Introduction
The concept of enhanced recovery after surgery
(ERAS) has been widely accepted in clinical practice, with the
benefits of improving outcomes and decreasing length of hospital
stay (1). The important components
of a successful anesthetic in an ERAS protocol are reduction of
opioid use and optimized pain control using a multimodal approach,
which includes neuroaxial or regional anesthesia techniques for the
primary anesthetic (2). Transversus
abdominis plane (TAP) block is a regional anesthesia technique that
has been widely used in abdominal surgery (3,4). TAP
block provides effective postoperative analgesia following
abdominal surgery, and it can be a useful strategy to reduce
perioperative opioid consumption, maintain intraoperative
hemodynamic stability and promote early recovery from anesthesia
(5,6). In addition, it is simple to perform TAP
block, and there are minimal procedure-associated complications
(7).
Although numerous studies have been performed
regarding the impact of TAP blocks on postoperative analgesia
(4–6), the usefulness of TAP blocks during
surgery have not been well studied. As an important part of a
multimodal analgesic regimen, TAP blocks can reduce intraoperative
opioid use. Recently, closed-loop titration guided by processed
electroencephalography, such as bispectral index (BIS), has become
clinically applicable, and can result in improved anesthetic
control (8). The system automates
anesthetic administration and thus helps avoid human error
(8,9). This automated system may enable
quantification of the anesthetic-sparing effect of an adjuvant,
such as epidural catheter or TAP block for analgesia (8,9). A
recent study indicated that thoracic epidural analgesia combined
with general anesthesia could decrease remifentanil and propofol
requirements by one-half and one-third when using hemodynamic
criteria or BIS for the titration of analgesia, respectively
(9).
The present study was designed to use a closed-loop
titration system guided by BIS to quantify the effect of TAP blocks
on the intraoperative use of propofol and remifentanil. The primary
hypothesis was that TAP blocks may decrease perioperative propofol
and remifentanil consumption under general anesthesia. Secondly,
the effect of TAP blocks on hemodynamics, time to tracheal
extubation and postoperative analgesia were investigated.
Materials and methods
Study protocol
This prospective, randomized, double-blind clinical
study was approved by the local ethics committee clinical trials
register (approval no. ChiCTR-IOR-17014111). Following the
collection of written informed consent, 60 patients aged 18–75
years with American Society of Anesthesiologists physical status
score II/III (3,6) scheduled for laparoscopic colectomy
under general anesthesia were enrolled in the present study.
Patients were recruited from March 1st 2017 to February 25th 2018
in Yantai Yuhuangding Hospital (Yantai, China).
Randomization and blinding
Patients were subjected to the following exclusion
criteria: History of allergy to the drugs used in the present
study, psychological disorders, infection of the block site, any
other contraindications of TAP block, tolerance to opioids or use
of opioids within 48 h prior to the study. The patients and all
staff involved in patient management and data collection were
blinded to group assignment until the end of the study. All TAP
blocks were performed by experienced anesthesiologists who did not
participate in data collection. The bilateral TAP blocks were
performed under general anesthesia. A third anesthesiologist, who
was not involved in the management of the patients or study,
prepared the randomized medications. The prepared syringes
contained either 20 ml normal saline for the CON group or 20 ml
0.375% ropivacaine (Qilu Pharmaceutical Co., Ltd., Jinan, China)
for the TAP group.
Anesthesia and TAP block
The visual analogue scale (VAS) (0=no pain and
10=the worst possible pain) was used for postoperative pain
assessment. On arrival at the operating room, patients were
randomized into the control (CON) group (n=30) or the TAP group
(n=30) using a computer-produced randomized list. All patients were
non-invasively monitored for blood pressure (BP), electrocardiogram
(ECG), heart rate (HR) and oxygen saturation (SpO2).
