Introduction
The lower urinary tract consists of the bladder and
the urethra. Generally, the male urethra is 16–22 cm in length,
with an average inner diameter of 5–7 mm, while the female urethra
is 3–5 cm long, with an inner diameter of ~6 mm (1). Conventional radiography, such as
retrograde and excretory urethrography, has been used for a century
as the standard imaging technique in conventional research on the
morphology and function of the lower urinary tract (2,3). Under
certain circumstances, other imaging techniques, including
ultrasound and magnetic resonance imaging (MRI) may be conducive to
the diagnosis of the lower urinary tract diseases (4,5).
However, methods including excretory urography, retrograde
urography and contrast urography have a number of defects,
including the use of an invasive procedure or a lack of
quantitative indicators (6,7). Therefore, quantitative evaluation of
the anatomical form, such as the dynamic contraction of the bladder
and urethra during urination, may not be conducted thoroughly.
Computed tomography (CT) using a multi-row detector
(for example, 64-row multi-slice spiral CT) enables fast image
capture and the generation of 2-dimensional (2D) and 3D
reconstructed images via computer post-processing, and this
relatively novel diagnostic technique has been used to evaluate
lesions of the lower urinary tract (8–10). As
the most recent CT technique, 640-slice dynamic volume CT (DVCT)
has excellent spatial and temporal resolution, a wide capture range
and a fast data acquisition system, with volume capture that
provides 3D and 4D reconstructions of the region of interest.
The aim of the present study was to investigate the
application of 640-slice DVCT to the lower urinary tract during
urination, and provide a novel means for the quantitative
examination of organic or functional lesions of the lower urinary
tract.
Patients and methods
Patients
In this study, 70 healthy subjects admitted to The
Second People's Hospital of Yunnan Province (Kunming, China) from
September 2012 to June 2016 were included, with 43 males, aged
50.91±12.87 years, and 27 females, aged 49.76±11.08 years. Certain
exclusion criteria were applied: Given the potential harm caused by
radiation, healthy subjects (men and women) who had future
fertility plans were excluded, and so the subjects in this study
were predominantly middle aged and elderly. In addition, patients
with a history of diseases of the bladder and the genitourinary
system were also excluded.
Prior to the examination, all subjects were informed
of the entire scanning approach, the significance of the study, and
the risks associated with the exposure to X-rays, confirmed no
iodine allergies, and provided written informed consent. The study
was approved by the hospital ethics committee of The Second
People's Hospital of Yunnan Province.
Examination methods, scanning conditions,
and image generation using 640-slice DVCT
Preparation prior to examination
All subjects were asked to urinate and to self-test
the duration of urination. A high-pressure injector was used to
rapidly inject 50 ml iopamidol (Iopamiro; Bracco Imaging S.p.A.,
Milan, Italy; 370 mgI/ml; 18.5 g iodine) via a cubital vein
catheter. Subjects were asked to not to urinate until their bladder
was sufficiently full (when they felt a strong urge to urinate),
and to lie on the examination bed. A urinal bottle was attached to
the distal end of the penis of each male subject, while a urinal
bowl was placed under the buttocks of each female subject.
Examination method and scanning
conditions
In the supine, lateral or semi-sitting position,
with feet forward, double orientation (coronal and sagittal)
scanning was performed as the patient breathed calmly, using a CT
scanner (Aquilion One TSX-301A; Toshiba Corporation, Tokyo Japan).
