Introduction
Osteonecrosis of the femoral head (ONFH) is a
pathological process primarily caused by interrupted local blood
circulation, which can cause apoptosis of osteocytes and osseous
tissue necrosis (1,2). The lack of effective therapy for ONFH
is a difficulty that needs to be overcome in clinical practice.
Several methods have been used to treat early-stage ONFH, such as
drug therapy, core decompression, vascularized bone grafting and
rotational osteotomy. However, the clinical results of these
methods are not satisfactory (3,4).
Previous studies have described the use of
mesenchymal stem cells (MSCs) to promote local bone repair and
healing (5,6). MSCs are pluripotent and can
differentiate into several lineages of cells, which have shown
potency in the treatment of numerous ischemic diseases, such as
myocardial infarction (7,8), nerve injury (9) and bone defect (10). Prior studies have found that the
implantation of MSCs into the necrotic area of the femoral head was
able to improve local bone regeneration (11,12).
MSCs are able to differentiate into osteoblasts to promote local
bone healing directly (13,14). Furthermore, MSCs are able to secrete
growth factors such as vascular endothelial growth factor (VEGF),
angiopoietin 1, stromal cell-derived factor 1 and basic fibroblast
growth factor, which have angiogenic potency and can promote local
revascularization, thereby improving bone healing indirectly
(15,16).
Hypoxia inducible factor-1α (HIF-1α) is a key
mediator of the adaptive cell response to hypoxia, which controls
the expression of numerous genes and modulates cell proliferation,
differentiation and pluripotency (17). Previous experiments have suggested
that HIF-1α could enhance the osteogenic differentiation of MSCs
and the expression of angiogenic factors, thus promoting their bone
healing capacity (18). In a prior
study, we implanted HIF-1α transgenic MSCs into the necrotic area
of the femoral head, and found that this treatment resulted in
improved osteogenic and angiogenic capacity in vitro and
in vivo, leading to better results for early-stage ONFH
(19). However, the risks of
lentivirus vectors, such as tumorigenesis (20), should be seriously considered before
clinical application.
Dimethyloxalylglycine (DMOG) is a cell permeable
prolyl-4-hydroxylase inhibitor, which is able to stabilize
expression of HIF-1α in cells at normal oxygen tension (21). Therefore, DMOG is hypothesized to be
an alternative strategy for enhancing HIF-1α expression in MSCs. In
a previous study, we demonstrated that DMOG could increase HIF-1α
expression in MSCs, accordingly enhancing their bone healing
capacity (22). In the present
study, we investigated whether DMOG was able to enhance the bone
repair capacity of adipose-derived stem cells (ASCs) in treating
early-stage ONFH.
Materials and methods
Animals
Healthy New Zealand rabbits weighing 2.5–3 kg and
aged 2–3 months were provided by the Experimental Animal Centre of
Shanghai Jiao Tong University affiliated Sixth People's Hospital
(Shanghai, China). Animals were maintained in single cages at a
controlled temperature (15–25°C)under a 12-h light/dark cycle and
fed with a standard diet. Animals received humane care in
compliance with the Guide of the US Department of Health for the
care and use of laboratory animals (23). The experiment protocol was approved
by the Animal Ethics Committee of Shanghai Jiao Tong
University.
Isolation and culture of ASCs
Primary ASCs were harvested from the adipose tissue
of New Zealand rabbits. Briefly, the animals were anesthetized with
pentobarbital sodium (3 mg/100 g; Sigma-Aldrich; Merck KGaA,
Darmstadt, Germany). Adipose tissues were harvested and digested
with 0.1% collagenase I (Sigma-Aldrich) for 1 h. The complex was
filtered with a 100-µm nylon mesh (Shanghai Bolting Cloth
Manufacturing Co., Ltd., Shanghai, China) and centrifuged at room
temperature for 30 min at 363 × g The cells were then resuspended
with Dulbecco's modified Eagle's medium (Gibco; Thermo Fisher
Scientific, Inc., Grand Island, NY, USA) supplemented with 10%
fetal bovine serum (Invitrogen; Thermo Fisher Scientific, Inc.,
Carlsbad, CA, USA), and were plated on culture flask (Corning Life
Sciences, Tewksbury, MA, USA). The cells were cultured at 37°C in a
humidified 5% CO2 incubator. The culture medium was
replaced every 3 days, and non-adherent cells were removed. The
cells were passaged approximately at a 1:3 split at subconfluence.
The cells of four to six passages were used for the following
experiments.
Western blot analysis
To evaluate the influence of DMOG (Sigma-Aldrich) on
the expression of HIF-1α protein in ASCs, the cells were seeded on
six-well plates at 3×105 cells/well and regular medium
(Dulbecco's modified Eagle's medium supplemented with 10% fetal
bovine serum) was added with different concentrations of DMOG (0,
200, 500 and 1,000 µM). After 1, 3 and 7 days, total protein was
harvested from the cultured cells according to standard protocols
(24). Briefly, cells were washed
three times with (PBS; Sinopharm Chemical Reagent Co., Ltd.,
Shanghai, China), and then solubilized in lysis buffer (Thermo
Fisher Scientific, Inc., Waltham, MA, USA) at 4°C for 10 min.
Lysates were centrifuged at 14,000 × g for 15 min. The supernatants
were collected and stored at −80°C. The protein concentration was
measured using a bicinchoninic protein assay kit (Thermo Fisher
Scientific, Inc.). Proteins (10 µg) from each sample were then
separated using 12% SDS-PAGE (Bio-Rad Laboratories, Inc., Hercules,
CA, USA) and transferred to nitrocellulose membranes. They were
then blocked in 5% non-fat milk at room temperature for 1 h.
Primary antibodies against HIF-1α (1:800; ab1; Abcam, Cambridge,
MA, USA) were added to incubate with the membranes at 4°C
overnight. Then, infrared-conjugated secondary antibodies
(1:10,000; ab97040; Abcam) were added to incubate with the
membranes for 1 h at room temperature. The resulting membranes were
scanned in an Odyssey Scanner (Li-COR Biosciences, Lincoln, NE,
USA), and quantified using Odyssey software version 3.0. The
protein levels were normalized against those of β-actin (1:500;
ab6276; Abcam).
