Introduction
Atopic dermatitis (AD) is a chronic, pruritic skin
condition that occurs most frequently in children, but can also
affect adults. It is a complex, multifactorial, inflammatory
disease; it affects an increasing number of patients and follows a
relapsing course (1).
Patients with AD have a broad spectrum of clinical
manifestations and a personal or family history of type I allergies
(allergic rhinitis, asthma) associated with elevated serum
immunoglobulin E (IgE) levels.
During the past 3 decades, the incidence of AD has
clearly increased, especially in industrialized countries. Nowadays
the prevalence is 15–30% in children and 2–10% in adults, and AD is
becoming one of the most common chronic skin disorders in developed
countries, with an important socio-economic impact (2).
This cutaneous disease has a major impact on
patients' quality of life (QoL), due to the intense pruritus, sleep
loss, dietary restrictions and the psychosocial boundaries it
creates (3).
AD ethiopathogenesis and its causative factors
remain a matter of debate, despite the numerous studies carried
out. Epidermal barrier abnormalities and gene-environment
interactions contribute to the clinical heterogenicity of AD, from
dry skin to infection and severe erythroderma (4).
Recent studies reveal that clinically
normal-appearing skin may present minimal inflammation with a
sparse perivascular T-cell infiltrate. Langerhans cells with
surface-bound IgE are likely to be present, even if to a lesser
extent than within affected regions. Disturbed barrier function due
to dehydration and reduced stratum corneum (SC) were detected in
clinically healthy skin. These facts substantiate the need for
dermatologists to consider the correct evaluation and therapeutic
management of apparently healthy skin, along with lesional sites
(5).
QoL assessment has become an important tool in
evaluating the impact of chronic conditions such as eczema
(6). It is currently considered an
important outcome measure in clinical trials and practice,
assessing the disease progression and the response to treatment.
Patients' QoL can be influenced by many factors and is mainly
related to the AD symptoms. The most common and life-impacting one
is pruritus, a major complaint in most AD cases. This may impact
the psychosomatic aspect of the condition and deserves special
consideration during therapeutic management.
The Dermatology Life Quality Index (DLQI) is one of
the most common instruments used in research and general practice
for measuring QoL (7).
For clinical evaluation of the cutaneous lesions
during all therapeutic phases it is mandatory to determine the
severity of AD. The European Task Force on Atopic Dermatitis
(ETFAD) has developed the SCORing AD (SCORAD). This established a
consensus on assessment methods for AD, making possible the
comparison between study results (8). There are studies showing that AD
impacts negatively on the QoL, proportional to the severity of the
disease (9).
High-frequency ultrasonography (HF-USG) has been
used in dermatology since the 1970s. It has been consistently
improved and nowadays it offers the clinician the opportunity of
real-time imaging, with the possibility of various measurements of
morphological, physiological and pathological aspects. The images
reflect the structure and tissue composition, influenced by the
properties of the specific sound wave. Echogenicity of the dermis
is one of the main relevant parameters, influenced by several
factors. It is determined by orientation of collagen fibers, ground
substance and water content (10–12).
An increase in echogenicity is caused by diseases
with accumulation of fibers, besides increased number of
inflammatory or neoplastic cells. Fiber damage will lower the
echogenicity of the dermis. In inflammatory dermatoses, such as AD,
it is easy to detect a subepidermal low-echogenic band (SLEB).
A main ultrasonographic characteristic of AD is the
SLEB, accompanied by lower echogenicity of the other layers of the
skin, compared to healthy skin. The SLEB is observed mainly due to
edema and inflammatory cell infiltration has been reported in
correlation with disease severity. It could be used as a major
parameter for monitoring the treatment efficacy (13).
In light of these facts, the present study aims to
assess lesional and non-lesional skin of AD patients with the use
of HF-USG, focusing on skin barrier function and inflammation,
quantified by the SLEB. In non-lesional skin, a hypoechoic band
could indicate a subclinical eczematous reaction, anticipating the
typical skin lesions.
Patients and methods
Participants
We included in our study a group of 10 patients, 8
women and 2 men. They joined the study on a volunteer basis. They
were diagnosed with AD in accordance with the Hanifin and Rajka
criteria (14), with a minimum of
one active lesion at the time of the study. We excluded patients
with uncertain diagnoses, as well as patients with overlapping
conditions (for instance, an overlap of AD and systemic lupus
erythematosus), which could impact overall skin health. Patients
were of different ages, ranging from 15 to 74 years.