The upper bound of the single field of view included the upper edge
of the bladder, limited by the detector's maximum width of 16 cm,
and the lower bound included the male posterior urethra and a part
of the anterior urethra, as well as the full length of the female
urethra. The Dy-Volume capture mode was employed, with a capture
thickness of 0.5 mm and an interval of 5–10 sec. For patients with
a self-tested duration of urination ≤60 sec, an interval of 5 sec
was used for data capture, while for that >60 sec, an interval
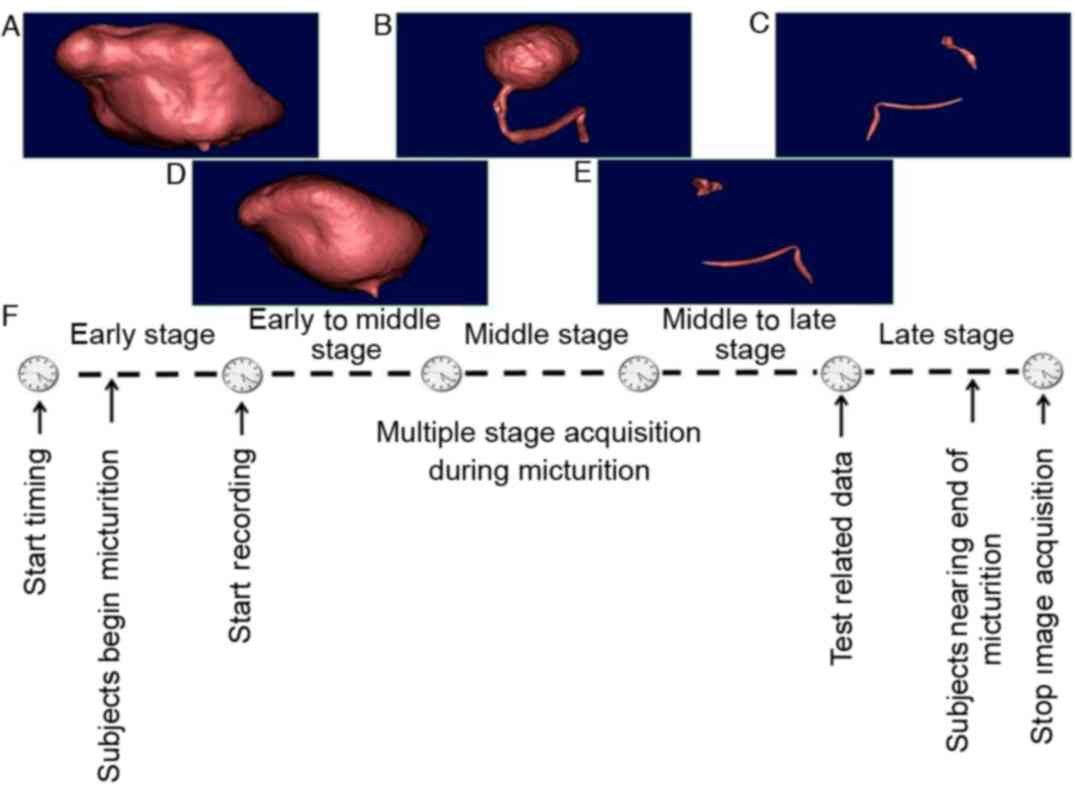
of 10 sec was used. All the subjects continued to urinate. The
scanning was stopped at the end of urination. The detailed
detection method and settings used for 640-slice DVCT were as
described in the manufacturer's instructions. The scanning process
of excretory cystography and urethrography using 640-slice DVCT is
shown in Fig. 1.
Image generation and
post-processing
The volume data of all phases were imported into a
Vitrea post-processing workstation (VPMC-13204 B; Vital Images,
Inc., Minnetonka, MN, USA). The 3D images of the lower urinary
tract were marked by threshold selection, to produce the
multiplanar reconstruction (MPR) and 3D volume images. MPR is able
to provide the sections from any angle, and 3D volume images are
able to display the target structure in 3D from various directions.
The continuous playback of whole-phase MPR enabled dynamic 2D
analysis of the bladder excretion to be performed, and 4D motion
images of the lower urinary tract were obtained by the continuous
playback of 3D images.
Volume CT dose index (CTDIvol) and
dose length product (DLP)
According to the initial diagnostic reference level
for adult CT perfusion (CTP) scanning specified in this study (the
reference value of effective absorbed dose was set as 19.8 mSV used
in abdominal CTP), the recommended dose for routine pelvic CT
examination is a CTDIvol of 35 mGy and DLP of 780 mGy.cm, with an
effective dose of 11.7 mSv. In the present study, during the
process of urination, an average of 10 sets of images were
captured. The mean CTDIvol was 27.4 mGy and the mean DLP was 439
mGy.cm, with an effective dose of 6.585 mSv. The effective dose
when ≤15 sets were captured was 9.8775 mSv, which was in line with
International Commission on Radiological Protection requirements
(11).
Examination using conventional CT
For comparison, SOMATOM Sensation 16 CT (Siemens AG,
Munich, Germany) was used to scan the bladder with the same methods
as Aquilion One, as described above. The matrix was set to 512×512,
the voltage was 100 kV and current was set to 100 mA.
