Introduction
Kashin-Beck disease (KBD) is an endemic
osteochondropathy, mainly located in Eastern Siberia in Russia, the
diagonal broad belt extending from the Northeast to the Southwest
of China, affecting over 0.642 million patients with 37,917 million
people at risk (1,2). Clinically, the disease manifests as
deformed, enlarged interphalangeal joints with shortened fingers,
and limited range of motion (ROM) in the joints of the extremities,
which develops in 4 stages (3).
Similar to other degenerative joint diseases, the large
weight-bearing joints are the most degenerated in adult KBD
patients, especially the knee joint. The primary aim of the
therapeutic management of KBD, referring to osteoarthritis (OA), is
pain relief, protection of ROM, and prevention of secondary
functional disability and joint damage. No medical intervention has
been shown to arrest disease progression or reverse joint damage
and few studies can be found on the validity of medical therapy
methods at present (4–6). It is therefore important to identify a
useful therapeutic regimen for KBD.
Intra-articular injections, such as those with
sodium hyaluronic acid (HA), are widely used in the treatment of
knee OA. Although HA has been shown to affect chondrocytes,
synoviocytes, and the inflammatory process, it has been
demonstrated that the primary objective of HA injections is
visco-supplementation of the joint, which aims to increase the
elastic viscous properties and restoration of the rheological
properties of the synovial fluid in the arthritic joints (7). For the treatment with HA, most studies
reported that clinical improvement begins with a delayed onset
between 2 and 5 weeks, lasting 6 months or up to 1 year (7–9).
Literature reviews revealed that few studies observed the effects
of HA on KBD, even though the benefits of HA therapy on OA patients
are well known (10–12).
Physical therapy agents (PTA) play an important role
in the treatment of OA of the knee. Deep heat such as short waves
and electrotherapeutic modalities such as interferential therapy
are used to treat acute and chronic pain associated with OA
(13–19).
Our use of HA started based on empirical evidence,
in an attempt to improve mobility and reduce pain in KBD patients,
with knee deformity. After witnessing an initial result within the
first year, we performed a formal clinical trial, which was
undertaken between August 2006 and March 2009. The aim was to study
the effects of HA therapy on the clinical signs and evolution of
the disease.
Patients and methods
Patients
The present study was performed with the approval of
the Xi'an Jiaotong University Ethics Committee and in compliance
with the Helsinki Declaration (register no. ChiCTR-TRC-12002189
http://www.chictr.org/).
The study was a clinical trial: two intervention
treatments including intra-articular HA injections in the knee and
PTA were conducted within 48 months of follow-up. We examined
patients with KBD of the knee joint according to the national
diagnosis criteria of KBD in China (3,20). All
123 patients had grade II knee KBD, radiologically confirmed
according to the analysis of X-ray films of the right hand, knee
and hip joints. The patients suffered pain in the affected knee
that continued for at least 6 months. Patients were excluded from
the study if they had received intra-articular injections in the
joint and/or attended physiotherapy sessions for the affected knee,
within the 6 months prior to the study, if they had a history of
allergy or hypersensitivity to drugs or eggs, or if they were
ascertained or suspected to be pregnant or were lactating. Patients
were also excluded if they had a known or suspected joint infection
or a specific condition (neoplasm, diabetes mellitus, paresis,
osteonecrosis, or recent trauma) or poor general health status that
would interfere with the functional assessments during the study.
Baseline characteristics (weight, height, age, gender and related
radiological assessment of the knee and radiological degree) were
recorded prior to the treatment. Laboratory assessment (according
to standard methods) made at the entry and after 6 months included
the following evaluation: routine hematological variables, and
functional tests of the kidney and liver.
Treatments
The patients were divided into the HA or PTA group
(n=62 and 61 per group, respectively). Each participant was
informed with regard to the study and provided signed consent for
treatment. In patients with bilateral disease, the more painful
knee was treated. Patients in the first group received HA. The test
drug was 20 mg sodium hyaluronate (20 mg/2 ml, 500–700,000;
Shanghai Qisheng Biological Preparation Co., Ltd, Shanghai, China),
(→3)-2-acetamido-2-deoxy-β-D-glucopyranosyl-(1→4)-β-D-glucopyranosyluronic
acid-(1→) n, C14H20NNaO11.
Injections were performed by two physicians in an anterolateral
approach (along the patellar tendon) with the knee in 90° flexion,
and an evaluator unaware of each patient's treatment group, not
present at the time or place of each weekly injection, assessed the
patients for their symptoms and side effects at baseline and at
first injection, 1 week later. A volume of 2 ml was injected
intra-articularly into each knee joint once a week for five
consecutive weeks without local anesthetics. Strict sterile
procedures were applied to prevent septic infection. The 6th
injection was carried out in the 3rd month and the 7th injection
was carried out in the 6th month.
PTA were applied to each patient of the other group,
five times a week for 3 weeks every month for 6 months with a
series of infrared (IRH-3100; Korea), short-wave diathermy pulsed
patterns and interferential therapy. Each of them was continued for
approximately 20 sec, for 1 h.
