Introduction
Chronic venous disease (CVD) affects millions of
people and most of the patients are diagnosed with CVD in advanced
stages (1–5). The estimated prevalence of varicose
veins varies between 5 and 30% in the adult population and with a
female to male predominance, respectively 3 to 1. Other data are
suggesting a higher male prevalence (3). According to most authors, risk factors
include age, sex, a family history of varicose veins, obesity,
pregnancy, phlebitis, previous leg injury and behavioural factors
such as prolonged standing and perhaps a sitting posture at work
(6,7). At the initiative of the Union
Internationale de Phlébologie, a large-scale international survey
named Vein Consult Program (VCP) was carried out in 20 countries.
The VCP concluded that the worldwide presence of CVD was 83.6% and
the study underlined the importance of adequate screening for CVD
and training of both GPs and specialist physicians (1). The main goal of CVD treatment is
reducing the symptoms (heaviness, leg pains, oedema and swelling)
and improving the patient's quality of life (QoL), which is
affected in many patients. QoL can be defined as the functional
effect of the disease, respectively of the treatment of the
disease, as perceived by the patient (8) and there are specific validated scales
which are able to collect data regarding different QoL
parameters.
It is well-known that CVD negatively impacts the
well-being of the patients, both at the physical and the
psychological levels, nevertheless there is still a paucity of
scientific data regarding the impact of CVD on QoL, and according
to our knowledge, there is no other epidemiological research
performed in Romania to evaluate the impact of newly diagnosed CVD
on all CIVIQ-20 items regarding quality of life.
Materials and methods
The study was multicentre, prospective and
observational and took place in Romania, based on a transversal
method. In this study adult patients were recruited by 110
investigators, located in Romania's urban area. The recruitment
took place in June to August 2016 and included 1,893 patients. The
investigators were general practitioners (GPs) selected in
compliance with national regulations, in a randomly manner, and the
purpose of this study was to collect information about CVD
presence, demographic data, frequency of disease's signs and
symptoms, associated risk factors, therapeutic management practice
and impact on QoL parameters of patients with diagnosed with
CVD.
The investigators' responsibility was to establish
and maintain a treatment compliant with current medical practice
guidelines and in the best interest of the patient. In this study,
no medical analyses or specific treatments were prescribed, thus
the patients' care was not influenced by the participation in this
study.
Each investigator included 18 consecutive patients
who attended the practice for various reasons. Patients selection
was based on the following criteria: Patients with the minimum age
at inclusion 18 years, newly diagnosed with CVD or patients
diagnosed with CVD, but without treatment for CVD within the last
past 6 months, or prior inclusion. Patients attending for emergency
visits were excluded. Informed consent was obtained from each
participant.
The study visit consists in an initial GP interview
regarding age, sex, height, weight, BMI, occupation, reason for
addressing GP, level of daily physical activity, hours spent
standing and sitting. For women additional data regarding number of
births, as well as the use of hormonal replacement therapy and/or
birth control pills was recorded.
Data regarding presence of CVD symptoms were
recorded and their magnitude was self-evaluated by each of the
patients on a VAS scale (heavy legs, pain in the legs, sensation of
swelling or burning, night cramps). The time when symptoms occurred
at highest intensity, as well as the other possible CDV signs
noticed during clinical examination (oedema, spider veins, varicose
veins, skin modifications, or ankle ulcers) were recorded. For each
patient the GPs evaluated the clinical, aetiological, anatomical
and pathophysiological (CEAP) clinical stages by visual
examination. In addition, CVD therapeutic management
recommendations and duration of prescribed treatment was
recorded.
Each patient completed the CIVIQ-20 questionnaire
regarding QoL. CIVIQ-20 is a reliable, validated instrument
valuable in assessing the treatment effects in longitudinal,
multinational studies of patients with chronic venous disease
(9).
Based on the results of the CIVIQ 20 questionnaire
the Global Index Score (GIS) was calculated as the difference
between the final score and the minimum possible score, divided by
the difference between the theoretical maximum and minimum scores,
multiplied by 100. The formula used was the following: GIS =
[(Final score - minimal possible score)/(Theoretical maximal -
minimal score)] × 100. The score ranges from 0 to 100 (10).
The observational study was approved by the National
Agency for Medicines and Medical Devices (NAMMD) and received
positive opinion from the National Bioethics Committee for Medicine
and Medical Devices (NBCMMD).