Preparation of transplanted
composite
A self-assembling peptide gel (BeaverNano™ hydrogel;
Cyagen Biosciences, Inc., Guangzhou, China) was used as the
scaffold for loading ASCs. The transplanted composite was prepared
by mixing cells with the hydrogels according to the manufacturer's
protocol. In brief, 1×107 ASCs were suspended in 1 ml
10% sucrose solution (Sinopharm Chemical Reagent Co., Ltd.), and
the cell suspension was mixed with the hydrogels in an equal
volume. Then, PBS was slowly added to the mixed hydrogel composites
in an equal volume and incubated for 30 min at room temperature to
allow cross-linking. For the DMOG-treated ASCs, cells were cultured
in regular medium with 1,000 µM DMOG for 24 h prior to being mixed
with the hydrogel. To ensure ASCs were continuously exposed to DMOG
after implantation into the femoral head, 1,000 µM DMOG was added
to PBS during the composite mixing procedure.
Animal ONFH model and treatment
protocol
A total of 50 New Zealand rabbits (age, 2–3 months)
were used to established ONFH models according to previously
reported protocols (25). In brief,
one injection of lipopolysaccharide (LPS; 10 µg/kg; Sigma-Aldrich)
was administered intravenously at day 1, then three injections of
methylprednisolone (MPS; 20 mg/kg; Pfizer, Inc., New York, NY, USA)
were administered intramuscularly at days 2, 3 and 4. Six rabbits
died of the inductive protocol after the injection. ONFH was
confirmed using magnetic resonance imaging (MRI; GE Healthcare,
Chicago, IL, USA) at 6 weeks after the last injection of MPS. The
stage of ONFH was evaluated respectively by two experienced
radiologists in a blinded fashion. Then the rabbits with
early-stage ONFH were randomly divided into four groups: i) Group I
(n=11) did not receive any therapy and served as controls; ii)
Group II (n=11) only received core decompression of the femoral
head; iii) Group III (n=11) received core decompression and normal
ASC transplantation; and iv) Group IV (n=11) received core
decompression and DMOG-treated ASC transplantation.
Surgical procedure and perfusion
The surgical procedure was performed as previously
reported (26). In brief, the
animals were anesthetized with intravenous pentobarbital, and a
lateral approach was made to expose the greater trochanter under
aseptic conditions. A drill with an diameter of 1 mm was inserted
at the flare of the greater trochanter and into the necrotic area
of the femoral head, assisted by a C-arm X-ray machine. The
necrotic tissue was then removed completely, and the cell-hydrogel
composites were transplanted into the necrotic area through the
bone tunnel made by drill for Groups III and IV. The bone tunnel
was sealed with an absorbable collagen sponge plug, and the wound
was closed in layers. Following the operation, animals received
gentamicin (80 MU/day; Shanghai No.1 Biochemical &
Pharmaceutical Co., Ltd., Shanghai, China) intramuscularly as
prophylaxis for 3 days, and all animals were free to move.
Four weeks after the surgery, animals were
anesthetized with intravenous pentobarbital. The abdominal cavity
of the rabbits was opened. A syringe needle was inserted in the
abdominal aorta distal to the heart, and the abdominal aorta
proximal to the heart was ligated. Then the abdominal vein was cut
open, and heparinized normal saline (Shanghai No.1 Biochemical
& Pharmaceutical Co., Ltd.) was injected in the vasculature
through the needle at a flow speed of ~20 mm/min. When the outflow
was limpid, a silicone injection compound (MICROFIL MV-122; Flow
Tech, Inc., Carver, MA, USA) was pumped into the vasculature of the
femoral head. The animals were then stored at 4°C to ensure
polymerization of the contrast agent. After 1 h, the proximal parts
of the femurs were harvested and fixed in 4% paraformaldehyde.
Micro-computed tomography (CT)
scanning
To evaluate bone regeneration in the necrotic area
of the femoral head, the samples were scanned with micro-CT. The
scan was performed using a micro-CT scanner (SkyScan 1076; Bruker
micro-CT, Kontich, Belgium) at a resolution of 25 µm and with the
following settings: Anode current, 450 µA; X-ray voltage, 80 KVp;
and exposure time, 400 msec. Bone tissue was defined at the
threshold of 800 Hounsfield units (HU). The necrotic area of the
femoral head was selected as the region of interest (ROI) with the
aid of preoperative MRI. The parameters of bone volume/total volume
(BV/TV) and bone mineral density (BMD) of ROI were calculated,
which indicated the bone regeneration of the necrotic area.
These samples were then decalcified with 10%
ethylenediaminetetraacetic acid (Sinopharm Chemical Reagent Co.,
Ltd., Shanghai, China) at 37°C for 3 weeks. Following
decalcification, the samples underwent micro-CT examination again
at a resolution of 18 µm per voxel to evaluate the vascularization
of the necrotic area. For segmentation of vessels from background,
noise was removed with a low pass Gaussian filter and vessels were
defined at the threshold of 85 HU. To reconstruct the
three-dimensional architecture of blood vessels in the necrotic
area, the vessels were included at each two-dimensional section by
built-in ‘Contouring Program’ for automatic reconstruction of
three-dimensional images. The axial slices through the samples were
visualized, and the volume of the vessels in the necrotic area was
calculated.
Histology and
immunohistochemistry
After micro-CT scanning, samples were dehydrated and
made transparent using dimethylbenzene (Sinopharm Chemical Reagent
Co., Ltd.). They were then embedded in wax and sectioned into 6 µm
coronal planes. Sections were stained with hematoxylin and eosin
(H&E) and observed under a light microscope (Leica Microsystems
GmbH, Wetzlar, Germany). Image-Pro Plus 6.0 software (Media
Cybernetics, Inc., Rockville, MD, USA) was used to evaluate new
bone formation at ×100 magnification in six randomly selected
fields per section. Bone density was defined as the ratio of new
bone area to total area. The border of the new bone and osteoid
tissue was difficult to define, so osteoid tissue was not included
in new bone calculations.
Immunohistochemistry was performed using antibodies
specific for CD31 (1:200; ab24590; Abcam) and HIF-1α (1:100;
ab8366; Abcam). In brief, these sections were rehydrated and
incubated with primary antibodies at 4°C overnight, then incubated
with biotinylated secondary IgGs (1:500; BA1001; Wuhan Boster
Biological Technology, Ltd., Wuhan, China). Sections were treated
with ABC complex and developed with 3,3′-diaminobenzidine (both
Wuhan Boster Biological Technology, Ltd.), then stained with
hematoxylin. All sections were consistently maintained in liquid,
and sections incubated without primary antibodies were used as a
control.
Statistical analysis
Data are expressed as the mean ± standard deviation.
One-way analysis of variance with an Student-Newman-Keuls post
hoc analysis was applied to determine statistical significance.
