Introduction
Brain natriuretic peptide (BNP) is a 32-amino acid
peptide which functions as a cardiac neurohormone that is
predominantly released from the cardiac ventricle in response to
left ventricular (LV) volume expansion and pressure overload
(1). As such, BNP is a potent
vasodilator and a natriuretic factor that regulates salt and water
homeostasis. Increased secretion of BNP predominantly occurs in
response to increased tension in the ventricular walls, decreased
oxygen supply, acute myocardial infarction (MI), chronic cardiac
heart failure (HF) and during hypertrophy of the heart (2). It has previously been demonstrated that
BNP levels are useful for the diagnosis of LV systolic and
diastolic dysfunction, and these levels correlate with the severity
and prognosis of the dysfunction (3). As BNP is predominantly released from
the LV myocardium, it is necessary to measure the regional function
of the sympathetic nervous system in the left ventricle in order to
elucidate the mechanisms associated with the release of BNP release
and the clinical significance of the increased BNP levels during HF
(4).
The prognostic importance of BNP and the N-terminal
of pro (NT-pro)BNP has previously been investigated in patients
with acute coronary syndromes and patients with HF, and both
markers were shown to be strong predictors of mortality and
morbidity (5). In particular,
diastolic wall stress has been demonstrated to have a stronger
correlation with NT-proBNP levels, as compared with systolic wall
stress (6). Previous studies have
suggested that the estimation of BNP values via a fast and reliable
blood test may be accepted as a diagnostic tool for assessing
asymptomatic diastolic dysfunction in patients with hypertrophic
cardiomyopathy (HCM), diabetes and hypertension (7–9).
Furthermore, as BNP has been demonstrated to be a highly useful,
simple and noninvasive diagnostic biomarker, BNP levels may be used
for the differential diagnosis of cardiac and pulmonary dyspnea in
emergency departments to guide therapy (10). However, whether BNP levels are
predictors of morbidity and mortality in patients with diastolic
dysfunction is yet to be investigated. Therefore, the present
observational study aimed to elucidate the effects of BNP levels on
the survival time of patients with diastolic dysfunction by
grouping and following up 708 inpatients with cardiovascular
disease until endpoint events occurred.
Materials and methods
Ethics statement
The data collection in the present study was
conducted according to the principles of the Declaration of
Helsinki (https://en.wikipedia.org/wiki/Declaration_of_Helsinki),
and this process did not affect the normal course of therapy. All
data were analyzed anonymously. The protocol of the present study
was approved by the Ethics committee of the hospital, and written
informed consent was obtained from each patient.
Subjects and procedures
In the present observational study, 708 inpatients
with cardiovascular disease at the Division of Cardiology (Jinshan
Hospital of Fudan University) were followed-up between May 2006 and
December 2008 until endpoints occurred. The duration of follow-up
ranged between 20 and 51 months and averaged 30.86 months. The mean
age of patients was 66 years, and the majority of the patients were
male (395/708; 55.8%). Patients were classified according to an
initial BNP cut-off point of 80 pg/ml. Endpoints were defined as
mortality or readmission due to cardiovascular disease, or
mortality due to any other reason.
Measurement of plasma BNP
concentration
Blood samples for the analysis of plasma BNP levels
were harvested from the antecubital vein upon patient admission.
BNP levels were analyzed using the Triage® BNP Test
(Biosite Diagnostics, Inc., San Diego, CA, USA), which is a
single-use fluorescence immunoassay device that is designed to
determine BNP levels in ethylenediaminetetraacetic
acid-anticoagulated whole blood or plasma specimens (EDTA purchased
from Biosite Diagnostics, Inc.). Briefly, the specimen was added to
the sample port of the test device using a 250-µl transfer pipette
and the device was inserted into the Triage® meter
(Biosite Diagnostics, Inc.). BNP analysis was automatically
conducted after the sample had reacted with the reagents within the
BNP device. Reaction and analysis lasted ~15 min. BNP
quantification was conducted based on the quantity of fluorescence
detected by the meter within the measurement zone on the device,
where increased fluorescence indicated a higher concentration of
BNP in the specimen (11).
Echocardiography
M-mode and two-dimensional images, and color flow
Doppler recordings were obtained using Vivid-7 ultrasound system
(GE Healthcare Bio-Sciences, Pittsburgh, PA, USA) operating at
2.0–3.5 MHz, as previously described (11). LV ejection fraction (LVEF) was
calculated according to the Simpson formula outlined by Teichholz
et al (12). In the present
study, LVEF ≥50% indicated that LV systolic function was normal,
whereas LVEF <50% indicated systolic dysfunction. A 7.5 MHz
pulsed Doppler transducer (GE Healthcare Bio-Sciences) was used to
measure diastolic transmitral Doppler parameters, including the
peaks of early (E) and late diastolic (A) mitral flow velocities.
Diastolic dysfunction was defined as an E/A ratio ≤1.
Statistical analysis
Baseline characteristics of patients enrolled in the
present were presented as percentages and medians with
interquartile ranges for dichotomous and continuous variables,
respectively. Between-group baseline characteristics comparisons
were performed using Wilcoxon rank-sum test and the χ2
test for continuous and variables discrete, respectively. Survival
curves were generated using Kaplan-Meier estimates; between-group
differences in survival duration were compared using the log-rank
test. Between-groups differences in the incidence of endpoint
events were evaluated via relative risk (RR).
