Introduction
During the process of surgery, perioperative massive
hemorrhage is also a major problem needed to be solved first in the
clinic (1). Most patients will cause
a disorder of coagulation function due to the traumatic invasive
surgery (2). Moreover, the patient
is extremely prone to have massive hemorrhage, which endangers the
patient's life and health (3). In
clinic, a patient who is in the perioperative period is required to
provide timely blood products to supplement the normal blood
circulation in the patient (4). When
facing the problem how to choose the most appropriate opportunity
of blood transfusion, the most traditional method in clinic is to
estimate whether the patient's coagulation function and erythrocyte
function are abnormal or not (5).
However, at present, with the continuous increase of difficult
diseases, the defects of traditional detection methods are becoming
more and more obvious. For example, the timeliness and
effectiveness of the detection are poor, and real-time blood
function detection cannot be achieved (6). When facing the situation of sudden
massive hemorrhage, an effective prejudgment cannot be made, which
may lead to excessive blood loss and threaten patient's life
(7). Therefore, research on how to
detect the coagulation function of the patient in real-time in
clinic is urgent and a major breakthrough is required.
With the continuous development of modern medical
technology, thromboelastography (TEG) was developed. TEG can draw
changeable images according to the dynamic changes of patient's
coagulation function and can accurately and integrally estimate the
general situation of coagulation function and the formation of
thrombus of patient, and the monitoring is convenient and fast
(8,9). Since 2015, the surgical department of
our hospital have widely used TEG as the judgment indicator for the
perioperative blood transfusion of patients, and now enough
research cases have been accumulated. Τhe value of TEG in
perioperative clinical blood transfusion is researched through
retrospective analysis, and the purpose is to provide effective
reference and guidance when choosing the opportunity of blood
transfusion of patient in clinic in the future.
Patients and methods
General data
Seventy-four patients, who were admitted by the
surgical department in the First Hospital of Zibo (Zibo, China)
from March 2015 to March 2018, were selected for the study and were
retrospectively analysed. There were 43 males and 31 females, aged
from 29 to 67 years, and the average age was 48.94±10.54 years.
Inclusion criteria: All patients had surgery in the hospital;
patient condition assessment before anesthesia was in the grade
from I to II according to ASA (10);
intraoperative blood loss >1,000 ml; patients had complete case
data; patients were willing to cooperate with the hospital for the
investigation work. Exclusion criteria: Patients had severe organ
failure; patients had blood diseases that may affect coagulation
function; patients took anticoagulant or antiplatelet drugs in
recent 2 months; patients had emergency operations; patients had
liver dysfunction; patients were transferred to other hospitals;
patients had mental illness.
This study was approved by the Ethics Committee of
the First Hospital of Zibo (Zibo, China). Patients who participated
in this research had complete clinical data. The signed informed
consents were obtained from the patients or the guardians.
Grouping methods
Of the 74 patients, only 34 patients took the
traditional coagulation function testing method as the blood
transfusion guide during the perioperative period and they were
regarded as the control group. The other 40 patients used TEG as
the blood transfusion guide during the perioperative period and
they were regarded as the TEG group.
Operation methods
The anesthesia induction, intraoperative anesthesia
maintenance and operation of the patients in the two groups were
completed by the senior clinicians in the hospital, and the
operation methods of the same kind of diseases were consistent.
Blood transfusion methods
The control group: Blood gas analysis, the test of
coagulation function and blood routine function were carried out
respectively before and after the operation (the interval was 1 h),
when Hb <70 g/l and Hct <25%, 2 units of the suspended
erythrocytes was added; when PLT <50×109 U/l, 1 unit
of platelets was added; 2 g of fibrinogen was added when fibrinogen
was <1.2 mg/dl. The TEG group: TGE detector (purchased from
American Haemoscope company, TEG5000 thromboelastograph) was used
for real-time monitoring based on the monitoring of the control
group; when R value was >10 min, it indicated that the clotting
factor was reduced, and the frozen plasma (15 ml/kg) was added;
when MA value was >70 min, 1 unit of platelets was added; when
Angle value was >72 degrees, 2 g of fibrinogen was added.