P<0.05 was considered to indicate a statistically significant
difference. Statistical analysis was performed using SPSS software,
version 12.0 (SPSS, Inc., Chicago, IL, USA).
Results
HIF-1α overexpression in rabbit
ASCs
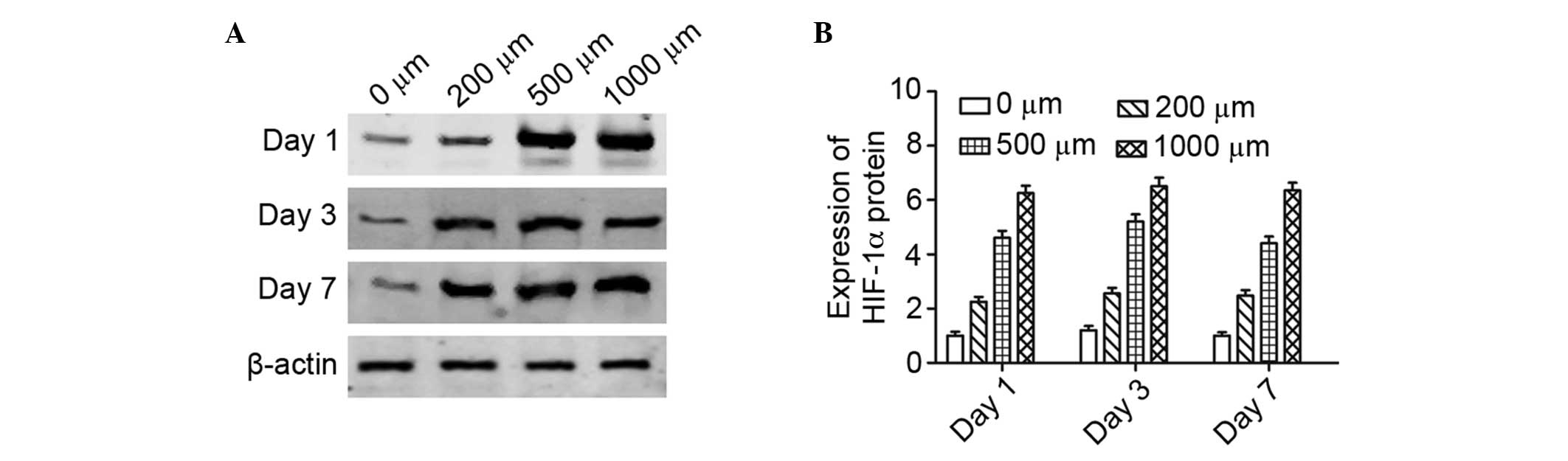
Western blot analysis was performed to detect the
protein expression of HIF-1α in rabbit ASCs treated with different
concentrations of DMOG. The data showed the expression of HIF-1α
protein was increased in response to DMOG treatment in a
dose-dependent manner (Fig. 1).
After treatment for 1 day, the HIF-1α expression in cells
respectively increased by ~2-, 4- and 5-fold for 200, 500 and 1,000
µM DMOG, respectively, compared with the untreated ASCs. After
treatment for 7 days, the levels of HIF-1α protein in ASCs had no
significant difference compared with ASCs treated with DMOG for 1
days, which indicated DMOG could enhance HIF-1α expression at least
for 7 days.
Assessment of bone regeneration in the
necrotic area
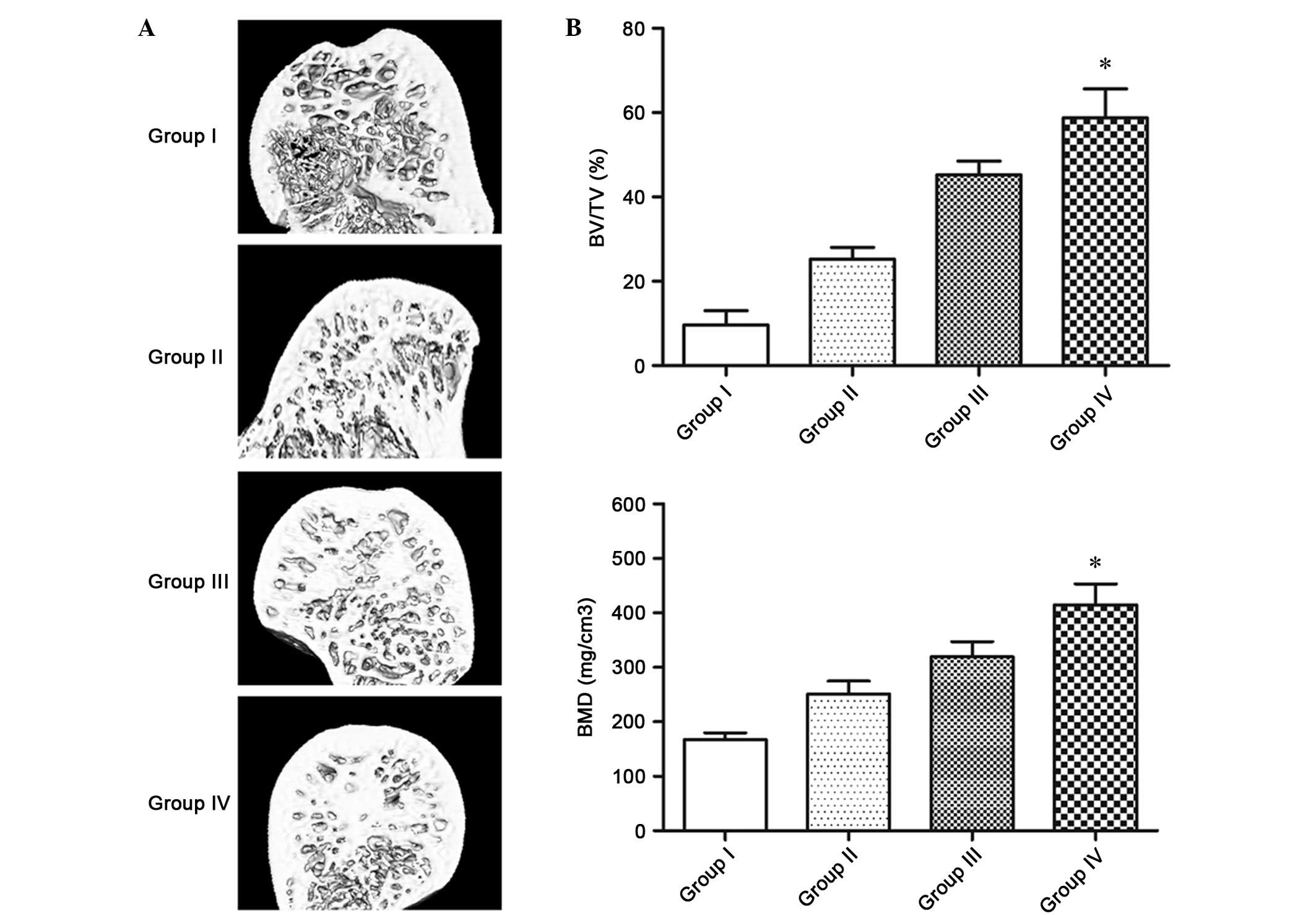
Bone regeneration in the necrotic area of each group
was initially analyzed using micro-CT scanning. Bone
microarchitecture of each group was reconstructed in three
dimensions for presentation (Fig.
