Introduction
Spontaneous intracranial artery dissection is an
uncommon cause of stroke; however, it is a notable cause of stroke
in young and middle-aged adults. The proportion of intracranial
artery dissection in cervicocephalic dissection varies between
ethnic origin (1). For example, it
was reported that only 11% of cervicocephalic artery dissection
occurs in the intracranial arteries of Europeans, compared with
67–78% in East Asians (2,3). The majority of cases of intracranial
artery dissection affect the vertebrobasilar system (3–5). This
condition occurs relatively rarely in the anterior circulation,
particularly in the anterior cerebral artery (ACA) (5–7).
Previous studies have suggested that only 5.8–7.7% of cases of
intracranial artery dissection occur in the ACA (4,5), and ACA
dissection commonly affects middle-aged patients (7). Although intracranial artery dissection
usually presents with subarachnoid hemorrhage (SAH) or cerebral
infarction (7,8). The concurrent presence of SAH and
cerebral infarction in patients with intracranial artery dissection
is rare (8,9). In the present study, a rare case of SAH
concomitant with acute ischemic stroke (AIS) in the territory of
the ACA due to ACA dissection is described. The symptoms and
angiography of the patient got improved with only conservative
treatment.
Case report
The patient, a 57-year-old woman with a 10-year
history of hypertension, was transferred to the Emergency
Department of Zhejiang Provincial People's Hospital (People's
