Introduction
Congenital cataract is a severe eye disease with a
complex pathogenesis that causes blindness in children. The
development of genomics research has allowed the in-depth study of
the cataract pathogenesis (1,2). During
embryogenesis, viral and parasitic infections may influence the
development of congenital cataract (3–5).
Lifestyle changes, including changes in modern human sexuality and
co-habitation with pets has resulted in increased herpes simplex
virus (HSV) and toxoplasma (TOX) infection rates among pregnant
women (6,7). In addition, the incidence of adverse
pregnancy outcomes, including congenital cataracts, has also
increased (6). A recent survey by Li
et al (8) reported a primary
infection of TOX, rubella virus (RV), cytomegalovirus (CMV) or HSV,
abbreviated as TORCH infection, positivity rate of 17.2% among
pregnant women living in Beijing, with the highest positivity rates
being those of HSV immunoglobulin (Ig)M. These infections with
TORCH during pregnancy can produce an embryopathy characterized by
limb hypoplasia, eye and brain damage, skin lesions, and even
death. The infection typically gains access to the fetus via the
placenta (8). Following an
investigation into the lifestyle habits of 2,356 pregnant women
from 2005 to 2007, including a survey on pets, raw food diets,
living conditions, and other lifestyle habits, Thaller et al
(9) demonstrated that there was an
increased incidence of infection with TOX among pregnant women
living in rural areas who ate homemade bacon. Following infection,
the immune systems of the pregnant women produce a series of
antibodies that are transferred to the developing fetus through the
placenta, and remain present for a specific period of time
following birth (10). Mahalakshmi
et al (10) reported an
association between IgM antibodies against TORCH pathogens and
congenital cataracts in a retrospective study of 593 children in
Tamil Nadu Hospital of Chennai, India, using ELISA.
The present study aimed to determine the positivity
rates of TORCH serum IgG and IgM antibodies in children with
congenital cataracts, and compare these with the positivity rates
in the non-TORCH control group; this includes assessment of the
differences between single and double eye disease which are
associated with TORCH infection. The study also examined any
statistically significant differences in HSV II IgG levels in
children with congenital cataracts.
Materials and methods
Study subjects
The study population consisted of a cataract and a
control group. The cataract group included 69 children with
congenital cataracts who were diagnosed and admitted to the
Children's Hospital, Zhejiang University School of Medicine
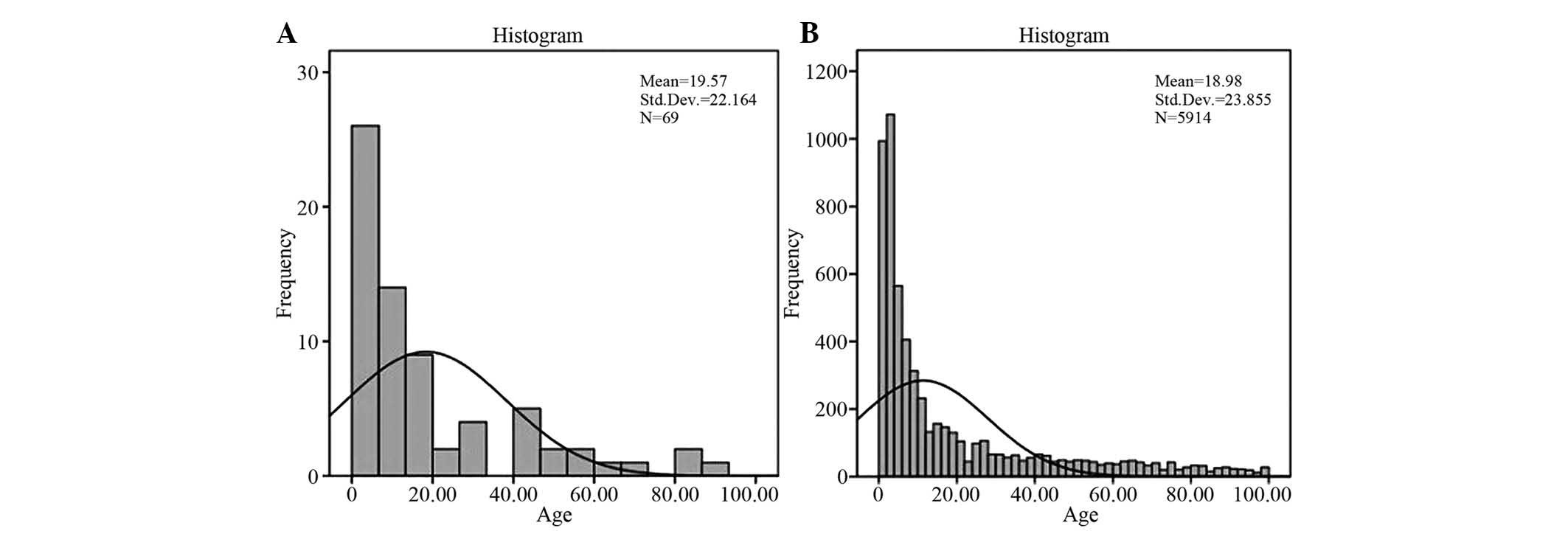
(Hangzhou, China) for surgical treatment. There were 33 boys and 36