Urination phase division and urine
volume detection
The beginning and end of the movement of each
structure (the bladder, female urethra and the proximal male
urethra) were recorded. For quantitative measurement, the urination
process was equally divided into the early, early to middle,
middle, middle to late, and late voiding phases chronologically,
and the urine volume and urine flow rate of each phase were
measured. Following urination, the urine was collected and the
urine volumes were recorded using a measuring cylinder.
Observation of the status of the male
posterior urethra and female urethra
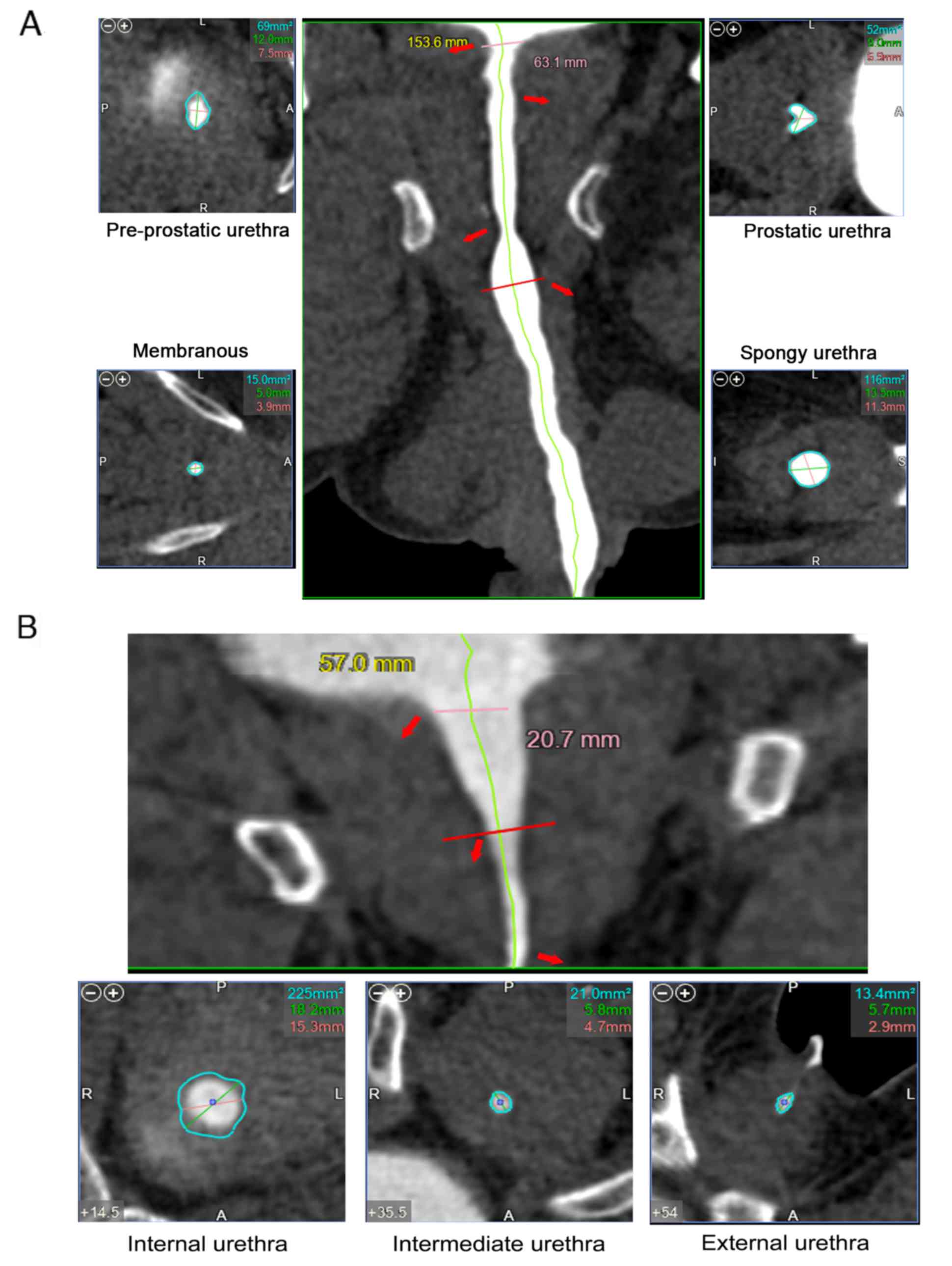
The curved multiplanar reconstruction technique
(12) was employed to mark the male
posterior urethra and a part of the anterior urethra, as well as
the female urethra. For the male urethra, the maximum diameter and
the cross-sectional area of the pre-prostatic (internal urethral
orifice), the prostatic (verumontanum), the membranous and the
spongy urethra were measured, respectively (Fig. 2A). For the female urethra, the
maximum diameter and cross-sectional area of the internal,
intermediate and external urethral orifices were measured,
respectively (Fig. 2B). Among the
different scan phases, it was possible for certain phases to show
the absence of filling with the urethral contrast agent. In such
cases, two deputy chief physicians jointly confirmed and selected a
phase with the most evident filling of urethral contrast agent for
measurement. All measured data of the lower urinary tract were
statistically compared.