Hospital of Hangzhou Medical College, Hangzhou, China) in May 2014.
She presented with sudden-onset left hemiparesis with urinary
incontinence, and a prodromal right temporal headache. Her blood
pressure was 199/115 mmHg on admission. Neurological examination
revealed left facial palsy, with muscle power rated as 4 on a scale
from 0 to 5 in the left upper extremity and 0 in the left lower
extremity, as follows: 0, no contraction; 1, flicker or trace of
contraction; 2, active movement with gravity eliminated; 3, active
movement against gravity; 4, active movement against gravity and
resistance; and 5, normal power. The National Institutes of Health
Stroke Scale (NIHSS) score was 7, and the modified Rankin Scale
(mRS) score was 5.
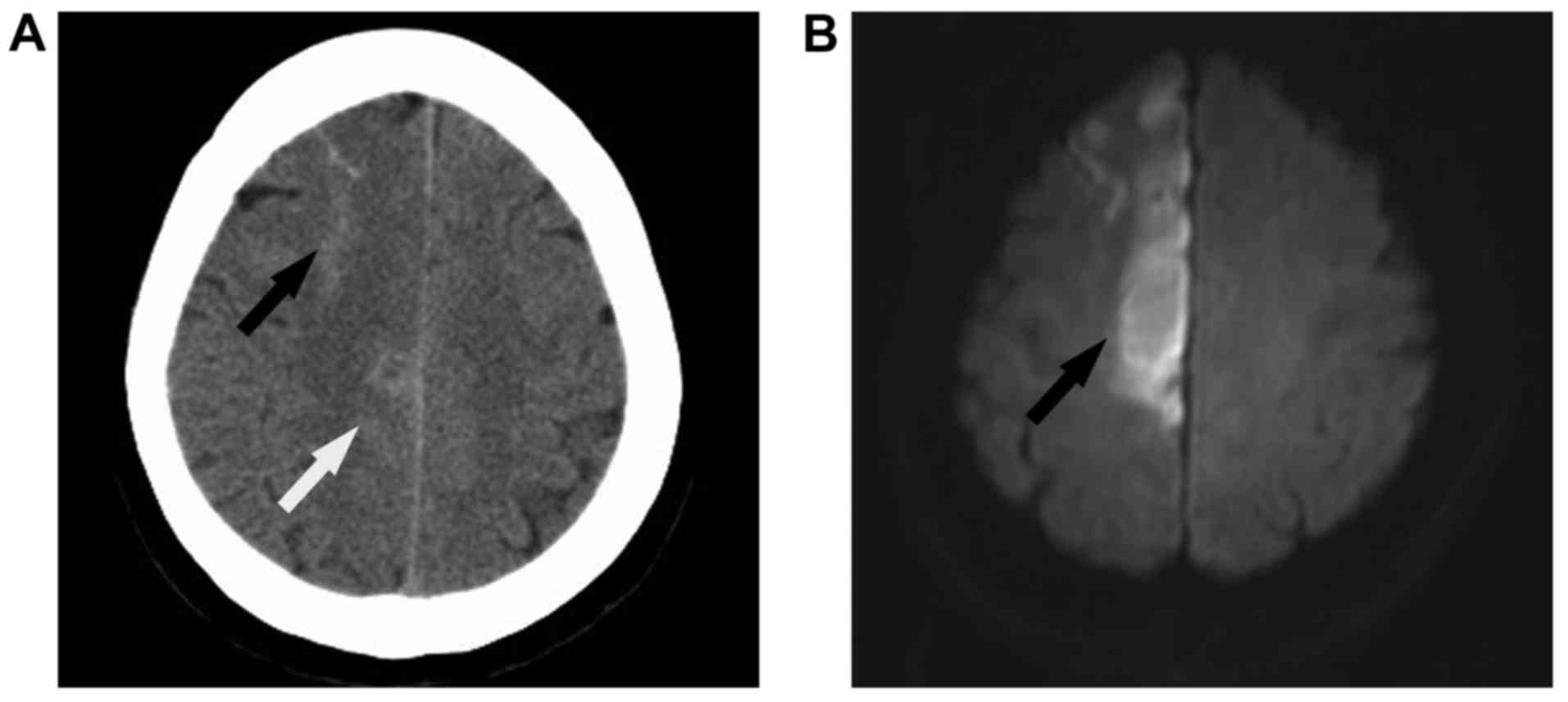
A computed tomography (CT) scan of the brain
revealed a high-density lesion within the right superior frontal
sulcus and right interhemispheric fissure (Fig. 1A). Brain magnetic resonance imaging
(MRI) conducted 2 days later demonstrated an acute infarct in the
territory of the right ACA (Fig.
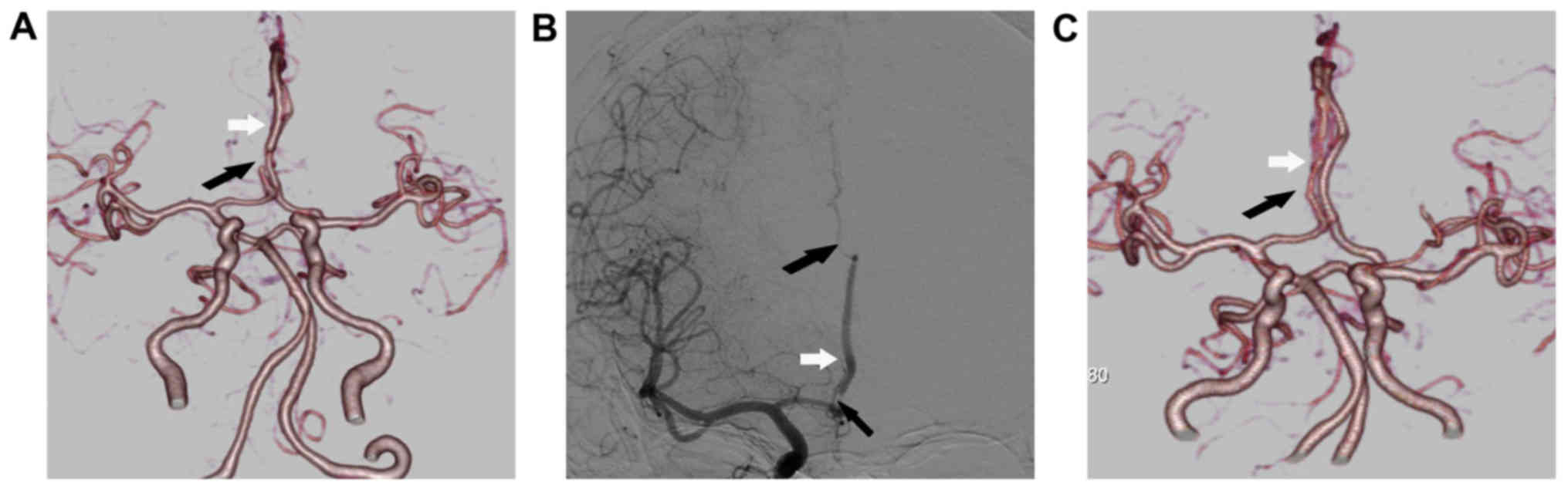
1B). CT angiography on day 5 and brain digital subtraction
angiography on day 6 showed severe stenosis at the origin of the A2
segment with distal dilatation and occlusion at the origin of the
A3 segment of the right ACA (Fig. 2A and
B, respectively), suggesting a diagnosis of ACA dissection.
Treatment with atorvastatin (Pfizer, Inc., New York,
NY, USA) at a dose of 20 mg/day was prescribed to the patient.