Clinical assessments were made at the start of the
study, and at 1, 3, 6, 12, 18 and 24 months.
The patients could use paracetamol (to a maximum of
2 g daily) during the study period as considered appropriate by the
physician. The use of NSAIDs was not permitted during the study
period; any pretreatment with NSAIDs had to be discontinued 15 days
before the start of the study. Patients were withdrawn from the
study if a severe reaction to the injections occurred or if there
was evidence of an active infection in the injected joint at any
time during the study period.
Efficacy parameters
The primary efficacy criterion was joint pain
measured using WOMAC A visual analog pain scale (VAS). Secondary
efficacy variables included joint stiffness (WOMAC B) and physical
function (WOMAC C), total WOMAC, Short Form 36 (SF-36) health
survey questionnaire, daily paracetamol consumption, global
efficacy judgment by the patient and the investigator using a
four-point scale (‘How well do you feel the treatment has worked
thus far?’, i.e., not effective, slightly effective, moderately
effective, very effective), presence of effusion or swelling of
soft tissue, and tenderness of the signal joint (VAS) assessed by
palpation along the joint line.
Safety parameters
Vital signs were recorded at baseline and at every
visit. Blood and urine samples were collected at screening, at week
1 and at the end of treatment (week 4) for laboratory safety
analyses. Adverse events (AEs) were recorded at each visit and
assessed by the investigator. Patients were asked to assess the
tolerability of the study treatment globally (‘How well did you
tolerate the treatment?’) at each visit after baseline using a
5-point rating scale (nil, poor, moderate, good, very good). The
investigators also provided a judgment on tolerability (‘How well
do you think the patient tolerated the treatment?’) using the same
scale. In both groups the following clinical parameters were used
to assess the response to the treatment: the ROM of both knees
(measurement with a goniometer of active extension and flexion.
However, only flexion was measured because none of the patients had
restriction of extension), time to walk a distance of 15 m
(measured with a stop-watch and reported in sec), amount of soft
tissue swelling and synovial effusion (measured by a meter on volar
patellar area and noted if patellar click sign was present by
bimanual examination).
Statistical analysis
SPSS for Windows software was used for data
management and statistical analysis. Primary analyses were