2A). The samples of Group I, which received no treatment,
showed few destroyed trabeculae in the necrotic area of the femoral
head. In Group II, which received core decompression, the
trabeculae in the necrotic area was thin and sparse. In Group III,
which received core decompression and transplantation of normal
ASCs, the trabeculae in the necrotic area was more intact. In Group
IV, which received core decompression and transplantation of DMOG
treated ASCs, the trabeculae in the necrotic area appeared intact
and well distributed. Quantitative analysis indicated nearly no new
bone formation in the necrotic area of Group I (Fig. 2B). By contrast, ~25.2±2.8% of the
necrotic area was regenerated in Group II, 45.5±3.4% in Group III
and 58.8±7.4% in Group IV. The BMD of the new bone in the necrotic
area of Group IV was also significantly higher than that of other
three groups (P<0.05).
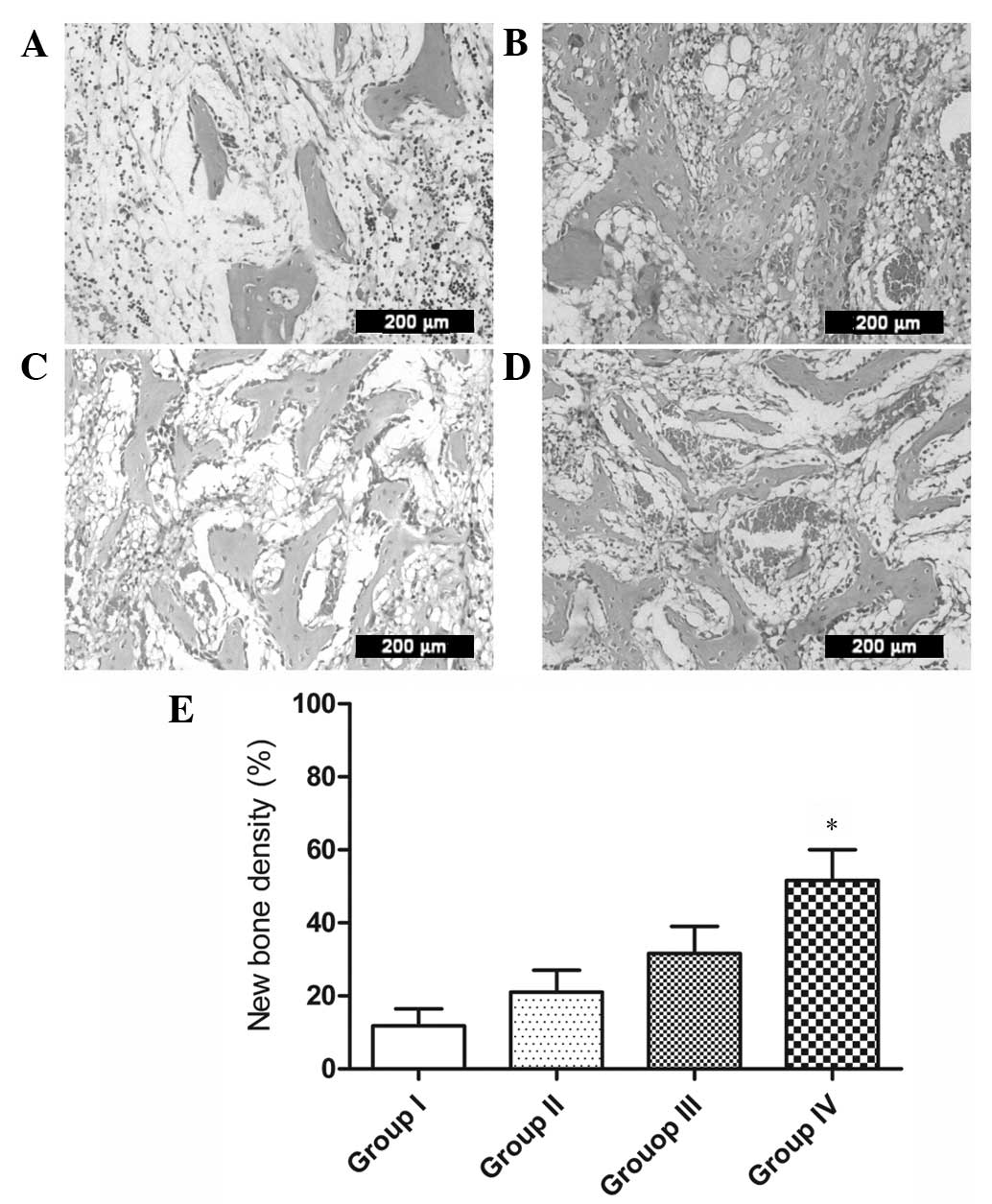
Bone regeneration in the necrotic area of each group
was also evaluated using H&E staining. In Group I, there were
numerous fat cells and rare trabecular tissue in the necrotic area,
and numerous empty lacunae distributed along the trabeculae
(Fig. 3A). In Group II, there was
less granulation tissue and fewer fat cells in the necrotic area,
and some empty lacunae were observed (Fig. 3B). In Group III, there was some
disordered trabecular tissue in the necrotic area, which was
obviously more than in Group II (Fig.
3C). In Group IV, there was substantial trabecular tissue, and
large osteocytes were distributed along the trabeculae (Fig. 3D). Histomorphometric analysis
confirmed that new bone in Group IV was more than that of other
three groups, which was consistent with the micro-CT data
(P<0.05; Fig. 3E).