Neuromuscular blockade was monitored using the CONCERT-CL
neuromuscular blockade monitoring system provided by VERTARK
Technology Co., Ltd. (Guangxi, China), whereas BIS was monitored
using a BIS™ (Aspect Medical Systems, Inc., Norwood, MA,
USA). General anesthesia was induced using 0.05 mg/kg midazolam
(Jiangsu Nhwa Pharmaceutical Co., Ltd. Xuzhou, China), 0.4 µg/kg
sufentanil (Yichang Humanwell Pharmaceutical Co., Ltd., Yichang
China), 1.5–2.0 mg/kg propofol (Diprivan; AstraZeneca,
Macclesfield, UK) and 0.15 mg/kg cisatracurium (Jiangsu Hengrui
Medicine Co., Ltd, Jiangsu, China). Following intubation, general
anesthesia was maintained by propofol and remifentanil using
closed-loop titration guided by BIS. No inhalation anesthetic was
used. A previously described titration system and parameters of
target-controlled infusion were used for propofol and remifentanil
(Yichang Humanwell, Pharmaceutical Co., Ltd., Yichang, China),
respectively (10–12). The initial target concentrations of
propofol in the plasma (2–4 µg/ml) were selected by the
anesthesiologists according to standard practice. The target
concentration of propofol was automatically adjusted using the
closed-loop system to maintain a BIS value between 45–55 during
surgery. The target concentration of remifentanil was set at 2–8
ng/ml. The anesthesiologists administered the medication manually
or switched to manual infusion during surgery if required. The
closed-loop infusion of cisatracurium was used following induction
guided by the reappearance of the second twitch during train of
four stimulation. Ringer's acetate solution was used for volume
replacement. All aspects of anesthesia management, except for the
drug infusion, were performed by the anesthesiologists according to
current clinical practice.
The tidal volume was set at 6–8 ml/kg and the
respiratory rate at 12 breaths/min to maintain end-tidal
CO2 tension at 35–45 mmHg. Sufentanil was administered
at 0.3 µg/kg prior to skin incision. TAP block was performed
following induction using a similar method to that previously
described (13). Briefly, a
high-frequency linear ultrasound (US) probe (Venue 50; 7–12 MHz; GE
Healthcare, Chicago, IL, USA) was placed laterally to the abdominal
wall between the costal margin and the iliac crest on the mid
axillary line. A satisfactory image aimed to visualize the
subcutaneous fat, external oblique muscle, internal oblique muscle,
transversus abdominis muscle, peritoneum and intraperitoneal
cavity. The needle was introduced in the plane of the ultrasound
probe directly beneath the probe and advanced until it reached the
plane between the internal oblique and the transversus abdominis
muscles. The correct location of the needle tip was confirmed by
injection of 1 ml normal saline, which resulted in separation
between the internal oblique and transversus abdominis muscle.
Subsequently, 20 ml prepared solution was injected under
US-directed visualization. The same steps were repeated on the
opposite side.
Hemodynamic changes were treated according to study
protocol. Atropine (Shandong Xinhua Pharmaceutical Co., Ltd., Zibo,
China) was administered when HR was <45 bpm, esmolol (Qilu
Pharmaceutical Co., Ltd.) was administered when HR exceeded 120
bpm, phenylephrine was administered when BP was <80% of the
pre-induction value, and nicardipine was administered when systolic
blood pressure exceeded 160 mmHg.