conducted by intent-to-treat using the last observation carried
forward technique for missing data, with participants analyzed
according to their initial assignment. To compare the groups with
regard to demographic measurements, the independent samples t-test
or Chi-square test were used between the group analyses. The
differences between groups were verified by independent samples
t-test. The repeated measurement variables in each group (HA or
PTA) were analyzed using analysis of variance (ANOVA) (general
linear model for repeated measures). The level of significance was
set at 0.05 for all statistical tests. All tests of hypotheses and
reported P-values were two-sided.
Results
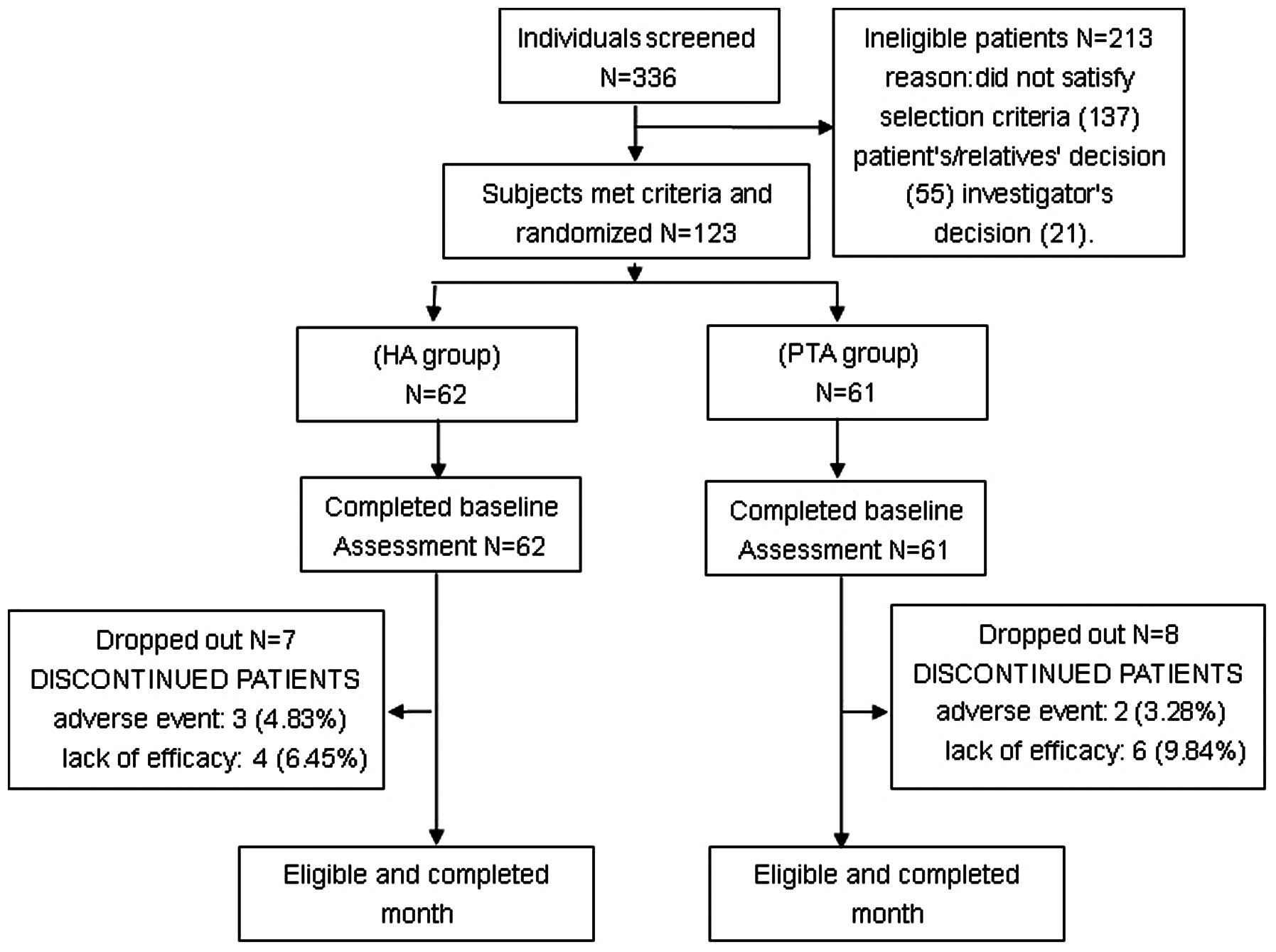
From a pool of 336 individuals, 123 met the
screening criteria (Fig. 1). Of the
123 patients, 62 patients were randomized into the HA group and the
remaining 61 patients in the PTA group. All participants were given
a baseline assessment. Fifteen patients (7 patients in the HA group
and 8 patients in the PTA group) dropped out of the study between
month 1 and month 24 of assessments due to an adverse event, lack
of effectiveness, loss to follow-up or patient decision. A total of
108 patients completed the 24-month study (Fig. 1). The remaining 108 patients (55 in
the HA group and 53 in the PTA group) were considered eligible for
an effectiveness analysis.
Baseline characteristics
Table I shows
baseline demographic data, KBD symptoms, and prior treatment for
all the patients eligible for an effectiveness analysis. The two
randomized groups were comparable at baseline, and there were no
significant differences between the groups for these parameters
(P<0.05). In addition, there were no relevant differences in
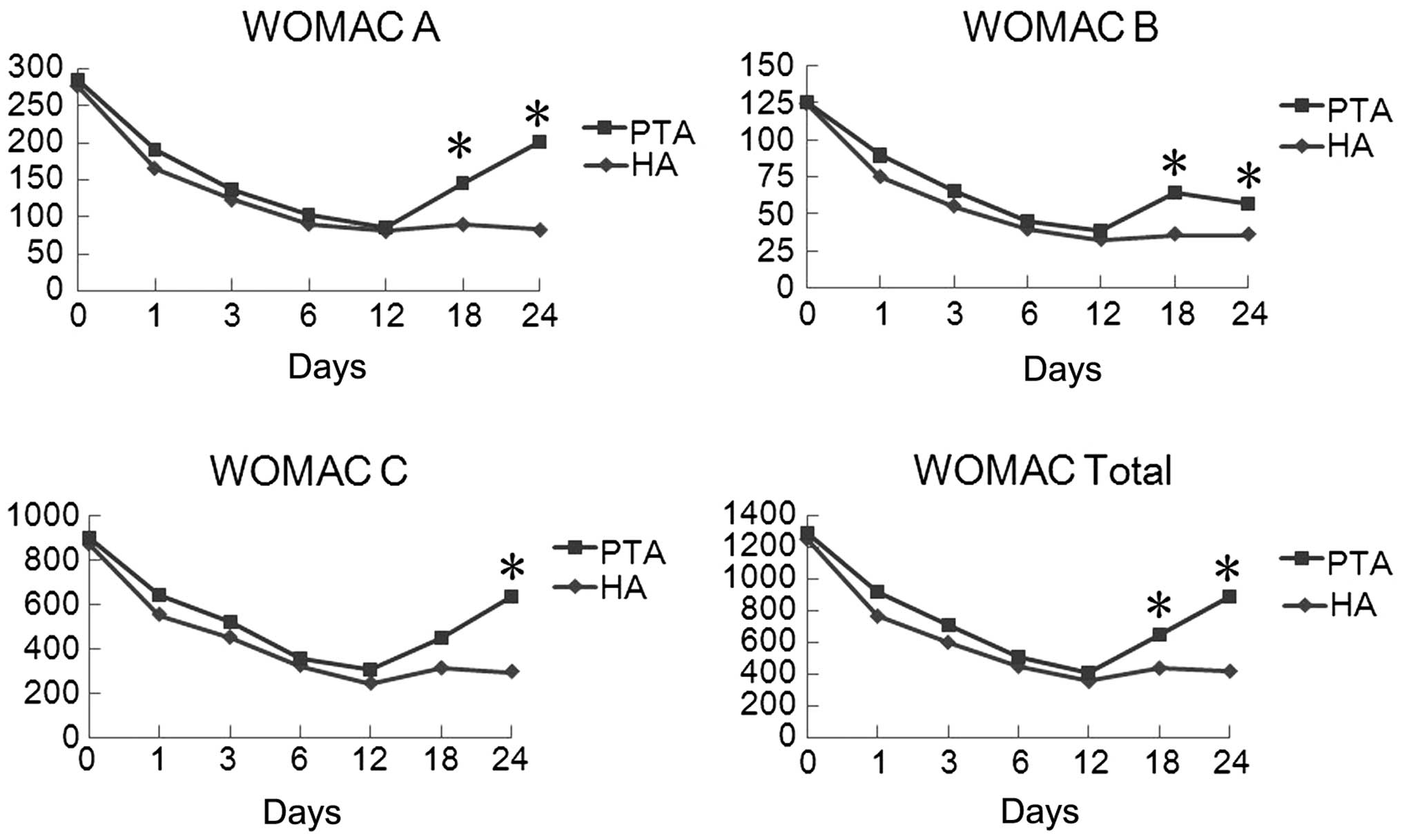
baseline values for the other efficacy parameters (Table I; Fig.
2).
 | Table I.Demographic and clinical
characteristics of patients at baseline. |
Table I.
Demographic and clinical
characteristics of patients at baseline.
| Characteristics | HA group | PTA group | P-value |
|---|
| N | 55 | 53 |
|
| Age (years) | 62.4±9.0 | 58.7±8.3 | NS |
| Female/male (%) | 40/15
(72.7/27.3) | 35/18
(64.2/34.0) | NS |
| BMI
(kg/m2) | 30.1±5.2 | 30.9±2.3 | NS |
| Stiffness (min) | 9.6±8.2 | 10.5±6.1 | NS |
| Right/left (%) | 36/19
(65.5/34.5) | 35/18
(66.0/34.0) | NS |
| Range of motion
(degree) | 118.6±12.3 | 121.3±9.0 | NS |
| Peripheral
measurement of knee (m) | 42.6±4.1 | 41.2±2.6 | NS |
Efficacy results
The mean values and the Student's t-test statistics