Observation indicators
The coagulation function indicators of the patients
in the two groups in 2 h before the operation and in 24 h after the
operation were: Hb, APTT, Pt, Hct, Plt, Fib; intraoperative
transfusion amount and intraoperative blood loss of the patients in
the two groups; the condition of blood transfusion of the patients
in the two groups during the perioperative period: the suspended
erythrocyte, fibrinogen, Plt, the condition of plasma use; the
clinical results of the patients in the two groups: The occurrence
rate of the postoperative rebleeding, the length of hospital stay
and mortality.
Statistical methods
The data were analysed and processed by using SPSS
24.0 statistical software (IBM Corp., Armonk, NY, USA); the
enumeration data were expressed in the form of a rate; the
comparison between the groups was performed by using Chi-square
test; the measurement data were expressed as the mean ± standard
deviation and the comparison between the groups was performed by
using t-test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Comparison of the general data
The age, weight, BMI, preoperative blood routine
indicators, operation time, sex, ASA grade and the type of
operation were compared between the two groups, and no significant
difference (P>0.050) was found, indicating that the patients in
the two groups were comparable (Table
I).
 | Table I.Comparison of the clinical data of the
patients in the two groups [n (%)]. |
Table I.
Comparison of the clinical data of the
patients in the two groups [n (%)].
| Data | TEG group (n=40) | Control group
(n=34) | χ2 or t
value | P-value |
|---|
| Age (years) | 48.14±9.16 | 49.07±9.86 | 0.420 | 0.676 |
| Weight (kg) |
62.18±15.67 |
63.14±14.89 | 0.269 | 0.789 |
| BMI
(kg/m2) | 21.24±6.24 | 21.54±6.17 | 0.207 | 0.837 |
| Preoperative WBC
(×109/l) |
3.16±2.54 |
3.08±2.49 | 0.136 | 0.892 |
| Preoperative RBC
(×1012/l) |
4.07±1.14 |
4.15±1.08 | 0.308 | 0.759 |
| Preoperative PLT
(×109/l) | 167.24±50.14 | 172.33±42.86 | 0.465 | 0.644 |
| Operation time
(min) | 138.14±34.86 | 142.27±38.12 | 0.487 | 0.628 |
| Sex |
|
| 0.128 | 0.721 |
| Male | 24 (60.00) | 19 (55.88) |
|
|
|
Female | 16 (40.00) | 15 (44.12) |
|
|
| Living
environment |
|
| 0.003 | 0.956 |
| City | 28 (70.00) | 24 (70.59) |
|
|
|
Countryside | 12 (30.00) | 10 (29.41) |
|
|
| ASA |
|
| 0.085 | 0.771 |
| I
grade | 19 (47.50) | 15 (44.12) |
|
|
| II
grade | 21 (52.50) | 19 (55.88) |
|
|
| Type of
operation |
|
| 0.171 | 0.918 |
|
Orthopedic operation | 17 (42.50) | 14 (41.18) |
|
|
| Surgical
operation | 16 (40.00) | 15 (44.12) |
|
|
| Other
operation | 7
(17.50) | 5
(14.71) |
|
|
Comparison of coagulation function
before and after the operation
When comparing the coagulation function indicators
of the patients in the two groups in 2 h before the operation and
in 24 h after the operation, it was shown that there was no
significant difference between the two groups (P>0.050).
However, APTT and Pt of the patients in the two groups both
increased when compared with those before the treatment
(P<0.050) and Hb, Hct, Plt and Fib both decreased (P<0.050)
(Table II).
| Table II.The comparison of coagulation function
indicators before and after the operation. |
Table II.