The patients were referred to the Department of
Dermatology, part of Iuliu Hatieganu University of Medicine and
Pharmacy, or to DEA Clinic, due to the exacerbation of skin lesions
in the period from November 2017 to April 2018. We performed a full
skin examination, searching for clinical signs of AD (15). We noted that patients presented
marked xerosis and typical lesions of AD: facial pallor, keratosis
pilaris, palmar hyperliniarity, periocular manifestations,
lichenification, prurigo and pitiriazis alba.
The study was designed as a matched case-control
study, where each patient is its own control, by choosing two
homologous areas for HF-USG: one with an active dermatitis lesion
and one deemed clinically healthy. The study was approved by the
Ethics Committee of ‘Iuliu Hatieganu’ University of Medicine and
Pharmacy (Cluj-Napoca, Romania). The patients were informed of
their role in the study, the data that was collected during the
study, and signed informed consents to participate in the study,
and for the study results to be published.
Clinical evaluation
Each patient was evaluated clinically with regards
to the severity, extent and psychological impact of the disease. We
assessed the clinical severity of AD using SCORAD. We registered
the patients, age, weight, height, and medical conditions (16).
Patients experience a variety of symptoms due to AD,
these may affect their QoL. DLQI was used to quantify the impact of
AD on the patients' QoL (17).
We performed HF-USG, focusing on the measurements on
the thickness and intensity of the dermis, and the SLEB, both in
apparently healthy skin, and in an active patch of AD. For this we
used the DermaLab Combo® device (Cortex Technology,
Hadsund, Denmark) (13).
Statistical analysis
The descriptive statistical analysis was performed
in Microsoft Excel (Microsoft, Redmond, WA, USA), while the
inferential statistical analysis was carried out using MedCalc
Statistical Software version 18.2.1 (MedCalc Software bvba, Ostend,
Belgium). To describe continuous variables, the median and 25 and
75th percentiles were used. To determine the correlations between
variables, Spearman's rho coefficient test was used.
Results
Study group features
Our study group of 10 subjects included 8 female
patients and 2 male patients, aged between 15 and 74 years. The