for the efficacy parameters are shown in Table II. The primary efficacy parameter,
pain on WOMAC A, decreased to a similar extent in the two groups
during the 12-month treatment period: from a mean value of
285.1±70.0 mm VAS at baseline to 85.7±83.8 mm at 12 months in the
PTA group and from 278.0±65.0 mm at baseline to 80.7±70.6 mm at 12
months in the HA group. Although HA appeared to have a faster onset
of efficacy at month 1, there were no statistically significant
differences between the groups during the treatment period showing
that PTA is as effective as HA for pain reduction.
| Table II.Efficacy parameters-mean absolute
values and MW statistics. |
Table II.
Efficacy parameters-mean absolute
values and MW statistics.
| WOMAC (mean ±
SD) | HA (n=55) | PTA (n=53) |
|---|
| WOMAC A |
|
|
|
Baseline |
278.0±65.0 |
285.1±70.0 |
| Month
1 |
166.2±84.3a |
190.5±93.6 |
| Month
3 |
123.2±85.9a |
136.1±94.8a |
| Month
6 |
90.3±74.2a |
102.0±92.7a |
| Month
12 |
80.7±70.6a |
85.7±83.8a |
| Month
18 |
90.1±95.2a |
145.2±128.8 |
| Month
24 |
82.6±85.3a |
201.3±150.5 |
| WOMAC B |
|
|
Baseline |
124.8±38.5 |
125.5±45.6 |
| Month
1 |
75.2±37.9a |
89.7±48.5a |
| Month
3 |
55.3±38.8a |
65.2±45.0a |
| Month
6 |
39.6±33.3a |
45.7±42.1a |
| Month
12 |
32.6±34.0a |
38.9±36.7a |
| Month
18 |
36.3±36.5a |
64.6±48.9a |
| Month
24 |
36.1±37.2a |
56.9±56.2a |
| WOMAC C |
|
|
Baseline |
875.1±265.3 |
901.8±252.5 |
| Month
1 |
556.6±313.1 |
643.9±354.1 |
| Month
3 |
453.2±312.5a |
518.4±311.3a |
| Month
6 |
326.0±266.0a |
357.5±310.2a |
| Month
12 |
245.4±260.2a |
305.0±279.1a |
| Month
18 |
313.7±317.6a |
448.5±403.5a |
| Month
24 |
297.8
±322.9a |
639.0±516.5 |
| WOMAC total |
|
|
Baseline |
1253.2±354.3 |
1293.6±343.8 |
| Month
1 |
768.0±406.6a |
928.4±481.7 |
| Month
3 |
603.7±416.7a |
712.6±482.1 |
| Month
6 |
451.9±366.4a |
512.1±451.2a |
| Month
12 |
357.7±346.1a |
415.1±424.0a |
| Month
18 |
441.2±450.4a |
658.3±586.4 |
| Month
24 |
421.8±454.0a |
896.6±652.3 |
| SF-36 (sum
score) |
|
|
Baseline |
358.0±114.2 |
355.3±121.6 |
| Month
18 |
556.6±142.3a |
507.9±136.7a |
| Month
24 |
542.9±156.6a |
514.1±146.7a |
However, following treatment interruption, pain
increased rapidly in the PTA group (from a mean value of 85.7±83.8
mm at month 12 to 145.2±128.8 mm at month 18 and 201.3±150.5 mm at
month 24) while it remained stable in the HA group (from a mean
value of 80.7±70.6 mm at month 12 to 90.1±95.2 mm at month 18 and
82.6±85.3 mm at month 24) with a statistically significant
difference in favor of HA at month 18 (P<0.05) and month 24
(P<0.05) (Table II).