Statistical analysis
The data obtained in this study were presented as
bar chart or line charts. Student's t-tests were used for
statistical analysis on SPSS 18.0 software (SPSS, Inc., Chicago,
IL, USA). The average value of each set was the result from three
independent experiments, shown as the mean ± standard deviation.
P<0.05 was considered to indicate a statistically significant
result.
Results
The application of 640-slice DVCT
increases the accuracy of detection of the bladder urine
volume
No significant difference was observed between the
total bladder urine volume of the 43 normal males determined by
DVCT (344.28±182.29 ml) and the actual urine volumes (351.79±178.36
ml) (P>0.05). In addition, no statistically significant
difference was identified between the total bladder urine volume of
the 27 normal females determined by DVCT (355.76±232.56 ml) and the
actual urine volumes (342.47±197.34 ml). However, the total bladder
urine detected by conventional CT was not significantly different
compared with the urine volume detected by 640-slice DVCT
(P>0.05).
Using 640-slice DVCT dynamically
observes the urine flow rate and the changes in the bladder volume
at all voiding phases
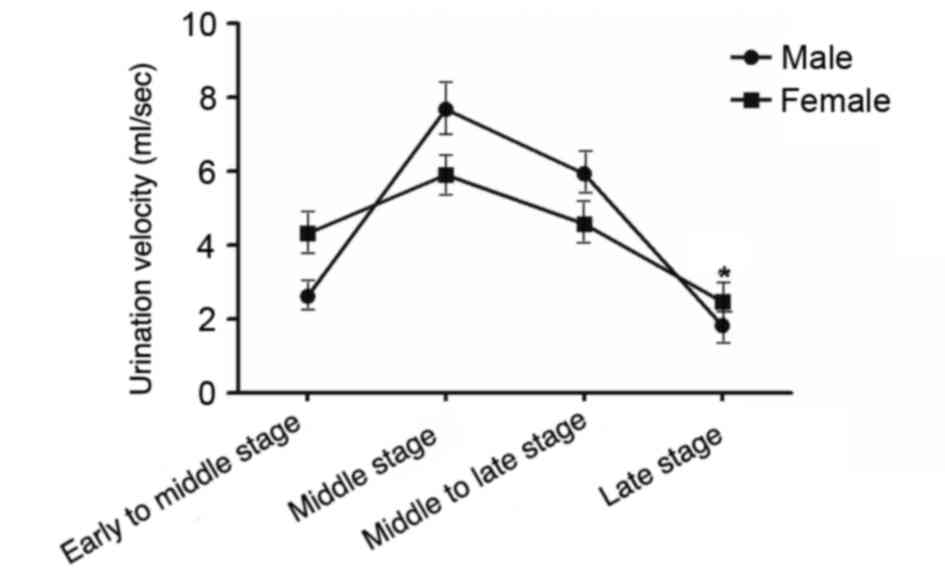
Analysis of the data for the normal subjects
demonstrated that males and females had their average maximum urine
flow rate at the middle voiding phase. In particular, the average
maximum urine flow rate at the middle voiding phase was 7.68±6.42
ml/sec for males, and 5.90±4.92 ml/sec for females. According to
the statistical analysis, there was significant difference in the
average flow rate at the late voiding phase between males and
females. The calculated average urine flow rate at the late voiding
phase was greater for females than for males, with the other phases
exhibiting no significant difference (Fig. 3). Males and females had a peak flow
rate in the middle voiding phase, with the flow rate presenting a
bell-shaped distribution.
