Introduction
There is much debate concerning the definition,
classification and criteria of acute liver failure (ALF) (1–3). In the
USA, these criteria include evidence of coagulation abnormality,
typically an international normalized ratio (INR) ≥1.5, and hepatic
encephalopathy (HE) in a patient without preexisting cirrhosis and
with an illness lasting <26 weeks (2). In China, an ALF diagnosis necessitates
evidence of an INR of ≥1.5 or prothrombin activity (PTA) ≤40%,
onset of HE of grade ≥2 within 2 weeks of the onset of symptoms and
an absence of preexisting liver disease (3). Subacute liver failure (SALF) is
diagnosed under the following criteria: i) Serum total bilirubin
(T-Bil) ≥10 mg/dl or increased daily levels of T-Bil (T-Bil/d) to
≥1 mg/dl; ii) INR ≥1.5 or PTA ≤40%; and iii) length of illness
>2 weeks and <26 weeks, in the presence or absence of HE
(3). In China, acute viral infection
is common, including hepatitis A, B and E viruses (HAV, HBV and
HEV), and is causative of most cases of ALF and SALF (3,4). By
contrast, acute viral infection is a less prevalent cause in
developed countries, in which drug-induced ALF, typically due to
acetaminophen, is the most common etiology (5,6).
However, the etiology of 17% of ALF cases remains indeterminate
following extensive evaluation (5).
As for the developed world, ALF and SALF are rare;
an overall incidence of 1–6 cases per million every year has been
reported (5). In countries like
China where infective hepatitis is common, rates are expected to be
higher (5). ALF or SALF are serious
clinical syndromes, with high mortality rates, ranging between
60–80% (5,6). However, no etiology-specific treatments
currently exist to improve the prognosis of non-acetaminophen ALF
and SALF (6). Although the precise
etiologies of ALF and SALF are unclear, excessive inflammation is
established to have a key role in the pathophysiology of ALF and
SALF (7,8). In fact, sudden and severe disorder of
hepatic function in ALF results from severe degeneration or
necrosis of extensive numbers of hepatocytes, induced by
inflammatory mediators, cytotoxic substances and activated
lymphocytes (7,8). Hepatocyte degeneration is reversible,
whereas hepatocyte necrosis is irreversible. The occurrence of
massive or submassive hepatic necrosis may indicate that the
patient is unlikely to survive (9);
therefore, it is important to improve the prognosis of ALF in order
to prevent extensive hepatocyte degeneration from progressing to
hepatic necrosis. Corticosteroids can rapidly inhibit an excessive
immune response and inflammatory reaction (10,11).
Corticosteroids have several other hepatoprotective roles,
including preventing cytolysis of ballooned hepatocytes and
protecting hepatocytes against apoptosis induced by cadmium
toxicity (12–14). Previous work by the present authors
and other groups has revealed that corticosteroids are effective in
treating pre-acute-on-chronic liver failure (pre-ACLF) associated
with HBV and severe acute exacerbation (SAE) of chronic hepatitis B
(15–17). Therefore, treating ALF and SALF with
corticosteroids is a reasonable treatment regimen. A few previous
case reports demonstrated that corticosteroids were effective in
treating ALF associated with viral infection, drug-induced ALF,
autoimmune ALF and ACLF associated with HBV (16,18,19).
However, the administration of corticosteroids in patients with ALF
and SALF remains controversial. A recent report by Karkhanis et
al (20) revealed that
corticosteroids were not effective in improving the prognosis of
patients with ALF. These extent of hepatic necrosis and the
regenerative ability of hepatocytes are important in determining
the prognosis of liver failure (3).
When extensive confluent cellular necrosis develops, the
administration of corticosteroids is not able to improve the
prognosis of patients with ALF and SALF. This is as corticosteroids
have a limited effect on the regenerative ability of hepatocytes
over a short time period (21).
Therefore, the selection of appropriate patients and the timing of
intervention with corticosteroids are very important factors in the
prognosis of patients with ALF and SALF.
Therefore, the present study aimed to evaluate the
efficacy of corticosteroids in improving rates of transplant-free
or spontaneous survival (SS) of patients with ALF and SALF, and to
determine the patients who respond best to corticosteroids, and the
most appropriate timing of corticosteroid administration.
Materials and methods
Ethics statement
Written informed consent was obtained from all of
the patients or their next-of-kin. The protocol was approved by the
Ethics Committee of Southwest Hospital, Chongqing, China.
Patients and study design
The present study was a retrospective analysis of
randomly selected patients with ALF and SALF who were hospitalized
in the Department of Infectious Diseases, Southwest Hospital
(Chongqing, China) from 2000–2012. The eligibility criteria for
patients with ALF were as follows: i) Serum T-Bil ≥10 mg/dl or an
increased T-Bil/d ≥1 mg/dl; ii) PTA ≤40%; iii) onset of HE grade ≥2
within 2 weeks of onset of symptoms; and iv) an absence of
preexisting liver disease (22). The
eligibility criteria for patients with SALF were as follows: i)
Serum T-Bil ≥10 mg/dl; ii) PTA ≤40%; iii) length of illness <26
weeks (with or without HE); and iv) absence of preexisting liver
disease. A total of 238 patients were enrolled in the study,
including 73 patients with ALF and 165 patients with SALF.
Subsequent to obtaining informed consent, the detailed clinical and
laboratory data were anonymously collected on admission to the
hospital, and once a week until week 12, and then once every 4
weeks until week 24 or until mortality. The etiologies of ALF and
SALF in the present sample were determined to include 108 cases
associated with viral infection (HAV=4, HBV=85, HEV=12,
cytomegalovirus=3, Epstein-Barr virus=2 and herpes simplex virus=2)
and 130 patients associated with non-viral infection
(drug-induced=58, autoimmune=2, hyperthyroidism=4 and
indeterminate=66).
The primary endpoint was SS, defined as survival
without transplantation or death until 24 weeks after admission to
the hospital. Amongst 238 patients, 1 patient received liver
transplantation on the 11th day of admission and survived, and 2
patients received liver transplantation on the 7th day of admission
but succumbed to pulmonary infection. These donor livers were from
victims of accidental deaths.