Spearman correlation was used to correlate
continuous data with BNP levels and the duration of patients
survival. BNP levels were evaluated via receiver operating
characteristic (ROC) and area under curve (AUC) analyses for the
prediction of clinical endpoints. In order to determine optimal
specificity (Sp) and sensitivity (Se) values the value closest to
the peak Sp and Se points on the ROC curve was identified.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Clinical characteristics
The baseline clinical characteristics of the patient
population investigated in the present study are shown in Table I. Patient risk factors included:
Hypertension (n=390; 55%); diabetes (n=147; 21%); hyperlipidemia
(n=101; 14%); renal dysfunction, which was defined by serum
creatinine >84 or >104 µmol/l in females and males,
respectively (n=115; 16%); MI (n=90; 13%); and pharmacological
intervention, including treatment with β-blockers, calcium
antagonists, diuretics, nitrates, antiplatelet agents, statins,
angiotensin converting enzyme inhibitor and angiotensin receptor
blocker. A total of 415 and 293 patients exhibited BNP ≤80 and
>80 pg/ml, respectively. During follow-up, 144 endpoint events
occurred, including 67 and 77 in the BNP ≤80 pg/ml and >80 pg/ml
groups, respectively. Among the two patient groups, mortality and
readmission rates were 32 (4.5%) and 112 (15.8%), respectively.
Mortality rates were significantly higher in the BNP >80 pg/ml
group, as compared with the BNP ≤80 pg/ml group (P<0.05);
whereas readmission was markedly elevated in the BNP ≤80 pg/ml
group, as compared with the BNP >80 pg/ml group. A total of 677
patients underwent echocardiograph detection at the same time,
including 499 (73.7%) patients with diastolic dysfunction and 277
(40.9%) patients with systolic dysfunction. The incidence of
endpoint events was significantly elevated in the BNP >80 pg/ml,
as compared with the BNP ≤80 pg/ml group (26.28 vs. 16.14%;
RR=1.63).
 | Table I.Baseline clinical characteristics of
patients grouped according to BNP level. |
Table I.
Baseline clinical characteristics of
patients grouped according to BNP level.
| Parameter | BNP ≤80 pg/ml
(%) | BNP >80 pg/ml
(%) | P-value |
|---|
| Patients (n) | 415 | 293 | – |
| Age (years) | 62
(54–72) | 74 (64–78.75) | <0.05 |
| Male (%) | 226 (54) | 169 (57) |
0.395 |
| Mortality (%) | 3
(0.72) | 29 (9.90) | <0.05 |
| Readmission
(%) | 64
(15.42) | 48
(16.38) |
0.73 |
| Endpoint
events | 67
(16.14) | 77
(26.28) |
0.001 |
| Diastolic
dysfunction | 297/397
(74.81) | 202/280
(72.14) |
0.451 |
| Systolic
dysfunction | 112/397
(28.21) | 165/280
(58.93) | <0.05 |
| Hypertension | 208 (50.12) | 182 (62.12) |
0.002 |
| Diabetes | 77
(18.55) | 70
(23.89) |
0.085 |
| Hyperlipidemia | 74
(17.83) | 27 (9.22) |
0.001 |
| Renal failure | 29 (6.99) | 86
(29.35) | <0.05 |
| Myocardial
infarction | 43
(10.36) | 47
(16.04) |
0.025 |
| Medications: |
|
|
|
|
β-blockers | 245 (59.04) | 148 (50.51) |
0.025 |
| Calcium
antagonists | 139 (33.49) | 99
(33.79) |
0.935 |
|
Diuretic | 126 (30.36) | 230 (78.50) | <0.05 |
|
Nitrates | 214 (51.57) | 141 (48.12) |
0.367 |
|
Antiplatelet agents | 328 (79.04) | 217 (74.06) |
0.121 |
|
Statins | 118 (28.43) | 79
(26.96) |
0.667 |
| ACEI or
ARB | 323 (77.83) | 239 (81.57) |
0.226 |
|
ACEI | 168 (40.48) | 127 (43.34) |
0.447 |
|
ARB | 155 (37.35) | 112 (38.23) |
0.813 |
Patient survival times decrease as BNP
levels increase
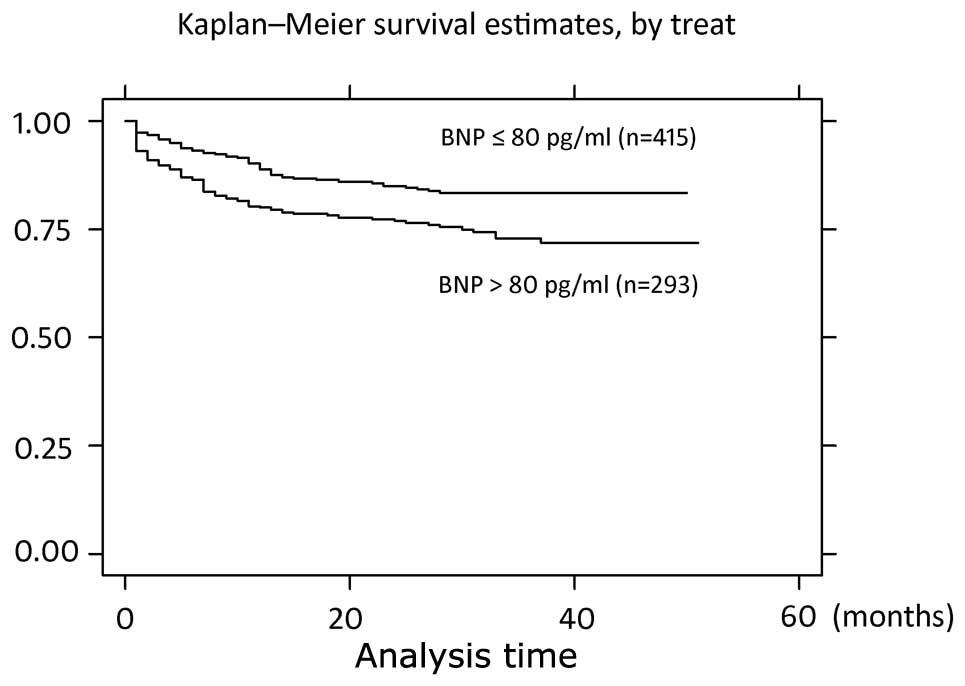
Kaplan-Meier analysis survival curves of patients
grouped according to initial BNP levels are shown in Fig. 1. This analysis was performed in order
to investigate whether the survival time of patients in the BNP ≤80
pg/ml group was increased compared with patients in the BNP >80
pg/ml group. The results demonstrated that patients in the BNP ≤80
pg/ml group survived significantly longer, as compared with the BNP
>80 pg/ml group (P=0.0006; log rank=11.74).