Statistical analysis
Statistical analysis was performed with SPSS version
15 (SPSS Inc., Chicago, IL, USA) and included the following:
descriptive analysis, Mann-Whitney U tests, Chi-square test and
ANOVA with Turkey's post hoc test.
The scales variables were reported with mean and
standard deviation, and summarize categorical variables using
frequencies and percentages. To investigate the relationship
between CEAP classification, symptoms and impact on QoL, a logistic
regression was performed. P-value <0.05 was considered to
indicate a statistically significant difference.
Results
In total 1,893 patients were included in the
observational study carried out in Romanian urban area. Most of the
patients included were females (79.08%) and 50.4% of patients
belonging to age group (51–70 years). The average BMI was 27.9±5.03
with no statistical sex difference.
Of the subjects 66.72% were enrolled in the study
during visit to the family doctor's office for another disease,
while only 18.86% of patients were enrolled during a visit for CVD
consultation. Risk factors were present for most patients: prolong
sitting (≥5 h/day) (42.02% females, 46.7% males), prolonged
standing (≥5 h/day) (44.4% females, 45.7% males). The CEAP
classification placed most of the patients in C3 class (31.85%),
followed by C2 class (28.00%), C1 class (21.02%) and C4a (8.87%)
(Table I).
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | % |
|---|
| Age (years) |
|
<30 | 2.80 |
|
30–50 | 29.11 |
|
51–70 | 50.40 |
|
>70 | 17.70 |
| Sex |
|
Female | 79.08 |
| Male | 20.92 |
| BMI
(kg/m2) | 27.09±5.03 |
| Level of
activity |
|
Inactive | 34.07 |
|
Active | 32.91 |
|
Mixed | 33.02 |
| Regular exercise
taken | 9.20 |
| Main reason for
visiting the physician |
| Medical
consult for other disease | 66.72 |
| Medical
consult for chronic venous disease | 18.86 |
| Medical
consult for hemorrhoidal disease | 2.32 |
|
Administrative matter | 12.10 |
| Among women
(N=1,497) |
| No. of births |
| 0 | 11.49 |
| 1 | 36.47 |
| 2 | 38.68 |
|
>2 | 13.36 |
| Current use of
hormonal replacement therapy | 2.47 |
| Current use of birth
control pills | 5.95 |
|
| Risk
factors | Female
(%) | Male (%) | Total (%) |
|
| Prolonged sitting
position (h/day) |
|
<5 | 57.98 | 53.28 | 57.00 |
| 5–10 | 35.74 | 37.12 | 36.03 |
|
>10 | 6.28 | 9.60 | 6.97 |
| Prolonged standing
position (h/day) |
|
<5 | 55.51 | 54.29 | 55.26 |
| 5–10 | 37.34 | 37.63 | 37.40 |
|
>10 | 7.15 | 8.08 | 7.34 |
|
| CEAP
classification | N | % |
|
| C0s
(symptomatic) | 104 | 5.49 |
| C1 | 398 | 21.02 |
| C2 | 530 | 28.00 |
| C3 | 603 | 31.85 |
| C4a | 168 | 8.87 |
| C4b | 44 | 2.32 |
| C5 | 41 | 2.17 |
| C6 | 5 | 0.26 |
Only 9.2% of patients enrolled in the study take
regular physical activity, being a significant sex difference in
favour of male population (P<0.05).
The most frequent CVD symptoms reported were heavy
leg sensation (85.74%), followed by swelling of the feet (77.28%)
and pain (73.11%) and ‘restless’ feet (72.42%), which occurred most
often in the evening or after prolonged standing or sitting and
during summer. Most of the patients reported ‘low’ or ‘moderate’
intensity of the CVD symptoms, 73.01% of the patients reported the
presence of more than 3 concomitant CVD symptoms. The most frequent
CVD signs were telangiectasia and reticular veins (79.19%),
varicose veins (65.77%) and edema (53.35%) (Table II).
| Table II.CVD signs and symptoms. |
Table II.