The primary predictor was corticosteroid use,
defined as any dose of oral prednisone or intravenous dexamethasone
(Dex). In 79.4% of patients with ALF, corticosteroid treatment
began following the onset of HE. In all 21 patients with SALF,
corticosteroid treatment commenced following the diagnosis of SALF,
which was determined subsequent to the onset of HE in 7 patients.
The subgroup analyses were performed based on clinical type (ALF
and SALF), etiologies (viral and non-viral infection) and the
severity of liver failure. Otherwise, the impact of steroid use on
survival was analyzed based on the timing of intervention. The
impact of corticosteroids, nucleoside/nucleotide analogues (NUCs)
and antiviral therapy on survival was also analyzed among the
patients with acute HBV-associated liver failure.
Corticosteroid administration
Deciding whether to administer corticosteroids was
entirely at the discretion of the physician in charge of a patient.
The timing, route of administration and dosing of corticosteroids
were also determined by the physician in charge of a patient and
the variables were not uniform. Intravenous Dex was first
administered in 85.5% (47/55) of patients, intravenous cortisol was
administered in 7.3% (4/55) of patients and oral prednisone was
administered in 7.3% (4/55) of patients, the timing of which was
determined by respective physicians. The initial dose of Dex or Dex
equivalents was 10 mg/d in 50.9% (28/55) of patients, 5–10 mg/d in
18.2% (10/55) of patients, 11–15 mg/d in 14.5% (8/55) of patients,
20 mg/d in 14.5% (8/55) of patients and 30 mg in one patient
(1.8%). The duration of steroid therapy was 1–4 days in 41.8%
(23/55) of patients, 5 days in 30.9% (17/55) of patients, 10 days
in 3.6% (2/55) of patients and more than 10 days in 23.6% (13/55)
of patients.
Antiviral therapy in HBV
Deciding whether to administer antiviral drugs was
entirely at the discretion of the physician in charge of a patient
and based on understanding the role of antiviral therapy in
treating liver failure associated with HBV infection. Of 85
patients, 43 (50.6%) patients received antiviral therapy with NUCs.
Lamivudine (100 mg/d) was administered to 62.8% (27/43) of the
patients, entecavir (0.5 mg/d) was administered to 34.9% (15/43) of
the patients and adefovir (10 mg/d) was administered to 1 patient
(2.3%).
Statistical analyses
Continuous variables are expressed as the mean ±
standard deviation. Categorical variables were analyzed using a
chi-square analysis, and continuous variables were tested using
Student's t–test. Additionally, univariate and multivariate
logistic regression analyses were performed to evaluate the
predictors of SS. All predictors with P<0.2 in the univariate
analysis were evaluated in the multivariate model and were then
sequentially removed to establish the final model. All analyses
were performed using the SPSS v. 10.0 statistical software package
(SPSS Inc., Chicago, IL, USA). P<0.05 was considered to
represent a statistically significant difference.
Results
Characteristics of the study
population
The clinical characteristics of patients with viral
and non-viral liver failure are presented in Table I. There were significant differences
between the two groups with regard to gender, coma grade, alanine
aminotransferase (ALT) levels, aspartate aminotransferase (AST)
levels and clinical type. No significant differences were observed
in baseline creatinine, INR and model for end-stage liver disease
(MELD) score between the two groups. The patients with viral liver
failure had a higher rate of corticosteroid use (34.3%) compared
with those with non-viral liver failure (13.8%; P<.001).
 | Table I.Baseline demographics of patients,
comparing etiology. |
Table I.
Baseline demographics of patients,
comparing etiology.
| Variable | Viral (n=108) | Non-viral
(n=130) | P-value |
|---|
| Gender (%) |
|
| <0.001 |
|
Male | 72 (66.7) | 51 (39.2) |
|
|
Female | 36 (33.3) | 79 (60.8) |
|
| Age, mean
years±SD | 35.1±15.8 | 38.3±19.3 | 0.186 |
| Type (%) |
|
| <0.001 |
|
ALF | 46 (42.6) | 27 (20.8) |
|
|
SALF | 62 (57.4) | 103 (79.2) |
|
| Coma grade (%) |
|
| 0.004 |
| 0 | 45 (41.7) | 90 (69.2) |
|
| 1 | 0 (0.0) | 1 (0.8) |
|
| 2 | 21 (19.4) | 16 (12.3) |
|
| 3 | 27 (25.0) | 18 (13.8) |
|
| 4 | 12 (11.1) | 8 (6.2) |
|
| Steroid use |
|
| <0.001 |
| Total
number of patients (%) | 37 (34.3) | 18 (13.8) |
|
| Daily
Dex dose, mg/d (range) | 10 (5–20) | 10 (5–30) |
| Days of
steroid use, mg/d (range) | 5 (1–90) | 5 (1–60) |
| Mean MELD | 31.3±6.2 | 30.2±6.5 | 0.162 |
| Laboratory
values |
|
|
|
| ALT,
IU/l | 1428±1637 | 591±740 | <0.001 |
| AST,
IU/l | 1229±1745 | 643±938 | 0.001 |
| T-Bil,
mg/dl | 21.4±10.3 | 24.2±11.2 | 0.050 |
| Cr,
mg/dl | 1.22±0.59 | 1.20±0.59 | 0.822 |
| INR | 3.35±1.70 | 3.08±2.02 | 0.268 |
The baseline characteristics of patients receiving
or not receiving corticosteroid therapy are reported in Table II. There was a significant
difference in gender between the two groups (P=0.218). The
incidence and the severity of HE at baseline were significantly
higher in the steroid use group than those not receiving steroid
treatment (P=0.009). No significant differences were observed in
baseline creatinine, INR and MELD scores between the two groups.
However, the baseline levels of serum ALT and AST values were
significantly higher in the steroid use group than those in the no
steroid use group (P<0.01). The baseline levels of serum T-Bil
were significantly lower in the steroid use group than those in the
no steroid use group (P<.001).
| Table II.Baseline characteristics of patients,
comparing steroid use. |
Table II.