Joint stiffness (WOMAC B), physical function (WOMAC
C) and total WOMAC showed the same trend as WOMAC A (Table II; Fig.
2). Tenderness on palpation decreased in the two groups with a
significant difference (P<0.05) (Table II).
The global efficacy judgments by the patients and
the investigators are presented in Table III and confirm the slow onset of
efficacy of HA with 76.4% in this group compared with 56.6% of the
patients in the PTA group judging that their treatment was
‘moderately effective’ to ‘very effective’ at month 1. The
judgments were comparable in the two treatment groups at the end of
the treatment. At month 12, a significantly (P<0.001) greater
proportion of HA-treated patients (78.1%) assessed treatment as
‘moderately effective’ to ‘very effective’, compared to 41.5% of
those treated with PTA while at month 24, these figures were 65.4%
in the HA group and 30.2% in the PTA group (P<0.001).
| Table III.Clinical assessments of the drug
treatments (global efficacy judgments by the patients and the
investigator). |
Table III.
Clinical assessments of the drug
treatments (global efficacy judgments by the patients and the
investigator).
|
| HA (n=55) | PTA (n=53) | P-value |
|---|
|
|
|
|
|
|---|
| Effective (%) | a | b | a | b | a | b |
|---|
| Month 1 |
|
|
|
| 0.042 | 0.144 |
|
Not | 9.1 | 11.0 | 20.8 | 17.0 |
|
|
|
Slightly | 14.5 | 12.7 | 22.6 | 24.5 |
|
|
|
Moderately | 36.4 | 40.0 | 28.3 | 28.3 |
|
|
|
Very | 40.0 | 36.4 | 28.3 | 30.2 |
|
|
| Month 6 |
|
|
|
| 0.003 | 0.013 |
|
Not | 7.3 | 9.1 | 13.2 | 11.3 |
|
|
|
Slightly | 10.9 | 12.7 | 35.8 | 35.8 |
|
|
|
Moderately | 5.5 | 40.0 | 30.2 | 32.1 |
|
|
|
Very | 36.4 | 36.4 | 20.8 | 20.8 |
|
|
| Month 12 |
|
|
|
| 0.001 | 0.002 |
|
Not | 12.7 | 9.1 | 28.3 | 4.5 |
|
|
|
Slightly | 9.1 | 12.7 | 30.2 | 30.2 |
|
|
|
Moderately | 43.6 | 38.2 | 24.5 | 22.6 |
|
|
|
Very | 34.5 | 8.2 | 17.0 | 22.6 |
|
|
| Month 24 |
|
|
|
| 0.001 | 0.001 |
|
Not | 20.0 | 21.8 | 39.6 | 43.4 |
|
|
|
Slightly | 14.5 | 12.7 | 30.2 | 26.4 |
|
|
|
Moderately | 23.6 | 21.8 | 13.2 | 13.2 |
|
|
|
Very | 41.8 | 43.6 | 17.0 | 17.0 |
|
|
Safety
Three patients of the HA group withdrew from the
study due to adverse reactions (malaise, tachycardia and
hypotension). The events occurred after the first injection. Two
cases of adverse event were observed in the PTA patients. No
clinically significant changes occurred in the laboratory
parameters or other vital signs in either group.