CVD signs and symptoms.
| Most common CVD
symptoms | N | % | VAS |
|---|
| Feeling heavy
legs | 1,604 | 85.74 | 5.3±1.83 |
| Sensation of
swelling | 1,445 | 77.28 | 5.0±1.89 |
| Pain in the calf | 1,376 | 73.11 | 5.0±1.96 |
| Burning in the
calf | 851 | 45.85 | 4.7±1.96 |
| Cramps in the
calf | 1,134 | 60.38 | 4.8±1.97 |
| Tingling in the
feet |
931 | 49.76 | 4.6±1.89 |
| ‘Tired’ or
‘restless’ feet | 1,359 | 72.42 | 5.1±1.90 |
| Time when CVD
symptoms appear at highest intensity |
| At the
end of the day |
| 51.93 |
|
| After
long periods of orthostatic position |
| 82.14 |
|
| During
the night |
| 39.67 |
|
| After a
long period of sitting on a chair |
| 51.61 |
|
| During
the summer |
| 58.21 |
|
| After
warm baths |
| 26.47 |
|
| While
walking |
| 34.28 |
|
|
Premenstrual |
| 7.71 |
|
|
Others |
| 6.18 |
|
| CVD signs observed
during the clinical examination |
|
Telangiectasia, reticular
veins |
| 79.19 |
|
|
Varicose veins |
| 65.77 |
|
|
Edema |
| 53.35 |
|
| Skin
changes (lipodermatosclerozis) |
| 14.90 |
|
| Skin
changes (white atrophy) |
| 5.18 |
|
|
Ulcer |
| 2.59 |
|
| Number of CVD
symptoms currently present |
|
None |
| 2.96 |
|
| 1 |
| 3.75 |
|
| 2 |
| 6.71 |
|
| 3 |
| 13.58 |
|
| >3 |
| 73.01 |
|
Patients received the following treatment
recommendation from GPs: lifestyle advice (99.21% of patients)
(most frequent advice given was to avoid long standing or sitting
periods (95.56%), to wear proper shoes (80.51%) and to practice
regular physical activities (80.14%); systemic treatment (96.21% of
patients) with the most recommended systemic treatment being MPFF
(48.39%), followed by diosmin + micronized hesperidin (21.52%);
local treatment recommendation was received by 73.01% of the
patients, while 30.74% of the patients were referred to a venous
specialist.
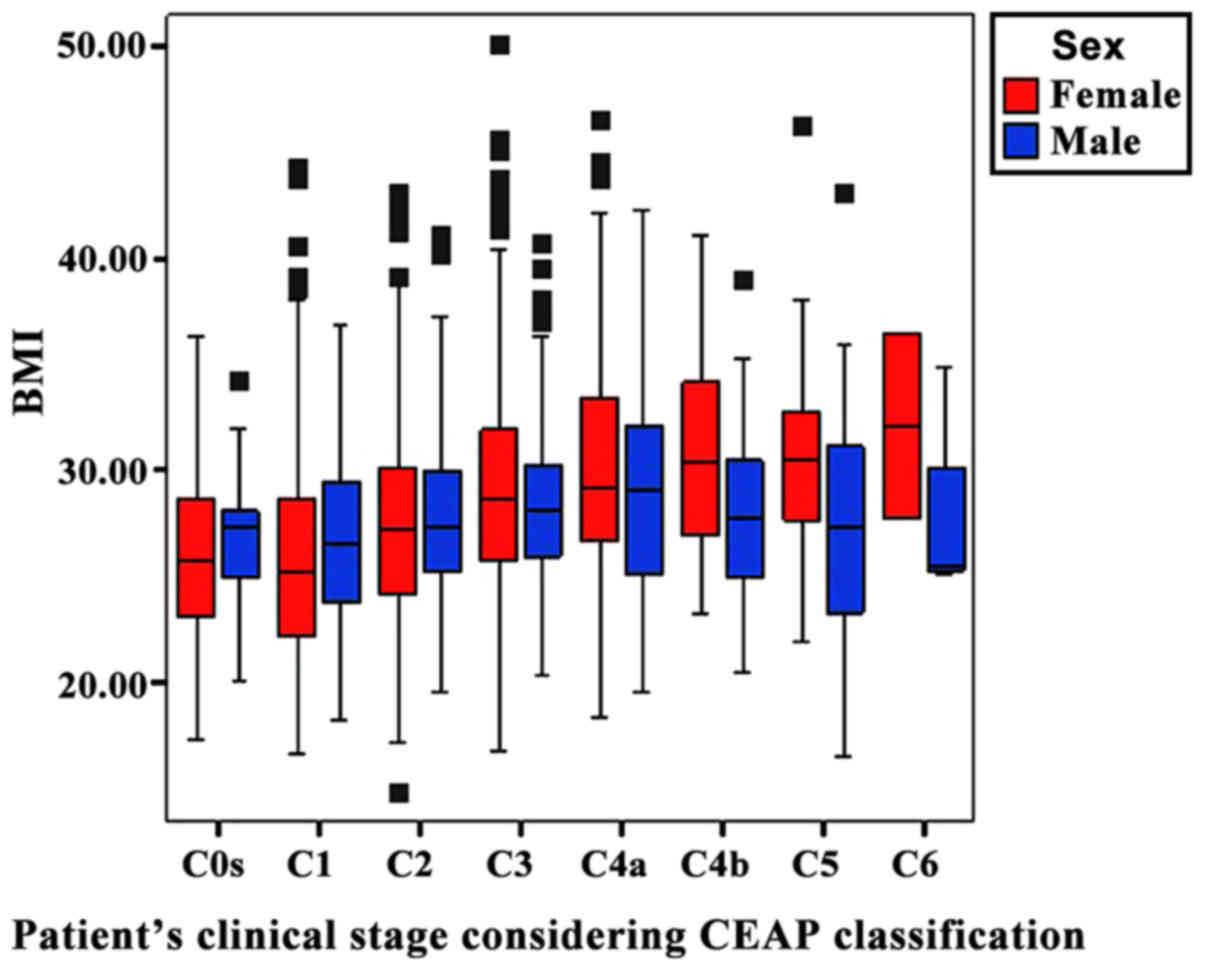
Based on Mann-Whitney U tests, it was noted that
CEAP C-classification of CVD was significantly higher for females
compared to males (P<0.001). In addition, a significant positive