Baseline characteristics of patients,
comparing steroid use.
| Variable | Steroids
(n=55) | No steroids
(n=183) | P-value |
|---|
| Gender (%) |
|
| 0.218 |
|
Male | 24 (43.6) | 99 (54.1) |
|
|
Female | 31 (56.4) | 84 (45.9) |
|
| Age, mean
years±SD | 30.8±12.5 | 38.7±18.8 | 0.004 |
| Type (%) |
|
| <0.001 |
|
ALF | 34 (60.8) | 39 (21.3) |
|
|
SALF | 21 (38.2) | 144 (78.7) |
|
| Coma grade (%) |
|
| 0.009 |
| 0 | 20 (36.4) | 115 (62.8) |
|
| 1 | 0 (0.0) | 1 (0.5) |
|
| 2 | 11 (20.0) | 27 (14.8) |
|
| 3 | 16 (29.1) | 29 (15.8) |
|
| 4 | 8 (14.5) | 12 (6.6) |
|
| Etiologies (%) |
|
| <0.001 |
|
Viral | 37 (67.3) | 71 (38.8) |
|
|
Non-viral | 18 (32.7) | 112 (61.2) |
|
| Mean MELD | 31.0±5.4 | 30.6±6.7 | 0.736 |
| Laboratory
values |
|
|
|
| ALT,
IU/l | 1878±1958 | 698±854 | <0.001 |
| AST,
IU/l | 1403±1626 | 760±1282 | 0.003 |
| T-Bil,
mg/dl | 18.4±8.6 | 24.3±11.1 | <0.001 |
| Cr,
mg/dl | 1.14±0.52 | 1.23±0.61 | 0.330 |
| INR | 3.47±1.29 | 3.12±2.02 | 0.231 |
Effects of corticosteroids on the
prognosis following liver failure
The SS of patients with liver failure was 24.37% at
24 weeks after admission to our hospital. There was no significant
difference in SS between the steroid use group and the no steroid
use group in an 8-week period (Table
III). However, SS rates after 12− and 24-week periods for
patients treated with corticosteroids were significantly higher
than those for patients not treated with corticosteroids (P=0.021
and 0.011, respectively) (Table
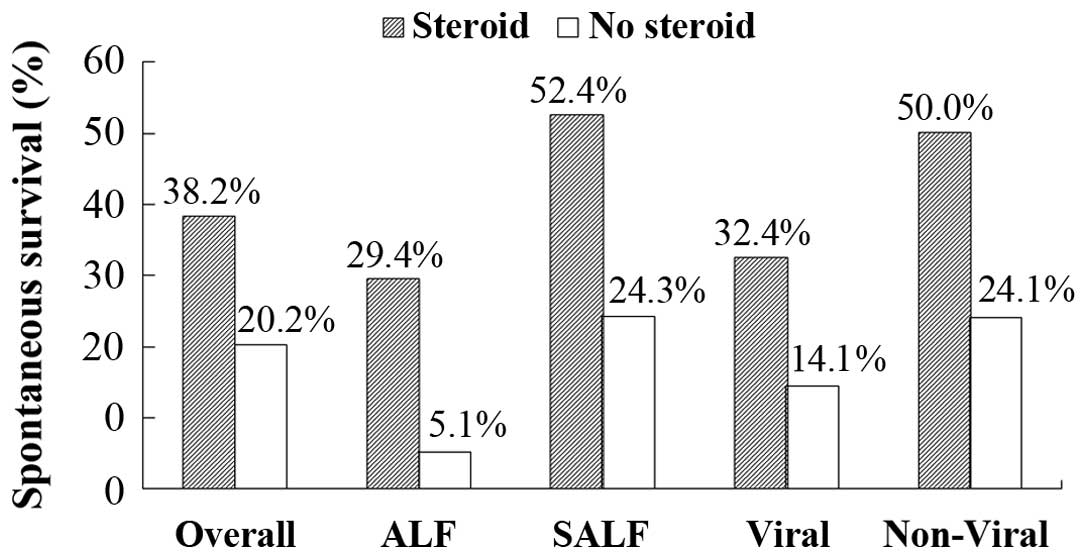
III and Fig. 1). In patients
with ALF, the rate of SS was 29.41% for patients who received
corticosteroids vs. 5.13% for those who did not receive
corticosteroids (P=0.013) (Fig. 1).
In patients with SALF, the rate of SS was 52.38% for those who
received corticosteroids vs. 24.31% for those who did not receive
corticosteroids (P=0.016) (Fig. 1).
For patients with viral and non-viral liver failure, respectively,
SS rates were 32.43 and 52.38% in the steroid use group, which was
significantly higher than the rates of 14.08 and 24.31% in the no
steroid group (P=0.042, 0.043). In the steroid use group, SS rates
in patients with SALF were higher than SS rates in patients with
ALF (52.38% vs. 29.41%); there was no significant difference
between SS rates in these groups (P=0.152). However, in the no
steroid use group, SS rate in patients with SALF was significantly
higher than in patients with ALF (24.31% vs. 5.13%) (P=0.007)
(Fig. 1).
| Table III.Spontaneous survival rate until 24
weeks of treatment. |
Table III.