The comparison of coagulation function
indicators before and after the operation.
| Index | TEG group (n=40) | Control group
(n=34) | t value | P-value |
|---|
| In 2 h before the
operation |
| Hb
(g/l) | 131.14±14.01 | 128.63±13.42 | 0.783 | 0.436 |
|
APTT(s) | 31.07±3.15 | 31.24±2.95 | 0.238 | 0.812 |
|
Pt(s) | 11.05±0.94 | 10.98±0.76 | 0.348 | 0.729 |
| Hct
(%) | 35.68±5.14 | 37.21±5.06 | 1.285 | 0.203 |
| Plt
(g/l) | 207.63±66.54 | 211.08±70.52 | 0.216 | 0.829 |
| Fib
(g/l) | 3.98±0.26 | 3.93±0.29 | 0.782 | 0.437 |
| In 24 h after the
operation |
| Hb
(g/l) |
96.14±7.05a |
95.23±8.14a | 0.515 | 0.608 |
|
APTT(s) |
35.08±4.66a |
33.87±5.24a | 1.051 | 0.297 |
|
Pt(s) |
16.23±2.51a |
15.14±3.01a | 1.700 | 0.094 |
| Hct
(%) |
26.96±6.56a |
27.08±7.12a | 0.075 | 0.940 |
| Plt
(g/l) |
142.37±69.52a |
146.72±72.37a | 0.263 | 0.793 |
| Fib
(g/l) |
3.08±0.49a |
2.96±0.55a | 0.992 | 0.324 |
Comparison of the condition of the
operation
There was no significant difference when comparing
the intraoperative blood loss of the patients in the two groups
(P>0.050), while the intraoperative transfusion amount in the
TEG group was 1,577.63±364.62 ml, which was significantly less than
the intraoperative transfusion amount in the control group
(2,574.46±514.63 ml), P<0.001 (Table III).
| Table III.The comparison of the condition of
the operation. |
Table III.
The comparison of the condition of
the operation.
| Index | TEG group
(n=40) | Control group
(n=34) | t value | P-value |
|---|
| Intraoperative
blood loss (ml) |
2,486.12±654.73 |
2,514.26±701.08 | 0.178 |
0.859 |
| Intraoperative