A total of 5 mg dezocine (Yangtze River
Pharmaceutical Group, Taizhou, China) and 0.25 mg palonosetron
(Qilu Pharmaceutical Co., Ltd.) were administered intravenously
(IV) 30 min prior to the end of surgery. The infusion of
cisatracurium was stopped ~30 min prior to the end of surgery. Upon
completion of surgery, patients were treated with 1.0 mg
neostigmine (Shandong Xinhua Pharmaceutical Group Co., Ltd., Zibo,
China) and 0.5 mg atropine, if necessary, to achieve a
T4/T1 ratio >0.9, and the propofol and
remifentanil infusions were stopped. Patients were extubated once
the extubation criteria were met, and time to extubation was
recorded. The patients were transferred to the post-anesthesia care
unit (PACU) where they received nasal O2 supplementation
and were monitored continuously for vital signs (HR, BP, ECG and
SpO2). Complications were recorded for 6 h
postoperatively, including nausea, vomiting, hemodynamic
instability, desaturation or apnea. The VAS score at 2 h
post-surgery and the time to the first rescue analgesic request
were recorded. A total of 5 mg dezocine IV was administered as
rescue analgesia when the VAS score was ≥4. A total of 4 mg
ondansetron (Qilu Pharmaceutical Co., Ltd.) was administered IV if
necessary to relieve nausea or vomiting.
Statistical analysis
The mean propofol dosage required for maintenance of
anesthesia was 4.7±1.6 mg/kg/h when propofol and remifentanil were
co-administered via closed-loop titration guided by BIS (14). The present study was designed to
provide 90% power for detecting a 30% decrease in propofol dosage
among patients receiving TAP block with a bilateral α risk value of
0.05. A total of 60 patients were recruited in the present study.
All data in the present study were analyzed with SPSS (version
17.0; SPSS, Inc., Armonk, NY, USA). Data were presented as the mean
± standard deviation and count (%), as appropriate. Following
assessment of normality, continuous data were compared using
Student's t-test, whereas the Mann-Whitney test was performed to
compare non-continuous and non-normally distributed data.
χ2 or Fisher's exact tests were used to analyze
proportions. P<0.05 was considered to indicate a statistically
significant difference.
Results
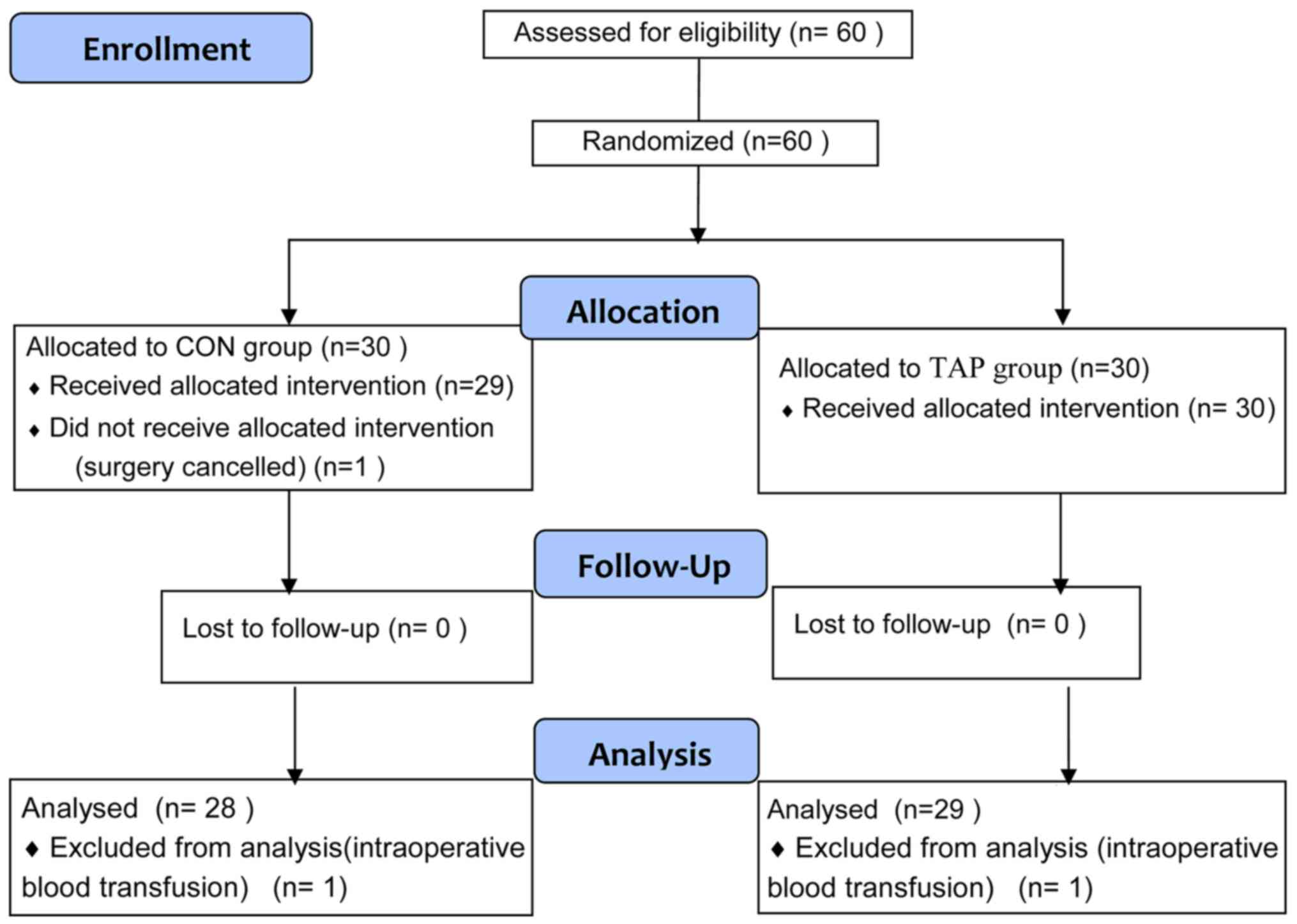