girls, aged 1 month and 9 days to 7 years and 7 months, with an
average age of 19.57±22.164 months. Among these, 32 cases of
children with monocular cataracts and 37 cases of children with eye
cataracts in both eyes were included. The human immunodeficiency
virus (HIV) and Treponema pallidum-specific passive
hemagglutination assays (TPHA) of the children were negative. Cases
that had a clear family history of genetic cataracts were excluded
from the study.
The control group consisted of 5,914 randomly
selected outpatients who were treated during the same time period
(between years 2006 and 2013), including 2,843 boys and 3,071 girls
aged 1 month to 7 years and 5 months (average age, 18.98±23.855
months). Their family genetic histories and HIV and TPHA test
results were unknown.
All cases were TORCH-positive or negative and all
suspicious cases (weak positive of suspected positive cases)
reported as positive were excluded. The study was conducted in
accordance with the declaration of Helsinki, and with approval from
the Ethics Committee of the Children's Hospital, Zhejiang
University School of Medicine (Hangzhou, China). Written informed
consent was obtained from all the legal guardians of the
participants.
Collection of blood samples
A total of 1–2 ml peripheral fresh vein serum was
collected from each patient and placed in anticoagulant tubes (BD
Biosciences, Franklin Lakes, NJ, USA) at room temperature for ≤8 h.
The samples that would be used for testing after 8 h were
immediately stored at 2–10°C, and those that were expected to be
tested after 24 h were immediately stored at −20°C. All samples
were tested within 2 days of collection.
ELISA
ELISA was conducted using the following
immunoglobulin (Ig)G and IgM test kits (Trinity Biotech Plc,
Jamestown, NY, USA); TOX-IgM (cat. no. 2325160); TOX-IgG (cat. no.
2325100); RV-IgM (cat. no. 2325360); RV-IgG (cat. no. (2325300);
CMV-IgM (cat. no. 2325260); CMV-IgG (cat. no. 2325200); HSV1-IgM
(cat. no. 2325460); HSV1-IgG (cat. no. 2325400); HSV2-IgM (cat. no.
2325560) and HSV2-IgG (cat. no. 2325500).
Detection step
Measuring process of serum TORCH antibody (CMV-IgG
was the example, and the measuring procedure of other pathogens was
the same). The Immune Status Ratio (ISR) for each specimen was
calculated by dividing the specimen optical density value by the
Cutoff Calibrator Value determined by multiplying the Correction
Factor by the mean Calibrator optical density.
A 50 ml 20X concentrated buffer solution I
(Tris-buffered saline with Tween 20 and ProClin as a preservative)
was diluted with 1 L deionized water and mixed thoroughly. Gen5
version 2.0 (BioTek, Winooski, VT, USA) and BioTek Eon Microplate
Spectrophotometer (BioTek) was used for the assay procedure.