median age was 26 years, with the 25th percentile at 21.75 and the
75th percentile at 32.5, 20% of patients had a BMI over 30, while
another 20% had a BMI under 18. The rest of the patients were of
normal weight, with a BMI between 18 and 25. The majority of
patients included in our study were young adults, with normal
BMI.
Skin assessment
The Fitzpatrick phototype distribution was as
follows: Patients (10%) were phototype I, 60% phototype II and 30%
phototype III. According to our geographic area, most of the
patients included, had the phototype specific for our region.
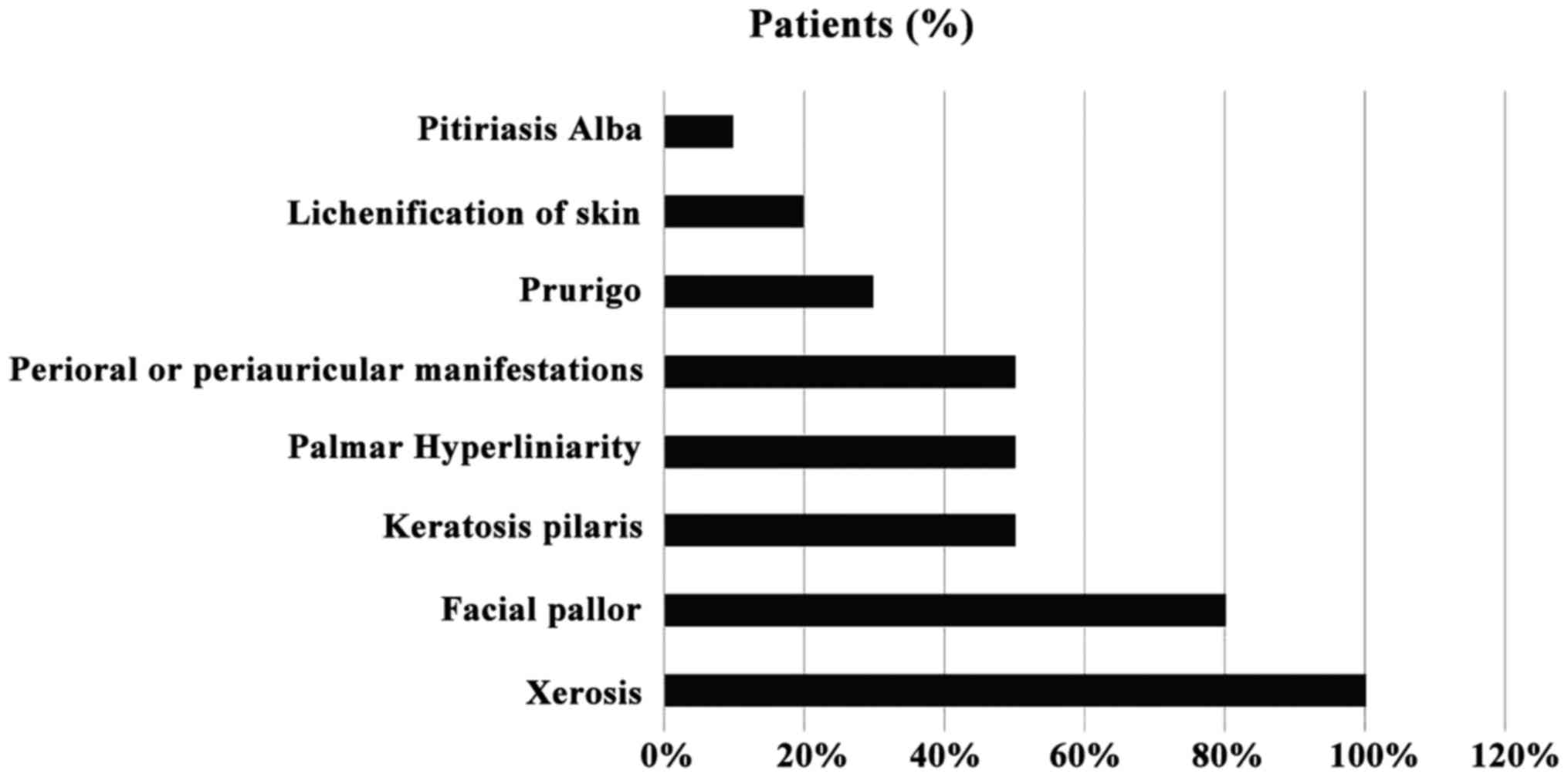
All the patients reported xerosis, with 80%
reporting facial pallor, 50% keratosis pilaris, 50% palmar
hyperliniarity and 50% periocular, perioral or periauricular
manifestations, 30% reported prurigo, 20% manifested
lichenification of the skin and 10% pitiriasis alba The reported
clinical manifestations are depicted in Fig. 1.
Questionnaire results
The median value for DLQI was 8, with the 25th
percentile at 4.75 and the 75th percentile at 15.75. Three of them
were experiencing only minimal impact of AD on their lives (DLQI
<5), four of them were moderately affected by the AD symptoms
(DLQI 6–10) and the other three patients had their QoL seriously
affected by AD (DLQI 11–20).
For the SCORAD questionnaire, the median value
obtained was 35.05, with the 25th percentile at 24.03 and the 75th
percentile at 54.23. Of the patients 30% presented mild AD (SCORAD,
25); other 40% registered SCORAD values between 25 and 50, being
diagnosed with moderate AD. Of the patients 30% had a severe form
of AD (SCORAD >50).
Ultrasound results
The non-lesional SLEB median was 13, with the 25th
percentile at 0 and the 75th percentile at 181. The lesional SLEB
median was 164, with the 25th percentile at 49.50 and 75th
percentile at 279.50. The non-lesional skin thickness median was
875.50 µm, with the 25th percentile at 622 µm and the 75th
percentile at 1409 µm. The lesional skin thickness had a median of
1099.50 µm, with the 25th percentile at 875.50 µm and the 75th
percentile at 1362 µm. The non-lesional intensity median was 60.4,
with 25th and 75th percentiles at 39.15 and 68.475 respectively.
The lesional intensity score median was at 37.95, with the 25th and
75th percentiles at 34.675 and 52.5, respectively.