Spontaneous survival rate until 24
weeks of treatment.
|
| Spontaneous
survival |
|
|---|
|
|
|
|
|---|
| Weeks after
admission | Steroid use
group | No steroid use
group | P-value |
|---|
| 1 | 32 (58.18) | 113 (61.75) | 0.640 |
| 2 | 26 (47.27) | 84 (45.90) | 0.878 |
| 3 | 22 (39.29) | 73 (39.89) | 0.988 |
| 4 | 21 (38.18) | 60 (32.79) | 0.517 |
| 8 | 21 (38.18) | 44 (24.04) | 0.057 |
| 12 | 21 (38.18) | 40 (21.86) | 0.021 |
| 24 | 21 (38.18) | 37 (20.22) | 0.011 |
Effect of corticosteroids, based on
the severity of liver failure
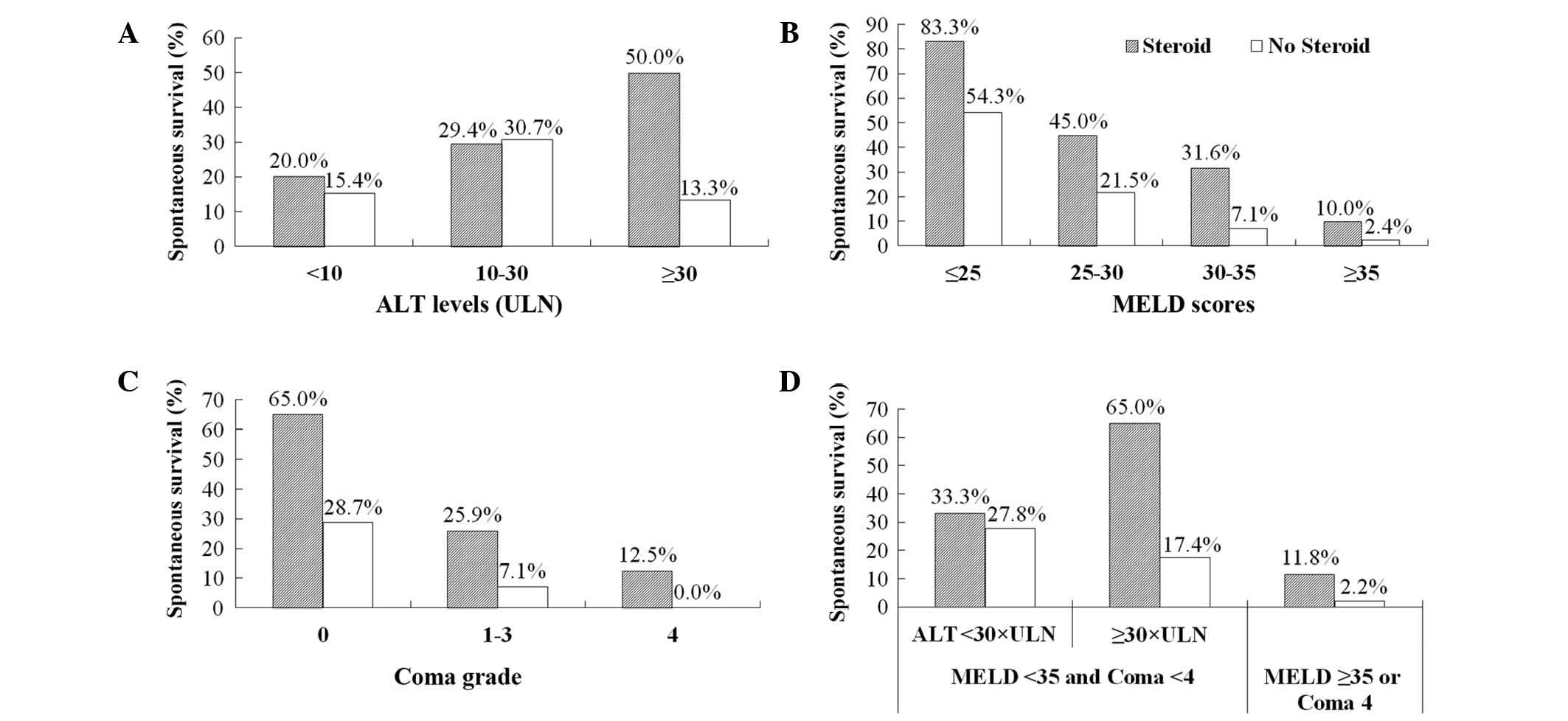
SS was significantly higher (P=0.004) in the steroid
use group (50.00%; 14/28) than in the no steroid use group (13.33%;
4/30) for patients with ALT levels ≥30x the upper limit of normal
(ULN) (Fig. 2A). In the no steroid
use group, SS rate was significantly higher among patients with ALT
levels of 10–30x the ULN than in patients with ALT levels <10x
the ULN [30.65% (19/62) vs. 15.38% (14/91); P=0.029], and was
non-significantly higher than the SS rate in patients with ALT
levels ≥30x ULN (P=0.080). SS rate was significantly higher in the
steroid use group (50.00%; 14/28) than in the no steroid use group
(13.33%; 4/30) in patients with AST levels ≥30x the ULN (P=0.004).
For patients with AST levels <30x the ULN, SS rate was
non-significantly (P=0.620) higher in the steroid use group
(25.93%; 7/27) than in the no steroid use group (21.57%; 33153).
The lower SS rate was closely associated with a higher MELD score
(P<0.001). The SS rate was significantly higher in the steroid
use group than in the no steroid use group in patients with MELD
scores of 25–35 (P=0.048; Fig.
2B).
Amongst 135 patients without HE at the baseline, 60
(44.4%) patients developed a different degree of HE following
treatment. The incidence of HE was 40.0% (8/20) in the steroid use
group and 45.2% (52/115) in the no steroid use group (P=0.808).
There was a significant difference in SS rates between the steroid
use group and the no steroid use group for patients without
baseline HE [65.00% (13/20) vs. 28.70% (33/115); P=0.004] and for
patients with baseline HE grades 1–3 [25.93% (7/27) vs. 7.14%
(4/56); P=0.034] (Fig. 2C).
Among patients with HE grades <4, MELD scores
<35 and ALT levels ≥30x the ULN, the SS rate was significantly
higher in the steroid use group (65.00%; 13/20) than in the no
steroid use group (17.39%; 4/23) (P=0.002) (Fig. 2D).