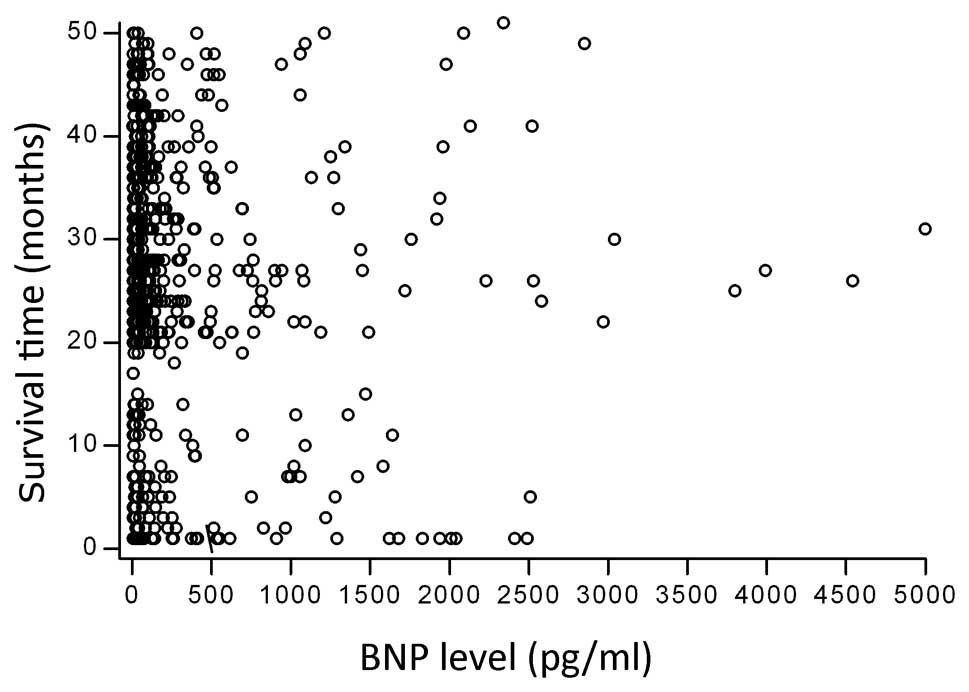
Spearman correlation analysis demonstrated that the
survival time of the 708 patients enrolled in the present study
markedly decreased as BNP levels increased (Spearman's rho=−0.1006;
P=0.0074). This negative correlation between the log BNP levels and
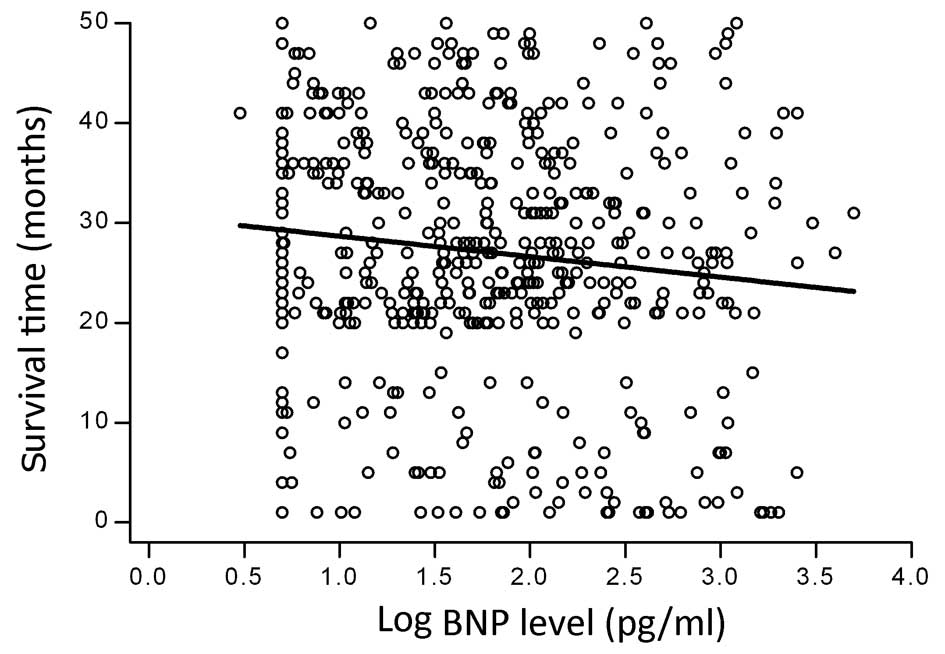
survival time is shown in Fig. 2. No
significant correlation was detected between BNP levels and
survival time in the 178 patients with normal LV diastolic function
(Spearman's rho=−0.931; P=0.2165) and 277 patients with systolic
dysfunction (Spearman's rho=−0.0007; P=0.9904)' whereas a negative
correlation was detected in the 499 patients with LV diastolic
dysfunction (E/A≤1) (Spearman's rho=−0.0899; P=0.0447). A scatter
plot demonstrating the correlation between the log BNP level and
duration of survival in patients with diastolic dysfunction are
shown in Fig. 3.