Fig. 1 illustrates
the CONSORT flow diagram of patient recruitment. A total of 60
patients were enrolled in the present trial. In the CON group, 1
patient withdrew due to surgery cancellation, and a further 2
patients (1 from the CON group and 1 from the TAP group) were
excluded due to intraoperative blood transfusion. A total of 57
patients completed the trial (28 in the CON group and 29 in the TAP
group). Patient characteristics did not differ significantly
between the two groups (P>0.05). Demographic and surgical
characteristics were comparable and there were no significant
differences between the groups (Table
I). The TAP block was easily localized via US and blocks were
uneventfully performed in all patients. There were no complications
associated with TAP block in the present study.
 | Table I.Clinical characteristics of patients
in the two groups. |
Table I.
Clinical characteristics of patients
in the two groups.
| Characteristic | CON group (n=28) | TAP group (n=29) | P-value |
|---|
| Age (years) | 58.5±11.2 | 59.2±10.6 | 0.73 |
| Male/female | 17/11 | 18/11 | 0.92 |
| ASA grade II/III | 10/18 | 12/17 | 0.66 |
| Right/left
hemicoloctomy | 13/15 | 15/14 | 0.69 |
| Weight (kg) | 73.2±11.4 | 74.3±11.5 | 0.72 |
| Height (cm) | 168.2±6.1 | 165.9±5.8 | 0.15 |
| BMI
(kg/m2) | 22.3±3.8 | 22.6±4.0 | 0.77 |
| Operative time
(min) | 162.6±48.5 | 166.8±38.7 | 0.72 |
| Blood loss (ml) | 156±85 | 162±94 | 0.80 |
| Infusion volume
(ml) | 1,864±425 | 1,786±501 | 0.53 |
| Urine output
(ml) | 624±104 | 674±121 | 0.10 |
Similar depths of anesthesia (BIS number, 45–55)
were maintained during the surgery, and the total doses of propofol
and remifentanil used were significantly less in the TAP group
compared with the CON group [propofol, 4.2±1.3 vs. 5.5±1.6 mg/kg/h
(P<0.001); remifentanil, 0.16±0.05 vs. 0.21±0.05 µg/kg/min
(P<0.001)]. The dose of cisatracurium was not significantly
different between the two groups (P>0.05). The frequency of
undesirable hemodynamic treatment effects (including hypotension,
hypertension, bradycardia and tachycardia) was also significantly
lower in the TAP group than in CON group (P<0.05; Table II).
| Table II.Comparison of anesthetic procedures
between the two groups during the maintenance phase. |
Table II.