transfusion amount (ml) |
1,577.63±364.62 |
2,574.46±514.63 | 9.717 | <0.001 |
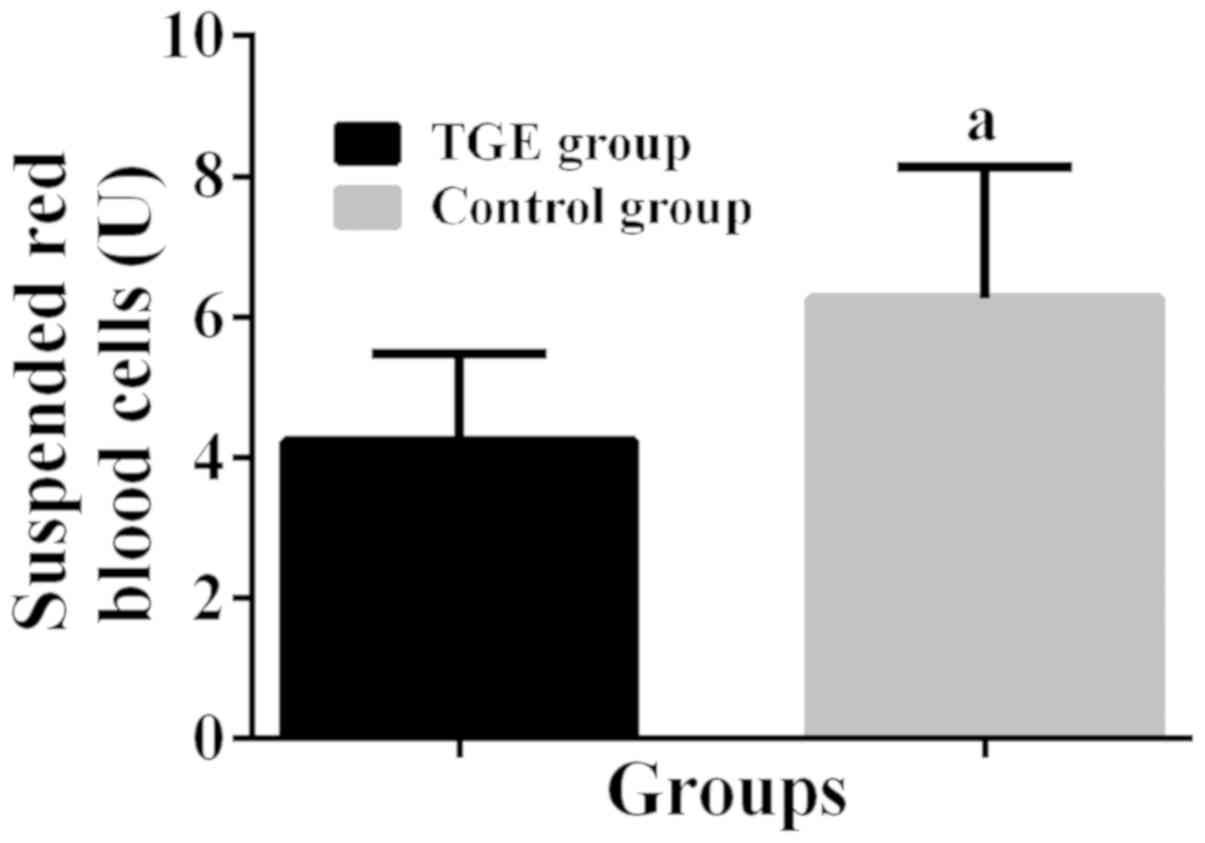
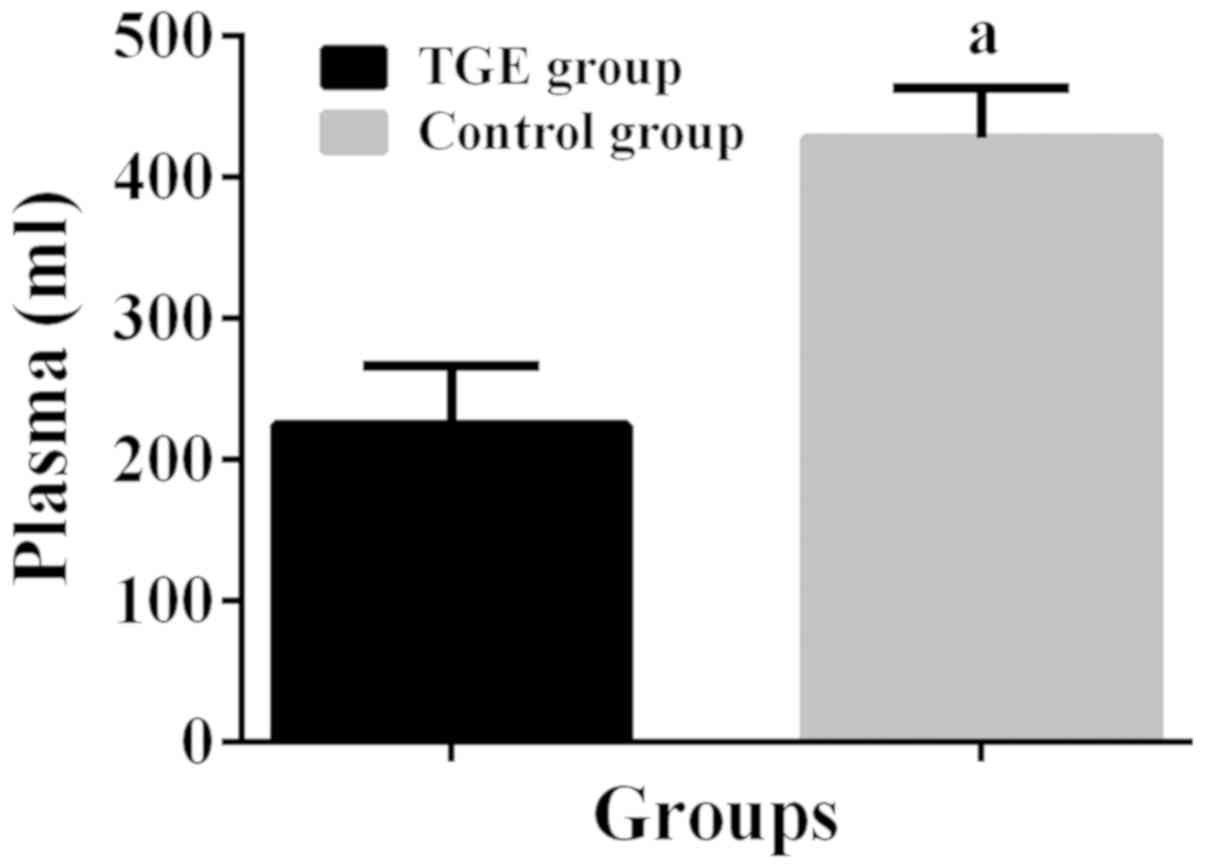
Comparison of the condition of the
blood transfusion
In the TEG group, 4.24±1.24 units of the suspended
erythrocytes was used during the perioperative period, which was
significantly less than that in the control group (6.27±1.86 units,
P<0.001); 1.94±0.75 units of Plt was used in the TEG group
during the perioperative period, which was significantly less than
that in the control group (3.42±1.24 units, P<0.001); 2.13±0.83
g of fibrinogen was used in the TEG group during the perioperative
period, which was significantly less than that in the control group
(3.24±1.22 g, P<0.001); 224.63±41.86 ml of plasma was used in
the TEG group during the perioperative period, which was
significantly less than that in the control group (427.86±35.14 ml,
P<0.001) (Figs. 1–4).
Comparison of the clinical
results
The length of hospital stay of the patients in the
TEG group was 16.24±2.16 days, which was significantly shorter than
that in the control group (18.96±5.62 days), P=0.006; there was no
significant difference when comparing the occurrence rate of the
postoperative rebleeding and mortality of the two groups
(P>0.050) (Table IV).
| Table IV.The comparison of the clinical
results of the patients in the two groups [n (%)]. |
Table IV.
The comparison of the clinical
results of the patients in the two groups [n (%)].
| Index | TEG group
(n=40) | Control group
(n=34) | χ2 or t
value | P-value |
|---|
| Length of hospital