correlation was observed between BMI and CVD C-class, but only for
females (P<0.001) (Fig. 1).
A positive correlation was observed between the
number of symptoms reported and the CEAP C-class (P<0.001) as
well as the intensity of symptoms measured on VAS and CVD CEAP
C-class (Table III).
| Table III.CVD symptoms intensity measured on
VAS. |
Table III.
CVD symptoms intensity measured on
VAS.
|
| Symptom intensity
measured on VAS (cm) |
|---|
|
|
|
|---|
|
C-classification | Feeling of heavy
legs | Sensation of
swelling | Pain in the
calf | Burning in the
calf | Cramps in the
calf | Tingling in the
feet | ‘Tired’ or
‘restless’ feet |
|---|
| C0s | 4.56±1.52 | 4.31±1.62 | 4.46±1.41 | 3.87±0.90 | 3.97±1.44 | 4.19±1.77 | 4.49±1.54 |
| C1 | 4.44±1.79 | 4.12±1.95 | 4.06±2.03 | 4.05±1.95 | 4.09±1.98 | 4.21±2.06 | 4.39±1.84 |
| C2 | 5.12±1.90 | 4.62±1.77 | 4.85±1.96 | 4.52±2.03 | 4.59±1.96 | 4.24±1.81 | 4.89±1.80 |
| C3 | 5.53±1.67 | 5.28±1.73 | 5.29±1.77 | 4.82±1.93 | 4.99±1.91 | 4.69±1.77 | 5.37±1.86 |
| C4a | 5.87±1.58 | 5.76±1.80 | 5.50±1.85 | 5.03±1.69 | 5.34±1.80 | 4.81±1.70 | 5.52±1.96 |
| C4b | 6.43±1.59 | 6.24±1.75 | 6.43±1.90 | 5.54±1.86 | 5.62±1.72 | 5.67±1.99 | 6.05±1.93 |
| C5 | 6.57±1.67 | 6.74±1.80 | 6.46±1.97 | 5.63±2.17 | 5.93±2.22 | 5.55±2.18 | 6.21±1.92 |
| C6 | 7.20±1.92 | 7.20±1.48 | 7.40±2.51 | 6.50±2.65 | 6.60±1.34 | 6.80±2.39 | 7.00±1.58 |
| P-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
All patients completed the CIVIQ-20 questionnaire
regarding quality of life and the results were translated into the
GIS. The GIS median value for the entire group was 30.48±18.23,
with no significant sex difference. A significant positive
correlation was found between GIS value and CVD C-class, for both
sexes, as well as for the total group (P<0.001) (Table IV). A significant positive
correlation was found between the number of symptoms and the GIS,
for the total group of patients (P<0.001).
| Table IV.CIVIQ-20 global index score vs.
C-class. |
Table IV.