The required number of microtest strips were placed
onto a micropore frame. A total of 4 quality control materials and
calibrators (1 negative quality control material, 2 calibrators,
and 1 positive quality control material) were used in each test. A
reagent blank was also prepared for each experiment. The quality
control materials and calibrators were used to confirm that the
software and photometer were configured correctly. Desiccant was
added to the unused microtest strips, which were placed into a
sealable bag and immediately stored at 4°C.
The test serum, quality control materials, and
calibrators were diluted with serum diluent (provided in CMV IgG
ELISA kit) at a 1:81 ratio (10+800 µl) and agitated. A total of 100
µl of the diluted calibrators, quality control materials, and serum
were added to each well (96 well microassay plate), and 100 µl
sample dilution was added to the blank well. The quality control
materials and calibrators were confirmed to be correctly configured
for the software and photometer. Each well was incubated at room
temperature (21–25°C) for 30±2 min.
Subsequently, the liquid in the micropores was
removed, and 250–300 µl diluted buffer solution (serum diluent with
0.1% ProClin as a preservative) was added to each hole. The
microtest strips were washed once with washing buffer (provided in
CMV IgG ELISA kit) using an automatic plate washer. The liquid was
removed from the micropores and the microplate was placed upside
down on absorbent paper to remove the remaining liquid, and washed
five times. Following the final rinse, the microplate was again
placed upside down on absorbent paper to remove all the remaining
liquid. Taking care to avoid the formation of bubbles, 100 µl goat
anti-human IgG horseradish-peroxidase enzyme conjugate was added to
each well, including the blank well. Each well was incubated at
room temperature (21–25°C) for 30±2 min, then washed as described
above. Tetramethyl benzidine chromogenic agent substrate (100 µl;
Trinity Biotech Plc) was added to each well, including the blank
well. Each well was incubated at room temperature (21–25°C) for
15±2 min. A total of 100 µl stop buffer (1N H2S04) was then added
to each well to terminate the reaction, including the blank well.
The microplate was gently agitated to allow thorough mixing. The
absorbance of each well was read 1 h following the addition of the
stop buffer using a Victor ELISA analyzer (BioTek) at a wavelength
of 450 nm. The absorbance of the reagent blank at 450 nm was
<0.150. If the reagent blank absorbance was ≥0.150, the
experiments were repeated.
Calculation and interpretation of the
experimental results
The mean optical density (OD) values of the
reference samples (the two calibrators) were calculated. To account
for day-to-day fluctuations in assay activity due to room
temperature and timing, Trinity Biotech Plc (Bray, Ireland) was
used to determine the correction factor. The critical correction
value was the mean absorbance value of the calibrator calculated in
the first step multiplied by the correction factor. The ISR value
of each sample was the OD value of each sample divided by the
critical correction value. This is a qualitative kit, and the
reference values were the cut-off values and the ISR values. The
ISR values were used to determine the test results (Table I). The results of all antibody tests
assessed in the current study were based on the ISR values. The
following formulae were used: Cut-off value = mean OD value of the
calibrator × correction factor; ISR value = OD value of patient
serum samples/cut-off value.
 | Table I.Interpretation of the ISR values. |
Table I.
Interpretation of the ISR values.
| ISR value | Result | Interpretation |
|---|
| ≤0.9 | Negative | Following ELISA,
anti-CMV IgG antibody was not detected, and the individual was thus
considered to be uninfected by CMV, which is the pathogen with
which susceptible people are first infected. |
| 0.91–1.09 | Suspected | The sample will
require re-testing. |
| ≥1.10 | Positive | Following ELISA,
anti-CMV IgG antibodies were detected, which suggested that the
patient was recently or currently infected. These individuals may
be at risk of the spread of CMV infection, but they were not
necessarily infected at the time of the test. |
Statistical analysis
SPSS 19.0 software (IBM SPSS, Armonk, NY, USA) was
used for all statistical analyses. The ages of the children were
compared using independent sample t-tests, and completely
randomized design of four tables χ2 tests were applied
to gender in order to compare the positivity rates of anti-TORCH
antibodies between the cataract and control groups. According to
the 2×2 tables (0.0%), the theoretical frequency was calculated,
and based on this minimum expected count the appropriate P-values
for Pearson χ2, calibration χ2, and Fisher's
exact tests were determined. Data were presented as the mean ±
standard deviation. P<0.05 was considered to indicate a
statistically significant result.
