Introduction
With the development of health care, the incidence
of invasive fungal infections (IFIs) in the high risk and impaired
immune-function population has been increasing (1). At present, it is believed that the main
risk factors for IFI include neutropenia, malignant hematopathy,
bone marrow transplantation, solid organ transplantation, severe
burn, glucocorticoids, long-term intensive care, chemotherapy, HIV
infection, invasive medical procedures and new immunosuppression
agents (2–4). The patients in ICU have the
characteristics of long-term bed rest, complicated basic diseases
and low immune system, which create the conditions for the breeding
and implantation of fungi, leading to an increasing number of
pulmonary fungal infections (5–7). The
early diagnosis of IFI, especially pulmonary fungal infection,
remains a challenge in medical research (8). Invasive pulmonary aspergillosis (IPA)
is the most common type in fungal pneumonia (9,10). At
present, the diagnosis of IFI relies on complex microbiological
methods (11,12), including culture and molecular
identification.
Multi-slice spiral computed tomography (CT), a
widely used imaging method in recent years, is reported to have
achieved good results in the differential diagnosis of complicated
pulmonary lesions by many scholars (13). Studies have also shown that CT is an
important tool for the early diagnosis of pulmonary infection in
immunocompromised hosts (14). The
density and spatial resolution of multi-slice spiral CT have been
greatly developed and unified. Its thin layer scan not only shows
the details and changes of lung tissue more clearly, but also shows
clearly all kinds of pathological changes, reconstructs images of
any plane, such as axial, sagittal and coronal plane, and provides
arbitrary section images by adjusting to different directions,
allowing us to better understand the details of the lesion and the
space anatomical relationship (15).
The purpose of this study was to investigate the
diagnostic value of 64-slice spiral CT in invasive pulmonary fungal
infection, and provide a reference for improving the treatment rate
and prognosis of patients with pulmonary fungal infection.
Patients and methods
General information
The clinical data of 82 suspected IFI patients
treated in the Department of Critical Care Medicine in The
Affiliated Hospital of Qingdao University (Qingdao, China) from
January 2016 to May 2018 were retrospectively analyzed, including
51 males and 31 females, with an average age of 40.59±10.34 years.
There were 21 patients with hematologic tumors, 42 patients treated
with immunosuppression agents, 7 patients treated with kidney
transplantation and 12 patients treated with solid tumor
chemotherapy. The main clinical symptoms were cough and
expectoration, and some patients presented with chest pain,
hemoptysis, and fever. All patients underwent X-ray and spiral CT
examinations during hospitalization. Finally, 64 patients were
diagnosed with IFI by pathology and sputum culture. Inclusion
criteria: suspected patients with clinical symptoms consistent with
IFI. Exclusion criteria: patients with other severe infections;
patients with allergies to CT contrast agents; patients with
short-term expected death; patients previously using antifungal
drugs. The patients and their families agreed to participate in tis
study and signed an informed consent. The study was approved by the
Ethics Committee of The Affiliated Hospital of Qingdao University.
The general information of the patients is shown in Table I.
 | Table I.General information [n (%)]. |
Table I.
General information [n (%)].
| Clinical data | Cases (n=82) |
|---|
| Sex |
|
| Male | 51 (62.20) |
|
Female | 31 (37.80) |
| Age (years) |
|
| ≥40 | 39 (47.56) |
|
<40 | 43 (52.44) |
| BMI
(kg/m2) |
|
| ≥21 | 37 (45.12) |
|
<21 | 45 (54.88) |
| Smoking |
|
| Yes | 59 (71.95) |
| No | 23 (28.05) |
| Hormone
administration |
|
| Yes | 48 (58.54) |
| No | 34 (41.46) |
| Severe disease
classification |
|
|
Hematologic tumor | 21 (25.61) |
|
Immunosuppression therapy | 42 (51.22) |
| Kidney
transplantation | 7 (8.54) |
| Solid
tumor chemotherapy | 12 (14.63) |
Detection methods
Sixty-four-slice spiral CT was performed using a CT
scanner obtained from GE Healthcare (Chicago, IL, USA). Patients
were placed in supine position and scanned with conventional plain
scan from lung apex to lung bottom (voltage, 120 kV; current,
200–250 mA; thick section, 5 mm; section interval, 5 mm). If
necessary, thinning and reconstruction were performed as needed,
and enhanced examination was performed. The lesion location was
scanned at a thickness of 2 mm and the section interval was 2 mm.