CIVIQ-20 global index score vs.
C-class.
|
C-classification | N | CIVIQ-20 global
index score | N (female) | CIVIQ-20 global
index score (female) | N (male) | CIVIQ-20 global
index score (male) |
|---|
| C0s | 104 | 19.65±12.65 | 85 | 20.43±12.07 | 19 | 16.18±14.86 |
| C1 | 398 | 18.59±13.28 | 335 | 18.60±12.93 | 63 | 18.55±15.11 |
| C2 | 530 | 28.15±15.18 | 414 | 29.09±14.93 | 116 | 24.82±15.66 |
| C3 | 603 | 33.96±15.88 | 490 | 34.28±15.44 | 113 | 32.57±17.66 |
| C4a | 168 | 43.70±18.27 | 119 | 45.35±17.22 | 49 | 39.69±20.23 |
| C4b | 44 | 58.41±13.95 | 29 | 59.40±14.09 | 15 | 56.50±13.97 |
| C5 | 41 | 62.44±15.45 | 23 | 62.28±14.33 | 18 | 62.64±17.21 |
| C6 | 5 | 76.25±8.24 | 2 | 83.13±9.72 | 3 | 71.67±3.15 |
| Total | 1893 | 30.48±18.23 | 1497 | 30.41±17.63 | 396 | 30.73±20.36 |
| P-value |
| <0.001 |
| <0.001 |
| <0.001 |
QoL was affected for most of the patients in ‘a
mild’ or ‘moderate’ degree, being noticed as a significant negative
impact on all physical, psychological, and social functioning and
pain components of CIVIQ-20. The impact on each CIVIQ-20 items was
positively correlated with severity of CVD CEAP class
(P<0.001).
Discussion
CVD is a common problem among the adult population
and has a significant impact on individuals and the entire health
care system. Chronic vein abnormalities are present in up to 50% of
individuals (2,3,11,12).
However, estimates of prevalence rates of chronic venous disease
vary depending upon the population studied (13). In Romania, Vein Direction study
showed that, in June-July 2015, the ratio of newly diagnosed CVD
cases was 369.5 for every 1,000 patients and the recorded CVD
prevalence during this period was 68.40% (14).
Nevertheless, without a proper CVD management,
patients might reach the stage where they will no longer be able to
perform daily activities and higher CEAP classification indicates a
higher socioeconomic problem. In case CVD pathology is associated
with other pathologies, mainly diabetes mellitus, the CVD ulcers
could become extremely difficult to treat (15). In addition to CVD impact, for those
patients, the diabetic neuropathy is associated with a whole range
of local and general complications that inflict important health
care costs and reduce the patient's quality of life (16).
One recent study demonstrated that female subjects
with cardiometabolic risk factors or female diabetic patients are
at greater risk of developing early chronic venous disorder than
the male subjects (17),
nevertheless the factors that determine whether a given patient
will progress from mild to more severe form of CVD remain largely
unknown.
An important aspect regarding the present
observational study is that according to the inclusion criteria all
patients were previous or during the current GP visit diagnosed
with CVD. Despite this, only 18.86% of patients visited the GPs for
‘medical consultation for CVD’, confirming the low addressability
rate, which was detected also in previous observational studies.
The GPs referred 30.7% of the patients to a vein specialist, most
of the referred patients being classified with a higher C-class,
fact that is suggestive for trying a conservative treatment in
early stage of CVD and most of the patients received lifestyle
advice, as well as venoactive pharmacological treatment. Another
important aspects that need to be considered are the CVD prevention
measurements, as well as the patient's adherence to the medical
treatment. Use of textile biomaterials in patients with high risks
in developing CVD, might be an efficient method of preventing the
disease (18). On the other hand,
for increasing patient treatment adherence the pharmacist plays an
important role, by delivering correct and complete information that
will enable patients to take correct decisions (19).
Patients who addressed GPs for ‘other medical
consultation’ presented CVD signs consistent with an advance stage
of CVD, suggesting that patients are ignoring the CVD signs and are
visiting physicians in a late phase of CVD, despite of the fact
that their quality of life was profoundly affected.
The study proved that CVD diagnosis was established
with a relative delay, most of the patients being initially
diagnosed as CEAP-class C3. This might suggest that additional to
encouraging patients to address physicians earlier, specialized
training is needed for GPs in order to detect CVD signs at earlier
stage and implement therapeutic management as early as possible. A
similar conclusion regarding adequate screening and additional
training for physicians was reached by the Vein Consult Program
(1).