Results
General characteristics
The age and gender of the cataract and control
groups had a skewed (non-normal) distribution (Fig. 1). Due to the fact that there were
>50 samples, Pearson χ2 tests were used to compare
the gender between the groups, whereas independent samples t-tests
were used to compare age. The results of both tests showed no
significant differences (P>0.05l Table II).
| Table II.Age and gender of the cataract and
control groups. |
Table II.
Age and gender of the cataract and
control groups.
| Parameter | Cataract group | Control group |
|---|
| Cases | 69 | 5,914 |
| Gender |
|
|
|
Female | 36/69 (52.2%) | 2843/5914
(48.1%) |
| Male | 33/69 (47.8%) | 3071/5914
(51.9%) |
| Age (months) | 19.57±22.164 | 18.98±23.855 |
Comparison of TORCH antibodies between
the cataract and control groups
The rates of anti-HSV II IgG antibody positivity
were significantly higher in children with cataracts (P=0.014);
however, the differences in anti-HSV II IgM positivity rates
between these groups was not statistically significant (P>0.05).
Similarly, differences in the expression levels of IgG and IgM
specific to other TORCH pathogens were also not statistically
significant (P>0.05; Tables III
and IV).
| Table III.Positive rates of anti-TORCH pathogen
IgG antibodies in the cataract and control groups. |
Table III.
Positive rates of anti-TORCH pathogen
IgG antibodies in the cataract and control groups.
| Group | N | HSV II IgG | HSV I IgG | RV IgG | TOX IgG | CMV IgG |
|---|
| Cataract group | 69 | 5/69 (7.20%) | 7/69 (10.10%) | 4/69 (5.80%) | 0/69 (0.00%) | 16/69 (23.20%) |
| Control group | 5,914 | 127/5,914
(2.10%) | 660/5,914
(11.20%) | 115/5,914 (2.6
0%) | 14/5,914 (0.20%) | 1003/5,914
(17.00%) |
| Table IV.Positive rates of anti-TORCH pathogen
IgM antibodies in the cataract and control groups. |
Table IV.
Positive rates of anti-TORCH pathogen
IgM antibodies in the cataract and control groups.
| Group | N | HSV II IgM | HSV I IgM | RV IgM | TOX IgM | CMV IgM |
|---|
| Cataract group | 69 | 1/69 (1.40%) | 1/69 (1.40%) | 1/69 (1.40%) | 0/69 (0.00%) | 10/69 (15.50%) |
| Control group | 5,914 | 48/5,914
(0.80%) | 28/5,914
(0.50%) | 38/5,914
(0.60%) | 2/5,914
(0.00%) | 696/5,914
(11.80%) |
Comparison of TORCH pathogen
positivity rates between children with monocular cataracts and
children with binocular cataracts
The results of the χ2 tests demonstrated
that no significant differences in the incidences of anti-TORCH IgG
and IgM antibodies were present between children with monocular and
binocular congenital cataracts (P>0.05; Tables V and VI).
| Table V.Positive rates of anti-TORCH pathogen
IgG antibodies in the monocular cataract and binocular cataract
groups. |
Table V.
Positive rates of anti-TORCH pathogen
IgG antibodies in the monocular cataract and binocular cataract
groups.
| Group | N | HSV II IgG | HSV I IgG | RV IgG | TOX IgG | CMV IgG |
|---|
| Monocular cataract
group | 32 | 2/32 (6.30%) | 6/32 (18.80%) | 4/32 (12.50%) | 0/32 (0.00%) | 5/32 (15.60%) |
| Binocular cataract
group | 37 | 3/37 (8.10%) | 1/37 (2.70%) | 0/37 (0.00%) | 0/37 (0.00%) | 11/37 (29.70%) |
| Table VI.Positive rates of anti-TORCH pathogen
IgM antibodies in the monocular cataract and binocular cataract
groups. |
Table VI.