No significant difference in the
bladder volume at all phases was detected between the 640-slice
DVCT and conventional CT groups
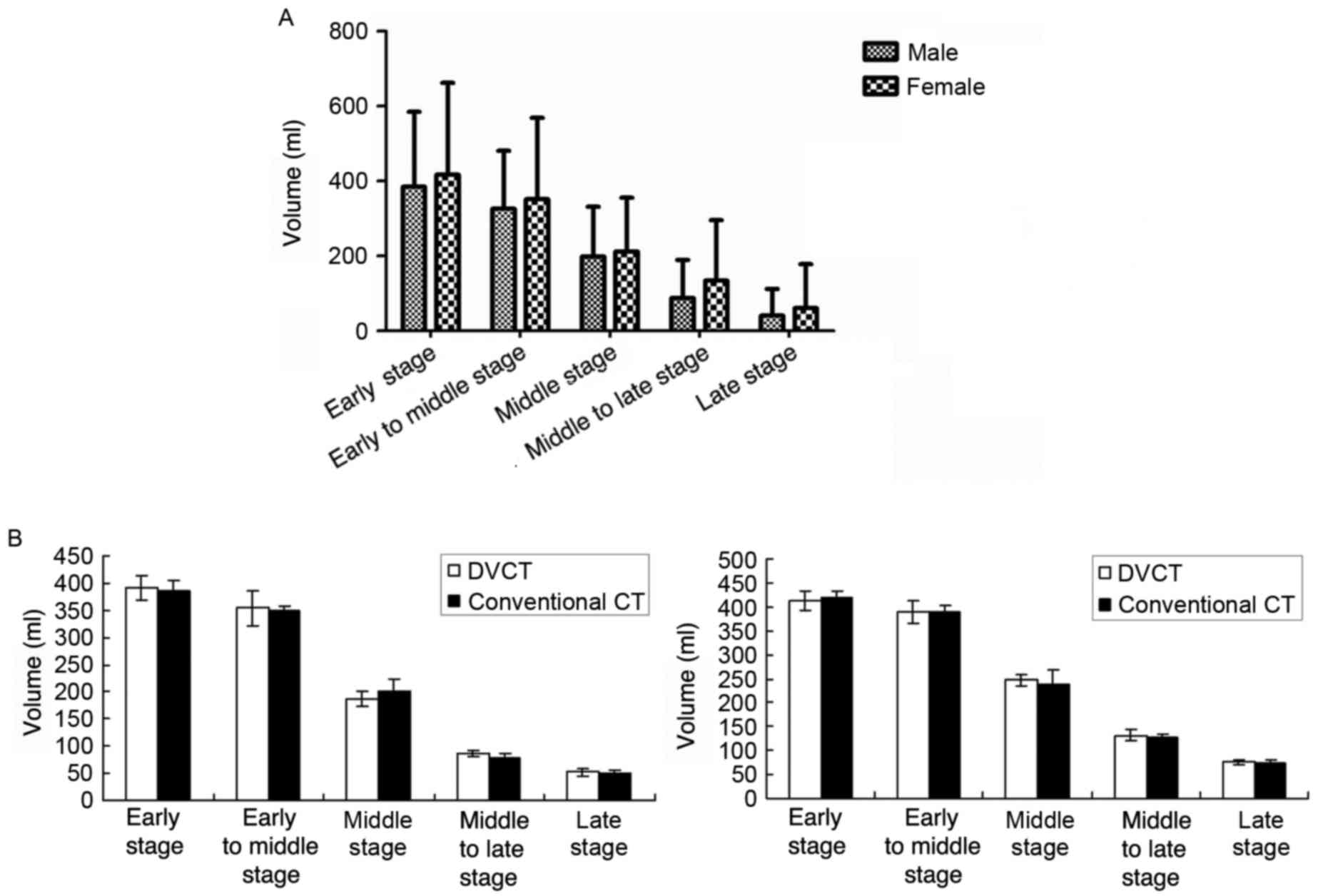
Statistical analysis revealed that there was no
significant difference in the bladder volume between normal males
and females at all voiding phases (Fig.
4A). In addition, no significant difference was identified
between the bladder volumes detected by DVCT and those detected by
conventional CT (Fig. 4B).