Comparison of anesthetic procedures
between the two groups during the maintenance phase.
| Procedure | CON group (n=28) | TAP group (n=29) | P-values |
|---|
| Propofol |
|
|
|
| Mean dose
(mg/kg/h) | 5.5±1.6 | 4.2±1.3 | <0.001 |
| Mean
target concentration (µg/ml) | 2.7±0.7 | 2.1±0.5 | <0.001 |
| Remifentanil |
|
|
|
| Mean dose
(µg/kg/min) | 0.21±0.05 | 0.16±0.05 | <0.001 |
| Mean
target concentration (ng/ml) | 6.1±1.5 | 4.8±1.1 | <0.001 |
| Mean dose of
cisatracurium (mg/kg/h) | 0.86±0.21 | 0.84±0.18 | 0.914 |
| Undesirable
hemodynamic effects |
|
|
|
|
Hypotension requiring
treatment by phenylephrine | 11 (39.3) | 6 (20.7) | 0.021 |
|
Hypertension requiring
treatment by nicardipine | 7 (25.0) | 2 (7.9) | 0.023 |
|
Bradycardia requiring
treatment by atropine | 3 (10.7) | 4 (13.7) | 1.000 |
|
Tachycardia requiring
treatment by esmolol | 3 (10.7) | 3 (10.3) | 1.000 |
| Time to tracheal
extubation (min) | 14.2±4.9 | 9.8±3.2 | 0.031 |
| Pain score at 2 h
following surgery | 3.4±1.6 | 1.8±0.6 | 0.014 |
| Time to first
rescue analgesia (min) | 126±34 | 324±72 | 0.026 |
| Nausea and
vomiting | 5 (17.8) | 4 (13.8) | 0.953 |
All patients met the extubation criteria at the end
of surgery. However, time to tracheal extubation was significantly
shorter in the TAP group (9.8±3.2 min) than the CON group (14.2±4.9
min; P<0.05). VAS pain score at 2 h following surgery was
significantly reduced in the TAP group compared with the CON group
(P<0.05; Table II). The time to
first rescue analgesia was significantly delayed in the TAP group
(324±72 min) compared with the CON group (126±34 min; P<0.05).
Postoperative nausea and vomiting occurred at comparable rates in
each group (P>0.05).
Discussion
The results of the present study indicate that TAP
blocks may reduce the consumption of propofol by 28% and
remifentanil by 26%. Infusion with guided closed-loop titration
promoted hemodynamic stability, shortened recovery time and
improved postoperative analgesia.
The goal of anesthesia is to reduce acute
postoperative pain and decrease surgical stress responses.
Anesthesiologists serve an important role in facilitating the
recovery of patients undergoing surgery using an ERAS protocol.
Successful implementation of ERAS programs require
anesthesiologists to be more involved in perioperative care and to
be more aware of the impact of anesthetic techniques on surgical
outcomes and recovery (15).
Optimizing perioperative pain management while reducing opioid use
were the major goals of the present study.
Although total intravenous anesthesia (TIVA) with
propofol and remifentanil may be sufficient, prolonged use of TIVA
may increase adverse effects, including delayed awakening,
myocardial depression and hemodynamic instability (15). Patients undergoing abdominal surgery
often suffer from uncontrolled postoperative pain (2,3,6). Opioids have been used to treat moderate
to severe postoperative pain; however, they may cause complications
such as nausea and vomiting, respiratory depression and circulatory
depression (16,17). TAP block is a regional anesthetic
technique that blocks the abdominal wall neural afferents by
introducing local anesthetic into the fascial plane between the
internal oblique and transversus abdominis muscles (3). Following its initial description in
2001 by Rafi et al (18), its
use in postoperative pain management has gained popularity. TAP
block can provide effective analgesia for a variety of abdominal
surgical procedures by decreasing somatic pain (19–21).