Assessment of neovascularization in
the necrotic area
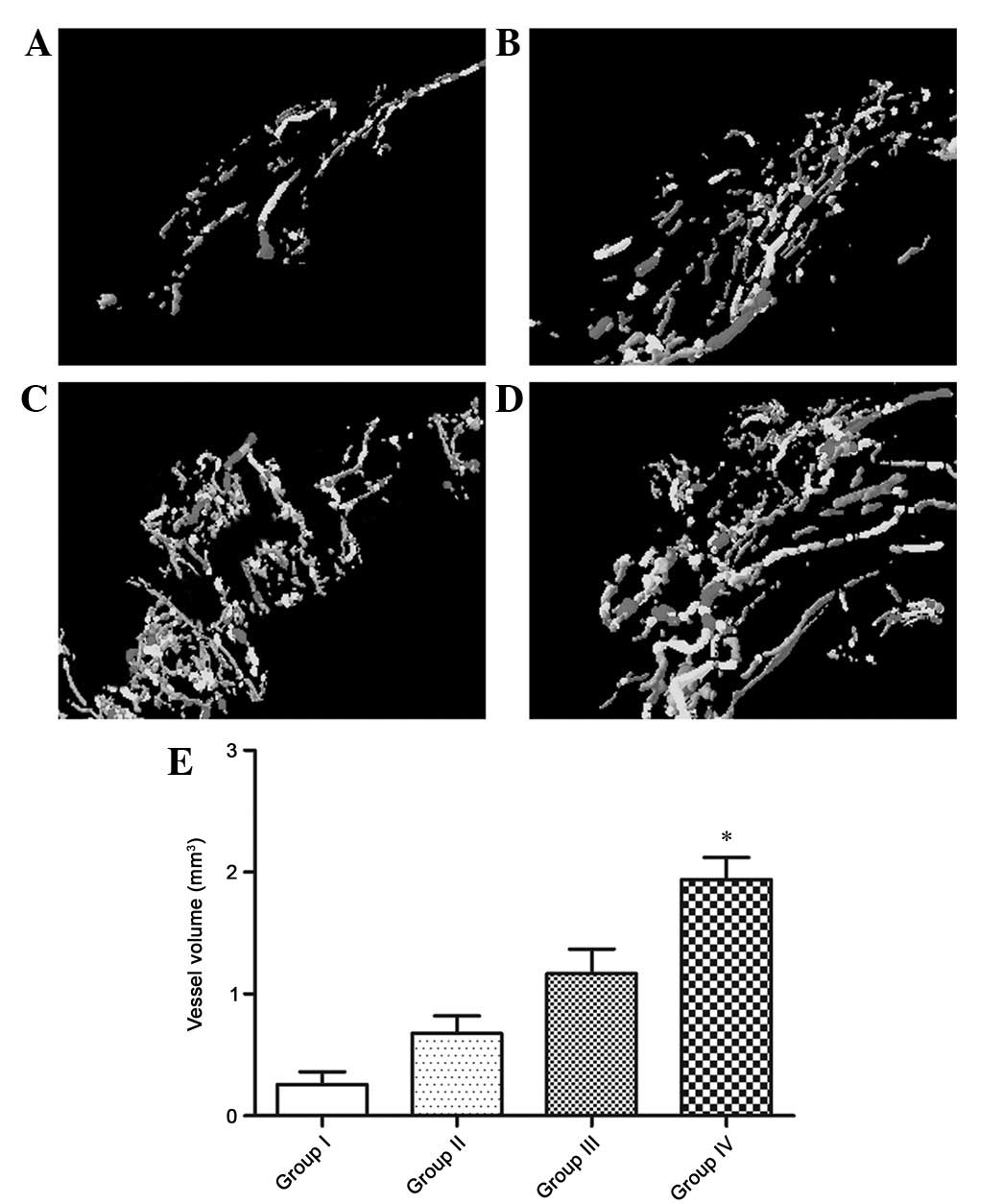
The vascularization in the necrotic area of each
group at four weeks after surgery was evaluated by perfusing the
blood vessels with a silicone injection compound and imaging with
micro-CT. The reconstructed three dimensional images showed the
morphology of regenerated vessels in the necrotic area. In Group I,
there was nearly no vascular architecture in the necrotic area
(Fig. 4A). In Group II, only some
blood vessels were observed (Fig.
4B). In Group III, the density of the vessels was significantly
higher than that of Group II (Fig.
4C). In Group IV, there were large vessels, which were
obviously increased compared to the other three groups (Fig. 4D). Quantitative analysis also showed
that the average number and volume of blood vessels penetrating in
the necrotic area of Group IV were significantly more than the
other three groups (P<0.05; Fig.
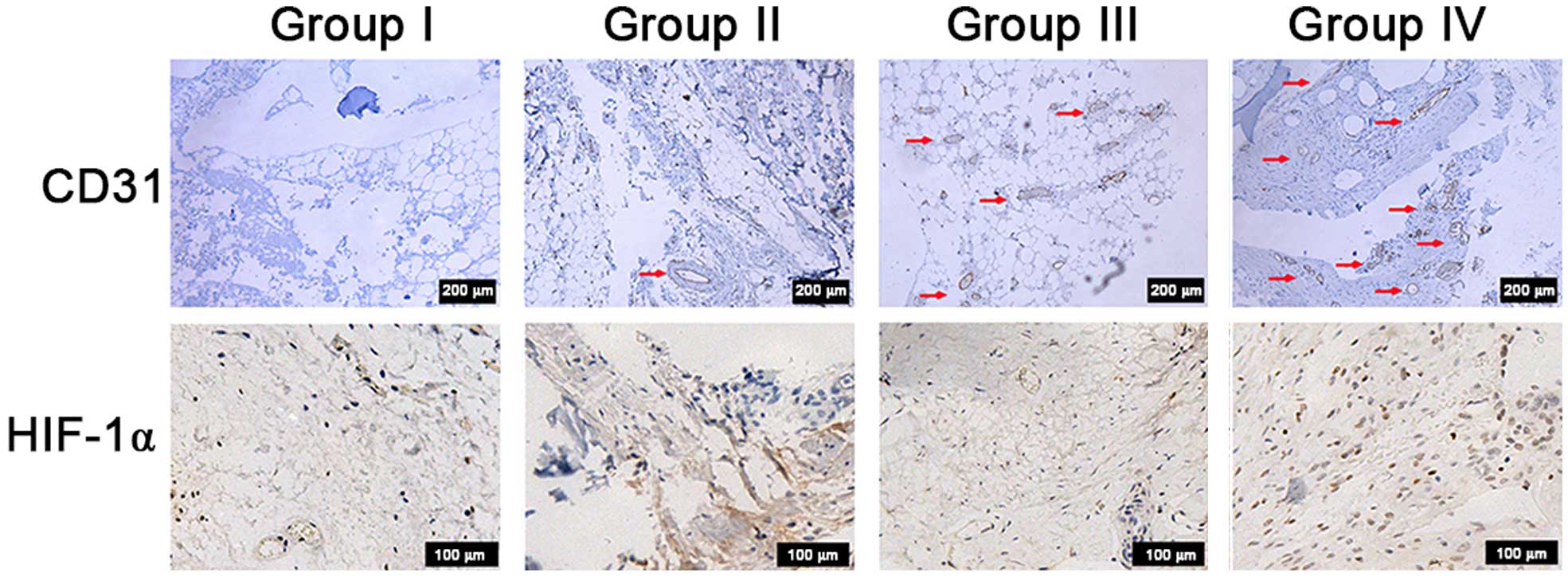
4E). In addition, immunohistochemistry for CD31 was performed
to evaluate newly formed vessels in the necrotic area. Blood
vessels were defined with positive CD31 stain and their typical
round or oval structure. The results showed more vessels in Group
IV than the other three groups, which supported the micro-CT
results (Fig. 5).