Following stabilization of her condition, the patient was returned
to her local hospital and rehabilitation, which included muscle
strength enhancement training and motion range training, was
initiated. A follow-up CT angiography performed 5 months after
onset demonstrated that the stenosis and dilatation of the A2
segment was much ameliorated (Fig.
2C). The previous diagnosis of ACA dissection was confirmed by
the rapid change observed in the repeat angiography. The NIHSS
score of the patient was improved to 3 and the mRS score was
improved to 3 at the 5-month follow-up.
Discussion
Simultaneous hemorrhage and ischemia due to ACA
dissection appears to be very rare. To the best of our knowledge,
only 14 cases of simultaneous hemorrhage and ischemia caused by ACA
dissection have been reported so far (7,9,10–17). The
age range of the individuals affected is from 35 to 64 years. All
of these cases presented with lower-extremity dominant hemiparesis
and some of them also complained of sudden onset headache. The SAH
was located in the interhemispheric fissure or frontal surface in
all cases (12–16). The patient in the present case was a
middle-aged woman with a 10-year history of hypertension. As two
typical clinical features observed in previous cases, sudden onset
headache and lower-extremity dominant hemiparesis were present on
admission in the present case. A CT scan of the current case
revealed SAH within the right superior frontal sulcus and right
interhemispheric fissure where SAH was often located in similar
patients from previous reports. Notably, all previous reports
describe patients from Japan and Korea and none of the patients
affected are from western countries. A case involving ssimultaneous
hemorrhage and ischemia due to ACA dissection has never been
reported in China before and the present case is the first such
report.
Diagnosis of ACA dissection can be challenging. The
pathognomonic radiological findings of artery dissection are double
lumen, mural hematoma and intimal flap (18). However, in view of the small size of
the ACA, it is not possible to observe these typical radiological
findings in all patients with ACA dissection. It has been reported
that intracranial artery dissection can present with aneurysmal
dilatation, segmental stenosis or occlusion (19). It is worthy of note that fusiform or
irregular aneurysmal dilation at a non-branching site is very
suggestive of intracranial artery dissection if it is associated
with a segmental stenosis. If those radiological findings rapidly
change on repeated imaging, for example, by an increase or
reduction in artery size, or the appearance of aneurysmal dilation,
the diagnosis of intracranial artery dissection can be confirmed
(1). Such serial changes on
follow-up angiograms were considered to be the most characteristic
angiographic findings in a patient with ACA dissection in a
previous report (7). In the present
case, segmental stenosis and fusiform aneurysmal dilation in the A2
segment and occlusion in the A3 segment of right ACA were
identified. A follow-up CT angiography conducted 5 months after
onset demonstrated that the stenosis in the A2 segment resolved and
dilatation in the A2 segment disappeared. The patient was confirmed
as a case of ACA dissection using those characteristic radiological
features. Therefore, in cases in which a diagnosis cannot be
confirmed in the acute stage, a follow-up angiogram is very
important as it may help with making the diagnosis.
Although artery dissection is an important cause of
SAH concomitant with AIS, previous reports indicate these
concurrent conditions may also occur in association with reversible
cerebral vasoconstriction syndrome (RCVS), cerebral amyloid
angiopathy (CAA) and cerebral artery atherosclerotic stenosis
(20–22). SAH usually affects the convexities of
the brain and is distant from the location of narrowing arteries in
the RCVS. Watershed infarcts rather than territorial infarcts often
coexist with SAH in RCVS (21). In
the present case, SAH was not only located in the convexities of
the brain but also in the right interhemispheric fissure. Brain MRI
demonstrated an acute infarct in the territory of the right ACA
near to the segment of the narrowing artery rather than in the
watershed area. Thus, the diagnosis of RCVS was excluded by those
imaging features. In 2014, Nakajima et al (19) suggested a diagnosis of CAA in two
patients presenting with SAH accompanied with AIS concomitantly.
However, none of the patients with CAA showed stenosis and
dilatation of the cerebral artery. Thus, the diagnosis of CAA was
not considered in the present case. Cerebral artery atherosclerotic
stenosis has been reported as another cause of SAH concomitant with
AIS (22,23). The exact mechanism by which cerebral
artery atherosclerotic stenosis causes SAH is unknown. Rupture of
the leptomeningeal collaterals could be the possible mechanism for
SAH exclusively localized in the convexities of the brain in all
the patients with cerebral artery atherosclerotic stenosis.