For this observational study the CVD was classified
by using only the C (clinical) part of CEAP and classification was
done by GPs, who are not routinely using the CEAP classification.
This fact could link to a moderate reproducibility of data, as
already described in the literature (20).
Obesity, due to increased abdominal pressure that
leads to a greater reflux, increased venous pressure and vein
diameter, represents a high impact CVD risk factor, together with
the lack of regular physical exercise (21). In the present study a positive
significant correlation was observed between BMI, and the severity
of CVD for the female group, but not for the male group.
During the study it was noted that female population
had a significantly higher C-class compared with men, fact similar
with other data in the literature (22).
In the present study 97.04% of all enrolled patients
reported at least one CVD symptom, and 73.01% of patients reported
more than 3 concomitant symptoms. The most common symptoms were
heavy legs (85.74%), sensation of swelling feet (77.28%) and pain
in the calf (73.11%), followed by cramps in the calf (60.38%). A
positive correlation was observed between the number of symptoms
reported and the CEAP C-class as well as the intensity of symptoms
measured on VAS (cm) and CVD CEAP C-class.
A positive significant correlation was found between
the severity of CVD C-class and degree in which quality of life is
affected (GIS). QoL was affected even in the very early stage of
CVD (namely C0s) and with the first symptom reported.
Quality of life was affected to a certain degree for
almost all patients, even for those included by physicians in CEAP
C0s class, were patients reported moderate or even considerable
pain.
It is known that chronic leg ulcers due to their
recurrent nature, difficult-to-treat and the long-term therapy
required for healing are high resources consumer for the healthcare
systems, as well as they impact on patient's quality of life in a
prohibitive manner (23). When
patients with chronic ulcer were analysed, a very severe impact on
quality of life level was noted correlating with depression
symptoms which were commonly present. Similarly, a systematic
review conducted by Herber et al concluded that patients
with leg ulcers have significantly higher levels of pain,
limitations regarding functional and social activities correlated
with lower vitality and emotional limitations (24).
All CIVIQ-20 items (physical, psychological, social
and pain) were affected for most of the patients, and the degree in
which they were affected was positively correlated with CVD
severity CEAP class, is suggestive of the magnitude of CDV impact
on patients' life.
Acknowledgements
OV received honoraria for the interpretation of
data.
Funding
The observational study was funded by Servier Pharma
(Bucharest, Romania).
Availability of data and materials
The datasets generated and/or analysed during the
present study are not publicly available due to the fact that they
belong to Servier, as Sponsor of the study, but are available from
the corresponding author on reasonable request, and with prior
permission of Servier.
Authors' contributions
DEB, TF, SB, IAM contributed to the acquisition of
the data and critical revision of manuscript for important
intellectual content. OV was responsible for the analysis of the
patient data and contributed to writing the manuscript. All authors
read and approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the National
Bioethics Committee of Medicines and Medical Devices (NBCMMD;
approval no. 15 SNI; Bucharest, Romania), and written informed
consent was obtained from each participant.
Patient consent for publication
Not applicable.
Competing interests
IAM is an employee of Servier Pharma Romania. The
other authors declare that they have no competing interests.
References
|
1
|
Rabe E, Guex JJ, Puskas A, Scuderi A,
Fernandez Quesada F and Coordinators VC: VCP Coordinators:
Epidemiology of chronic venous disorders in geographically diverse
populations: Results from the Vein Consult Program. Int Angiol.
31:105–115. 2012.PubMed/NCBI
|
|
2
|
Callam MJ: Epidemiology of varicose veins.
Br J Surg. 81:167–173. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Evans CJ, Fowkes FG, Ruckley CV and Lee
AJ: Prevalence of varicose veins and chronic venous insufficiency
in men and women in the general population: Edinburgh Vein Study. J
Epidemiol Community Health. 53:149–153. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Beebe-Dimmer JL, Pfeifer JR, Engle JS and
Schottenfeld D: The epidemiology of chronic venous insufficiency
and varicose veins. Ann Epidemiol. 15:175–184. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kaplan RM, Criqui MH, Denenberg JO, Bergan
J and Fronek A: Quality of life in patients with chronic venous
disease: San Diego population study. J Vasc Surg. 37:1047–1053.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jawien A: The influence of environmental
factors in chronic venous insufficiency. Angiology. 54 Suppl
1:S19–S31. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lacroix P, Aboyans V, Preux PM, Houlès MB
and Laskar M: Epidemiology of venous insufficiency in an
occupational population. Int Angiol. 22:172–176. 2003.PubMed/NCBI
|
|
8
|
van Korlaar I, Vossen C, Rosendaal F,
Cameron L, Bovill E and Kaptein A: Quality of life in venous
disease. Thromb Haemost. 90:27–35. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Launois R, Mansilha A and Jantet G:
International psychometric validation of the Chronic Venous Disease
quality of life Questionnaire (CIVIQ-20). Eur J Vasc Endovasc Surg.