HIF-1α expression in ASCs in vivo
Immunohistochemistry for HIF-1α was performed to
evaluate HIF-1α expression in ASCs in vivo (Fig. 5). In Groups I, II and III, there were
no obvious HIF-1α-positive cells observed in the necrotic area.
However, positive cells were apparent in Group IV, which indicated
that sustained release of DMOG could enhance the expression of
HIF-1α in ASCs in vivo.
Discussion
Corticosteroid-induced ONFH is a major type of ONFH,
which is a serious complication of corticosteroid treatment for
autoimmune diseases, such as systemic lupus erythematosus,
nephrotic syndrome and rheumatoid arthritis (27). The diagnostic or therapeutic strategy
for ONFH is best introduced at the early stage before the disease
becomes irreversible. Currently, the treatment methods of
early-stage ONFH are highly controversial (28). Core decompression is reported to be
effective for early-stage ONFH, and acts to reverse the natural
process of ONFH by providing a conduit for angiogenesis to
revascularize subchondral bone and reducing elevated intraosseous
pressures (29,30). However, the majority of studies about
the effectiveness of core decompression suggest that the results of
this approach are not satisfactory (31,32).
The aseptic necrotic bone in the femoral head
retains its normal strength until the natural process of
revascularization starts to remove the dead bone in preparation for
the formation of new bone. As repair advances, the speed of
angiogenesis and osteogenesis becomes slower than absorption of the
dead bone, which may cause a weakening of mechanical structure
(3). Jones hypothesized that new
capillaries could only penetrate 10–15 mm of necrotic bone, and
subchondral bone tissue usually can not be repaired (33). Furthermore, microfractures of the
subchondral bone may retard capillary penetration, and then the
loaded areas would collapse (33).
Thus, it is important for ONFH treatment to increase local
vascularization and new bone formation.
It has been reported that the MSCs pool of the
femoral head could not provide enough osteoblasts to meet the need
of local bone regeneration (34).
Researchers have also suggested that MSCs in the proximal femur
have a decreased proliferative and differentiation capacity at the
early stage of ONFH (35,36). Therefore, MSCs have been employed to
aid core decompression to treat early-stage ONFH (11,12,37).
Hypoxia inducible factor-1a (HIF-1α) is an important functional
subunit of the HIF family, which are crucial mediators of the
adaptive cells response to hypoxia (17). HIF-1α arose early in evolution, and
is widely expressed in most human tissues (17). A previous study found that HIF-1α
controls the expression of numerous genes in cells, cell
proliferation and differentiation (38). Our previous study showed that,
compared with normal MSCs, HIF-1α transgenic MSCs had improved
osteogenic and angiogenic capacity in vitro and better
potential to promote bone regeneration in the necrotic area of the
femoral head (19).
However, the risks of gene transduction, such as
tumorigenesis and permanent overexpression of the transduced gene,
limited its clinical application (20). To overcome these deficiencies, in the
present study dimethyloxaloylglycine (DMOG), a cell permeable
prolyl-4-hydroxylase inhibitor, was employed to enhance HIF-1α
expression in MSCs in place of the HIF-1α gene transduction.
DMOG is a small molecular drug, which is able to
stabilize the expression of HIF-1α in cells (21). At normal oxygen tension, HIF-1α is
modified by oxygen dependent prolyl hydroxylases, resulting in
rapid degradation through the ubiquitin-proteasome pathway
(22). Under hypoxic conditions,
prolyl hydroxylase activity decreases and HIF-1α is stabilized
(39). DMOG is able to inhibit
prolyl hydroxylase activity at normal oxygen tension, thus leading
to HIF-1α overexpression in cells. DMOG has been used to treat
ischemic skeletal muscles, middle cerebral artery occlusion and
ischemic myocardial injury, and all resulted in good outcomes in
previous experiments (40–42). Our previous study showed that DMOG
could significantly enhance VEGF production in ASCs and improved
the osteogenic differentiation potential of ASCs in vitro by
stabilizing the expression of HIF-1α in ASCs, and DMOG-treated ASCs
had an increased bone healing capacity and promoted local
revascularization in critical defects (22). In the present study, we investigated
the efficacy of implanting DMOG-treated ASCs to treat early-stage
corticosteroid-induced ONFH.
This study used a rabbit model with steroid-induced
early-stage ONFH. An animal model of ONFH is important for
evaluation of the effects of various methods of treating ONFH. In
the present model, osteonecrosis was induced by a combination of
LPS and MPS to mimic the pathological mechanism of steroid-induced
ONFH. It has been reported that this inductive protocol has a high
incidence of ONFH, and resulted in nearly no death, and suggested
that numerous histopathological and pathogenetic features of
steroid-induced ONFH in rabbits are similar to those observed in
human early-stage ONFH (25).
Therefore, the steroid-induced rabbit ONFH model may be effective
for testing the efficacy of the method developed for treatment of
steroid-associated ONFH for clinical application and confirmation
of their long-term effects in prevention of subchondral bone
collapse of the hips.