Correlations
In non-lesional skin measurements, DLQI was
correlated with skin thickness (Spearman's rho correlation
coefficient=0.657; P=0.039) and intensity (Spearman's rho CC=0.675,
P=0.032). The correlation of DLQI and SLEB was not statistically
significant (P=0.215). The SCORAD score was not significantly for
any of the investigated ultrasonographical markers: for SLEB,
P=0.590, for thickness P=0.511, and for intensity, P=0.556. The
correlations of lesional skin can be found in Table I, but they did not reach statistical
significance.
 | Table I.Correlation between DLQI, SCORAD and
HF-USG parameters. |
Table I.
Correlation between DLQI, SCORAD and
HF-USG parameters.
| Tests | DLQI | SCORAD | Lesional LEB | Lesional
thickness | Lesional
intensity |
|---|
| DLQI |
| Spearmans
rho correlation coefficient | 1.000 | 0.474 | −0.349 | 0.109 | 0.024 |
|
P-value | <0.001 | 0.166 | 0.324 | 0.763 | 0.947 |
| SCORAD |
| Spearmans
rho correlation coefficient | 0.474 | 1.000 | 0.177 | −0.309 | −0.515 |
|
P-value | 0.166 | <0.001 | 0.625 | 0.385 | 0.0128 |
Discussion
The most valuable finding of our study is that DLQI
is associated with the intensity and thickness of non-lesional
skin. This confirms that indeed, AD affects the overall skin
barrier, and this in itself causes an impact on the patients' QoL.
This finding is sustained by the current literature: it has been
established that apparently healthy skin presents subclinical
disturbances and changes in patients suffering from AD (4). Furthermore, the images obtained through
HF-USG correlate with histology results in the case of seemingly
healthy skin, supporting the same conclusion: that there is
subclinical change in the apparently healthy skin of patients with
AD (18). We follow with the notion
that these changes are meaningful enough to impact our patients'
QoL. The SCORAD results did not significantly correlate with our
ultrasonographic parameters, nor with the DLQI scores. This
suggests that the perception of the condition by the patient might
influence their QoL to a higher extent than the objective reality
of their condition.
The strength of our study is that, to our knowledge,
it is the first study in Romania that used HF-USG to assess changes
in AD and correlated it with clinical and subjective
parameters.
The major limitation to our study is the sample
size. We expect that the enlargement of this initial study would
attain a higher level of statistical significance.
With regards to our study group, it is skewed
towards young female adults. Both male participants included in the
study had BMIs outside of the reference range (one had a BMI of 17,
classified as underweight and the other had a BMI of 33 classified
as first degree obesity). A larger sample size is needed to
determine whether AD is correlated with abnormal weight in men.
Most of our patients are a Fitzpatrick phototype II,
with 1 patient being a I and 2 being a III. This limits the
conclusions of our study to populations in Central-Northern
Europe.
The medians of both DLQI and SCORAD classify as
moderate in terms of impact on the QoL and severity, thus pointing
out that our study results might not apply in patients with severe
or mild forms of AD.
Our aim is to continue this project and extend our
ultrasonographic evaluation (HF-USG) of AD patients, including
patients with mild or severe forms of the condition, and
crystallize the clinical and subjective image of the patient
suffering from AD.
Our results offer a basis to reassess the current
therapeutic approach, which for the moment focuses only on the
remission of active lesions. It might be reasonable to consider
targeting the overall state of the skin barrier, as well as its
impact on the patients' QoL.
In conclusion, our study revealed that HF-USG of the
skin is able to assess specific modifications of the AD, both in
lesional and non-lesional areas. The hypoechoic band (SLEB) can be
present even in the normal-looking, non-lesional skin of some AD,
presenting barrier function defects and may indicate subclinical
eczematous skin reactions, in early stages AD. In non-lesional
skin, the measured thickness corelates with patients QoL.
As a noninvasive and objective evaluation, HF-USG
could be included in the current management of AD, helping assess
disease severity and therapeutic outcome, in correlation with
common scales and scores.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contribution
MS and RFI were responsible for the aquisition and
analysis of the data regarding the disease and the HF-USG
parameters. AT and ANB contributed to the conception and design of
the study, and revising it critically for important intellectual
content. All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
‘Iuliu Hatieganu’ University of Medicine and Pharmacy (Cluj-Napoca,
Romania), and written informed consent was obtained from all
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AD
|
atopic dermatitis
|
|
HF-USG
|
high-frequency ultrasonography
|
|
SLEB
|
subepidermal low-echogenic band
|
|
DLQI
|
Dermatology Life Quality Index
|
|
QoL
|
Quality of Life
|
|
SCORAD
|
SCORing Atopic Dermatitis
|
References
|
1
|
Lawrance FE: Guidelines of care for the
management of atopic dermatitis-Part 1: Diagnosis and assessment of
atopic dermatitis. J Am Acad Dermatol. 70:338–351. 2015.
|
|
2
|
Wollenberg A and Bieber T: Proactive
therapy of atopic dermatitis - an emerging concept. Allergy.