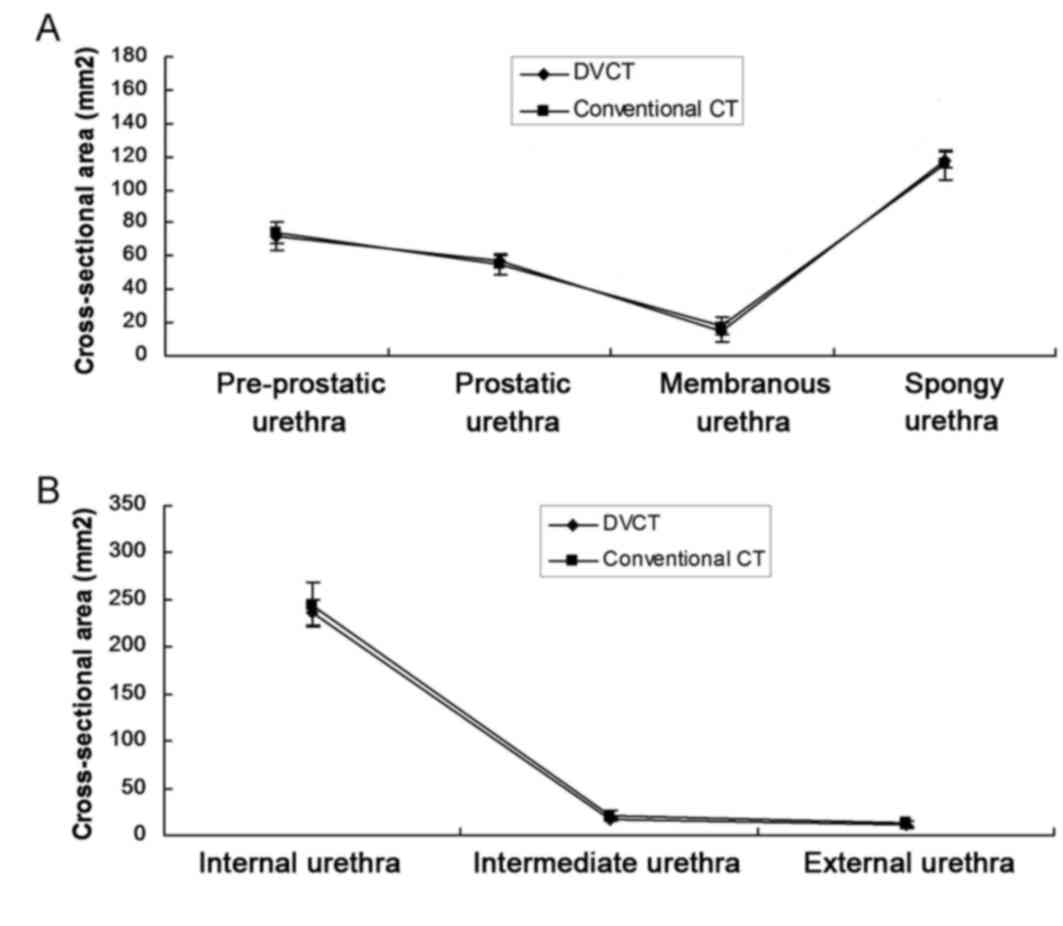
640-slice DVCT evaluates the status of
the male posterior urethra
The 640-slice DVCT and conventional CT methods were
respectively employed to measure the maximum diameter and the
cross-sectional area of the pre-prostatic, the prostatic, the
membranous, and the spongy regions of the male urethra, and the
results were statistically analyzed. The results exhibited no
significant difference between the values measured by 640-slice
DVCT and those measured using conventional CT (P>0.05; Fig. 5A).
640-slice DVCT evaluates the status of
the female urethra
The 640-slice DVCT and conventional CT methods were
respectively employed to measure the maximum diameter and the
cross-sectional area of the internal, intermediate and external
orifice regions of the female urethra. No significant difference
was detected between the values measured by 640-slice DVCT and
those measured by conventional CT (P>0.05; Fig. 5B).
Discussion
For studies of the lower urinary tract, conventional
urethrography has consistently been used as the gold standard for
nearly a century. It is a simple, easy and low-cost approach, as it
requires only conventional X-ray imaging and the retrograde
injection of diluted contrast agent to examine the lower urinary
tract (13,14). However, since X-ray photographs
obtained in the anteroposterior and double oblique views are
overlapped images, and the procedure is invasive, the feasibility
of this type of examination is limited (4,15).
Sonourethrography has been used to examine the lower urinary tract,
but is not widely applied because of its small field of vision and
a lack of recognition among urologists (4). MRI is also used to investigate
pathological conditions of the lower urinary tract, but the
inspection process is relatively complex (5,15,16), and
it is not suitable for use in subjects with a metal implant in the
pelvic area.
CT urethrography (CTU) could obtain similar results
to conventional urethrography (6–9).