In the present study, DMOG-treated ASCs were
implanted into the necrotic area of the femoral head to aid core
decompression in improving bone healing. Micro-CT and histological
results indicated there was increased bone regeneration in the
normal ASCs group than in the group that underwent core
decompression only, which suggests that ASCs could improve bone
healing on their own. Increased newly formed bone was observed in
the DMOG-treated ASCs group than in the normal ASCs group, which
indicated DMOG could enhance the bone healing capacity of ASCs in
the necrotic area. Micro-CT and immunohistochemistry detection of
CD31 showed that vessels formation was also increased in the
DMOG-treated ASCs group than in the other three groups. This may be
because DMOG could increase the expression and secretion of certain
angiogenic factors in ASCs in vivo by stabilizing the HIF-1α
expression in cells, which has been demonstrated by previous
experiments (43). It is
hypothesized that angiogenesis is closely associated with
osteogenesis, and that neovascularization is an favorable element
in bone regeneration. Therefore, the improved local blood supply
may also contribute to bone healing in the necrotic area.
In summary, the results of the present study showed
that DMOG-treated ASCs markedly increased vascularization and bone
regeneration in necrotic area of the femoral head in ONFH rabbits.
These findings suggest that DMOG could enhance the osteogenic
activity of ASCs in vivo, and may therefore provide a novel
and effective therapeutic option for early-stage
corticosteroid-induced ONFH.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (grant nos. 81272004, 81272003 and
81371962) and Foundation of Shanghai Sixth People's Hospital (grant
no. 1631).
Glossary
Abbreviations
Abbreviations:
|
MSCs
|
mesenchymal stem cells
|
|
HIF-1α
|
hypoxia inducible factor-1α
|
|
DMOG
|
dimethyloxalylglycine
|
|
ASCs
|
adipose-derived stem cells
|
|
ONFH
|
osteonecrosis of the femoral head
|
References
|
1
|
Kerachian MA, Harvey EJ, Cournoyer D, Chow
TY and Séguin C: Avascular necrosis of the femoral head: Vascular
hypotheses. Endothelium. 13:237–244. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bachiller FG, Caballer AP and Portal LF:
Avascular necrosis of the femoral head after femoral neck fracture.
Clin Orthop Relat Res. 87–109. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lieberman JR, Berry DJ, Mont MA, Aaron RK,
Callaghan JJ, Rajadhyaksha AD and Urbaniak JR: Osteonecrosis of the
hip: Management in the 21st century. Instr Course Lect. 52:337–355.
2003.PubMed/NCBI
|
|
4
|
Yoon TR, Song EK, Rowe SM and Park CH:
Failure after core decompression in osteonecrosis of the femoral
head. Int Orthop. 24:316–318. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yuan J, Cui L, Zhang WJ, Liu W and Cao Y:
Repair of canine mandibular bone defects with bone marrow stromal
cells and porous beta-tricalcium phosphate. Biomaterials.
28:1005–1013. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Liu G, Zhao L, Zhang W, Cui L, Liu W and
Cao Y: Repair of goat tibial defects with bone marrow stromal cells
and beta-tricalcium phosphate. J Mater Sci Mater Med. 19:2367–2376.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stamm C, Westphal B, Kleine HD, Petzsch M,
Kittner C, Klinge H, Schümichen C, Nienaber CA, Freund M and
Steinhoff G: Autologous bone-marrow stem-cell transplantation for
myocardial regeneration. Lancet. 361:45–46. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schächinger V, Erbs S, Elsässer A,
Haberbosch W, Hambrecht R, Hölschermann H, Yu J, Corti R, Mathey
DG, Hamm CW, et al: Intracoronary bone marrow-derived progenitor
cells in acute myocardial infarction. N Engl J Med. 355:1210–1221.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dadon-Nachum M, Sadan O, Srugo I, Melamed
E and Offen D: Differentiated mesenchymal stem cells for sciatic
nerve injury. Stem Cell Rev. 7:664–671. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yang Y, Hallgrimsson B and Putnins EE:
Craniofacial defect regeneration using engineered bone marrow
mesenchymal stromal cells. J Biomed Mater Res A. 99:74–85. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gangji V, De Maertelaer V and Hauzeur JP:
Autologous bone marrow cell implantation in the treatment of
non-traumatic osteonecrosis of the femoral head: Five year
follow-up of a prospective controlled study. Bone. 49:1005–1009.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tzaribachev N, Vaegler M, Schaefer J,
Reize P, Rudert M, Handgretinger R and Müller I: Mesenchymal
stromal cells: A novel treatment option for steroid-induced
avascular osteonecrosis. Isr Med Assoc J. 10:232–234.
2008.PubMed/NCBI
|
|
13
|
Cowan CM, Shi YY, Aalami OO, Chou YF, Mari
C, Thomas R, Quarto N, Contag CH, Wu B and Longaker MT:
Adipose-derived adult stromal cells heal critical-size mouse
calvarial defects. Nat Biotechnol. 22:560–567. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dudas JR, Marra KG, Cooper GM, Penascino
VM, Mooney MP, Jiang S, Rubin JP and Losee JE: The osteogenic
potential of adipose-derived stem cells for the repair of rabbit
calvarial defects. Ann Plast Surg. 56:543–548. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nikol S, Engelmann MG, Pelisek J, Fuchs A,
Golda A, Shimizu M, Mekkaoui C and Rolland PH: Local perivascular
application of low amounts of a plasmid encoding for vascular
endothelial growth factor (VEGF165) is efficient for therapeutic
angiogenesis in pigs. Acta Physiol Scand. 176:151–159. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Elçin YM, Dixit V and Gitnick G: Extensive
in vivo angiogenesis following controlled release of human vascular
endothelial cell growth factor: Implications for tissue engineering
and wound healing. Artif Organs. 25:558–565. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mazumdar J, Dondeti V and Simon MC:
Hypoxia-inducible factors in stem cells and cancer. J Cell Mol Med.
13:4319–4328. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zou D, Zhang Z, Ye D, Tang A, Deng L, Han
W, Zhao J, Wang S, Zhang W, Zhu C, et al: Repair of critical-sized
rat calvarial defects using genetically engineered bone
marrow-derived mesenchymal stem cells overexpressing
hypoxia-inducible factor-1α. Stem Cells. 29:1380–1390.
2011.PubMed/NCBI
|
|
19
|
Ding H, Gao YS, Hu C, Wang Y, Wang CG, Yin
JM, Sun Y and Zhang CQ: HIF-1α transgenic bone marrow cells can
promote tissue repair in cases of corticosteroid-induced
osteonecrosis of the femoral head in rabbits. PLoS One.