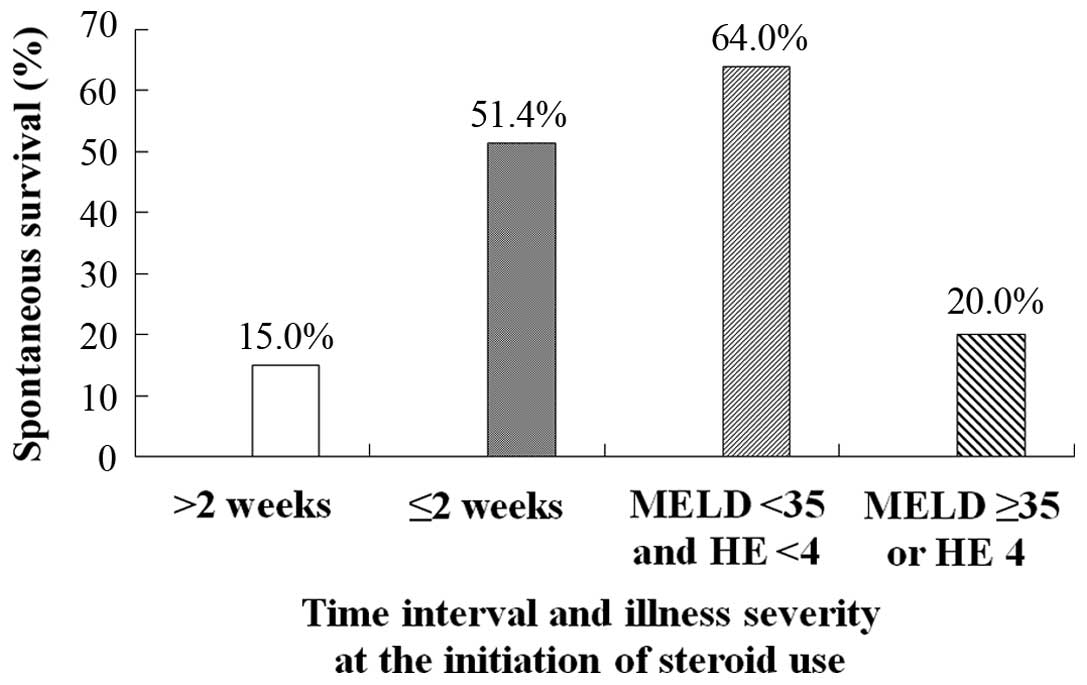
Analysis of outcome according to the
timing of steroid use
The time interval from the onset of symptoms to the
initiation of steroid use was 7.9±5.0 days in 21 spontaneous
survivals, and 13.3±8.2 days in 34 non-survivals, which was a
significant difference (P=0.010). The SS rate was 51.43% (18/35)
for patients with a time interval prior to administration of ≤2
weeks, and 15.00% (3/20) for patients with a time interval prior to
steroid treatment of >2 weeks (P=0.010) (Fig. 3). Among 35 patients with a time
before steroid treatment of ≤2 weeks, the SS rate was 64.00%
(16/25) for patients with MELD scores <35 and HE grades <4,
and 20.00% (2/10) for patients with MELD scores ≥35 or HE grade 4
(P=0.027) (Fig. 3).
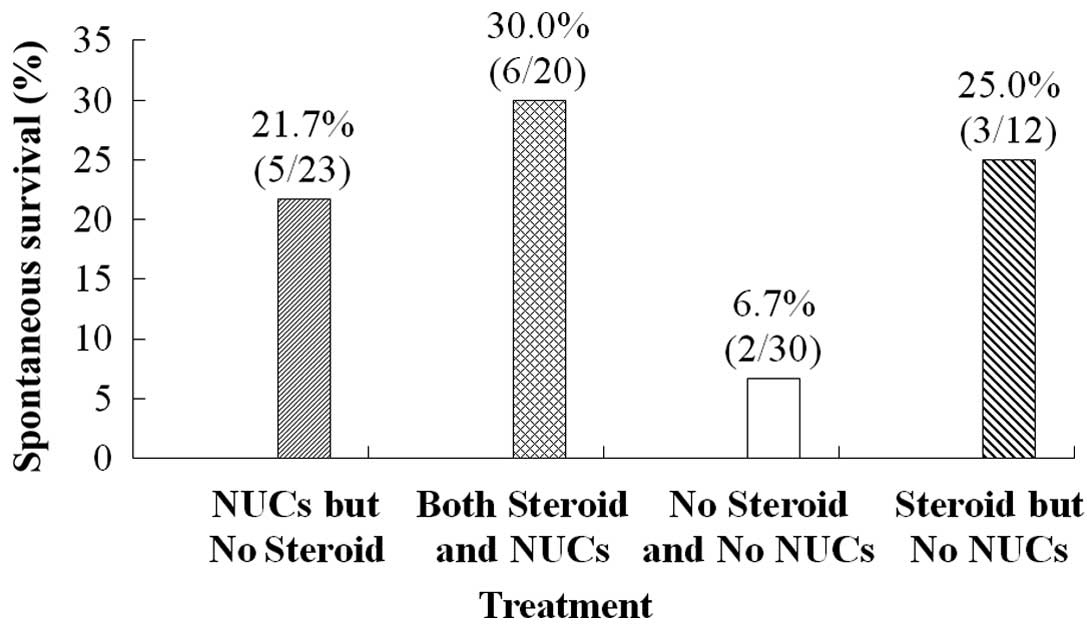
Effects of combined intervention with steroids and
NUCs on the prognosis following liver failure-associated with HBV.
In 85 patients with liver failure-associated with HBV, the SS rate
was higher in the steroid use group (28.13%; 9/32) than in the no
steroid use group (13.25%; 7/53), and also higher in the antiviral
group (25.58%; 11/43) than in the no antiviral group (11.90%;
5/42), but these were not significantly different (P=0.150, 0.102).
However, the SS rate was significantly higher in patients who
received combined intervention with steroids and NUCs compared to
patients who received neither steroid nor antiviral treatment with
NUCs (P=0.047) (Fig. 4).
Logistic regression to predict
spontaneous survival
Logistic regression was performed to identify
independent predictors of SS. The clinical type and etiologies of
liver failure were not predictive of SS in uni- or multivariate
models (Table IV). Steroid
treatment, age, onset of HE, MELD scores and ALT and AST levels
were significantly predictive of SS in uni- and multivariate
analyses (Table IV). Steroid
treatment was associated with increased SS rate in the univariate
analysis [odds ratio (OR), 3.912; P=0.013] and in the multivariate
analysis (OR, 4.241; P=0.007). Additionally, INR was significantly
predictive of SS in the univariate analysis (OR 0.553; P=0.034);
however, INR was not analyzed in the multivariate models along with
the MELD scores due to collinearity.
| Table IV.Univariate and multivariate analysis
for predicting spontaneous survival. |
Table IV.