High-speed 64-slice spiral CT is able to scan the entire urethra
and the bladder in <6 sec. The introduction of contrast agents,
as well as the high resolution and multi-dimensional
post-processing capability of CT, even for subjects for whom a
change in position is inconvenient, such as those with pelvic
fractures, enables a full range of axial and multi-planar images of
the lower urinary tract to be obtained in the supine position.
Compared with conventional urethrography, CTU may be less painful
for the subject being imaged. The comfortable position and
high-quality 3D images substantially improve the compliance of CTU
subjects. It is these advantages of CTU that enable male urethral
injury and female urethral fistula to be examined using 64-slice
spiral CT (9,10).
In 640-slice MDCT, all volume data in a 16-cm range
are captured in <0.35 sec to generate time-point images. For
example, when volumetric imaging of the bladder and urethra is
conducted, dynamic volume images of the bladder and urethra are
continuously captured by 640-slice MDCT during urination, and
measurements of the bladder and urethra are made at the early,
early to middle, middle, middle to late, and late phases by
division of the images according to time point, and collected for
statistical analysis. Previous studies have reported the use of
DVCT for imaging of the osteo-odonto-keratoprosthesis lamina, acute
chest pain or calcified coronary atherosclerotic plaque and airway
deformation (17–20). Therefore, in the present study, DVCT
technology was applied to predict the bladder volume and urine flow
rate of patients. The results revealed that there was no
significant difference between the total bladder urine volumes of
males and females measured using DVCT and the actual urine volumes.
This demonstrated that 640-slice MDCT was able to accurately
capture isotropic data of the bladder and urethra and measure the
volume values, displaying the anatomical data of the bladder and
urethra authentically and quantitatively. In addition, a
significant difference in the average flow rate at the late voiding
phase between males and females was identified, with females having
a higher calculated urine flow rate than males at the late voiding
phase. The reason for this is possibly that female subjects have an
active contraction of the detrusor at the late voiding phase.
However, this requires further confirmation by further
examinations.
The measurements in the present study focused on the
cross-sectional area and the inner diameter of the urethral
segments, which are previously unreported. To the best of our
knowledge, measurements of the cross-sectional area and the inner
diameter of each urethral segment during urination have not been
reported previously. For this reason, the correlation between the
widest diameter and the minimum diameter of the cross-sectional
area and the functional evaluation of the urethra is expected to
provide the basis for further research (21).
In conclusion, 640-slice DVCT is a promising
examination method for the replacement of traditional imaging
methods. Its advantage is that, by using only an approach and
position acceptable to the subject, in conformity with the
requirements of the radiation dose, data at each voiding phase is
obtained, 3D and 4D images are reconstructed, the anatomy of the
lower urinary tract is dynamically and accurately displayed, and
intramural data of the lower urinary tract can be quantified. This
method is likely to contribute to the diagnosis and quantitative
assessment of diseases in the lower urinary tract with anatomical
changes, in the absence of medical radiation exposure. This is the
first examination of the lower urinary tract by the application of
4D CT and quantitative assessment, and a large number of future
studies on various lower urinary tract diseases are required to
determine the clinical value of excretory cystography and
urethrography using 640-slice DVCT. However, due to the potential
risks of exposure to radiation, although the radiation dose used
for scanning was in the safe range, the use of the proposed method
is not recommended for children and childbearing women, due to the
special structure of their pelvic cavity.
Acknowledgements
Financial assistance was provided by Yunnan
Provincial Science and Technology Department (grant no.
2011FB229).
References
|
1
|
Zhu ZS, Wu H, Li RY and Wang DH: One-stage
urethroplasty with circumferential vascular pedicle preputial
island flap for perineal hypospadias. Zhonghua Zheng Xing Wai Ke Za
Zhi. 26:258–261. 2010.(In Chinese). PubMed/NCBI
|
|
2
|
Pavlica P, Menchi I and Barozzi L: New
imaging of the anterior male urethra. Abdom Imaging. 28:180–186.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kim B, Kawashima A and LeRoy AJ: Imaging
of the male urethra. Semin Ultrasound CT MR. 28:258–273. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gallentine ML and Morey AF: Imaging of the
male urethra for stricture disease. Urol Clin North Am. 29:361–372.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Milosevic M, Voruganti S, Blend R, Alasti
H, Warde P, McLean M, Catton P, Catton C and Gospodarowicz M:
Magnetic resonance imaging (MRI) for localization of the prostatic
apex: Comparison to computed tomography (CT) and urethrography.