Discussion
HA is a non-sulfated, non-epimerized, linear
glycosaminoglycan (GAG) existing in vivo as a polyanion of
HA and composed of repeating disaccharide units of D-glucuronic
acid and N-acetyl-D-glucosamine
(−>4GlcAbeta1->3GlcNAcbeta1->) (7,8). It is a
constituent of the extracellular matrix (ECM) of the skin, joints,
eye, and many other tissues and organs. In the joint, HA is an
important component of the extracellular matrix of the cartilage
(21). It is present in the
superficial layers of the synovial membrane and is found at high
concentration in the synovial fluid (22–28). HA
plays a key role in preserving the structural and functional
integrity of the cartilage matrix and in regulating a variety of
cellular activities through specific cellular receptors and
molecular interactions in addition to maintaining the viscoelastic
properties of synovial fluid. In vitro and in vivo
studies have shown that HA can induce proteoglycan synthesis and
aggregation, stimulate synoviocytes to produce more HA, modulate
the inflammatory response, reduce chemotaxis and leucocyte
migration and exert scavenger activity on free oxygen radicals
(5). These activities are mediated
by the binding of HA with intercellular adhesion molecule-1
(ICAM-1), CD44 integrin and the receptor for HA-mediated motility
(RHAMM), all of which are expressed on the surface of various cell
types, including inflammatory cells, synoviocytes and chondrocytes.
HA injected in the joint has a half-life of approximately 20 h when
joints are normal and approximately 12 h when joints are inflamed
(29). The above evidence shows that
the clinical effects of HA are due to its pharmacological action on
the cellular and tissue components of the joint. Therefore, it can
be excluded that the sustained beneficial effects of HA on symptoms
and clinical signs of KBD, such as OA, can be accounted only for a
temporary restoration of the synovial fluid viscoelasticity.
The effect of HA on KBD may be related to inhibiting
the levels of cytokines, specific cellular receptors, and molecular
interactions. It was reported that sodium HA administration has a
dose-dependent effect in vitro to promote the proliferation
and inhibition of apoptosis of chondrocytes from patients with KBD
(30,31). Phenotypic expression of types I, II,
III, and X collagen and MMP-13 in chondrocytes cultured in
vitro were significantly different between the KBD and control
cultures, showing degenerative and hypertrophic changes in
chondrocytes of KBD articular cartilage (30). Increases of the levels of tumor
necrosis factor (TNF)-α, vascular endothelial growth factor (VEGF)
and interleukin (IL)-1β may play a role in the pathogenesis of KBD.
Terminal chondrocytes differentiation, PTHrP, transforming growth
factor (TGF)-β1, and VEGF expression was altered showing
degenerative changes in KBD cartilage (32–36).
Previous findings showed that HA can promote the proliferation of
chondrocytes and has effects on the differentiation of these cells
(24–26,37).
In vitro experiments showed that HA can enhance the
synthesis of extracellular matrix proteins, including chondroitin
and keratin sulfate, while suppressing cartilage damage by
fibronectin fragments in vitro and in vivo (24,37–40).
The present findings have shown that while an
improvement was observed in the functions of all patients, pain
intensity decreased more rapidly and to lower levels with the use
of HA. In the present study, pain relief by the WOMAC pain subscale
was observed in the first month in the two groups. Similarly, this
pattern of decrease in pain was also observed by VAS.
Whether HA was used or not, the improvement in
function was persistent during the first year. The use of HA
injections should be considered for rapid and prolonged effect in
the improvement of knee KBD. Our findings support that HA
injections could lead to better results in pain reduction.
Our study has several limitations which must be
considered. The number of patients studied was small due to medical
costs, increasing the power of the study to show significant
effects. Second, since there was no other medicine-treated group,
such as a saline solution group, perhaps the HA treatment may not
be more effective than intra-articular or other drugs. However, the
main objective of this study was to assess the effects of HA on the
management of knee KBD, not to compare the effects of different
drug therapies. Furthermore, HA has been demonstrated to be
effective, and has been found to be superior to placebo injections,
and comparative studies have shown the differences between timing
of onset of effects, as reported above. In conclusion, this study
demonstrates that HA provides rapid pain relief, has beneficial
effects during the first year following treatment, and is well
tolerated in the management of knee KBD. For the treatment of
patients with knee KBD, our findings support that HA should be the
preferred therapeutic option.
In conclusion, the results of this study support the
observation that PTA is a useful, safe and well-tolerated treatment
for patients with knee OA, and who are receiving hyaluronan
therapy. Although all patients showed improvement for pain and
function, HA therapy was superior to PTA alone for pain relief and
had a longer lasting effect.
Acknowledgements
This study was supported by the Ministry of Science
and Technology (no. 2006DFA33610), the Natural Scientific Fund of
China (no. 30630058,81001225), the International Co-operative Fund
in Shaanxi, China and Finland (no. 2005KW-13), China and University
of Buffalo, USA (no. 08143004), and the Fundamental Research Funds
for the Central Universities (no. 08140003).
References
|
1
|
Chinese Health Statistical Digest.
http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohwsbwstjxxzx/s9092/201206/55044.htm.2012
|
|
2
|
Yamamuro T: Kashin-Beck disease: a
historical overview. Int Orthop. 25:134–137. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Xiong G: Diagnostic, clinical and
radiological characteristics of Kashin-Beck disease in Shaanxi
Province, PR China. Int Orthop. 25:147–150. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yue J, Yang M, Yi S, Dong B, Li W, Yang Z,
Lu J, Zhang R and Yong J: Chondroitin sulfate and/or glucosamine
hydrochloride for Kashin-Beck disease: a cluster-randomized,
placebo-controlled study. Osteoarthritis Cartilage. 20:622–629.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tang X, Pei FX, Zhou ZK, Liu G, Shen B,
Kang PD, Li J, Zhao XD, Li Q and Li Y: A randomized, single-blind
comparison of the efficacy and tolerability of hyaluronate acid and
meloxicam in adult patients with Kashin-Beck disease of the knee.