Previously, it was demonstrated that TAP blocks may decrease
postoperative pain and opioid consumption in women undergoing
cesarean section (22). TAP block
has also been demonstrated to reduce the use of opioids, improve
pain control and expedite recovery in laparoscopic colorectal
surgery patients (23). A previous
meta-analysis of the efficacy of TAP block demonstrated that it
reduced the requirement for postoperative opioids and associated
side-effects, and provided more effective pain relief (24), suggesting that there may be a role
for TAP blocks as part of an effective multimodal pain regimen.
Erdogan et al (5)
demonstrated that there was significantly lower remifentanil
consumption and anesthesia recovery time, but no significant
differences in desflurane consumption in liver transplant donors
who received TAP block, compared with donors who didn't receive TAP
block. Tsuchiya et al (6)
reported a similar sparing-effect of TAP block on sevoflurane and
fentanyl use in abdominal surgery. In these studies, the titration
of different anesthetics was mainly dependent on clinical
hemodynamic criteria. However, hemodynamic changes are influenced
by numerous variables, including preload state, pre-existing
cardiovascular conditions, surgical blood loss and vasopressor
usage. In the present study, anesthetic titration was performed
with a closed loop automated system, limiting investigator bias. In
addition, to the best of our knowledge, no previous studies
quantified the opioid sparing effect of TAP blocks on propofol and
remifentanil.
Anesthesiologists typically titrate anesthetics
based on a combination of hemodynamic changes and clinical signs,
alongside their knowledge of pharmacokinetics and pharmacodynamics.
The factors involved in the decision-making process are also
subject to variations between individuals. By contrast, closed-loop
titration used in the present study responds to changes in BIS
values, which may result in a more objective mode of maintenance of
anesthesia. By adding TAP blocks to a closed-loop protocol,
distinguishing the effect of propofol and remifentanil on the depth
of anesthesia may be possible. Guignard et al (25) reported in a previous controlled trial
that, following a pain stimulus, the BIS and hemodynamics changes
were similar. TAP blocks demonstrated a sparing effect on the
amount of propofol and remifentanil required to maintain surgical
anesthesia. TAP blocks also provided additional analgesia by
delaying the time for first rescue analgesic request, and VAS pain
scores 2 h after surgery were lower, which is consistent with past
meta-analysis studies (19,22,23).
Although intraoperative safety of surgical patients
has greatly improved, cardiovascular complications still pose
significant risks to high-risk patients with severe cardiovascular
disease undergoing abdominal surgery (26). In the present study, patients who
received TAP blocks exhibited less significant changes in
hemodynamics that required treatment with vasopressors. These
findings may be beneficial for critically ill and elderly patients
who may be more vulnerable to changes in hemodynamics.
The time to tracheal extubation was also decreased
in patients with TAP blocks, likely attributable to a decrease in
total remifentanil and propofol levels. The incidence of
postoperative nausea and vomiting was similar in both groups.
However, the present study was not powered for this result, given
the low incidence in patients who received total IV anesthesia and
palonosetron prior to the end of surgery.
There are limitations of the present study. Although
VAS scores were lower in the TAP block group, there is no objective
way to evaluate the anti-nociceptive effect of TAP block. Secondly,
only patients aged from 18–75 years were included, whereas elderly
patients (>75 years) were not included, which may introduce a
selection bias. A more age comprehensive study should be performed
in the future. Finally, the impact of TAP blocks on the
postoperative period, such as the length of stay in the PACU and
hospital admission, were not investigated in the present study.