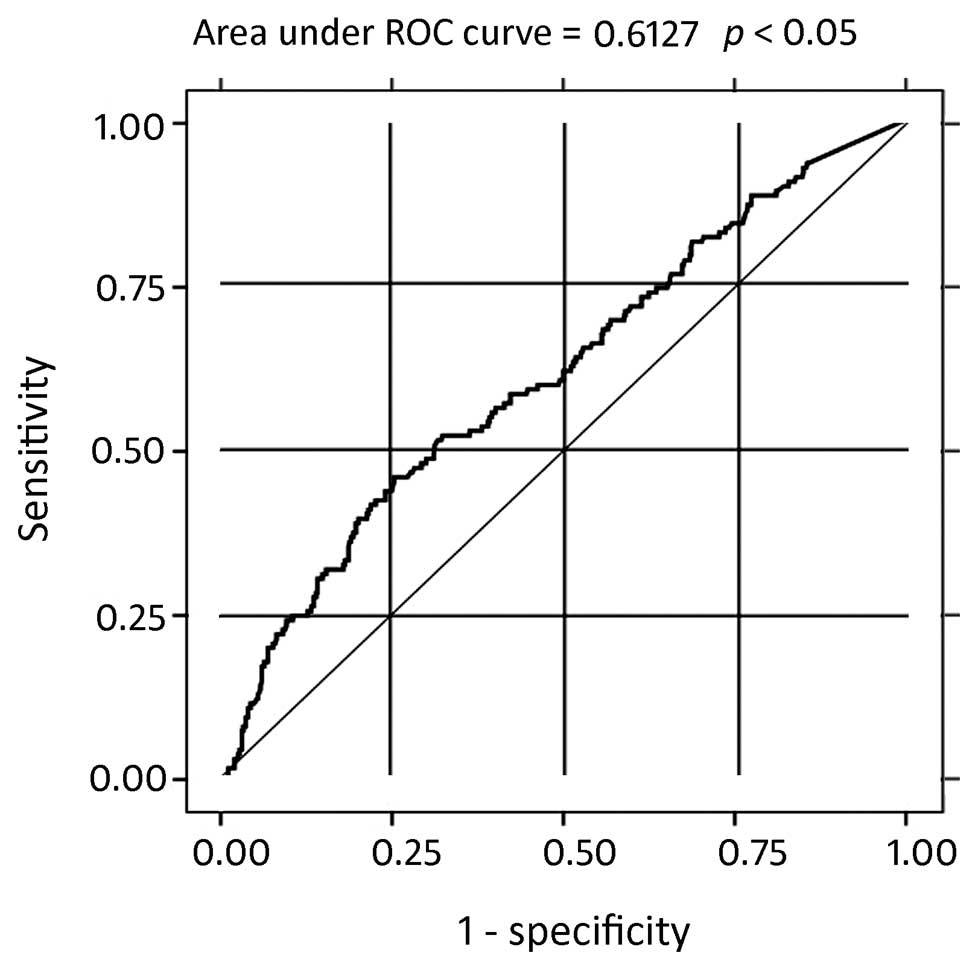
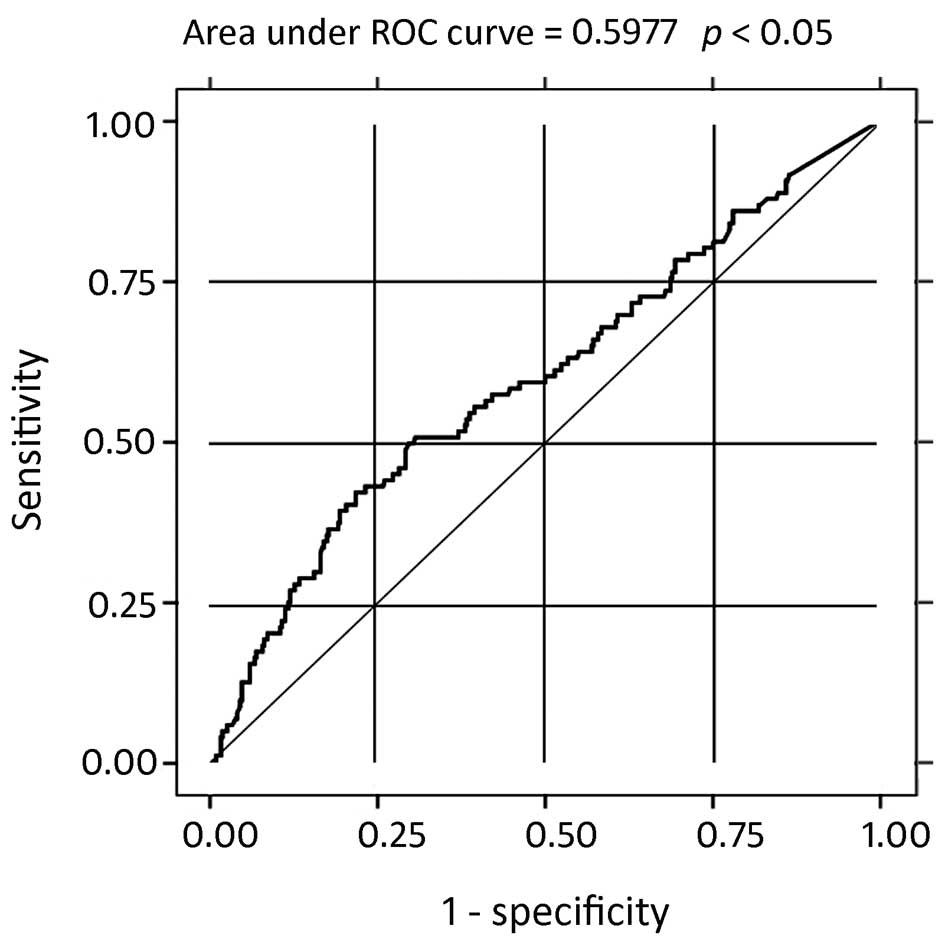
BNP levels can predict clinical
endpoints in patients with diastolic dysfunction
The predictive utility of plasma BNP levels for the
determination of compound clinical endpoints was calculated via ROC
analysis in all patients. The area under the ROC curve was 0.6127
[standard error (SE)=0.0268; 95% confidence interval (CI)
0.56015–0.66531]. The cut-off value of the plasma BNP level was 80
pg/ml (Se, 53.47%; Sp, 61.7%) (Fig.