Positive rates of anti-TORCH pathogen
IgM antibodies in the monocular cataract and binocular cataract
groups.
| Group | N | HSV II IgM | HSV I IgM | RV IgM | TOX IgM | CMV IgM |
|---|
| Monocular cataract
group | 32 | 1/32 (3.10%) | 1/32 (3.10%) | 0/32 (0.00%) | 0/32 (0.00%) | 5/32 (15.60%) |
| Binocular cataract
group | 37 | 0/37 (0.00%) | 0/37 (0.00%) | 1/37 (2.70%) | 0/37 (0.00%) | 10/37 (14.50%) |
Discussion
Previous studies carried out on congenital cataracts
caused by viral infections have predominantly focused on the RV
(11). With regard to other
pathogens, Madhavan et al (12) reported that HSV infection was
associated with patients with congenital cataracts in India; Raghu
et al (13) demonstrated that
congenital cataracts were associated with HSV I infections;
Shyamala et al (14) detected
HSV II DNA in children with congenital cataracts; and Kuot et
al (15) reported a case of a
patient with early-onset Fuchs' corneal endothelial dystrophy
associated with congenital cataracts and keratitis due to HSV
infection. In addition, Hutchison et al (16) previously established an animal
cataract model of Toxoplasma gondii infection.
Infections with TORCH pathogens such as HSV may
affect the ectodermal tissues (17),
from which the lens is derived. The author assumes that lens
opacification after birth and existence of additional factors are
likely the result of intrauterine TORCH infections, which can be
identified by the detection of maternal IgG antibodies in the baby.
However, IgG and IgM antibodies after birth are derived from the
immune response generated by self-infection in children; therefore,
the presence of IgM antibodies after birth may not be sufficient to
definitively correlate the presence of TORCH pathogens with the
development of congenital cataracts. The results of the analysis of
both IgG and IgM antibodies in the present study correlated with
the results of Mahalakshmi et al (10). However, lens opacification after
birth in infants positive for IgG antibodies may reflect past
infection, whereas for children with congenital cataract for whom
lens opacification is not present at birth, congenital cataract is
defined as cataract occuring within 1 years after birth. Some
children with congenital cataract at birth have transparent lens,
and these children typically have TORCH pathogens marked by IgM.
These children are likely to have an intrauterine infection or a
mother with an infection, and may harbor disease-causing viruses
but without detectable clinical symptoms. Upon a second virus
infection, the immune system would be re-activated, triggering a
number of unknown biological mechanisms, finally leading to the
appearance of clinical symptoms, such as cloudy lens.
In a study of HSV I primary infections, Lafaille
et al (18) observed that
children with toll-like receptor 3 (TLR3) innate immune defects
were more prone to developing HSV I encephalitis. Impaired TLR3 and
UNC-93B, which depend on interferon-α/β innate immunity, can lead
to HSV I manifestations in the central nervous system, particularly
in neurons and oligodendrocytes (18). Nerve fibers have yet to be identified
in the lens, although if present these may serve as a major route
for HSV neuronal infection, and may also influence lens development
via other direct or indirect means, such as keratitis, uveitis and
retinitis (19). HSV II primarily
leads to skin infections of the genital tract and below the waist,
and infection of the fetus during pregnancy is more likely to occur
(20). In the present study, the
comparison of children with cataracts and the relatively large
sample sizes demonstrated that anti-HSV I antibody expression
levels were not high; however, anti-HSV II IgG levels were higher,
suggesting that HSV infections may be risk factors of congenital
cataracts.