In conclusion, in laparoscopic colectomy, TAP blocks
may reduce propofol and remifentanil consumption within a
closed-loop anesthetic delivery system, shorten time to tracheal
extubation and promote intraoperative hemodynamic stability. TAP
blocks may also serve a vital role in multimodal analgesia for
abdominal surgeries and promote enhanced recovery following
surgery.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Nature and
Science Fund of Shandong Province, China (grant no. ZR2014HL109),
the Science and Technology Program Foundation of Yantai, China
(grant no. 2014WS009), and the Departments of Anesthesiology and
Pain Medicine of University of California Davis Health (grant no.
UL1 TR001860).
Availabilty of data and materials
The data used and analyzed during the current study
are available from the corresponding author on reasonable
request.
Authors' contributions
JM and XW performed the study and also were major
contributors in writing the manuscript. QS and TL analyzed the
data. JM and HL designed the study and revised the manuscript. JZ
interpreted the data and revised the manuscript critically. MJ and
GL performed the study and collected the data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
Approval was obtained from the Institutional Human
Investigations Committee and Institutional Review Board of The
Affiliated Yantai Yuhuangding Hospital of Qingdao University. All
patients provided written informed consent for participation.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Li Z, Wang Q, Li B, Bai B and Zhao Q:
Influence of enhanced recovery after surgery programs on
laparoscopy-assisted gastrectomy for gastric cancer: A systematic
review and meta-analysis of randomized control trials. World J Surg
Oncol. 15:2072017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wick EC, Grant MC and Wu CL: Postoperative
multimodal analgesia pain management with nonopioid analgesics and
techniques: A review. JAMA Surg. 152:691–697. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
McDonnell JG, O'Donnell B, Curley G,
Heffernan A, Power C and Laffey JG: The analgesic efficacy of
transversus abdominis plane block after abdominal surgery: A
prospective randomized controlled trial. Anesth Analg. 104:193–197.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim AJ, Yong RJ and Urman RD: The role of
transversus abdominis plane blocks in enhanced recovery after
surgery pathways for open and laparoscopic colorectal surgery. J
Laparoendosc Adv Surg Tech A. 27:909–914. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Erdogan MA, Ozgul U, Uçar M, Yalin MR,
Colak YZ, Çolak C and Toprak HI: Effect of transversus abdominis
plane block in combination with general anesthesia on perioperative
opioid consumption, hemodynamics, and recovery in living liver
donors: The prospective, double-blinded, randomized study. Clin
Transplant. 31:2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tsuchiya M, Takahashi R, Furukawa A,
Suehiro K, Mizutani K and Nishikawa K: Transversus abdominis plane
block in combination with general anesthesia provides better
intraoperative hemodynamic control and quicker recovery than
general anesthesia alone in high-risk abdominal surgery patients.
Minerva Anestesiol. 78:1241–1247. 2012.PubMed/NCBI
|
|
7
|
Conaghan P, Maxwell-Armstrong C, Bedforth
N, Gornal C, Baxendale B, Hong LL, Carly HM and Acheson AG:
Efficacy of transversus abdominis plane blocks in laparoscopic
colorectal resections. Surg Endosc. 24:2480–2484. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brogi E, Cyr S, Kazan R, Giunta F and
Hemmerling TM: Clinical performance and pafety of closed-loop
systems: A systematic review and meta-analysis of randomized
controlled trials. Anesth Analg. 124:446–455. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dumans-Nizard V, Le Guen M, Sage E, Chazot
T, Fischler M and Liu N: Thoracic epidural analgesia with
levobupivacaine reduces remifentanil and propofol consumption
evaluated by closed-loop titration guided by the bispectral index:
A double-blind placebo-controlled study. Anesth Analg. 125:635–642.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu Y, Li M, Yang D, Zhang X, Wu A, Yao S,
Xue Z and Yue Y: Closed-loop control better than open-loop control
of profofol TCI guided by BIS: A randomized, controlled,
multicenter clinical trial to evaluate the CONCERT-CL closed-loop
system. PLoS One. 10:e01238622015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Marsh B, White M, Morton N and Kenny GN:
Pharmacokinetic model driven infusion of propofol in children. Br J
Anaesth. 67:41–48. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Minto CF, Schnider TW, Egan TD, Youngs E,
Lemmens HJ, Gambus PL, Billard V, Hoke JF, Moore KH, Hermann DJ, et
al: Influence of age and gender on the pharmacokinetics and
pharmacodynamics of remifentanil. I. model development.