Radiother Oncol. 47:277–284. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vilalta L, Altuzarra R, Espada Y,
Dominguez E, Novellas R and Martorell J: Description and comparison
of excretory urography performed during radiography and computed
tomography for evaluation of the urinary system in healthy New
Zealand white rabbits (Oryctolagus cuniculus). Am J Vet Res.
78:472–481. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Diefenderfer DL and Brightling P: Dysuria
due to urachal abscessation in calves diagnosed by contrast
urography. Can Vet J. 24:218–221. 1983.PubMed/NCBI
|
|
8
|
Chou CP, Huang JS, Wu MT, Pan HB, Huang
FD, Yu CC and Yang CF: CT voiding urethrography and virtual
urethroscopy: Preliminary study with 16-MDCT. AJR Am J Roentgenol.
184:1882–1888. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhang XM, Hu WL, He HX, Lv J, Nie HB, Yao
HQ, Yang H, Song B, Peng GM and Liu HL: Diagnosis of male posterior
urethral stricture: Comparison of 64-MDCT urethrography vs.
standard urethrography. Abdom Imaging. 36:771–775. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Qi Z, Lemen LC, Lamba M, Chen HH,
Samaratunga R, Mahoney M and Hendrick RE: Radiation dose to the
breast by 64-slice CT: Effects of scanner model and study protocol.
Acad Radiol. 23:987–993. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cool DA, Lazo E, Tattersall P, Simeonov G
and Niu S; International Commission on Radiological Protection, :
ICRP publication 125: Radiological protection in security
screening. Ann ICRP. 43:5–40. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
De Filippo M, Castagna A, Steinbach LS,
Silva M, Concari G, Pedrazzi G, Pogliacomi F, Sverzellati N,
Petriccioli D, Vitale M, et al: Reproducible noninvasive method for
evaluation of glenoid bone loss by multiplanar reconstruction
curved computed tomographic imaging using a cadaveric model.
Arthroscopy. 29:471–477. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Theisen KM, Kadow BT and Rusilko PJ:
Three-dimensional imaging of urethral stricture disease and
urethral pathology for operative planning. Curr Urol Rep.
17:542016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kawashima A, Sandler CM, Wasserman NF,
LeRoy AJ, King BF Jr and Goldman SM: Imaging of urethral disease: A
pictorial review. Radiographics 24 Suppl. 1:S195–S216. 2004.
View Article : Google Scholar
|
|
15
|
Osman Y, El-Ghar MA, Mansour O, Refaie H
and El-Diasty T: Magnetic resonance urethrography in comparison to
retrograde urethrography in diagnosis of male urethral strictures:
Is it clinically relevant? Eur Urol. 50:587–593. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Oh MM, Jin MH, Sung DJ, Yoon DK, Kim JJ
and Moon du G: Magnetic resonance urethrography to assess
obliterative posterior urethral stricture: Comparison to
conventional retrograde urethrography with voiding
cystourethrography. J Urol. 183:603–607. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Norris JM, Kishikova L, Avadhanam VS,
Koumellis P, Francis IS and Liu CS: Comparison of 640-slice
multidetector computed tomography versus 32-slice MDCT for imaging
of the osteo-odonto-keratoprosthesis Lamina. Cornea. 34:888–894.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yu SJ, Zhang L, Chen YF and Zhang J:
Effects of heart rate on image quality and radiation dose of
‘triple rule-out’ 320-row-640-slice multidetector computed
tomography scan in patients with acute chest pain. Zhonghua Yi Xue
Za Zhi. 92:2652–2655. 2012.(In Chinese). PubMed/NCBI
|
|
19
|
Kristanto W, van Ooijen PM, Groen JM,
Vliegenthart R and Oudkerk M: Small calcified coronary
atherosclerotic plaque simulation model: Minimal size and
attenuation detectable by 64-MDCT and MicroCT. Int J Cardiovasc
Imaging. 28:843–853. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yin Y, Choi J, Hoffman EA, Tawhai MH and
Lin CL: A multiscale MDCT image-based breathing lung model with
time-varying regional ventilation. J Comput Phys. 244:168–192.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Watanabe H, Takahashi S and Ukimura O:
Urethra actively opens from the very beginning of micturition: A
new concept of urethral function. Int J Urol. 21:208–211. 2014.
View Article : Google Scholar : PubMed/NCBI
|