Based on independent viral infection rates, Malathi
et al (21) suggested that
10% of congenital cataracts were due to RV infection, and that IgM
antibodies in children <6 months of age with congenital
cataracts may be associated with RV. Highlighting the diversity of
rubella syndrome, Ferrini et al (22) reported the case of a 12-month-old
girl who developed a cataract 3 months after receiving the RV
vaccine. Rubella infection rates were low in this study, and did
not differ significantly between groups.
The most common symptom of the ocular manifestations
of congenital toxoplasmosis is chorioretinitis (92%), followed by
small eye and squint, iridocyclitis, cataract and glaucoma
(23). Vandenbroucke et al
(24) reported a case of congenital
cataracts in a baby positive for TOX infection. However, TOX
testing in the present study revealed a low incidence of TOX
infection, and there were no statistically significant differences
between groups.
Thibault et al (25) suggested that there was no causal
association between CMV infection and congenital cataracts.
However, a study of factors associated with cataract protein gene
mutations including heat shock factor 4 (Hsf4b) conducted by Zhang
et al (26) suggested that
Hsf4b participates in the negative regulation of the CMV promoter
as a downstream monitoring factor with a dual function as a
transcriptional activator and inhibitor, affecting the channel
activity of the lens protein and other biological substances. In
addition, CMV often causes retinal choroidal inflammation, an eye
inflammation that leads to changes in the lens environment, which
is the basis for the formation of cataracts. Tran et al
(27) demonstrated that 26% of
necrotizing retinitis had cataracts. Given the higher levels of
anti-CMV antibodies in the cataract group compared with the control
group in the current study (CMV IgM: 15.50 vs. 11.80%; CMV-IgG:
23.20 vs. 17.00%) we recommend preventive treatment.
Traditionally, pediatric ophthalmology considers
bilateral cataracts in children to be due to genetic and systematic
diseases, whereas monocular cataracts are attributed to local
phenomenon or abnormal development of other ocular structures
(28). In the present study, there
were no significant differences in the expression levels of TORCH
pathogenic antibodies among children with monocular and binocular
congenital cataracts.
Previous studies have demonstrated that the in
vivo expression levels of anti-TORCH antibodies in women varies
according to country and region. Lito et al (29) reported anti-RV IgG positivity rates
of 93.3%, anti-TOX IgG rates of 25.7% and anti-CMV IgG rates of
62.4% among pregnant women in Portugal; Vilibic-Cavlek et al
(30) reported anti-TOX IgG
seropositivity rates of 29.1%, RV rates of 94.6%, CMV rates of
75.3%, HSV I rates of 78.7%, and HSV II rates of 6.8% among
pregnant women in Croatia. Anti-TOX and CMV IgM positivity rates
were 0.25 and 0.09% respectively, HSV I and HSV II were 1.2%, and
RV rates were 0%. Sen et al (31) reported anti-CMV IgM positivity rates
of 19.4%, anti-RV IgM rates of 30.4%, anti-CMV IgM rates of 34.7%,
and anti-HSV II IgM rates of 33.5% in Indian women. Puccio et
al (32) reported CMV infection
rates of 62.5 and 91.4% among residents and immigrants in Italy,
respectively. These results indicate that the areas with the
highest anti-TORCH IgG antibody positivity rates in pregnant women
were predominantly economically developed areas. Conversely, the
areas with the highest anti-TORCH IgM antibody positivity rates in
pregnant women in developing countries were predominantly located
in underdeveloped communities, in which the occurrence of
congenital cataracts was also higher (33). These results also suggest that TORCH
pathogen infections are a risk factor for congenital cataracts.
In order to correct for errors due to the small
sample size and to verify the trends identified when comparing
cases with congenital cataracts to unaffected cases, the present
study used a large number of control samples from the outpatient
children. As TORCH pathogen positivity rates were not high and the
size of the cataract sample in this study was relatively small, the
significance of the results were limited. The half-life of maternal
anti-HSV IgG antibodies in the serum of children is unknown, and it
may be expressed to higher levels in neonatal serum. Therefore, it
may be possible to obtain more significant results by evaluating
cataracts during the neonatal period.