4 and Table II). In patients
with diastolic dysfunction, the area under the ROC curve was 0.5977
(SE=0.0345; 95% CI, 0.53020–0.66524). In this group, the cut-off
value of the plasma BNP level was 80 pg/ml (Se, 52.17%; Sp, 62.16%)
(Fig. 5 and Table III). No significant correlation was
detected between plasma BNP levels and the incidence of endpoint
events in patients with systolic dysfunction.
| Table II.Correlation between the log BNP level
and endpoint events in all patients. |
Table II.
Correlation between the log BNP level
and endpoint events in all patients.
|
| Endpoint
events |
|
|---|
|
|
|
|
|---|
| BNP level | Yes | No | Total |
|---|
| >80 pg/ml | 77 | 216 | 293 |
| ≤80 pg/ml | 67 | 348 | 415 |
| Total | 144 | 564 | 708 |
| Table III.Correlation between the log BNP level
and endpoint events in patients with diastolic dysfunction. |
Table III.
Correlation between the log BNP level
and endpoint events in patients with diastolic dysfunction.
|
| Endpoint
events |
|
|---|
|
|
|
|
|---|
| BNP level | Yes | No | Total |
|---|
| >80 pg/ml | 48 | 154 | 202 |
| ≤80 pg/ml | 44 | 253 | 297 |
| Total | 92 | 407 | 499 |
Discussion
BNP is a cardiac neurohormone secreted from the
ventricles into the plasma in response to ventricular volume
expansion and pressure overload (3).
It has previously been demonstrated that the determination of BNP
levels provides a straightforward method for the early detection of
HF, the assessment of HF severity and the effectiveness of
treatment (13). A previous study
(14) has shown that both BNP and
NT-proBNP are strong prognostic markers for numerous acute coronary
syndromes, including patients with unstable angina, non-ST and
ST-elevation MI (15–17) and stable angina pectoris (18,19). In
the absence of significant necrosis (20), BNP and NT-proBNP are present in human
coronary arteries (21) and are
associated with the extent and severity of coronary atherosclerotic
lesions (22). The results of the
present study were consistent with these previous findings; the
number of patients who suffered a MI was significantly elevated in
the BNP >80 pg/ml group, as compared with the BNP ≤80 pg/ml
group (P=0.025). It has previously been suggested that ischemia may
act as a stimulus for the release of BNP and NT-proBNP (23). Sympathetic nervous overactivity in
the left ventricle has been demonstrated to be an important
mechanism for the induction of BNP elevation in chronic ischemic HF
(4). Furthermore, previous studies
have shown that ventricular BNP gene expression is upregulated by
acute myocardial hypoxia, which results in increased plasma BNP and
proBNP levels (24,25).
NT-proBNP is independent of invasive measurements of
LV function and the severity of coronary artery disease (19). Previous studies have investigated the
prognostic importance of measuring BNP and NT-proBNP levels in
patients with HF and acute coronary syndromes, and both markers
were demonstrated to be strong and independent predictors of
morbidity and mortality (19,26,27).
These predictors were also detected in >60% of the subgroup of
patients with LV ejection fraction and in patients with diabetes
mellitus (28). Kragelund et
al (19) demonstrated that, when
measured immediately prior to coronary angiography, NT-proBNP
provides prognostic information on mortality in patients with
stable coronary heart disease (19).
The results of the present study were consistent with these
findings and suggest that BNP demonstrates the same prognostic
value as previous studies. The incidence of clinical endpoints,
which included mortality or readmission due to cardiovascular
disease, or mortality due to any other reason, was significantly
higher in the BNP >80 pg/ml group, as compared with the BNP ≤80
pg/ml group. Furthermore, Kaplan-Meier analysis survival curves
suggested a negative correlation between the log BNP level and
survival duration in patients with cardiovascular disease. Patients
in the BNP ≤80 pg/ml group survived significantly longer, as
compared with the BNP >80 pg/ml group (P=0.0006, log
rank=11.74); therefore, survival duration reduced as BNP levels
increased.
In the present study, a cut-off value of 80 pg/ml
plasma BNP was used for the prediction of cardiovascular morbidity
and mortality from all death causes, including cardiovascular
diseases (Se, 53.47%; Sp, 61.7%). BNP or NT-proBNP have previously
been shown to have a high negative predictive value as a single
test (29), and the results of the
present study were consistent with these findings. The present
study assessed inpatients with various diseases, including, but not
limited to, hypertension, diabetes, hyperlipidemia, renal failure
and MI, between May 2006 and December 2008 at the Division of
Cardiology (Jinshan Hospital of Fudan University). The results
demonstrated that BNP levels may be used for the prediction of
various cardiovascular diseases, rather than one or several
specific diseases. Therefore, the present study demonstrated the
wider application of BNP as a predictor, as compared with previous
studies (7–9).
A previous study has demonstrated that 40–50% of
individuals with HF have a normal ejection fraction, and diastolic
dysfunction is the presumed cause of diastolic HF (DHF) (30). Abnormalities in diastolic function
are often misdiagnosed as this condition does not always produce
signs and symptoms of HF, which leaves patients predisposed to
symptomatic HF and cardiac necrosis due to the delay in treatment
(31). The early diagnosis of LV
diastolic dysfunction during its initial phase facilitates the
initiation of effective treatment with the purpose of halting the
progress of the disease and delaying the development of symptomatic
HF (32). Echocardiography, using
both Doppler measurements of transmitral and pulmonary vein blood
flow velocities and tissue Doppler imaging, is a widely accepted
method for the clinical analysis of diastole (33). However, these assessments are: i)
Costly due to the requirement of complex equipment; ii)
time-consuming, as they involves the analysis of various variables;
and iii) difficult, therefore they must be performed by a trained
operator (34). Therefore, a simple,
objective, high sensitivity and high specificity method for the
evaluation of diastole function is required. An association between
BNP levels and the indices of diastolic function has previously
been described in patients with reduced and preserved LVEF
(35). Previous studies have
demonstrated that the estimation of BNP values provides a fast and
reliable blood test in the diagnosis of asymptomatic diastolic
dysfunction (7,8). In particular, the BNP test has
previously been evaluated for the prediction of asymptomatic
diastolic dysfunction in patients with hypertension (7); and BNP levels may be determined in
order to evaluate occult LV dysfunction in patients who are
periodically assessed for diabetic complications (8). Furthermore, Panou et al
(9) have demonstrated that BNP
assessment may be used as an adjunctive, reliable and objective way
of estimating cardiac dysfunction in HCM (9). These findings were supported by a
subsequent study that demonstrated that assessment of BNP levels
can be easily and rapidly performed in emergency departments to
guide therapy, follow the response to therapy and predict the
exercise capacity of patients (10).