Univariate and multivariate analysis
for predicting spontaneous survival.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | OR | P-value | OR | P-value |
|---|
| Steroid use | 3.912 | 0.013 | 4.241 | 0.007 |
| Age | 1.037 | 0.002 | 0.965 | 0.003 |
| Clinical type |
|
|
|
|
|
ALF | – | – | – | – |
|
SALF | 0.643 | 0.477 | 1.489 | 0.510 |
| Etiologies |
|
|
|
|
|
Viral | – | – | – | – |
|
Non-viral | 0.764 | 0.565 | 1.487 | 0.376 |
| HE |
|
|
|
|
| No | – | – | – | – |
|
Yes | 4.043 | 0.010 | 0.238 | 0.007 |
| MELD | 1.259 | <0.001 | 0.795 | <0.001 |
| INR | 0.553 | 0.034 | – | – |
| ALT | 0.999 | 0.004 | 1.001 | 0.004 |
| AST | 1.002 | 0.005 | 0.998 | 0.004 |
Discussion
In the present retrospective study, it was
demonstrated that the prognosis of patients with ALF and SALF was
poor; the SS rate was only 24.37%. Liver transplantation is a
valuable treatment to improve the prognosis following liver failure
(5,6,23).
However, it is nearly impossible for the majority of patients with
ALF to receive liver transplantation due to the financial burden
and lack of donor livers (24). NUC
is an etiology-specific treatment for hepatitis B-associated liver
failure (3). HBV DNA is reduced
rapidly following the administration of NUCs; however, the
improvement to liver function is delayed by a few weeks to a few
months. During this time, an excessive immune and inflammatory
reaction may continue and liver cell injury may progress (17). Thus, antiviral treatment with NUCs
cannot rapidly prevent disease progression and may only help to
improve the short-term SS rate of acute hepatitis B-associated
liver failure (25,26). The present work and other previous
studies have revealed that lamivudine did not reduce the short-term
mortality or risk of liver failure when treating patients with SAE
of chronic hepatitis B (15,17). The effect of artificial liver support
systems on survival following ALF has been more difficult to
determine (23). Whatever the
etiology and pathogenesis of ALF and SALF may be, persistently
severe and extensive inflammation in the liver has a key role in
inducing disease progression and poor outcomes of liver failure
(7,8). Treating ALF and SALF using
corticosteroids to inhibit excessive inflammation and prevent
cytolysis of extensive injured hepatocytes is a reasonable
treatment decision and may be an initial therapy. The present
results indicated that treatment with corticosteroids was able to
improve the SS rate in patients with ALF and SALF, and with viral
and non-viral liver failure. Using a multivariate analysis,
corticosteroid use was also identified to be an independent
predictor of an improved SS rate. These findings indicated that
intervention with corticosteroids was effective in preventing the
disease progression and improving the prognosis of ALF and SALF,
which was inconsistent with the results reported by Karkhanis et
al (20). The discrepancy in the
results in these two studies may be due to the different criteria
used to define SS. In the present study, SS was defined as survival
without transplantation until 24 weeks, whereas the Karkhanis et
al (20) study defined SS as
survival without transplantation for only 21 days. It is important
to note that many patients surviving to 3 weeks may succumb to
liver failure after 4–24 weeks. In the present study, the
difference in SS rate between the steroid use group and the no
steroid use group was significant until week 12. These results
indicated that it was not reasonable to evaluate the role of
corticosteroid treatment at 3 weeks upon SS rate in patients with
liver failure.
MELD scores and HE grades are key indicators of the
current disease severity and are associated with the prognosis of
liver failure (27). Extremely high
MELD scores or HE grade 4 are considered to be predictive of
end-stage liver failure and a particularly negative prognosis,
irrespective of therapy (27). The
present results demonstrated that irrespective of steroid use, SS
rate was extremely low for patients with MELD scores ≥35 and HE
grade 4. These findings confirmed that the extremely high MELD
scores and HE grade 4 were signs of end-stage liver failure. The
current results also indicated that SS rate was significantly
higher in the steroid use group than in the no steroid use group
for patients with MELD scores of 25–35 and for patients without HE
or with HE grades 1–3. This implies that corticosteroid treatment
was effective in improving the prognosis for patients with less
severe liver failure and ineffective for patients with progression
to end-stage liver failure.
The serum ALT levels may be a surrogate marker for
inflammation, and are markedly elevated during cell destruction
(20,28,29).
Decreased ALT levels during the advanced disease stage may indicate
regression of cell necrosis, marked parenchymal loss or
dysfunctional ALT synthesis (30). A
rapid drop in the initially elevated ALT levels is considered to be
an unfavorable prognostic sign. A significantly elevated ALT level
does not indicate that the current condition is serious, or that
the condition is end-stage liver failure; however, it predicts that
the patient has a markedly heightened risk of rapid disease
progression to end-stage liver failure (30). The present results revealed that SS
rate in patients not being administered steroids was significantly
higher among patients with ALT levels at 10–30x ULN than the SS in
patients with ALT levels <10x ULN. The current findings
indicated that a lower ALT level was an unfavorable prognostic sign
in ALF or SALF. The present results indicated that SS rate was
significantly higher in the steroid use group than in the no
steroid use group in patients with ALT levels ≥30x ULN, which
indicated that corticosteroid treatment was effective in improving
the prognosis of patients with potentially rapid disease
progression.