References
|
1
|
Dave A, Craig JE and Sharma S: The status
of intercellular junctions in established lens epithelial cell
lines. Mol Vis. 18:2937–2946. 2012.PubMed/NCBI
|
|
2
|
Wang B, Wang KJ, Zhu SQ, Wang J and Ma X:
Identification of the p. R116H mutation in a chinese family with
novel variable cataract phenotype: Evidence for a mutational hot
spot in αA-crystallin gene. Ophthalmic Genet. 33:134–138. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Matoba A: Ocular viral infections. Pediatr
Infect Dis. 3:358–368. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cotlier E: Congenital varicella cataract.
Am J Ophthalmol. 86:627–629. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lambert SR, Fernandes A, Drews-Botsch C
and Boothe RG: Multifocal versus monofocal correction of neonatal
monocular aphakia. J Pediatr Ophthalmol Strabismus. 31:195–201.
1994.PubMed/NCBI
|
|
6
|
Barah F: Prevalence of herpes simplex
types 1 and 2, varicella zoster virus, cytomegalovirus,
immunoglobulin G antibodies among female university students in
Syria. Saudi Med J. 33:990–994. 2012.PubMed/NCBI
|
|
7
|
Akinbami AA, Adewunmi AA, Rabiu KA, Wright
KO, Dosunmu AO, Dada MO and Adevemo TA: Seroprevalence of
Toxoplasma gondii antibodies amongst pregnant women at the
Lagos State University Teaching Hospital, Nigeria. Niger Postgrad
Med J. 17:164–167. 2010.PubMed/NCBI
|
|
8
|
Li Z, Yan C, Liu P, Yan R and Feng Z:
Prevalence of serum antibodies to TORCH among women before
pregnancy or in the early period of pregnancy in Beijing. Clin Chim
Acta. 403:212–215. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Thaller R, Tammaro F and Pentimalli H:
Risk factors for toxoplasmosis in pregnant women in central Italy.
Infez Med. 19:241–247. 2011.(In Italian). PubMed/NCBI
|
|
10
|
Mahalakshmi B, Therese KL, Devipriya U,
Pushpalatha V, Margarita S and Madhavan HN: Infectious aetiology of
congenital cataract based on TORCHES screening in a tertiary eye
hospital in Chennai, Tamil Nadu, India. Indian J Med Res.
131:559–564. 2010.PubMed/NCBI
|
|
11
|
Merdassi A, Limaiem R, Turki F, Chaker N,
Falfoul Y, Mghaieth F, Korchane N and Matri LE: Ophthalmologic
manifestations of congenital rubella. Arch Pediatr. 18:870–873.
2011.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Madhavan HN: Laboratory investigations on
viral and chlamydia trachomatis infections of the eye: Sankara
Nethralaya experiences. Indian J Ophthalmol. 47:241–246.
1999.PubMed/NCBI
|
|
13
|
Raghu H, Subhan S, Jose RJ, Gangopadhyay
N, Bhende J and Sharma S: Herpes simplex virus-1-associated
congenital cataract. Am J Ophthalmol. 138:313–314. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shyamala G, Sowmya P, Madhavan HN and
Malathi J: Relative efficiency of polymerase chain reaction and
enzyme-linked immunosorbant assay in determination of viral
etiology in congenital cataract in infants. J Postgrad Med.
54:17–20. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kuot A, Mills R, Craig JE, Sharma S and
Burdon KP: Screening of the COL8A2 gene in an Australian family
with early-onset Fuchs' endothelial corneal dystrophy. Clin
Experiment Ophthalmol. 42:198–200. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hutchison WM, Hay J, Lee WR and Siim JC: A
study of cataract in murine congenital toxoplasmosis. Ann Trop Med
Parasitol. 76:53–70. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Krummenacher C, Baribaud F, de Ponce Leon
M, Baribaud I, Whitbeck JC, Xu R, Cohen GH and Eisenberg RJ:
Comparative usage of herpesvirus entry mediator A and nectin-1 by
laboratory strains and clinical isolates of herpes simplex virus.