The results of the present study indicated that patients with
elevated BNP levels suffered poorer prognoses, as compared with
those with lower BNP levels. A negative correlation between BNP
levels and survival time was detected in patients with LV diastolic
dysfunction (n=499), and survival time decreased as BNP levels
rose. Furthermore, the predictive utility of plasma BNP levels for
the determination of compound clinical endpoints was demonstrated
in patients with diastolic dysfunction. In patients with diastolic
dysfunction enrolled in the present study, morbidity and mortality
associated with cardiovascular diseases were increased in patients
with elevated plasma BNP levels, as compared with patients with
lower BNP levels. In patients with systolic dysfunction, no
significant correlation or predictive value was detected between
plasma BNP levels and survival time and morbidity and mortality
from cardiovascular diseases.
The findings of the present study are consistent
with a previous study which has suggested that diastolic wall
stress may have a stronger correlation with NT-proBNP levels, as
compared with systolic wall stress (6). In a previous study, BNP levels
exhibited higher sensitivity (85 vs. 63%) and positive predictive
values (69 vs. 55%), as compared with the assessment of NT-proBNP
levels; although the negative predictive values of BNP and
NT-proBNP remained similar (70 and 71%, respectively) (36). Furthermore, measuring BNP levels has
been demonstrated to have a higher sensitivity and positive
predictive value for the accurate diagnosis of severe LVSD, as
compared with measuring NT-proBNP levels (36). The plasma half-life of BNP in humans
is ~20 min, whereas the circulating half-life of NT-proBNP is ~120
min (37). Therefore, BNP level
determination may facilitate assessment of the current severity of
LV dysfunction, guide therapy and track the immediate response to
therapy, whereas the use of NT-proBNP levels for assessment would
lag by ~10 h. Clearance of BNP occurs via two main mechanisms: i)
Binding to clearance receptors; and ii) enzymatic degradation by
neutral endopeptidase (38).
Clearance of NT-proBNP predominantly occurs via the kidney and
NT-proBNP levels significantly rise during mild renal failure,
which seriously affects the utility of NT-proBNP for diagnosis
(39,40), as ~29% of patients with HF suffer
from renal failure (41). In
patients aged ≥65, the BNP assay is a more useful diagnostic
indicator for cardiogenic pulmonary edema, as compared with proBNP
(39). The estimated glomerular
filtration rate has independent effects upon plasma BNP and
NT-proBNP concentrations in patients with chronic kidney disease,
and NT-proBNP appears to be more severely affected by declining
kidney function (42). Therefore,
based on these findings and the results of the present study, the
use of plasma BNP levels may result in a reliable and effective
assessment of prognosis in patients with cardiovascular
diseases.
The present study had several limitations. Firstly,
the number of patients enrolled in the study was small and the
follow-up period was relatively short. Therefore, future studies
with a larger sample of patients should be conducted over a longer
period in order to assess the predictive value of BNP in patients
with cardiovascular-related disease, particularly patients with LV
diastolic dysfunction. Secondly, echocardiographic parameters
should be interpreted with caution as the E/A may be affected by
rapid ventricular rate and atrial fibrillation. Thirdly, the
sensitivity and specificity of the predictive utility of plasma BNP
levels for the determination of compound clinical endpoints in all
patients or patients with LV diastolic dysfunction was not
particularly high. In a previous study, the combination of
NT-proBNP or BNP with LVEF substantially improved the risk
stratification for mortality, HF, and new ischemic events (43).
In conclusion, the prognoses of patients with
elevated BNP levels were correspondingly worse when compared with
patients with lower BNP levels. This correlation was demonstrated
to be significant in patients with LV diastolic dysfunction.
Therefore, the results of the present study suggested that BNP
levels may be used to predict the prognosis of patients with
cardiovascular disease, particularly in patients with LV diastolic
dysfunction.
Acknowledgements
We would like to thank Miss Feng-Ping Zhu for data
collection and Dr Lei-Jun Huang from Echo Laboratory for the
measurements of cardiographs.
References
|
1
|
Epshteyn V, Morrison K, Krishnaswamy P,
Kazanegra R, Clopton P, Mudaliar S, Edelman S, Henry R and Maisel
A: Utility of B-type natriuretic peptide (BNP) as a screen for left
ventricular dysfunction in patients with diabetes. Diabetes Care.
26:2081–2087. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Magnusson M, Melander O, Israelsson B,
Grubb A, Groop L and Jovinge S: Elevated plasma levels of NT-proBNP
in patients with type 2 diabetes without overt cardiovascular
disease. Diabetes Care. 27:1929–1935. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kremastinos DT, Tsiapras DP, Kostopoulou
AG, Hamodraka ES, Chaidaroglou AS and Kapsali ED: NT-proBNP levels
and diastolic dysfunction in beta-thalassaemia major patients. Eur
J Heart Fail. 9:531–536. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sakata K, Iida K, Mochiduki N and Nakaya
Y: Brain natriuretic peptide (BNP) level is closely related to the
extent of left ventricular sympathetic overactivity in chronic
ischemic heart failure. Inter Med. 48:393–400. 2009. View Article : Google Scholar
|
|
5
|
McKie PM, Rodeheffer RJ, Cataliotti A,
Martin FL, Urban LH, Mahoney DW, Jacobsen SJ, Redfield MM and
Burnett JC Jr: Amino-terminal proB-type natriuretic peptide and
B-type natriuretic peptide: Biomarkers for mortality in a large
community-based cohort free of heart failure. Hypertension.