The currently investigated MELD scores, HE grades
and serum ALT levels were all associated with the effects of
corticosteroid treatment and prognosis of liver failure. The
multivariate analysis results demonstrated that the independent
predictors of SS also included MELD scores, HE grades and serum ALT
levels. Both the present illness severity and the potential risk of
disease progression should therefore be considered when assessing
the effect of corticosteroid treatment and the prognosis of liver
failure. In the present study, the patients with MELD scores ≥35 or
HE grade 4 had an extremely low SS rate in the steroid use group
and in the no steroid use group (11.8 vs. 2.2%). Amongst patients
with HE grades <4 and MELD scores <35 and ALT levels ≥30x
ULN, the SS rate in the steroid use group was up to 65.0% and was
significantly higher than the rate of 17.4% reported in the no
steroid use group. These results indicated that corticosteroid
treatment was effective in improving SS for patients with less
severe liver failure and a potential risk of rapid disease
progression. Although the current findings are inconsistent with
those reported in the Karkhanis et al (20) study; we have a similar hypothesis
that the contradictory results of corticosteroid use in treating
liver failure were associated with the selection bias of the study
patients. Unquestionably, severe liver failure is a possible
negative outcome following any treatment, including steroid use.
Corticosteroid treatment may therefore be used to improve SS in
patients with less severe liver failure, slower disease progression
and an increased capacity for liver regeneration, as these
conditions are all associated with an improved survival rate.
An extremely high ALT level indicates that a patient
has a potential risk of disease progression; however, it also
indicates that the patient has extensive hepatocyte degeneration
but not extensive hepatocyte necrosis, suggesting that the patient
is in the early stages of liver failure (20). When large numbers of degenerated
hepatocytes have already been destroyed, the introduction of
steroids may not be effective in improving the prognosis of liver
failure (17). Fujiwara et al
(17) reported that none of the
eight patients studied recovered when steroids were administered
>10 days after the diagnosis of SAE of chronic hepatitis B;
however, 88.2% (15/17) of the patients recovered when steroids were
administered within 10 days of an SAE diagnosis. The present
results revealed that the time interval from the onset of symptoms
to the initiation of steroid use was significantly shorter in
survivors than in non-survivors. The SS rate was significantly
higher in patients administered corticosteroids after ≤2 weeks than
in patients administered these after >2 weeks. This indicated
that the timing of introduction of corticosteroids was crucial to
attenuate the frequency of liver failure. The current study also
reported that the SS rate was 64% in patients with MELD scores
<35 and HE grades <4; however, the SS rate was only at 20% in
patients with MELD scores ≥35 or HE grade 4, amongst 35 patients
with early introduction of corticosteroids (time interval, ≤2
weeks). These results indicated that early intervention with
steroids was effective in improving the prognosis of patients with
less severe liver failure; these findings were similar to the
results reported by Fujiwara et al (21). Therefore, corticosteroids should be
introduced as early as possible for patients with less severe liver
failure.
Lisotti et al (31) reported that lamivudine treatment was
helpful in improving the prognosis of patients with severe acute
HBV-associated hepatitis. Fujiwara et al (17) reported that a combined therapy of
NUCs and corticosteroids was unable to improve the recovery rates
of patients with SAE of chronic hepatitis B, but shortened the
treatment period of corticosteroids. The current results indicated
that the SS rate in patients receiving neither steroids nor NUCs
was significantly lower than that of patients who received a
combined treatment of NUC and corticosteroids. These findings
indicated that a combined treatment of NUC and corticosteroids was
able to improve the prognosis of acute hepatitis B liver
failure.
In conclusion, the present study, based on 13 years
of clinical data, demonstrated that corticosteroid use was able to
improve the SS rate in patients with ALF and SALF, irrespective of
their etiologies. The efficacy of corticosteroid treatment was
primarily associated with the disease severity and timing of
steroid administration. The patients responding best to
corticosteroids were those with less severe liver failure, and a
higher risk of rapid disease progression, with lower MELD scores
and HE grades but extremely high ALT levels. The optimal time of
intervention with corticosteroids was within 14 days of the onset
of symptoms. Patients with acute hepatitis B liver failure
benefited from a combined treatment of NUC and corticosteroid.
Acknowledgements
The present work was supported by a grant from the
Chinese National Natural Science Foundation project (grant no.
81270525). Thanks are given to the authors' colleagues at the
Department of Infectious Diseases, Southwest Hospital who cared for
the patients in this study, and particularly Jing Peng, Wei Sun, Ji
Wu and Yan Zhu for assisting with the index of cases and the
collection of clinical data.
Glossary
Abbreviations
Abbreviations:
|
ACLF
|
acute-on-chronic liver failure
|
|
ALF
|
acute liver failure
|
|
ALT
|
alanine aminotransferase
|
|
AST
|
aspartate aminotransferase
|
|
Dex
|
dexamethasone
|
|
HAV
|
hepatitis A virus
|
|
HBV
|
hepatitis B virus
|
|
HE
|
hepatic encephalopathy
|
|
HEV
|
hepatitis E virus
|
|
INR
|
international normalized ratio
|
|
MELD
|
model for end-stage liver disease
|
|
NUCs
|
nucleo(s/t)ide analogues
|
|
PTA
|
prothrombin activity
|
|
SALF
|
subacute liver failure
|
|
SS
|
spontaneous survival
|
|
T-Bil
|
total bilirubin.
|
References
|
1
|
Wlodzimirow KA, Eslami S, Abu-Hanna A,
Nieuwoudt M and Chamuleau RA: Systematic review: Acute liver
failure-one disease, more than 40 definitions. Aliment Pharmacol
Ther. 35:1245–1256. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Polson J and Lee WM: AASLD position paper:
The management of acute liver failure. Hepatology. 41:1179–1197.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Liver, Failure and Artificial Liver Group,
. CSoID and Severe Liver and Disease and Artificial Liver Group,
CSoH: Guideline for diagnosis and treatment of liver failure. Zhong
Hua Lin Chuang Gan Ran Bing Za Zhi. 5:321–327. 2012.(In
Chinese).
|
|
4
|
Ke WM, Li XJ, Yu LN, Lai J, Li XH, Gao ZL
and Chen PJ: Etiological investigation of fatal liver failure
during the course of chronic hepatitis B in southeast China. J
Gastroenterol. 41:347–351. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bernal W, Auzinger G, Dhawan A and Wendon
J: Acute liver failure. Lancet. 376:190–201. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Patton H, Misel M and Gish RG: Acute liver
failure in adults: An evidence-based management protocol for
clinicians. Gastroenterol Hepatol (NY). 8:161–212. 2012.
|
|
7
|
Wu Z, Han M, Chen T, Yan W and Ning Q:
Acute liver failure: Mechanisms of immune-mediated liver injury.