64:276–278. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eichenfield LF, Tom WL, Berger TG, Krol A,
Paller AS, Schwarzenberger K, Bergman JN, Chamlin SL, Cohen DE,
Cooper KD, et al: Guidelines of care for the management of atopic
dermatitis: Section 2. Management and treatment of atopic
dermatitis with topical therapies. J Am Acad Dermatol. 71:116–132.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Polańska A, Dańczak-Pazdrowska A, Silny W,
Jenerowicz D, Olek-Hrab K and Osmola-Mańkowska A: Nonlesional skin
in atopic dermatitis is seemingly healthy skin - observations using
noninvasive methods. Wideochir Inne Tech Malo Inwazyjne. 8:192–199.
2013.PubMed/NCBI
|
|
5
|
Polańska A, Dańczak-Pazdrowska A, Silny W,
Jenerowicz D, Osmola-Mańkowska A and Olek-Hrab K: Evaluation of
selected skin barrier functions in atopic dermatitis in relation to
the disease severity and pruritus. Postepy Dermatol Alergol.
29:373–377. 2012. View Article : Google Scholar
|
|
6
|
Basra MK, Salek MS, Camilleri L, Sturkey R
and Finlay AY: Determining the minimal clinically important
difference and responsiveness of the Dermatology Life Quality Index
(DLQI): Further data. Dermatology. 230:27–33. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Heinl D, Chalmers J, Nankervis H and
Apfelbacher CJ: Eczema trials: Quality of life instruments used and
their relation to patient-reported outcomes. A systematic review.
Acta Derm Venereol. 96:596–601. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rehal B and Armstrong AW: Health outcome
measures in atopic dermatitis: A systematic review of trends in
disease severity and quality-of-life instruments 1985–2010. PLoS
One. 6:e175202011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Holm JG, Agner T, Clausen ML and Thomsen
SF: Quality of life and disease severity in patients with atopic
dermatitis. J Eur Acad Dermatol Venereol. 30:1760–1767. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fornage BD: High-frequency sonography of
the skin. Eur J Ultrasound. 2:173–182. 1995. View Article : Google Scholar
|
|
11
|
Gutierrez M, Wortsman X, Filippucci E, De
Angelis R, Filosa G and Grassi W: High-frequency sonography in the
evaluation of psoriasis: Nail and skin involvement. J Ultrasound
Med. 28:1569–1574. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marina ME, Botar Jid C, Roman II, Mihu CM
and Tătaru AD: Ultrasonography in psoriatic disease. Med Ultrason.
17:377–382. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Polańska A, Dańczak-Pazdrowska A, Jałowska
M, Żaba R and Adamski Z: Current applications of high-frequency
ultrasonography in dermatology. Postepy Dermatol Alergol.
34:535–542. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Filipowska-Grońska A, Weryńska-Kalemba M,
Bożek A, Filipowska B, Żebracka-Gala J, Rusinek D, Kula D and
Jarząb J: The frequency of polymorphic variants of filaggrin gene
and clinical atopic dermatitis. Postepy Dermatol Alergol. 33:37–41.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lifschitz C: The impact of atopic
dermatitis on quality of life. Ann Nutr Metab. 66:34–40. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rzany B: Too many instruments for
measuring Quality of Life in Atopic Dermatitis. J Eur Acad Dermatol
Venereol. 31:574. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kong TS, Han TY, Lee JH and Son SJ:
Correlation between severity of atopic dermatitis and sleep quality
in children and adults. Ann Dermatol. 28:321–326. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Polańska A, Dańczak-Pazdrowska A, Silny W,
Woźniak A, Maksin K, Jenerowicz D and Janicka-Jedyńska M:
Comparison between high-frequency ultrasonography and
histopathology in atopic dermatitis. Ski Res Technol. 19:432–437.
2013.
|