47:874–880. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Krittayaphong R, Boonyasirinant T,
Saiviroonporn P, Thanapiboonpol P, Nakyen S and Udompunturak S:
Correlation between NT-pro BNP levels and left ventricular wall
stress, sphericity index and extent of myocardial damage: A
magnetic resonance imaging study. J Card Fail. 14:687–694. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Karaca I, Gülcü E, Yavuzkir M, Dağli N,
Ilkay E, Ozbay Y, Işik A and Arslan N: B-type natriuretic peptide
level in the diagnosis of asymptomatic diastolic dysfunction.
Anadolu Kardiyol Derg. 7:262–267. 2007.PubMed/NCBI
|
|
8
|
Kremastinos DT, Hamodraka E, Parissis J,
Tsiapras D, Dima K and Maisel A: Predictive value of B-type
natriuretic peptides in detecting latent left ventricular diastolic
dysfunction in beta-thalassemia major. Am Heart J. 159:68–74. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Panou FK, Kotseroglou VK, Lakoumentas JA,
Chrysanthopoulou SA, Armeniakos JA, Stratigou T, Veve H and
Zacharoulis AA: Significance of brain natriuretic peptide in the
evaluation of symptoms and the degree of left ventricular diastolic
dysfunction in patients with hypertrophic cardiomyopathy. Hellenic
J Cardiol. 47:344–351. 2006.PubMed/NCBI
|
|
10
|
Eroglu S, Yildirir A, Bozbas H, Aydinalp
A, Ulubay G, Eldem O, Simsek V, Ozin B and Muderrisoglu H: Brain
natriuretic peptide levels and cardiac functional cpacity in
patients with dyspnea and isolated diastolic dysfunction. Int Heart
J. 48:97–106. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gong H, Wang X, Ling Y, Shi Y and Shi H:
Prognostic value of brain natriuretic peptide in patients with
heart failure and reserved left ventricular systolic function. Exp
Ther Med. 7:1506–1512. 2014.PubMed/NCBI
|
|
12
|
Teichholz LE, Kreulen T, Herman MV and
Gorlin R: Problems in echocardiographic volume determinations:
Echocardiographic-angiographic correlations in the presence of
absence of asynergy. Am J Cardiol. 37:7–11. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
He Q, Wu G and Lapointe MC: Isoproterenol
and cAMP regulation of the human brain natriuretic peptide gene
involves Src and Rac. Am J Physiol Endocrinol Metab.
278:E1115–E1123. 2000.PubMed/NCBI
|
|
14
|
Suo M, Hautala N, Földes G, Szokodi I,
Tóth M, Leskinen H, Uusimaa P, Vuolteenaho O, Nemer M and Ruskoaho
H: Posttranscriptional control of BNP gene expression in
angiotensin II-induced hypertension. Hypertension. 39:803–808.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
James SK, Lindahl B, Siegbahn A,
Stridsberg M, Venge P, Armstrong P, Barnathan ES, Califf R, Topol
EJ, Simoons ML and Wallentin L: N-terminal pro-brain natriuretic
peptide and other risk markers for the separate prediction of
mortality and subsequent myocardial infarction in patients with
unstable coronary artery disease: A global utilization of
strategies to open occluded arreries (GUSTO)-IV substudy.
Circulation. 108:275–281. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Morrow DA, de Lemos JA, Blazing MA,
Sabatine MS, Murphy SA, Jarolim P, White HD, Fox KA, Califf RM and
Braunwald E: Investigators: Prognostic value of serial B-type
natriuretic peptide testing during follow-up of patients with
unstable coronary artery disease. JAMA. 294:2866–2871. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Morrow DA, de Lemos JA, Sabatine MS,
Murphy SA, Demopoulos LA, DiBattiste PM, McCabe CH, Gibson CM,
Cannon CP and Braunwald E: Evaluation of B-type natriuretic peptide
for risk assessment in unstable angina/non-ST-elevation myocardial
infarction: B-type natriuretic peptide and prognosis in
TACTICS-TIMI 18. J Am Coll Cardiol. 41:1264–1272. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ceriani L and Giovanella L: Cardiac
natriuretic peptides after myocardial infarction: Relationship with
infarct size, left ventricular function and remodelling assessed by
99mTc-sestamibi gated-single photon emission tomography. Clin Chem
Lab Med. 45:226–231. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kragelund C, Grønning B, Køber L,
Hildebrandt P and Steffensen R: N-terminal pro-B-type natriuretic
peptide and long-term mortality in stable coronary heart disease. N
Engl J Med. 352:666–675. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Barbosa MM, Nunes Mdo C, Castro LR,
Nominato LF, Alencar MC and Ribeiro AL: Correlation between NT-pro
BNP levels and early mitral annulus velocity (E') in patients with
non-ST-segment elevation acute coronary syndrome. Echocardiography.
25:353–359. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Casco VH, Veinot JP, de Kuroski Bold ML,
Masters RG, Stevenson MM and de Bold AJ: Natriuretic peptide system
gene expression in human coronary arteries. J Histochem Cytochem.