Mediastinal and pulmonary windows were used to observe the size,
number, location, shape, density, boundary, surrounding structure
and other imaging findings of lesions. The bedside chest
radiography (X-ray) was performed by 12A radiographic device
(Toshiba Medical Systems Corp., Tokyo, Japan), and chest
radiography by GE Revolution XQ/i (GE Healthcare). All patients
were examined in prone position and scans were carried out 2–3
times.
Outcome measures
Taking the results of pathology and sputum culture
as the gold standard, the imaging features of CT in confirmed
patients were analyzed and the sensitivity, specificity, accuracy,
positive coincidence rate, negative coincidence rate, misdiagnosis
rate and missed diagnosis rate of X-ray and CT in IFI were
calculated.
Statistical analysis
SPSS 17.0 statistical software (Shanghai Cabit
Information Technology Co., Ltd., Shanghai, China) was used for
analysis. t-test was used for the measurement data. P<0.05 was
considered to indicate a statistically significant difference.
Results
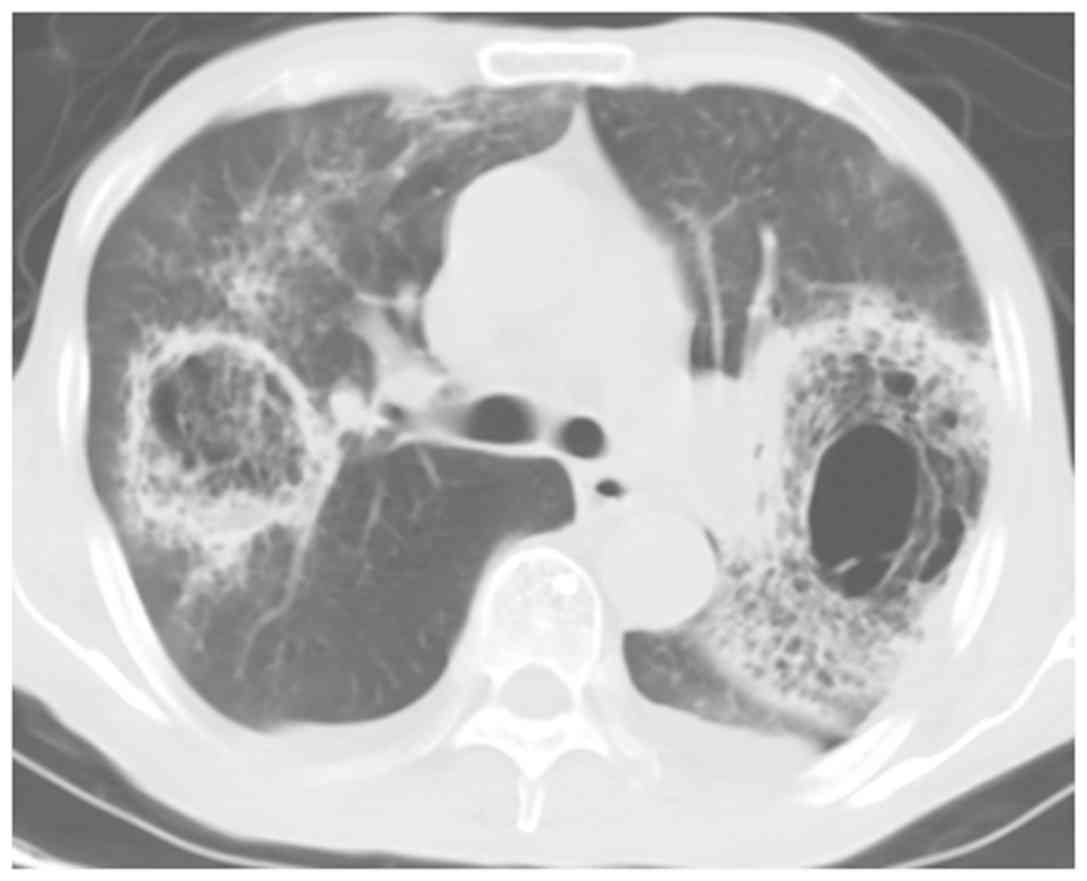
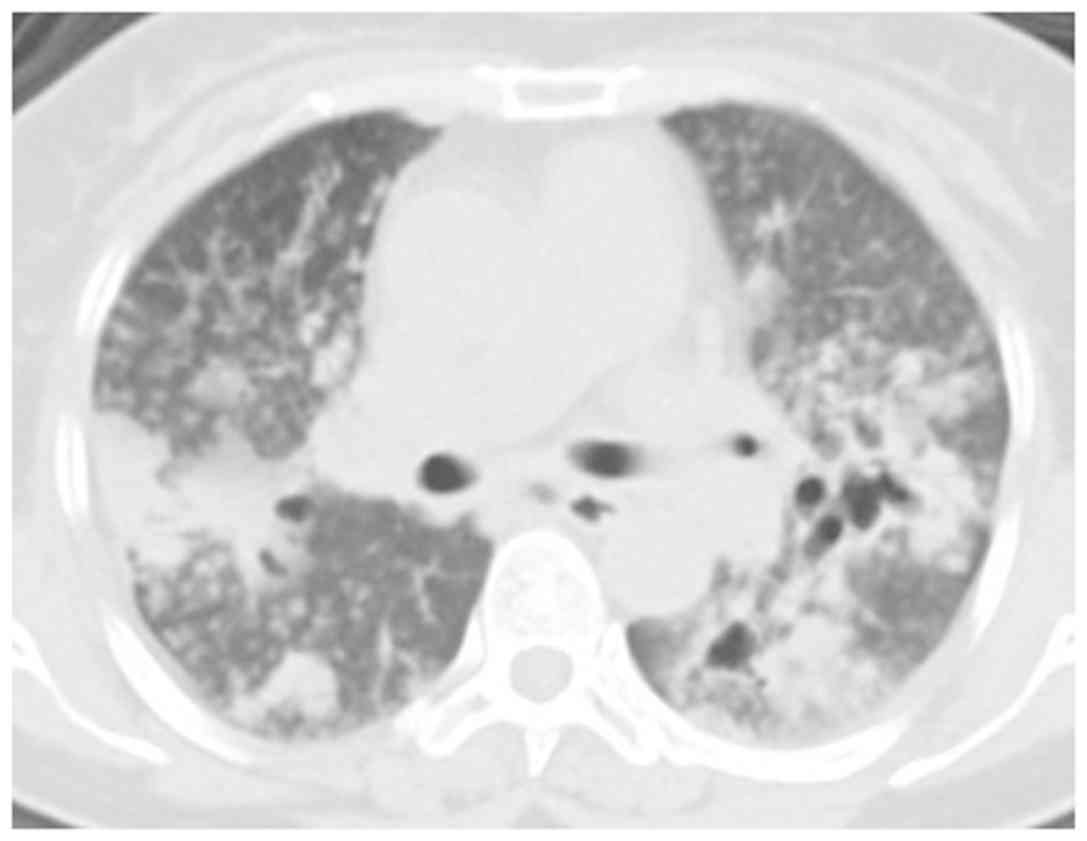
Spiral CT findings in 64 patients
Among 64 confirmed patients, there were 14 cases of
pulmonary mucormycosis, 15 cases of pulmonary Candida
infection, 20 cases of pulmonary Aspergillus infection, 13
cases of pulmonary Cryptococcus infection and 2 cases of
pulmonary histoplasmosis. Representative CT scans are shown in
Figs. 1–5.