Virology. 322:286–299. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lafaille FG, Pessach IM, Zhang SY,
Ciancanelli MJ, Herman M, Abhyankar A, Ying SW, Keros S, Goldstein
PA, Mostoslavsky G, et al: Impaired intrinsic immunity to HSV-1 in
human iPSC-derived TLR3-deficient CNS cells. Nature. 491:769–773.
2012.PubMed/NCBI
|
|
19
|
Newman H and Gooding C: Viral ocular
manifestations: A broad overview. Rev Med Virol. 23:281–294. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ashshi AM, Batwa SA, Kutbi SY, Malibary
FA, Batwa M and Refaat B: Prevalence of 7 sexually transmitted
organisms by multiplex real-time PCR in fallopian tube specimens
collected from Saudi women with and without ectopic pregnancy. BMC
Infect Dis. 15:5692015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Malathi J, Therese KL and Madhavan HN: The
association of rubella virus in congenital cataract-a
hospital-based study in India. J Clin Virol. 23:25–29. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ferrini W, Aubert V, Balmer A, Munier FL
and Abouzeid H: Anterior uveitis and cataract after rubella
vaccination: A case report of a 12-month-old girl. Pediatrics.
132:e1035–e1038. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vutova K, Peicheva Z, Popova A, Markova V,
Mincheva N and Todorov T: Congenital toxoplasmosis: Eye
manifestations in infants and children. Ann Trop Paediatr.
22:213–218. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Vandenbroucke S, Foets B, Wouters C and
Casteels I: Bilateral congenital cataract with suspected
lens-induced granulomatous uveitis. J AAPOS. 18:492–494. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Thibault M, Leydet J, Tournier-Lasserve E,
Crow YJ, Rivier F, Echenne B, Langlois C, Daudet H, Sarda P and
Roubertie A: Genetic syndromes that mimic congenital infections:
Report of 2 cases. Arch Pediatr. 18:1297–1301. 2011.(In French).
PubMed/NCBI
|
|
26
|
Zhang J, Hu YZ, Xueli L, Li S, Wang M,
Kong X, Li T, Shen P and Ma Y: The inhibition of CMV promoter by
heat shock factor 4b is regulated by Daxx. Int J Biochem Cell Biol.
42:1698–1707. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tran TH, Bodaghi B, Rozenberg F, Cassoux
N, Fardeau C and LeHoang P: Viral cause and management of
necrotizing herpetic retinopathies. J Fr Ophtalmol. 27:223–236.
2004.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chan WH, Biswas S, Ashworth JL and Lloyd
IC: Congenital and infantile cataract: Aetiology and management.
Eur J Pediatr. 171:625–630. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lito D, Francisco T, Salva I, Tavares Md,
Oliveira R and Neto MT: TORCH serology and group B Streptococcus
screening analysis in the population of a maternity. Acta Med Port.
26:549–554. 2013.(In Portuguese). PubMed/NCBI
|
|
30
|
Vilibic-Cavlek T, Ljubin-Sternak S, Ban M,
Kolaric B, Sviben M and Mlinaric-Galinovic G: Seroprevalence of
TORCH infections in women of childbearing age in Croatia. J Matern
Fetal Neonatal Med. 24:280–283. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sen MR, Shukla BN and Tuhina B: Prevalence
of serum antibodies to TORCH infection in and around Varanasi,
Northern India. J Clin Diagn Res. 6:1483–1485. 2012.PubMed/NCBI
|
|
32
|
Puccio G, Cajozzo C, Canduscio LA, Cino L,
Romano A, Schimmenti MG, Giuffrè M and Corsello G: Epidemiology of
toxoplasma and CMV serology and of GBS colonization in pregnancy
and neonatal outcome in a Sicilian population. Ital J Pediatr.
40:232014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Maida JM, Mathers K and Alley CL:
Pediatric ophthalmology in the developing world. Curr Opin
Ophthalmol. 19:403–408. 2008. View Article : Google Scholar : PubMed/NCBI
|