Anesthesiology. 86:10–23. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hebbard P, Fujiwara Y, Shibata Y and Royse
C: Ultrasound-guided transversus abdominis plane (TAP) block.
Anaesth Intensive Care. 35:616–617. 2007.PubMed/NCBI
|
|
14
|
Liu N, Chazot T, Hamada S, Landais A,
Boichut N, Dussaussoy C, Trillat B, Beydon L, Samain E, Sessler DI
and Fischler M: Closed-loop coadministration of propofol and
remifentanil guided by bispectral index: A randomized multicenter
study. Anesth Analg. 112:546–557. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baldini G and Fawcett WJ: Anesthesia for
colorectal surgery. Anesthesiol Clin. 33:93–123. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kumar K, Kirksey MA, Duong S and Wu CL: A
Review of opioid-sparing modalities in perioperative pain
management: Methods to decrease opioid use postoperatively. Anesth
Analg. 125:1749–1960. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sarin A, Litonius ES, Naidu R, Yost CS,
Varma MG and Chen LL: Successful implementation of an enhanced
recovery after surgery program shortens length of stay and improves
postoperative pain, and bowel and bladder function after colorectal
surgery. BMC Anesthesiol. 16:552016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rafi AN: Abdominal field block: A new
approach via the lumbar triangle. Anaesthesia. 56:1024–1026. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Abdallah FW, Laffey JG, Halpern SH and
Brull R: Duration of analgesic effectiveness after the posterior
and lateral transversus abdominis plane block techniques for
transverse lower abdominal incisions: A meta-analysis. Br J
Anaesth. 111:721–735. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Johns N, O'Neill S, Ventham NT, Barron F,
Brady RR and Daniel T: Clinical effectiveness of transversus
abdominis plane (TAP) block in abdominal surgery: A systematic
review and meta-analysis. Colorectal Dis. 14:635–642. 2012.
View Article : Google Scholar
|
|
21
|
Abdallah FW, Chan VW and Brull R:
Transversus abdominis plane block: The effects of surgery, dosing,
technique, and timing on analgesic outcomes. A systematic review.
Reg Anesth Pain Med. 37:193–209. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Eslamian L, Jalili Z, Jamal A, Marsoosi V
and Movafegh A: Transversus abdominis plane block reduces
postoperative pain intensity and analgesic consumption in elective
cesarean delivery under general anaesthesia. J Anesth. 26:334–338.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pedrazzani C, Menestrina N, Moro M, Brazzo
G, Mantovani G, Polaiti E and Guqlielmi A: Local wound infiltration
plus transversus abdominis plane (TAP) block versus local wound
infiltration in laparoscopic colorectal surgery and ERAS program.
Surg Endosc. 30:5117–5125. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Siddiqui MR, Sajid MS, Uncles DR, Cheek L
and Baig MK: A meta-analysis of the clinical effectiveness of
transverse abdominis plane block. J Clin Anesth. 23:7–14. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Guignard B, Menigaux C, Dupont X, Fletcher
D and Chauvin M: The effect of remifentanil on the Bispectral index
change and hemodynamic responses after orotracheal intubation.
Anesth Analg. 90:161–167. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tsuchiya M, Sato EF, Inoue M and Asada A:
Open abdominal surgery increases intraoperative oxidative stress:
Can it be prevented? Anesth Analg. 107:1946–1952. 2008. View Article : Google Scholar : PubMed/NCBI
|