Clin Rheumatol. 31:1079–1086. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mathieu F, Suetens C, Begaux F, De
Maertelaer V and Hinsenkamp M: Effects of physical therapy on
patients with Kashin-Beck disease in Tibet. Int Orthop. 25:191–193.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shimizu M, Higuchi H, Takagishi K,
Shinozaki T and Kobayashi T: Clinical and biochemical
characteristics after intra-articular injection for the treatment
of osteoarthritis of the knee: prospective randomized study of
sodium hyaluronate and corticosteroid. J Orthop Sci. 15:51–56.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Briem K, Axe MJ and Snyder-Mackler L:
Functional and perceived response to intra-articular hyaluronan
injection in patients with knee osteoarthritis: persistence of
treatment effects over 5 months. Knee Surg Sports Traumatol
Arthrosc. 17:763–769. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bannuru RR, Natov NS, Obadan IE, Price LL,
Schmid CH and McAlindon TE: Therapeutic trajectory of hyaluronic
acid versus corticosteroids in the treatment of knee
osteoarthritis: a systematic review and meta-analysis. Arthritis
Rheum. 61:1704–1711. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liang KY: Research progress of
intraarticular injection of hyaluronic acid (HA) for osteoarthritis
in recent three years. Zhongguo Gu Shang. 23:962–964. 2010.(In
Chinese). PubMed/NCBI
|
|
11
|
Yasuda T: Progress of research in
osteoarthritis. Pharmacological effects of hyaluronic acid. Clin
Calcium. 19:1644–1652. 2009.(In Japanese). PubMed/NCBI
|
|
12
|
Akasaki Y, Matsuda S and Iwamoto Y:
Progress of research in osteoarthritis. The anti-inflammatory
effects of intra-articular injected statin on experimental
osteoarthritis. Clin Calcium. 19:1653–1662. 2009.(In Japanese).
PubMed/NCBI
|
|
13
|
Lin H and He C: Progress of foreign
clinical research of exercise therapy of knee osteoarthritis.
Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 22:1389–1392. 2008.(In
Chinese). PubMed/NCBI
|
|
14
|
Brakke R, Singh J and Sullivan W: Physical
therapy in persons with osteoarthritis. PM R. 4(Suppl): S53–S58.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gonçalves RS, Cabri J and Pinheiro JP:
Evaluation of patient characteristics as predictors of health
status in knee osteoarthritis patients referred for physical
therapy. Acta Reumatol Port. 36:137–144. 2011.PubMed/NCBI
|
|
16
|
Pisters MF, Veenhof C, Schellevis FG, De
Bakker DH and Dekker J: Long-term effectiveness of exercise therapy
in patients with osteoarthritis of the hip or knee: a randomized
controlled trial comparing two different physical therapy
interventions. Osteoarthritis Cartilage. 18:1019–1026. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Benito Peinado PJ, Cupeiro Coto R and
Calderón Montero FJ: Physical exercise as non pharmacologic therapy
in knee osteoarthritis. Reumatol Clin. 6:153–160. 2010.(In
Spanish). PubMed/NCBI
|
|
18
|
Kladny B: Physical therapy of
osteoarthritis. Z Rheumatol. 64:448–455. 2005.(In German).
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mayer ME: Physical therapy and exercise in
osteoarthritis of the knee. Ann Intern Med. 132:9232000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Farooq U, Xiong G, Irshad R and Yaqoob S:
Pattern of joints involvement in Kashin-Beck disease: a local
osteochondropathy in China. J Ayub Med Coll Abbottabad. 22:97–100.
2010.PubMed/NCBI
|
|
21
|
Olczyk P, Komosinska-Vassev K,
Winsz-Szczotka K, Kuznik-Trocha K and Olczyk K: Hyaluronan:
structure, metabolism, functions, and role in wound healing.
Postepy Hig Med Dosw (Online). 62:651–659. 2008.(In Polish).
PubMed/NCBI
|
|
22
|
Schiavinato A, Finesso M, Cortivo R and
Abatangelo G: Comparison of the effects of intra-articular
injections of Hyaluronan and its chemically cross-linked derivative
(Hylan G-F20) in normal rabbit knee joints. Clin Exp Rheumatol.