However, in the present case, SAH was located in the convexities of
the brain and also in the right interhemispheric fissure. The
possible mechanism of SAH in this case maybe the direct rupture of
the artery dissection. Furthermore, the rapid change of segment
stenosis and dilation on repeated imaging that was observed in the
present case would not occur in a patient with cerebral artery
atherosclerotic stenosis. Therefore, the diagnosis of cerebral
artery atherosclerotic stenosis was also excluded in this case.
The appropriate treatment of simultaneous hemorrhage
and AIS due to ACA dissection remains controversial. It has been
suggested that patients with intracranial artery dissection and SAH
should be treated with surgical or endovascular procedures because
of the high incidence of rebleeding (20). Medical treatment, such as with
anticoagulant or antiplatelet agents, has been suggested for
patients with intracranial artery dissection without SAH (20). However, in the 15 cases of ACA
dissection with SAH and ischemia (which includes the present case),
only 6 cases underwent surgical or endovascular procedures and all
of them showed evident dissection aneurysm (7–9,12,16,17). In
addition, 6 cases, including the present case, received only
conservative treatment without antithrombotic therapy §1,13–16).
All of them experienced a good recovery and none of them suffered
from rebleeding or further ischemia. In the present case, the
patient's NIHSS score was improved to 3 and mRS score was improved
from 5 to 3 at 5 months after onset following conservative
treatment. The follow-up CT angiography showed clear improvements
in the stenosis and dilatation in the A2 segment, which provides
angiographic confirmation of the effectiveness of conservative
treatment for the first time. Therefore, SAH concomitant with AIS
due to ACA dissection maybe a somewhat benign type of SAH.
Conservative treatment without antithrombotic therapy maybe a safe
and effective choice in patients with SAH concomitant with AIS due
to ACA dissection.
In conclusion, simultaneous hemorrhage and ischemia
due to ACA dissection is very rare and, to the best of our
knowledge, the present case is the first to be reported in China.
Conservative treatment without antithrombotic therapy maybe a safe
and effective choice in patients with SAH concomitant with ischemia
due to ACA dissection.
Glossary
Abbreviations
Abbreviations:
|
SAH
|
subarachnoid hemorrhage
|
|
AIS
|
acute ischemic stroke
|
|
ACA
|
anterior cerebral artery
|
|
NIHSS
|
National Institutes of Health Stroke
Scale
|
|
mRS
|
modified Rankin Scale
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
RCVS
|
reversible cerebral vasoconstriction
syndrome
|
|
CAA
|
cerebral amyloid angiopathy
|
References
|
1
|
Kwak JH, Choi JW, Park HJ, Chae EY, Park
ES, Lee DH and Suh DC: Cerebral artery dissection: Spectrum of
clinical presentations related to angiographic findings.
Neurointervention. 6:78–83. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Huang YC, Chen YF, Wang YH, Tu YK, Jeng JS
and Liu HM: Cervicocranial arterial dissection: Experience of 73
patients in a single center. Surg Neurol. 72 Suppl 2:S20–S27. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mizutani T: Natural course of intracranial
arterial dissections. J Neurosurg. 114:1037–1044. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ono H, Nakatomi H, Tsutsumi K, Inoue T,
Teraoka A, Yoshimoto Y, Ide T, Kitanaka C, Ueki K, Imai H and Saito
N: Symptomatic recurrence of intracranial arterial dissections:
Follow-up study of 143 consecutive cases and pathological
investigation. Stroke. 44:126–131. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Guridi J, Gállego J, Monzón F and Aguilera
F: Intracerebral hemorrhage caused by transmural dissection of the
anterior cerebral artery. Stroke. 24:1400–1402. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ohkuma H, Suzuki S, Kikkawa T and
Shimamura N: Neuroradiologic and clinical features of arterical
dissection of the anterior cerebral artery. AJNR Am J Neuroradiol.
24:691–699. 2003.PubMed/NCBI
|
|
7
|
Suzuki I, Nishino A, Nishimura S, Numagami
Y, Suzuki H, Utsunomiya A, Suzuki S, Uenohara H and Sakurai Y:
Nontraumatic arterial dissection of the anterior cerebral artery:
six cases report. No To Shinkei. 57:509–515. 2005.(In Japanese).
PubMed/NCBI
|
|
8
|
Inoue T, Fujimura M, Mastsumoto Y, Kondo
R, Inoue T, Shimizu H and Tominaga T: Simultaneous occurrence of
subarachnoid hemorrhage and cerebral infarction caused by anterior
cerebral artery dissection treated by endovascular trapping. Neurol
Med Chir (Tokyo). 50:574–577. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yasukama K, Kamijo Y, Momose G, Kobayashi
S and Ikeda A: A case of anterior cerebral artery dissecting
aneurysm presenting subarachnoid hemorrhage and cerebral infarction
at the same time. Surg Cerebral Stroke. 21:461–466. 1993.