stay (days) | 16.24±2.16 | 18.96±5.62 | 2.828 | 0.006 |
| Occurrence rate of
the postoperative rebleeding | 4
(10.00) | 7
(20.59) | 1.628 | 0.202 |
| Mortality | 1 (2.50) | 1 (2.94) | 0.014 | 0.907 |
Discussion
Coagulation function is the key to determine the
condition of perioperative bleeding of patient, and keeping
patient's coagulation function in a stable state is the fundamental
solution to reduce the occurrence of operating massive hemorrhage
in patients (11). During the
operation, traumatic invasive procedures, blood loss in
vitro, oxidative reaction in the body and the various aspects
of factors could cause coagulopathy in patient (12–14). The
blood circulation is a necessary part of the rehabilitation of
patient's body; slight damage of coagulation function causes the
prolongation of the rehabilitation cycle, and the treatment effect
is not good and serious damage of coagulation function endangers
patient's life and health (15). In
order to keep the patient's blood circulation operating normally,
perioperative blood transfusion is necessary and an extremely
important part (16). During the
process of perioperative blood transfusion, patients may have some
symptoms, such as low calcium, high potassium, and pH imbalance due
to the massive loss of clotting factors and platelets and the
infusion of erythrocyte suspension, and the anticoagulant infused
into the blood may also cause coagulation function becoming
abnormal again (17,18). Therefore, how to accurately assess
the blood transfusion amount and blood transfusion type of patient
during the perioperative period is a research hotspot in clinic.