40:783–789. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
CIVIQ Users' Guide: Calculation of the
global index score. https://www.civiq-20.com/scoring-missing-data/calculation-global-index-scoreAugust
27–2017
|
|
11
|
Zahariev T, Anastassov V, Girov K,
Goranova E, Grozdinski L, Kniajev V and Stankev M: Prevalence of
primary chronic venous disease: The Bulgarian experience. Int
Angiol. 28:303–310. 2009.PubMed/NCBI
|
|
12
|
Brand FN, Dannenberg AL, Abbott RD and
Kannel WB: The epidemiology of varicose veins: The Framingham
Study. Am J Prev Med. 4:96–101. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Criqui MH, Jamosmos M, Fronek A, Denenberg
JO, Langer RD, Bergan J and Golomb BA: Chronic venous disease in an
ethnically diverse population: The San Diego Population Study. Am J
Epidemiol. 158:448–456. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Feodor T, Vittos O and Mitea L: Chronic
venous disease in Romania: An epidemiological study. Int Angiol. 35
(Suppl 1):632016.
|
|
15
|
Nwabudike LC and Tatu AL: Magistral
prescription with silver nitrate and Peru Balsam in difficult to
heal diabetic foot ulcers. Am J Ther. Jun 13–2017.(Epub ahead of
print). doi: 10.1097/MJT.0000000000000622. View Article : Google Scholar
|
|
16
|
Căruntu C, Negrei C, Boda D, Constantin C,
Căruntu A and Neagu M: Biotechnological advances for diagnosis of
peripheral diabetic neuropathy. Rom Biotechnol Lett. 19:9846–9858.
2014.
|
|
17
|
Zhong J, Chen J, Zhao ZG, He HB, Yan ZC,
Liu DY, Zhu ZM and Ni YX: Diabetes mellitus is associated with
early chronic venous disorder of the lower extremities in Chinese
patients with cardiometabolic risk factors. Diabetes Metab Res Rev.
30:505–512. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brănișteanu DE, Nichifor M, Dorobăț CM,
Brănișteanu DC, Petrariu FD, Molodoi AD, Radu DC and Boda D: Use of
textile biomaterials for the topic treatment of chronic venous
disease. Rom Biotechnol Lett. 20:10618–10625. 2015.
|
|
19
|
Ratiu MP, Purcarea I, Popa F, Purcarea VL,
Purcarea TV, Lupuleasa D and Boda D: Escaping the economic turn
down through performing employees, creative leaders and growth
driver capabilities in the Romanian pharmaceutical industry.
Farmacia. 59:119–130. 2011.
|
|
20
|
Sinabulya H, Holmberg A and Blomgren L:
Interobserver variability in the assessment of the clinical
severity of superficial venous insufficiency. Phlebology. 30:61–65.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
van Rij AM, De Alwis CS, Jiang P, Christie
RA, Hill GB, Dutton SJ and Thomson IA: Obesity and impaired venous
function. Eur J Vasc Endovasc Surg. 35:739–744. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vuylsteke ME, Thomis S, Guillaume G,
Modliszewski ML, Weides N and Staelens I: Epidemiological study on
chronic venous disease in Belgium and Luxembourg: Prevalence, risk
factors, and symptomatology. Eur J Vasc Endovasc Surg. 49:432–439.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Scott TE, LaMorte WW, Gorin DR and
Menzoian JO: Risk factors for chronic venous insufficiency: A dual
case-control study. J Vasc Surg. 22:622–628. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Herber OR, Schnepp W and Rieger MA: A
systematic review on the impact of leg ulceration on patients'
quality of life. Health Qual Life Outcomes. 5:442007. View Article : Google Scholar : PubMed/NCBI
|