8:e636282013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cesana D, Ranzani M, Volpin M, Bartholomae
C, Duros C, Artus A, Merella S, Benedicenti F, Sergi L Sergi,
Sanvito F, et al: Uncovering and dissecting the genotoxicity of
self-inactivating lentiviral vectors in vivo. Mol Ther. 22:774–785.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jaakkola P, Mole DR, Tian YM, Wilson MI,
Gielbert J, Gaskell SJ, von Kriegsheim A, Hebestreit HF, Mukherji
M, Schofield CJ, et al: Targeting of HIF-alpha to the von
Hippel-Lindau ubiquitylation complex by O2-regulated prolyl
hydroxylation. Science. 292:468–472. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ding H, Gao YS, Wang Y, Hu C, Sun Y and
Zhang C: Dimethyloxaloylglycine increases the bone healing capacity
of adipose-derived stem cells by promoting osteogenic
differentiation and angiogenic potential. Stem Cells Dev.
23:990–1000. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
National Research Council Institute for
Laboratory Animal Research, . Guide for the Care and Use of
Laboratory Animals. National Academies Press; Washington, DC:
1996
|
|
24
|
Ding H, Chen S, Yin JH, Xie XT, Zhu ZH,
Gao YS and Zhang CQ: Continuous hypoxia regulates the osteogenic
potential of mesenchymal stem cells in a time-dependent manner. Mol
Med Rep. 10:2184–2190. 2014.PubMed/NCBI
|
|
25
|
Qin L, Zhang G, Sheng H, Yeung KW, Yeung
HY, Chan CW, Cheung WH, Griffith J, Chiu KH and Leung KS: Multiple
bioimaging modalities in evaluation of an experimental
osteonecrosis induced by a combination of lipopolysaccharide and
methylprednisolone. Bone. 39:863–871. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sun Y, Feng Y and Zhang C: The effect of
bone marrow mononuclear cells on vascularization and bone
regeneration in steroid-induced osteonecrosis of the femoral head.
Joint Bone Spine. 76:685–690. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Griffith JF, Antonio GE, Kumta SM, Hui DS,
Wong JK, Joynt GM, Wu AK, Cheung AY, Chiu KH, Chan KM, et al:
Osteonecrosis of hip and knee in patients with severe acute
respiratory syndrome treated with steroids. Radiology. 235:168–175.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ohzono K, Saito M, Sugano N, Takaoka K and
Ono K: The fate of nontraumatic avascular necrosis of the femoral
head. A radiologic classification to formulate prognosis. Clin
Orthop Relat Res. 277:73–78. 1992.
|
|
29
|
Hopson CN and Siverhus SW: Ischemic
necrosis of the femoral head. Treatment by core decompression. J
Bone Joint Surg Am. 70:1048–1051. 1988.PubMed/NCBI
|
|
30
|
Maniwa S, Nishikori T, Furukawa S,
Kajitani K, Iwata A, Nishikawa U and Ochi M: Evaluation of core
decompression for early osteonecrosis of the femoral head. Arch
Orthop Trauma Surg. 120:241–244. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dailiana ZH, Toth AP, Gunneson E, Berend
KR and Urbaniak JR: Free vascularized fibular grafting following
failed core decompression for femoral head osteonecrosis. J
Arthroplasty. 22:679–688. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Scully SP, Aaron RK and Urbaniak JR:
Survival analysis of hips treated with core decompression or
vascularized fibular grafting because of avascular necrosis. J Bone
Joint Surg Am. 80:1270–1275. 1998.PubMed/NCBI
|
|
33
|
Jones JP Jr: Concepts of etiology and
early pathogenesis of osteonecrosis. Instr Course Lect. 43:499–512.
1994.PubMed/NCBI
|
|
34
|
Hernigou P, Beaujean F and Lambotte JC:
Decrease in the mesenchymal stem-cell pool in the proximal femur in
corticosteroid-induced osteonecrosis. J Bone Joint Surg Br.
81:349–355. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gangji V, Hauzeur JP, Schoutens A,
Hinsenkamp M, Appelboom T and Egrise D: Abnormalities in the
replicative capacity of osteoblastic cells in the proximal femur of
patients with osteonecrosis of the femoral head. J Rheumatol.
30:348–351. 2003.PubMed/NCBI
|
|
36
|
Lee JS, Lee JS, Roh HL, Kim CH, Jung JS
and Suh KT: Alterations in the differentiation ability of
mesenchymal stem cells in patients with nontraumatic osteonecrosis
of the femoral head: Comparative analysis according to the risk
factor. J Orthop Res. 24:604–609. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Yan ZQ, Chen YS, Li WJ, Yang Y, Huo JZ,
Chen ZR, Shi JH and Ge JB: Treatment of osteonecrosis of the
femoral head by percutaneous decompression and autologous bone
marrow mononuclear cell infusion. Chin J Traumatol. 9:3–7.
2006.PubMed/NCBI
|
|
38
|
Riddle RC, Khatri R, Schipani E and
Clemens TL: Role of hypoxia-inducible factor-1alpha in
angiogenic-osteogenic coupling. J Mol Med (Berl). 87:583–590. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Piret JP, Lecocq C, Toffoli S, Ninane N,
Raes M and Michiels C: Hypoxia and CoCl2 protect HepG2 cells
against serum deprivation- and t-BHP-induced apoptosis: A possible
anti-apoptotic role for HIF-1. Exp Cell Res. 295:340–349. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ockaili R, Natarajan R, Salloum F, Fisher
BJ, Jones D, Fowler AA III and Kukreja RC: HIF-1 activation
attenuates postischemic myocardial injury: Role for heme
oxygenase-1 in modulating microvascular chemokine generation. Am J
Physiol Heart Circ Physiol. 289:H542–H548. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Milkiewicz M, Pugh CW and Egginton S:
Inhibition of endogenous HIF inactivation induces angiogenesis in
ischaemic skeletal muscles of mice. J Physiol. 560:21–26. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Nagel S, Papadakis M, Chen R, Hoyte LC,
Brooks KJ, Gallichan D, Sibson NR, Pugh C and Buchan AM:
Neuroprotection by dimethyloxalylglycine following permanent and
transient focal cerebral ischemia in rats. J Cereb Blood Flow
Metab. 31:132–143. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ding H, Chen S, Song WQ, Gao YS, Guan JJ,
Wang Y, Sun Y and Zhang CQ: Dimethyloxaloylglycine improves
angiogenic activity of bone marrow stromal cells in the
tissue-engineered bone. Int J Biol Sci. 10:746–756. 2014.
View Article : Google Scholar : PubMed/NCBI
|