View Article : Google Scholar
|
|
10
|
Kato N, Yamada Y, Hyodo A and Nose T: A
case of anterior cerebral artery dissection presenting subarachnoid
hemorrhage and cerebral infarction. No Shinkei Geka J. 9:157–161.
2000.(In Japanese).
|
|
11
|
Miyahara K, Sakata K, Gondo G, Kanno H and
Yamamoto I: Spontaneous dissection of the anterior cerebral artery
presenting subarachnoid hemorrhage and cerebral infarction: A case
report. No Shinkei Geka. 29:335–339. 2001.(In Japanese). PubMed/NCBI
|
|
12
|
Kimura S, Igarashi T, Kotani A and
Katayama Y: Nontraumatic arterial dissection of the anterior
cerebral artery with simultaneous cerebral infarction and
subarachnoid hemorrhage: A case report. No Shinkei Geka.
38:273–278. 2010.(In Japanese). PubMed/NCBI
|
|
13
|
Suzuki K, Mishina M, Okubo S, Abe A, Suda
S, Ueda M and Katayama Y: Anterior cerebral artery dissection
presenting subrarachnoid hemorrhage and cerebral infarction. J
Nippon Med Sch. 79:153–158. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nanbara S, Tsutsumi K, Takahata H,
Fujimoto T, Kawahara I, Ono T, Toda K, Baba H and Yonekura M:
Spontaneous dissection of the anterior cerebral artery that
simultaneously presented with cerebral infarction and subarachnoid
hemorrhage, successfully treated with conservative management: A
case report. No Shinkei Geka. 40:635–642. 2012.(In Japanese).
PubMed/NCBI
|
|
15
|
Im TS, Lee YS, Suh SJ, Lee JH, Ryu KY and
Kang DG: Two cases of subarachnoid hemorrhage from spontaneous
anterior cerebral artery dissection: A case of simultaneous
hemorrhage and ischemia without aneurysmal formation and another
case of hemorrhage with aneurysmal formation. J Cerebrovasc
Endovasc Neurosurg. 16:119–124. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kato Y, Hayashi T, Uchino A, Kakehi Y,
Yamane F, Ishihara S and Tanahashi N: Fusiform dilatation of the
outer contour of a dissected anterior cerebral artery revealed by
magnetic resonance cisternography in a patient with simultaneous
cerebral infarction and subarachnoid hemorrhage. J Stroke
Cerebrovasc Dis. 23:1717–1720. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Han M, Rim NJ, Lee JS, Kim SY and Choi JW:
Feasibility of high-resolution MR imaging for the diagnosis of
intracranial vertebrobasilar artery dissection. Eur Radiol.
24:3017–3024. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ahn SS, Kim BM, Suh SH, Kim DJ, Kim DI,
Shin YS, Ha SY and Kwon YS: Spontaneous symptomatic intracranial
vertebrobasilar dissection: Initial and follow-up imaging findings.
Radiology. 264:196–202. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nakajima M, Inatomi Y, Yonehara T, Hirano
T and Ando Y: Nontraumatic convexal subarachnoid hemorrhage
concomitant with acute ischemic stroke. J Stroke Cerebrovasc Dis.
23:1564–1570. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Singhal AB, Hajj-Ali RA, Topcuoglu MA, Fok
J, Bena J, Yang D and Calabrese LH: Reversible cerebral
vasoconstriction syndromes: Analysis of 139 cases. Arch Neurol.
68:1005–1012. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kleinig TJ, Kimber TE and Thompson PD:
Convexity subarachnoid haemorrhage associated with bilateral
internal carotid artery stenosis. J Neurol. 256:669–671. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Debette S, Compter A, Labeyrie MA,
Uyttenboogaart M, Metso TM, Majersik JJ, Goeggel-Simonetti B,
Engelter ST, Pezzini A, Bijlenga P, et al: Epidemiology,
pathophysiology, diagnosis, and management of intracranial artery
dissection. Lancet Neurol. 14:640–654. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Geraldes R, Sousa PR, Fonseca AC, Falcão
F, Canhão P and e Melo T Pinho: Nontraumatic convexity subarachnoid
hemorrhage: Different etiologies and outcomes. J Stroke Cerebrovasc
Dis. 13:e23–e30. 2014. View Article : Google Scholar
|