The traditional blood routine and coagulation function have a low
detection mobility and their real-time monitoring ability is poor,
thereby they cannot meet the clinical accurate judgment for the
condition of patient's blood transfusion; TEG is the only effective
method to continuously and dynamically monitor the process of blood
coagulation when the blood transfusion amount is extremely low
(19,20). Not only does it have a good
monitoring effect on the changes in cells and plasma, but also have
a clear judgment on the generation time of blood clots (21). At present, there are still only a few
studies on TEG worldwide and few accurate references, which are on
TEG and can be used as a guide in clinic. Therefore, this study
aims to prove that the diagnostic value of TEG in the condition of
blood transfusion of the patients who are in the perioperative
period by comparing TEG and traditional blood coagulation
monitoring applied in the condition of blood transfusion of the
patients who are in the perioperative period.
The results of this study showed that there was no
significant difference in the inspection results of coagulation
function of the patients in the two groups in 2 h before the
operation and in 24 h after the operation, suggesting that TEG
would not affect the patient's coagulation function, such as the
traditional detection method, which was also available for the
patients who were in the perioperative period. When comparing the
intraoperative blood transfusion amount and intraoperative blood
loss in the two groups, it was shown that there was no significant
difference in the intraoperative blood loss of the patients in the
two groups, but the intraoperative blood transfusion amount in the
TEG group was significantly less than that in the control group.
Further comparison of the condition of the blood transfusion
between the two groups showed that the use of each infusion
solution of the patients in the TEG group was significantly lower
than that in the control group, which was consistent with the
results of Lawson et al (22). The length of hospital stay of the
patients in the TEG group was significantly lower than that in the
control group, and there was no significant difference when
comparing the occurrence rate of the postoperative rebleeding and
mortality in the TEG group with those in the control group,
suggesting that TEG could make a more accurate judgment on the
perioperative blood transfusion of patient. In terms of the
reasons, it was considered that during the monitoring process of
TEG, the generation time (R value) of the patient's blood clot was
used as the infusion basis of plasma; the maximum amplitude (MA
value) of the formation of thrombus was used as the infusion basis
of Plt, and the intensity (K value) of fibrinogen was used as the
infusion basis of fibrinogen (23,24),
which more reasonably and accurately guided the patient's
mathematical situation. Compared with the traditional coagulation
function test, TEG can infuse the targeted blood products into the
patients who are in the perioperative period, and accurately adjust
the improved condition of blood coagulation in patient's body
according to the quality of the blood transfusion to achieve the
purpose of significantly improving the coagulation function of
patient. TEG can comprehensively reflect the process, in which the
blood clot forms and fiber dissolves in the sample blood, and
reflect the interaction between clotting factors and platelets,
which has a more accurate judgment for patient's overall
coagulation condition (25).
Moreover, the generation speed of TEG monitoring results are
significantly faster than that of the traditional coagulation
function test, which helps to instruct doctors to make timely
decision and treatment for the blood transfusion. Since the
transfusion condition of the patients in the TEG group was more
accurate, it was speculated that this was one of the reasons why
the recovery period of the TEG group was shorter than that of the
control group. There was no statistical difference in the
postoperative rebleeding rate between the two groups, and it was
speculated that the reason for this was the experimental error,
which was caused by the small sample size; in terms of the actual
number of the patients, the patients in the TEG group were
significantly less than those in the control group.
The results of this experiment showed that TEG was
more suitable for estimating the blood transfusion of a patient who
was in the perioperative period when compared with the traditional
coagulation function test, but there were still some shortcomings.
For example, TEG is a test in vitro, and detecting
differences between patient and the internal environment in
patient's body may cause errors in the results of coagulation
function (e.g., the effects of patient's vascular endothelium and
vascular nose, on coagulation function); and the patient usually is
in anesthesia during the operation, also patient's body temperature
is low, which may have an effect on the results. The test result of
TEG for the general coagulation function of patient is better, but
it has a weaker ability to distinguish the abnormality in certain
coagulation process. Moreover, the number of cases included in this
study was small, and the statistical analysis of large data could
not be carried out.
In summary, compared with the traditional
coagulation function test, TEG is more accurate for estimating the
coagulation function of patient, and is more suitable for
estimating the condition of blood transfusion of patient in the
perioperative period; also, it can shorten the recovery period of
patient and it is worthwhile to promote in the clinic.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HS and BS conceived the study and drafted the
manuscript. JL and LW acquired the data. BS and GS analyzed the
data. HS and JL revised the manuscript. All authors revised, read
and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
the First Hospital of Zibo (Zibo, China). Patients who participated
in this research had complete clinical data. The signed informed
consents were obtained from the patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Clark NP, Douketis JD, Hasselblad V,
Schulman S, Kindzelski AL and Ortel TL; BRIDGE Investigators, :
Predictors of perioperative major bleeding in patients who
interrupt warfarin for an elective surgery or procedure: Analysis
of the BRIDGE trial. Am Heart J. 195:108–114. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Paparella D and Whitlock R: Safety of
salvaged blood and risk of coagulopathy in cardiac surgery. Semin
Thromb Hemost. 42:166–171. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Drolz A, Horvatits T, Roedl K, Rutter K,
Staufer K, Kneidinger N, Holzinger U, Zauner C, Schellongowski P,
Heinz G, et al: Coagulation parameters and major bleeding in
critically ill patients with cirrhosis. Hepatology. 64:556–568.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kim JL, Park JH, Han SB, Cho IY and Jang
KM: Allogeneic blood transfusion is a significant risk factor for
surgical-site infection following total hip and knee arthroplasty:
A meta-analysis. J Arthroplasty. 32:320–325. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Le Quellec S, Paris M, Nougier C, Sobas F,
Rugeri L, Girard S, Bordet JC, Négrier C and Dargaud Y:
Pre-analytical effects of pneumatic tube system transport on
routine haematology and coagulation tests, global coagulation
assays and platelet function assays. Thromb Res. 153:7–13. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rhee C, Lethbridge L, Richardson G and
Dunbar M: Risk factors for infection, revision, death, blood
transfusion and longer hospital stay 3 months and 1 year after
primary total hip or knee arthroplasty. Can J Surg. 61:165–176.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hanafy AS, Badawi R, Basha MAA, Selim A,
Yousef M, Elnawasany S, Mansour L, Elkhouly RA, Hawash N and
Abd-Elsalam S: A novel scoring system for prediction of esophageal
varices in critically ill patients. Clin Exp Gastroenterol.
10:315–325. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
De Pietri L, Bianchini M, Montalti R, De
Maria N, Di Maira T, Begliomini B, Gerunda GE, di Benedetto F,
Garcia-Tsao G and Villa E: Thrombelastography-guided blood product
use before invasive procedures in cirrhosis with severe
coagulopathy: A randomized, controlled trial. Hepatology.
63:566–573. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abuelkasem E, Lu S, Tanaka K, Planinsic R
and Sakai T: Comparison between thrombelastography and
thromboelastometry in hyperfibrinolysis detection during adult
liver transplantation. Br J Anaesth. 116:507–512. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Marian AA, Bayman EO, Gillett A, Hadder B
and Todd MM: The influence of the type and design of the anesthesia
record on ASA physical status scores in surgical patients: Paper
records vs. electronic anesthesia records. BMC Med Inform Decis
Mak. 16:29–38. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Iba T, Gando S, Saitoh D, Ikeda T, Anan H,
Oda S, Kitamura N, Mori S, Kotani J and Kuroda Y: Efficacy and
bleeding risk of antithrombin supplementation in patients with
septic disseminated intravascular coagulation: A third survey. Clin
Appl Thromb Hemost. 23:422–428. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rasmussen KC, Højskov M, Johansson PI,
Kridina I, Kistorp T, Salling L, Nielsen HB, Ruhnau B, Pedersen T
and Secher NH: Impact of albumin on coagulation competence and
hemorrhage during major surgery: A randomized controlled trial.