X-ray and CT diagnosis
Taking pathological diagnosis as the gold standard,
the number of true-negative, true-positive, false-negative and
false-positive results in X-ray diagnosis were 13, 43, 21 and 5,
respectively, while those in CT diagnosis were 11, 59, 5 and 7,
respectively (Tables II and
III).
| Table II.X-ray diagnosis. |
Table II.
X-ray diagnosis.
|
| Pathological
diagnosis |
|
|---|
|
|
|
|
|---|
| X-ray diagnosis | Negative | Positive | Total |
|---|
| Negative | 13 | 21 | 34 |
| Positive | 5 | 43 | 48 |
| Total | 18 | 64 | 82 |
| Table III.CT diagnosis. |
Table III.
CT diagnosis.
|
| Pathological
diagnosis |
|
|---|
|
|
|
|
|---|
| CT diagnosis | Negative | Positive | Total |
|---|
| Negative | 11 | 5 | 16 |
| Positive | 7 | 59 | 66 |
| Total | 18 | 64 | 82 |
Comparison of diagnostic value of
X-ray and CT
The sensitivity, specificity, accuracy, positive
coincidence rate, negative coincidence rate, misdiagnosis rate and
missed diagnosis rate of X-ray in IFI were 67.19, 72.22, 68.29,
89.58, 38.24, 27.78 and 32.81%, respectively, while those of CT in
IFI were 92.18, 61.11, 85.37, 89.39, 68.75, 38.89 and 7.81%,
respectively. The sensitivity, accuracy and negative coincidence
rate of CT in the diagnosis of IFI were significantly higher than
those of X-ray (P<0.05), with a sensitivity of 92.18%, which
indicates that CT had a high diagnostic value in IFI (Table IV).
| Table IV.Comparison of the diagnostic value of
X-ray and CT. |
Table IV.
Comparison of the diagnostic value of
X-ray and CT.
| Diagnosis | X-ray (n=82) (%) | CT (n=82) (%) | t | P-value |
|---|
| Sensitivity | 67.19 | 92.18 | 12.36 | <0.001 |
| Specificity | 72.22 | 61.11 | 0.500 | 0.480 |
| Accuracy | 68.29 | 85.37 | 6.713 | <0.050 |
| Positive
coincidence rate | 89.58 | 89.39 | 0.001 | 0.974 |
| Negative
coincidence rate | 38.24 | 68.75 | 18.68 | <0.001 |
| Misdiagnosis
rate | 27.78 | 38.89 | 0.500 | 0.480 |
| Missed diagnosis
rate | 32.81 | 7.81 | 12.36 | <0.001 |
Discussion
In recent years, with the widespread use of
antibiotics, hormones and immunosuppression agents, the number of
IFIs has increased (16). However,
because of the lack of clinical specificity of IFI, the condition
is easily covered up by the primary disease, resulting in delay of
the treatment. This is the reason why the highest mortality rate
can reach 80% (17). IFI has become
one of the leading causes of death in patients with solid organ
transplantation and hematological malignancy (18,19).
Therefore, the way to make accurate and in time diagnosis of IFI is
an urgent issue to be addressed. At present, the gold standard for
the diagnosis of IFI is pathological biopsy, but it is not accepted
by patients and doctors because of the trauma caused. The
sensitivity and specificity of traditional methods, such as
respiratory sputum culture are only ~50% (20). Studies have shown that CT plays an
important role in the diagnosis of fungal infections (21). CT has also been reported to have
higher spatial and density resolution than X-ray, and to make good
imaging observation of the basic pathological changes in IFI
(22). In the diagnosis of pulmonary
fungal infection, CT is expressed as scattered nodules, masses or
patchy focis, and other signs, such as halo. Meniscus signs may
also appear, and the occurrence of one or both signs at the same
time is common (23). It has also
been reported that subpleural wedge-shaped consolidation may occur
in invasive pulmonary Aspergillus infection imaging
(24).
In the present study, with pathological diagnosis as
the gold standard, the diagnostic value of X-ray and CT in IFI was
compared and the imaging features of CT diagnosis were analyzed.
The results showed that the sensitivity, accuracy and negative
coincidence rate of CT in the diagnosis of IFI were significantly
higher than those of X-ray (P<0.05), with a sensitivity of
92.18%, which indicates that CT has a high diagnostic value in IFI.