50:799–809. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Weber M, Dill T, Arnold R, Rau M, Ekinci
O, Müller KD, Berkovitsch A, Mitrovic V and Hamm C: N-terminal
B-type natriuretic peptide predicts extent of coronary artery
disease and ischemia in patients with stable angina pectoris. Am
Heart J. 148:612–620. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Omland T: B-type natriuretic peptides:
Prognostic markers in stable coronary artery disease. Expert Rev
Mol Diagn. 8:217–225. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Goetze JP, Christoffersen C, Perko M,
Arendrup H, Rehfeld JF, Kastrup J and Nielsen LB: Increased cardiac
BNP expression associated with myocardial ischemia. FASEB J.
17:1105–1107. 2003.PubMed/NCBI
|
|
25
|
Goetze JP, Gore A, Møller CH, Steinbrüchel
DA, Rehfeld JF and Nielsen LB: Acute myocardial hypoxia increases
BNP gene expression. FASEB J. 18:1928–1930. 2004.PubMed/NCBI
|
|
26
|
Omland T, Persson A, Ng L, O'Brien R,
Karlsson T, Herlitz J, Hartford M and Caidahl K: N-terminal
pro-B-type natriuretic peptide and long-term mortality in acute
coronary syndromes. Circulation. 106:2913–2918. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
de Lemos JA, Morrow DA, Bentley JH, Omland
T, Sabatine MS, McCabe CH, Hall C, Cannon CP and Braunwald E: The
prognostic value of B-type natriuretic peptide in patients with
acute coronary syndromes. N Engl J Med. 345:1014–1021. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kragelund C, Gustafsson I, Omland T,
Grønning B, Køber L, Faber J, Strande S, Steffensen R and
Hildebrandt P: Prognostic value of NH2-terminal proB-type
natriuretic peptide in patients with diabetes and stable coronary
heart disease. Diabetes Care. 29:1411–1413. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kelder JC, Rutten FH and Hoes AW:
Clinically relevant diagnostic research in primary care: The
example of B-type natriuretic peptides in the detection of heart
failure. Fam Pract. 26:69–74. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Redfield MM, Jacobsen SJ, Burnett JC Jr,
Mahoney DW, Bailey KR and Rodeheffer RJ: Burden of systolic and
diastolic ventricular dysfunction in the community: Appreciating
the scope of the heart failure epidemic. JAMA. 289:194–202. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shimabukuro M, Higa N, Oshiro Y, Asahi T
and Takasu N: Diagnostic utility of brain-natriuretic peptide for
left ventricular diastolic dysfunction in asymptomatic type 2
diabetic patients. Diabetes Obes Metabo. 9:323–329. 2007.
View Article : Google Scholar
|
|
32
|
Görmüş U, Ozmen D, Ozmen B, Parildar Z,
Ozdoğan O, Mutaf I and Bayindir O: Serum N-terminal-pro-brain
natriuretic peptide (NT-pro-BNP) and homocysteine levels in type 2
diabetic patients with asymptomatic left ventricular diastolic
dysfunction. Diabetes Res Clin Pract. 87:51–56. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Metra M, Ponikowski P, Dickstein K,
McMurray JJ, Gavazzi A, Bergh CH, Fraser AG, Jaarsma T, Pitsis A,
Mohacsi P, et al: Advanced chronic heart failure: A position
statement from the study group on advanced heart failure of the
heart failure association of the european society of cardiology.
Eur J Heart Fail. 9:684–694. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Nagueh SF, Appleton CP, Gillebert TC,
Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka
PA and Evangelista A: Recommendations for the evaluation of left
ventricular diastolic function by echocardiography. J Am Soc
Echocardiogr. 22:107–133. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Grewal J, McKelvie R, Lonn E, Tait P,
Carlsson J, Gianni M, Jarnert C and Persson H: BNP and NT-proBNP
predict echocardiographic severity of diastolic dysfunction. Eur J
Heart Fail. 10:252–259. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kotaska K, Popelova J, Tiserova M, Telekes
P, Vrzanova M, Bronsky J, Halacova M, Kukacka J and Prusa R:
NT-proBNP and BNP values in cardiac patients with different degree
of left ventricular systolic dysfunction. Biomed Pap Med Fac Univ
Palacky Olomouc Czech Repub. 150:125–130. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mair J, Hammerer-Lercher A and Puschendorf
B: The impact of cardiac natriuretic peptide determination on the
diagnosis and management of heart failure. Clin Chem Lab Med.
39:571–588. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ruskoaho H: Cardiac hormones as diagnostic
tools in heart failure. Endor Rev. 24:341–356. 2003. View Article : Google Scholar
|
|
39
|
Ray P, Arthaud M, Birolleau S, Isnard R,
Lefort Y, Boddaert J and Riou B: Comparison of brain natriuretic
peptide and probrain natriuretic peptide in the diagnosis of
cardiogenic pulmonary edema in patients ages 65 and older. J Am
Geriatr Soc. 53:643–648. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Sykes E, Karcher RE, Eisenstadt J, Tushman
DA, Balasubramaniam M, Gusway J and Perason VJ: Analytical
relationships among Biosite, Bayer and Roche methods for BNP and
NT-proBNP. Am J Clin Pathol. 123:584–590. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Fonarow GC ADHERE Scientific Advisory
Committee: The acute decompensated heart failure national registry
(ADHERETM): Opportunities to improve care of patients hospitalized
with acute decompensated heart failure. Rev Cardiovasc Med. 4(Suppl
7): S21–S30. 2003.
|
|
42
|
Vickery S, Price CP, John RI, Abbas NA,
Webb MC, Kempson ME and Lamb EJ: B-type natriuretic peptide (BNP)
and amino-terminal proBNP in patients with CKD: Relationship to
renal function and left ventricular hypertrophy. Am J Kidney Dis.
46:610–620. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Richards AM, Nicholls MG, Espiner EA,
Lainchbury JG, Troughton RW, Elliott J, Frampton C, Turner J,
Crozier IG and Yandle TG: B-type natriuretic peptides and ejection
fraction for prognosis after myocardial infarction. Circulation.
107:2786–2792. 2003. View Article : Google Scholar : PubMed/NCBI
|