Medicine (Baltimore). 95:e27202016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Douketis JD, Wang G, Chan N, Eikelboom JW,
Syed S, Barty R, Moffat KA, Spencer FA, Blostein M and Schulman S:
Effect of standardized perioperative dabigatran interruption on the
residual anticoagulation effect at the time of surgery or
procedure. J Thromb Haemost. 14:89–97. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Spahn DR, Spahn GH and Stein P:
Indications and risks of fibrinogen in surgery and trauma. Semin
Thromb Hemost. 42:147–154. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gonzalez E, Moore EE, Moore HB, Chapman
MP, Chin TL, Ghasabyan A, Wohlauer MV, Barnett CC, Bensard DD,
Biffl WL, et al: Goal-directed hemostatic resuscitation of
trauma-induced coagulopathy: A pragmatic randomized clinical trial
comparing a viscoelastic assay to conventional coagulation assays.
Ann Surg. 263:1051–1059. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yang T, Lu JH, Lau WY, Zhang TY, Zhang H,
Shen YN, Alshebeeb K, Wu MC, Schwartz M and Shen F: Perioperative
blood transfusion does not influence recurrence-free and overall
survivals after curative resection for hepatocellular carcinoma: A
Propensity Score Matching Analysis. J Hepatol. 64:583–593. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pohlman TH, Fecher AM and Arreola-Garcia
C: Optimizing transfusion strategies in damage control
resuscitation: Current insights. J Blood Med. 9:117–133. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qiu L, Wang DR, Zhang XY, Gao S, Li XX,
Sun GP and Lu XB: Impact of perioperative blood transfusion on
immune function and prognosis in colorectal cancer patients.
Transfus Apheresis Sci. 54:235–241. 2016. View Article : Google Scholar
|
|
19
|
Jiang L, Nick AM and Sood AK: Fundamental
principles of cancer biology: Does it have relevance to the
perioperative period? Curr Anesthesiol Rep. 5:250–256. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gary JL, Schneider PS, Galpin M, Radwan Z,
Munz JW, Achor TS, Prasarn ML and Cotton BA: Can thrombelastography
predict venous thromboembolic events in patients with severe
extremity trauma? J Orthop Trauma. 30:294–298. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cybulska P, Goss C, Tew WP, Parameswaran R
and Sonoda Y: Indications for and complications of transfusion and
the management of gynecologic malignancies. Gynecol Oncol.
146:416–426. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lawson PJ, Moore HB, Moore EE, Stettler
GR, Pshak TJ, Kam I, Silliman CC and Nydam TL: Preoperative
thrombelastography maximum amplitude predicts massive transfusion
in liver transplantation. J Surg Res. 220:171–175. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kreutz RP, Schmeisser G, Maatman B,
Schaffter A, Sinha A, von der Lohe E and Breall JA: Fibrin clot
strength measured by thrombelastography and outcomes after
percutaneous coronary intervention. Thromb Haemost. 117:426–428.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Adler M, Ivic S, Bodmer NS, Ten Cate H,
Bachmann LM, Wuillemin WA and Nagler M: Thromboelastometry and
thrombelastography analysis under normal physiological conditions -
systematic review. Transfus Med Hemother. 44:78–83. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
David JS, Imhoff E, Parat S, Augey L,
Geay-Baillat MO, Incagnoli P and Tazarourte K: Use of
thrombelastography to guide posttraumatic hemostatic therapy: More
coagulation factor concentrates and less allogenic blood
transfusion? Transfus Clin Biol. 23:205–211. 2016.(In French).
View Article : Google Scholar : PubMed/NCBI
|