By analyzing the causes of misdiagnosis and missed diagnosis, it
has been found that 6 out of 7 cases misdiagnosed with CT are
caused by host factors. Although some studies have shown that the
diagnosis of fungal infection has a greater dependence on host
factors (11), we believe that
misdiagnosis can also be caused by excessive interpretation of host
factors in the misdiagnosis case analysis. When the causes of
misdiagnosis and missed diagnosis of X-ray were analyzed, it was
found that most of them were difficult to diagnose because of
unclear imaging features. Therefore, we believe that when imaging
cannot be judged, sputum culture or serum marker examination should
be performed in time to further determine the diagnostic results.
For example, when a patient has pulmonary artery embolism and
incurable long-term pulmonary abscess, it can be considered as
pulmonary mucormycosis infection. In the analysis of the imaging
features of CT in this study, it was found that the multiple
nodules and meniscus signs appeared more frequently in the
collected cases, which coincided with the CT imaging features of
IFI described in related literature (22). Some studies have suggested that the
CT manifestations of pneumonia caused by different strains have
their own characteristics (25). For
example, meniscus sign is the characteristic of Aspergillus
infection, and multiple nodule and small patch are the
characteristics of Cryptococcus infection. In the diagnostic
criteria developed by the European Organization for Cancer Therapy
and Fungal Research Group, the meniscus sign and the cavity
appearing in the consolidation are all characteristic
manifestations of pulmonary fungal infection (26).
In conclusion, the diagnostic value of CT in IFI is
higher than that of traditional X-ray, and CT has a better
enhancement effect in many fungal areas infected with IFI. However,
some lesions are difficult to distinguish, so it is necessary to
make a comprehensive judgment and diagnosis by combining the
clinical data and the medical history of the patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JW, JLi and FY were responsible for the CT result
analysis. JLin and CZ recorded and analyzed the general data of
patients. JLi, FY and LZ contributed to the statistical analysis.
The final version was read and approved by all the authors.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Affiliated Hospital of Qingdao University (Qingdao, China).
Signed written informed consents were obtained from the patients or
their guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Badiee P and Hashemizadeh Z: Opportunistic
invasive fungal infections: Diagnosis & clinical management.
Indian J Med Res. 139:195–204. 2014.PubMed/NCBI
|
|
2
|
Ribes JA, Vanover-Sams CL and Baker DJ:
Zygomycetes in human disease. Clin Microbiol Rev. 13:236–301. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Baddley JW: Clinical risk factors for
invasive aspergillosis. Med Mycol. 49 Suppl 1:S7–S12. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Badiee P, Alborzi A and Farhoudi F: A case
of Candida mediastinitis after dental extraction. J Infect
Dev Ctries. 5:75–78. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vandewoude KH, Blot SI, Depuydt P, Benoit
D, Temmerman W, Colardyn F and Vogelaers D: Clinical relevance of
Aspergillus isolation from respiratory tract samples in
critically ill patients. Crit Care. 10:R312006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Garnacho-Montero J, Amaya-Villar R,
Ortiz-Leyba C, León C, Alvarez-Lerma F, Nolla-Salas J,
Iruretagoyena JR and Barcenilla F: Isolation of Aspergillus
spp. from the respiratory tract in critically ill patients: Risk
factors, clinical presentation and outcome. Crit Care. 9:R191–R199.
2005. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cornillet A, Camus C, Nimubona S, Gandemer
V, Tattevin P, Belleguic C, Chevrier S, Meunier C, Lebert C, Aupée
M, et al: Comparison of epidemiological, clinical, and biological
features of invasive aspergillosis in neutropenic and
nonneutropenic patients: A 6-year survey. Clin Infect Dis.
43:577–584. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Georgiadou SP, Sipsas NV, Marom EM and
Kontoyiannis DP: The diagnostic value of halo and reversed halo
signs for invasive mold infections in compromised hosts. Clin
Infect Dis. 52:1144–1155. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bruno C, