Introduction
Acute organophosphorus pesticide poisoning (AOPP) is
among the most common medical acute conditions with complex
symptoms and a high mortality rate (1–3).
Patients with AOPP typically exhibit mortality-associated
complications such as secondary infections, myocardial injury,
liver-kidney dysfunction and multiple organ failure (4). Currently, AOPP severity is usually
evaluated on the basis of patient symptoms, including dizziness,
headaches, nausea, vomiting, salivation, sweating, blurred vision
and signs of fatigue (5), and
routine blood and urine laboratory tests. Urine tests typically
assess the organophosphorus metabolic product content. In addition,
the determination of cholinesterase levels in the plasma of
patients with AOPP is widely used in the clinical diagnosis,
treatment and prognosis prediction of AOPP (6,7).
C-reactive protein (CRP) is a reactive substance in
acute lesions, and elevated plasma levels of CRP are a result of
inflammation and trauma. In AOPP, toxins may cause lesions in
tissues and organs in the body, leading to increased plasma CRP
levels (8). In addition, copeptin
has good stability in the plasma, usually indicating the levels of
antidiuretic hormone (9). Copeptin
is considered to be a novel marker that indicates individual stress
and is thus used in the prognostic evaluation of diseases caused by
system disorders (10). Therefore,
plasma CRP and copeptin may reflect the degree of lesions caused by
AOPP. Furthermore, acute physiology and chronic health evaluation
II (APACHE II) scoring, as a commonly used clinical scoring method,
may be applied to evaluate the severity and prognosis of acute
critical diseases (9,11,12).
However, to the best of our knowledge, there has been no reports
investigating the changes in plasma CRP and copeptin levels in
patients with AOPP, or evaluating the AOPP prognosis using APACHE
II scoring. Thus, the aims of the present study were to evaluate
the changes of CRP and copeptin levels in the plasma of AOPP
patients, and to determine the prognosis of AOPP using APACHE II
scoring.
Materials and methods
Patients
Between April 2012 and May 2014, 100 patients with
AOPP admitted to the Affiliated Hospital of Taishan Medical
University (Tai'an, China) were selected for the study. The
diagnosis of AOPP was based on the following criteria: i) History
of exposure to toxins; ii) typical clinical manifestations and
symptoms (5); iii) symptom
improvement following treatment with reactivating agent; and iv)
reduction in activity of plasma cholinesterase. All patients had
accidentally ingested organophosphorus pesticides (50–450 ml).
According to the AOPP diagnosis and classification standards
(13), 54 patients presented mild
AOPP, 32 presented moderate AOPP and 14 presented severe AOPP. The
basic clinical characteristics of all patients are listed in
Table I. In addition, 100 healthy
subjects, including 45 men and 55 women with an average age of
39.6±8.17 years (age range, 30–50 years), were included as the
control group. The gender ratio and average age of the control
group was not significantly different, as compared with the AOPP
group. The present study was approved by the Ethics Committee of
Taishan Medical University. Written informed consent was obtained
from all patients or their families.
 | Table I.Clinical characteristics of
patients. |
Table I.
Clinical characteristics of
patients.
| Characteristic | Severe (n=14) | Moderate (n=32) | Mild (n=54) |
|---|
| Female (n) | 9 | 18 | 34 |
| Male (n) | 5 | 14 | 20 |
| Unable to raise head
(n) | 13 | 28 | 43 |
| Age (years) |
17.1±5.12 |
29.4±7.41 |
30.1±10.27 |
| APACHE II score | 20.91±2.65 | 12.54±3.56 |
9.75±5.63 |
| Blood lactate level
(mmol/l) |
5.67±0.52 |
3.53±0.49 |
2.26±0.21 |
| Acetylcholine
esterase level (IU/l) |
324.4±107.8 | 862.7±98.6 | 2,011.1±185.6 |
| Twitch disappearance
time (h) | 29.51±5.68 | 12.52±7.52 |
9.24±8.23 |
| Atropine dose
(mg) |
301.4±120.4 | 256.8±96.4 | 150.4±63.8 |
| Reactivating agent
dose (g) | 15.8±3.4 | 12.5±5.2 |
9.5±2.5 |
All AOPP patients received routine gastric lavage
with water, oxygen intake, electrocardiogram monitoring and
intravenous injection with 1–1.5 g pralidoxime chloride (Sihuan
Pharmaceutical Holdings Group, Co., Ltd., Beijing, China) and 1–2
mg atropine (China Resources Double-Crane Pharmaceutical, Co.,
Ltd., Beijing, China). In cases of respiratory failure, the
patients were subjected to intubation and ventilation, assisted by
the S9 VPAP™ Auto double level automatic ventilator (ResMed, San
Diego, CA, USA). In cases of asystole, the patients were treated
with chest compression and cardiopulmonary resuscitation, in
addition to water and electrolyte imbalance rectification,
nutritional improvement and appropriate dehydration. Patients with
severe symptoms underwent plasma purification therapy.