20:445–454. 2002.PubMed/NCBI
|
|
23
|
Kitano T, Ateshian GA, Mow VC, Kadoya Y
and Yamano Y: Constituents and pH changes in protein rich
hyaluronan solution affect the biotribological properties of
artificial articular joints. J Biomech. 34:1031–1037. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nehrer S, Chiari C, Domayer S, Barkay H
and Yayon A: Results of chondrocyte implantation with a
fibrin-hyaluronan matrix: a preliminary study. Clin Orthop Relat
Res. 466:1849–1855. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Echigo R, Mochizuki M, Nishimura R and
Sasaki N: Suppressive effect of hyaluronan on chondrocyte apoptosis
in experimentally induced acute osteoarthritis in dogs. J Vet Med
Sci. 68:899–902. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Knudson CB, Nofal GA, Pamintuan L and
Aguiar DJ: The chondrocyte pericellular matrix: a model for
hyaluronan-mediated cell-matrix interactions. Biochem Soc Trans.
27:142–147. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cortivo R, Brun P, Cardarelli L, O'Regan
M, Radice M and Abatangelo G: Antioxidant effects of hyaluronan and
its alpha-methyl-prednisolone derivative in chondrocyte and
cartilage cultures. Semin Arthritis Rheum. 26:492–501. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Knudson W and Knudson CB: Assembly of a
chondrocyte-like pericellular matrix on non-chondrogenic cells.
Role of the cell surface hyaluronan receptors in the assembly of a
pericellular matrix. J Cell Sci. 99:227–35. 1991.PubMed/NCBI
|
|
29
|
Magdalou J, Netter P, Fournel-Gigleux S
and Ouzzine M: Agrecan and articular cartilage: assessment of
glycosyltransferases for the restoration of cartilage matrix in
osteoarthritis. J Soc Biol. 202:281–288. 2008.(In French).
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gao Z, Guo X, Duan C, Ma W, Xu P, Liu R,
Gu Q and Chen J: In vitro effects of sodium hyaluronate on the
proliferation and the apoptosis in chondrocytes from patients with
Kashin-Beck disease and osteoarthritis. J Nanjing Med Univ.
23:104–110. 2009. View Article : Google Scholar
|
|
31
|
Tanaka M, Masuko-Hongo K, Kato T, Nishioka
K and Nakamura H: Suppressive effects of hyaluronan on MMP-1 and
RANTES production from chondrocytes. Rheumatol Int. 26:185–190.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tang X, Zhou Z, Shen B, Yang J, Kang P, Li
J, Crook N, Li Q, Min L and Pei F: Serum levels of TNF-α, IL-1β,
COMP, and CTX-II in patients with Kashin-Beck disease in Sichuan,
China. Rheumatol Int. 32:3503–3509. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yan D, Kang P, Shen B, Yang J, Zhou Z,
Duan L and Pei F: Serum levels of IL-1β, IL-6 and TNF-α in rats fed
with Kashin-Beck disease-affected diet. Int J Rheum Dis.
13:406–411. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Guo X, Zuo H, Cao CX, Zhang Y, Geng D,
Zhang ZT, Zhang YG, von der Mark K and von der Mark H: Abnormal
expression of Col X, PTHrP, TGF-beta, bFGF, and VEGF in cartilage
with Kashin-Beck disease. J Bone Miner Metab. 24:319–328. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Wang SJ, Guo X, Ren FL, Zhang YG, Zhang
ZT, Zhang FJ and Geng D: Comparison of apoptosis of articular
chondrocytes in the pathogenesis of Kashin-beck disease and primary
osteoarthritis. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 28:267–270.
2006.(In Chinese). PubMed/NCBI
|
|
36
|
Wang SJ, Guo X, Zuo H, Zhang YG, Xu P,
Ping ZG, Zhang Z and Geng D: Chondrocyte apoptosis and expression
of Bcl-2, Bax, Fas, and iNOS in articular cartilage in patients
with Kashin-Beck disease. J Rheumatol. 33:615–619. 2006.PubMed/NCBI
|
|
37
|
Grad S, Lee CR, Gorna K, Gogolewski S,
Wimmer MA and Alini M: Surface motion upregulates superficial zone
protein and hyaluronan production in chondrocyte-seeded
three-dimensional scaffolds. Tissue Eng. 11:249–256. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lin LC, Chang SJ, Lin CY, Lin YT, Chuang
CW, Yao CH and Kuo SM: Repair of chondral defects with allogenous
chondrocyte-seeded hyaluronan/collagen II microspheres in a rabbit
model. Artif Organs. 36:E102–109. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Eshed I, Trattnig S, Sharon M, Arbel R,
Nierenberg G, Konen E and Yayon A: Assessment of cartilage repair
after chondrocyte transplantation with a fibrin-hyaluronan matrix -
correlation of morphological MRI, biochemical T2 mapping and
clinical outcome. Eur J Radiol. 81:1216–1223. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Barbucci R, Torricelli P, Fini M, Pasqui
D, Favia P, Sardella E, d'Agostino R and Giardino R: Proliferative
and re-defferentiative effects of photo-immobilized micro-patterned
hyaluronan surfaces on chondrocyte cells. Biomaterials.
26:7596–7605. 2005. View Article : Google Scholar : PubMed/NCBI
|