: Feasibility of contrast material volume reduction
in coronary artery imaging using 320-slice volume CT. Eur Radiol.
20:1337–1343. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
de Graaf FR, Schuijf JD, van Velzen JE,
Kroft LJ, de Roos A, Reiber JH, Boersma E, Schalij MJ, Spanó F,
Jukema JW, et al: Diagnostic accuracy of 320-row multidetector
computed tomography coronary angiography in the non-invasive
evaluation of significant coronary artery disease. Eur Heart J.
31:1908–1915. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dewey M, Zimmermann E, Deissenrieder F,
Laule M, Dübel HP, Schlattmann P, Knebel F, Rutsch W and Hamm B:
Noninvasive coronary angiography by 320-row computed tomography
with lower radiation exposure and maintained diagnostic accuracy:
Comparison of results with cardiac catheterization in a
head-to-head pilot investigation. Circulation. 120:867–875. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
de Graaf FR, Schuijf JD, van Velzen JE,
Boogers MJ, Kroft LJ, de Roos A, Reiber JH, Sieders A, Spanó F,
Jukema JW, et al: Diagnostic accuracy of 320-row multidetector
computed tomography coronary angiography to noninvasively assess
in-stent restenosis. Invest Radiol. 45:331–340. 2010.PubMed/NCBI
|
|
19
|
Desbiolles L, Leschka S, Plass A, Scheffel
H, Husmann L, Gaemperli O, Garzoli E, Marincek B, Kaufmann PA and
Alkadhi H: Evaluation of temporal windows for coronary artery
bypass graft imaging with 64-slice CT. Eur Radiol. 17:2819–2828.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Raff GL, Abidov A, Achenbach S, Berman DS,
Boxt LM, Budoff MJ, Cheng V, DeFrance T, Hellinger JC and Karlsberg
RP: Society of Cardiovascular Computed Tomography: SCCT guidelines
for the interpretation and reporting of coronary computed
tomographic angiography. J Cardiovasc Comput Tomogr. 3:122–136.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Schmitt F, Grosu D, Mohr C, Purdy D, Salem
K, Scott KT and Stoeckel B: 3 Tesla MRI: Successful results with
higher field strengths. Radiologe. 44:31–47. 2004.PubMed/NCBI
|
|
22
|
Peng LJ and Tian GP: Inflammatory reaction
and stent restenosis after coronary stent implantation. Shi Yong
Xin Nao Fei Xue Guan Bing Za Zhi. 14:13–15. 2006.(In Chinese).
|
|
23
|
Kitagawa T, Fujii T, Tomohiro Y, Maeda K,
Kobayashi M, Kunita E and Sekiguchi Y: Noninvasive assessment of
coronary stents in patients by 16-slice computed tomography. Int J
Cardiol. 109:188–194. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhu H, Warner JJ, Gehrig TR and Friedman
MH: Comparison of coronary artery dynamics pre- and post-stenting.
J Biomech. 36:689–697. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Şatiroğlu Ö, Bostan M and Bozkur E: Acute
coronary syndrome due to bare metal stent fracture in the right
coronary artery. Kardiol Pol. 69:859–861. 2011.PubMed/NCBI
|
|
26
|
Bilen E, Yasar Saatci A, Bilge M, Karakas
F, Kırbas O and Ipek G: Acute coronary syndrome due to complete
bare metal stent fracture in the right coronary artery. Int J
Cardiol. 139:e44–e46. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kang WC, Han SH, Ahn TH and Shin EK: Acute
myocardial infarction caused by rupture of minimal intrastent
intimal hyperplasia after implantation of bare-metal stent. Int J
Cardiol. 120:e37–e40. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Giuliani G, Maehara A and Parodi G: Vessel
response evaluation by optical coherence tomography after
drug-eluting stent implantation in the left main coronary artery. G
Ital Cardiol (Rome). 11:2462010.(In Italian). PubMed/NCBI
|
|
29
|
Ruygrok PN, Webster MW, Ardill JJ, Chan
CC, Mak KH, Meredith IT, Stewart JT, Ormiston JA and Price S:
Vessel caliber and restenosis: A prospective clinical and
angiographic study of NIR stent deployment in small and large
coronary arteries in the same patient. Catheter Cardiovasc Interv.
59:165–171. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sousa JE, Costa MA, Sousa AG, Abizaid AC,
Seixas AC, Abizaid AS, Feres F, Mattos LA, Falotico R, Jaeger J, et
al: Two-year angiographic and intravascular ultrasound follow-up
after implantation of sirolimus-eluting stents in human coronary
arteries. Circulation. 107:381–383. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ahmed JM: Serial intravascular ultrasound
assessment of the efficacy of intracoronary gamma radiation for
preventing recurrent in-stent restenosis. Minerva Cardioangiol.
50:507–515. 2002.PubMed/NCBI
|