APACHE II scoring
APACHE II scoring was conducted in order to measure
the severity of AOPP in patients (14). APACHE II scores are determined from a
patient's age and physiological indicators, including the
alveolar-arterial oxygen gradient or partial pressure of oxygen in
arterial blood, body temperature (rectal), mean arterial pressure,
arterial pH, heart rate, respiratory rate, serum levels of sodium
and potassium, levels of creatinine, the hematocrit, white blood
cell count, and the Glasgow Coma Scale (14). The worst value for each indicator
within 1 day after hospitalization was recorded into a electronic
table produced by Microsoft Excel 2010 (Microsoft Corporation,
Redmond, WA, USA). Patients with one missing/unrecorded indicator
received an APACHE II score of zero, while those with more than two
missing/unrecorded indicators were not scored. Factors associated
with a high-risk of disease progression and mortality, including
blood lactate level, acetylcholine esterase level, twitch
disappearance time and an inability to raise the head, as
determined by our hospital, were measured via routine blood and
urine tests upon admission of the patients to the hospital. If
these factors were exacerbated following active treatment, the
patient was considered to have toxification progression. A higher
APACHE II score corresponded to a more severe disease and indicated
an elevated risk of mortality (14)
Enzyme-linked immunosorbent assay
(ELISA)
On days 1, 3 and 7, 5 ml plasma was obtained from
fasting peripheral blood. The concentrations of plasma CRP and
copeptin were measured using the CRP ELISA kit (DRG Instruments
GmbH, Marburg, Germany) and the Copeptin ELISA kit (48T/96T; MLBIO,
Shanghai, China), respectively, according to the manufacturer's
protocol. The protein expression levels were quantified using the
SpectraMax® M5 Microplate Reader (Molecular Devices, LLC,
Sunnyvale, CA, USA) and analyzed using the SoftMax® Pro Data
Acquisition and Analysis software, version 5.4.1 (Molecular
Devices, LLC).
Statistical analysis
All the results were analyzed using SPSS software,
version 19.0 (IBM SPSS, Armonk, NY, USA). The data are expressed as
the mean ± standard deviation. Differences between groups were
compared using the Student's t-test, and multivariate analysis was
performed using logistic regression analysis. The Kaplan-Meier
method was used to analyze the prognostic asymptomatic survival
curves in relation to the CRP and copeptin levels in the patient
plasma. Analysis of prognostic determination was performed using
the area under the receiver operating characteristic (ROC) curve.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Levels of CRP and copeptin in patients
with severe AOPP are increased with time, but not in patients with
moderate or mild AOPP
To measure the changes of CRP and copeptin contents
in the plasma after treatment, ELISA was conducted. The plasma CRP
and copeptin levels were increased with the increase of AOPP
severity on days 1, 3 and 7 after AOPP, and were significantly
higher compared with those in the control group (P<0.05).
Patients with severe AOPP exhibited increasing plasma CRP and
copeptin contents over time (P<0.01), while patients with mild
and moderate AOPP exhibited reduced plasma CRP and copeptin
contents over time. On day 7 after AOPP, plasma CRP and copeptin
contents in all severity groups of AOPP patients remained
significantly increased compared with the levels in the control
group (P<0.05; Table II). These
results suggest that the plasma levels of CRP and copeptin in
patients with severe AOPP increased over time; however, this is did
not occur in patients with moderate or mild AOPP.
| Table II.Changes in plasma CRP and copeptin
contents in AOPP patients following treatment. |
Table II.
Changes in plasma CRP and copeptin
contents in AOPP patients following treatment.
|
| CRP level in
different groups (mg/l) | Copeptin level in
different groups (ng/ml) |
|---|
|
|
|
|
|---|
| Time | Severe | Moderate | Mild | Control | Severe | Moderate | Mild | Control |
|---|
| Day 1 | 23.5±11.2 | 15.2±9.4 | 7.3±4.2 | 3.2±2.3 | 11.4±5.9 | 7.2±3.6 | 2.3±1.1 | 0.8±0.3 |
| Day 3 | 27.6±15.2 | 12.3±5.4 | 5.3±3.5 | 3.2±2.3 | 13.2±6.3 | 5.9±2.4 | 1.5±0.8 | 0.8±0.3 |
| Day 7 |
63.5±29.5a |
8.3±3.8a | 4.3±2.1a | 3.2±2.3 |
33.5±12.7b | 4.1±1.6b | 1.1±0.7b | 0.8±0.3 |
Amelioration of relevant factors
improves the prognosis of AOPP
To evaluate the effect of relative factors on the
prognosis of AOPP, logistic regression analysis was used. The data
showed that higher APACHE II scores, low blood lactate and
acetylcholine esterase levels, an increased twitch disappearance
time, a higher reactivating agent dose and an inability to raise
the head were high risk factors (P<0.05; Table III). Therefore, the amelioration of
these parameters may improve the prognosis of AOPP.
| Table III.Logistic regression analysis of the
effect of multiple factors on prognosis. |
Table III.
Logistic regression analysis of the
effect of multiple factors on prognosis.
|
|
|
|
|
|
| 95.0% CI for Exp
(B) |
|---|
|
|
|
|
|
|
|
|
|---|
| Parameter | B | SE | Wald | Sig | Exp (B) | Upper limit | Lower limit |
|---|
| Blood lactate
level | 2.298 | 0.618 | 30.417 | 0.036 | 4.463 | 1.491 |
9.293 |
| APACHE II scores | 4.153 | 0.385 | 20.154 | 0.001 | 3.163 | 1.141 | 10.698 |
| Acetylcholine
esterase level | 3.396 | 0.601 |
7.986 | 0.002 | 3.038 | 1.642 |
8.125 |
| Twitch disappearance
time | 1.150 | 0.516 |
4.977 | 0.026 | 3.160 | 1.150 |
8.681 |
| Inability to raise
head | 3.012 | 0.412 | 27.138 | 0.001 | 5.934 | 1.118 |
8.637 |
| Reactivating agent
dose | 2.146 | 0.634 | 25.141 | 0.005 | 4.362 | 1.637 |
9.153 |
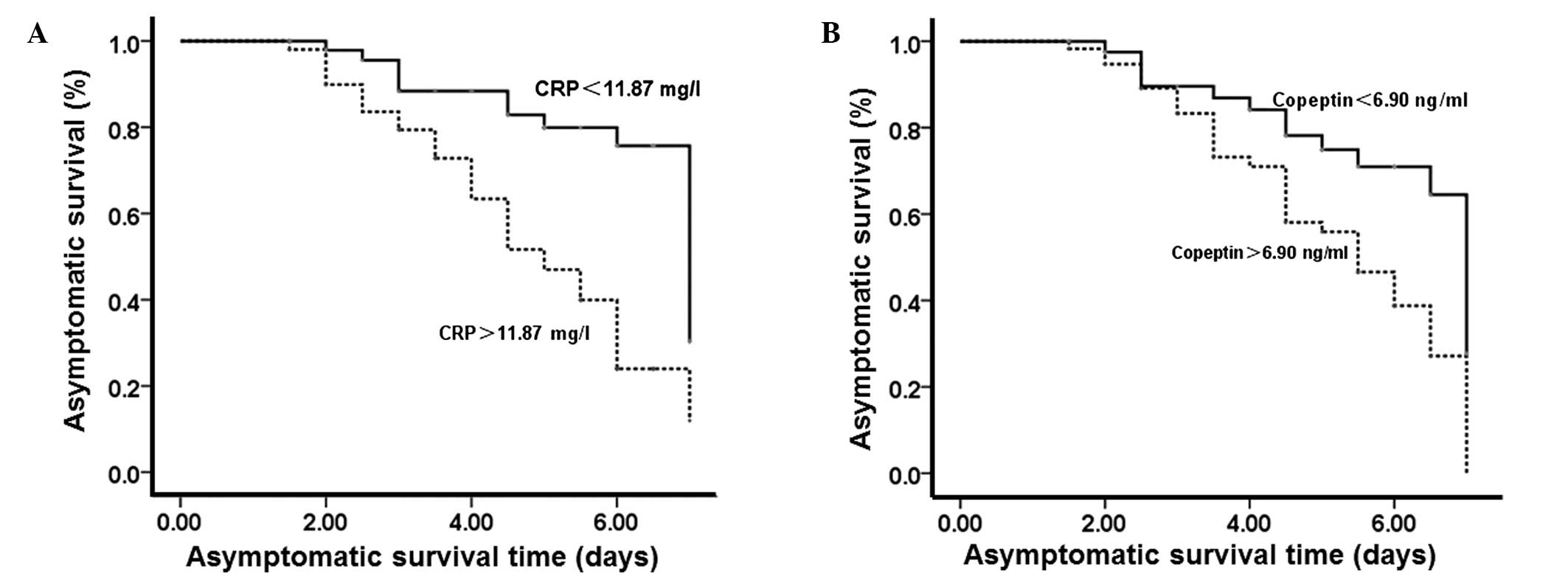
Increased plasma levels of CRP and
copeptin indicate a poorer prognosis
To test the effect of plasma CRP and copeptin on
prognosis, Kaplan-Meier analysis was performed on the prognostic
asymptomatic survival curves. According to the plasma CRP and
copeptin levels at 1 week after AOPP, the number of patients with
CRP levels that were higher and lower than the median value (11.87
mg/l) was 15 and 85, respectively. In addition, the number of
patients with copeptin levels that were higher and lower than the
median value (6.90 ng/ml) was 19 and 81, respectively. Kaplan-Meier
analysis of prognostic asymptomatic curves showed that patients
with plasma CRP and copeptin levels higher than the median values
had a worse prognosis (P<0.05; Fig.
1). The results suggest that higher CRP and copeptin levels in
the plasma indicate a poorer prognosis.
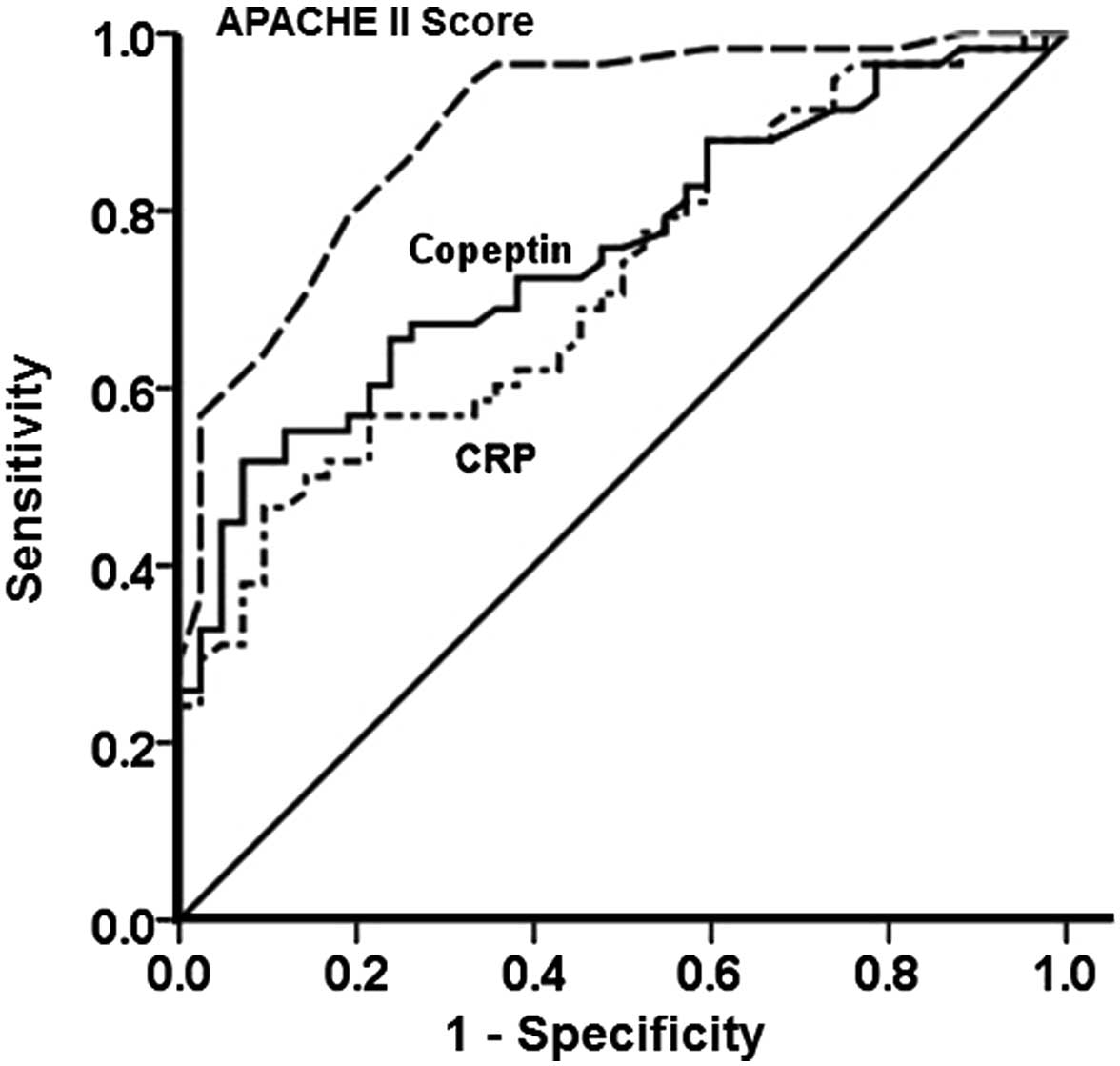
CRP and copeptin levels and APACHE II
scores can be used as predictors of AOPP patient survival
To evaluate the predictive role of CRP levels,
copeptin levels and APACHE II scores on the survival of AOPP
patients, ROC curves were plotted using SPSS software. The areas
under the ROC curves were 0.89, 0.75 and 0.72 for CRP, copeptin and
APACHE II scores, respectively (P<0.01). In addition, the
optimum diagnostic cut-off points for CRP, copeptin and APACHE II
scores were 10.2 mg/l, 6.3 ng/ml and 10.5, respectively. Notably,
all the CRP levels, copeptin levels and APACHE II scores had a
sensitivity and specificity of >90% (Fig. 2). The results indicate that CRP
levels, copeptin levels and APACHE II scores may be used for the
prediction of survival in AOPP patients.
Discussion
The present study showed that the levels of CRP and
copeptin on days 1, 3 and 7 after AOPP were increased according to
the severity of AOPP, and were significantly increased compared
with the control group. In addition, the levels of CRP and copeptin
in patients with severe AOPP increased over time, while those in
patients with mild or moderate AOPP decreased over time. This may
be due to the degree of toxification. Patients with mild or
moderate AOPP exhibit reduced acetylcholine stimulation of the
cholinergic nerves, stress responses, lesions on organs and
inflammation, leading to relatively low plasma CRP levels. By
contrast, patients with severe AOPP have severe poisoning of
tissues and organs, multiple organ failure and severe inflammation,
leading to relatively high plasma CRP levels. A previous study
demonstrated that AOPP patients have elevated plasma copeptin
levels, as compared with normal subjects, and that its levels
increase with increasing poisoning severity (15). In addition, this difference is
negatively correlated with the levels of acetylcholine esterase, an
indicator that reflects AOPP severity (16). Consistent with this observation, the
results of the present study indicated that the plasma copeptin
content was closely associated with poisoning lesions in AOPP
patients, and was variable at different time points.
A previous study indicated that APACHE II scoring
reflects the degree of lesions in organophosphate poisoning, with
higher scores indicating a higher possibility of respiratory
failure (17). Another study
suggested that acetylcholine accumulation in AOPP patients affects
the peripheral cholinergic nerves and inhibits the central nervous
system (8). Logistic regression
analysis in the present study demonstrated that APACHE II scores,
blood lactate level, acetylcholine esterase level, twitch
disappearance time, inability to raise head and reactivating agent
dose are high-risk factors for the prognosis of AOPP patients.
Kaplan-Meier analysis of asymptomatic survival curve suggested that
patients with plasma CRP or copeptin levels higher than the median
values were more likely to present other clinical symptoms and
reduced treatment efficacy, leading to poorer prognosis. In
addition, ROC analysis in the present study demonstrated that the
plasma CRP and copeptin levels and APACHE II scoring have good
sensitivity and specificity for the evaluation of AOPP
prognosis.
The treatment of AOPP is a clinical challenge for
emergency physicians. Active CRP and copeptin plasma levels, APACHE
II scoring, evaluation of disease and prognosis, and effective
treatment plans are directly associated with the survival of
patients. In conclusion, the present study revealed that changes in
the CRP and copeptin plasma levels, and the APACHE II scoring may
be associated with the prediction of AOPP prognosis. However, the
present study consisted of a relatively small number of patients,
and did not investigate the effect of combined cardiovascular,
diabetic, liver or kidney dysfunctions on the plasma levels of CRP
and copeptin; thus, further studies are required to confirm the
findings.
Acknowledgements
The authors would like to thank Dr Changqin Li and
Dr Jixue Shi at the Affiliated Hospital of Taishan Medical
University for their assistance with the design of the experiments
and write-up.
References
|
1
|
Wang Y, Lin K, Wu D, Wang Z, Wang Q, Mi X
and Liu C: Clinical investigations of changes in serum enzymes and
C-reactive protein in patients with acute toxification. Zhong Guo
Wei Zhong Bing Ji Jiu Yi Xue. 16:55–56. 2004.(In Chinese).
|
|
2
|
Wang Z, Lv Y and Cui T: Analysis of cause
of death by acute organophosphorus pesticide poisoning. Zhong Guo
She Qu Yi Shi. 14:106–107. 2012.(In Chinese).
|
|
3
|
Han L and Cui X: Application of intestinal
protection in adjuvant therapy of severe organophosphorus
poisoning. Shi Yong Yao Wu Yu Lin Chuang. 13:154–156. 2010.(In
Chinese).
|
|
4
|
Katan M, Morgenthaler N, Widmer I, Puder
JJ, König C, Müller B and Christ-Crain M: Copeptin, a stable
peptide derived from the vasopressin precursor, correlates with the
individual stress level. Neuro Endocrinol Lett. 29:341–346.
2008.PubMed/NCBI
|
|
5
|
Li H, Zhao C and Qiu Q: Clinical
characteristics and prognosis of ICU patients with severe acute
organic phosphorus poisoning. Xian Dai Zhong Xi Yi Jie He Za Zhi.
17:1812–1813. 2008.(In Chinese).
|
|
6
|
Zhang X, Li Q, Liu Y and Zhao J:
Determination of blood amylase in patients with acute
organophosphorus pesticide poisoning. Zhong Guo Wei Zhong Bing Ji
Jiu Yi Xue. 12:4332000.(In Chinese).
|
|
7
|
Wang J, Liu H, Yang Y, Zhang R and Zhang
Z: Clinical meaning of morphologic alteration of neutrophils in the
patients with acute organic phosphorus poisoning. Zhong Guo Ji Jiu
Yi Xue. 22:561–562. 2002.(In Chinese).
|
|
8
|
Pan D and Zhang Z: Clinical value of high
sensitivity C-reactive protein on AOPP and prognosis of patients
with the disease to determine. Hua Bei Mei Tan Yi Xue Tuan Xue Bao.
13:599–600. 2011.(In Chinese).
|
|
9
|
Zhang H, Ren G, Yin J and Sun W: Copeptin
expression in patients with acute organophosphorus poisoning and
its clinical significance. Shi Yong Yi Xue Xa Zhi She. 29:576–578.
2013.(In Chinese).
|
|
10
|
Zheng X: Current situation and advance of
APACHE-II score in the clinical application. Yi Xue Zong Shu.
17:3297–3298. 2011.(In Chinese).
|
|
11
|
Sam KG, Kondabolu K, Pati D, Kamath A,
Kumar Pradeep G and Rao PG: Poisoning severity score, APACHE II and
GCS Effective clinical indices for estimating severity and
predicting outcome of acute organophosphorus and carbamate
poisoning. J Forensic Leg Med. 16:239–247. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Akdur O, Durukan P, Ozkan S, Avsarogullari
L, Vardar A, Kavalci C and Ikizceli I: Poisoning severity score,
Glasgow coma scale, corrected QT interval in acute organophosphate
poisoning. Hum Exp Toxicol. 29:419–425. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dai Z, Shi Y and Nei KX: Practice of
Internal Medicine (13th). Beijing, China: People's Health
Publishing House. 1723–1724. 2009.
|
|
14
|
Knaus WA, Draper EA, Wanger DP and
Zimmerman JE: APACHE II. A severity of disease classification
system. Crit Care Med. 13:818–829. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li J, Wang R and He J: Copeptin and
ischemia modified albumin expression and significance of early in
acute paraquat poisoning. Shi Yong Lin Chuang Yi Xue Za Zhi.
18:40–43. 2014.(In Chinese).
|
|
16
|
Hu N, Huang M and Li W: The value of
APACHE II scoring system in assessment of severity and prognosis of
patients with organophosphate insecticide poisoning. Hua Zhong Ke
Ji Da Xue Tong Ji Yi Xue Yuan. 12:25–29. 2011.(In Chinese).
|
|
17
|
Deng Y, Wang F, Sun H and Wang X and Wang
X: Risk factor in the patients with intermediate syndrome after
acute organophosphorus pesticides poisoning. Zhong Guo Ji Jiu Yi
Xue. 28:704–706. 2008.(In Chinese).
|