Liver Int. 30:782–794. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Malhi H and Gores GJ: Cellular and
molecular mechanisms of liver injury. Gastroenterology.
134:1641–1654. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Weng HL, Cai X, Yuan X, Liebe R, Dooley S,
Li H and Wang TL: Two sides of one coin: massive hepatic necrosis
and progenitor cell-mediated regeneration in acute liver failure.
Front Physiol. 6:1782015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Higuchi N, Kato M, Kotoh K, Kohjima M,
Aishima S, Nakamuta M, Fukui Y, Takayanagi R and Enjoji M:
Methylprednisolone injection via the portal vein suppresses
inflammation in acute liver failure induced in rats by
lipopolysaccharide and d-galactosamine. Liver Int. 27:1342–1348.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lu YS, Pu LY, Li XC and Wang XH:
Methylprednisolone inhibits activated CD4+ T cell survival promoted
by toll-like receptor ligands. Hepatobiliary Pancreat Dis Int.
9:376–383. 2010.PubMed/NCBI
|
|
12
|
Dich J, Vind C and Grunnet N: Long-term
culture of hepatocytes: Effect of hormones on enzyme activities and
metabolic capacity. Hepatology. 8:39–45. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Oh HY, Namkoong S, Lee SJ, Por E, Kim CK,
Billiar TR, Han JA, Ha KS, Chung HT, Kwon YG, et al: Dexamethasone
protects primary cultured hepatocytes from death receptor-mediated
apoptosis by upregulation of cFLIP. Cell Death Differ. 13:512–523.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ferrigno A, Gregotti C, Richelmi P and
Vairetti M: Dexamethasone protects cultured rat hepatocytes against
cadmium toxicity: Involvement of cellular thiols. In Vitro Cell Dev
Biol Anim. 46:445–449. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang XQ, Jiang L, You JP, Liu YY, Peng J,
Zhang HY, Xu BY and Mao Q: Efficacy of short-term dexamethasone
therapy in acute-on-chronic pre-liver failure. Hepatol Res.
41:46–53. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mao Q, Zhang HY, You JP and Zhang XQ:
Severe acute exacerbation of chronic hepatitis B during pegylated
interferon treatment and early intervention with corticosteroid.
Virol J. 9:1362012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fujiwara K, Yasui S, Yonemitsu Y, Fukai K,
Arai M, Imazeki F, Suzuki A, Suzuki H, Sadahiro T, Oda S and
Yokosuka O: Efficacy of combination therapy of antiviral and
immunosuppressive drugs for the treatment of severe acute
exacerbation of chronic hepatitis B. J Gastroenterol. 43:711–719.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yamada K, Yamamoto Y, Uchiyama A, Ito R,
Aoki Y, Uchida Y, Nagasawa H, Kimura H, Ichiyama T, Fukao T and
Kohno Y: Successful treatment of neonatal herpes simplex-type 1
infection complicated by hemophagocytic lymphohistiocytosis and
acute liver failure. Tohoku J Exp Med. 214:1–5. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Czaja AJ: Corticosteroids or not in severe
acute or fulminant autoimmune hepatitis: Therapeutic brinksmanship
and the point beyond salvation. Liver Transpl. 13:953–955. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Karkhanis J, Verna EC, Chang MS, Stravitz
RT, Schilsky M, Lee WM and Brown RS Jr: Steroid use in acute liver
failure. Hepatology. 59:612–621. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fujiwara K, Yasui S, Yonemitsu Y, Mikata
R, Arai M, Kanda T, Imazeki F, Oda S and Yokosuka O: Efficacy of
high-dose corticosteroid in the early stage of viral acute liver
failure. Hepatol Res. 44:491–501. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Blei AT and Cordoba J: Hepatic
Encephalopathy. Am J Gastroenterol. 96:1968–1976. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang DW, Yin YM and Yao YM: Advances in
the management of acute liver failure. World J Gastroenterol.
19:7069–7077. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lu H, Lu L, Zhang F, Zhai Y and Wang X:
Living donor liver transplantation: where do we stand and where are
we going? Hepatobiliary Surg Nutr. 5:141–144. 2016.PubMed/NCBI
|
|
25
|
Yu S, Jianqin H, Wei W, Jianrong H, Yida
Y, Jifang S, Liang Y, Zhi C and Hongyu J: The efficacy and safety
of nucleos(t)ide analogues in the treatment of HBV-related
acute-on-chronic liver failure: a meta-analysis. Ann Hepatol.
12:364–372. 2013.PubMed/NCBI
|
|
26
|
Kumar M, Satapathy S, Monga R, Das K,
Hissar S, Pande C, Sharma BC and Sarin SK: A randomized controlled
trial of lamivudine to treat acute hepatitis B. Hepatology.
45:97–101. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Du WB, Pan XP and Li LJ: Prognostic models
for acute liver failure. Hepatobiliary Pancreat Dis Int. 9:122–128.
2010.PubMed/NCBI
|
|
28
|
Canbay A, Chen SY, Gieseler RK, Malago M,
Karliova M, Gerken G, Broelsch CE and Treichel U: Overweight
patients are more susceptible for acute liver failure.
Hepatogastroenterology. 52:1516–1520. 2005.PubMed/NCBI
|
|
29
|
Rueff B and Benhamou JP: Acute hepatic
necrosis and fulminant hepatic failure. Gut. 14:805–815. 1973.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wong VW and Chan HL: Severe acute
exacerbation of chronic hepatitis B: A unique presentation of a
common disease. J Gastroenterol Hepatol. 24:1179–1186. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lisotti A, Azzaroli F, Buonfiglioli F,
Montagnani M, Alessandrelli F and Mazzella G: Lamivudine treatment
for severe acute HBV hepatitis. Int J Med Sci. 5:309–312. 2008.
View Article : Google Scholar : PubMed/NCBI
|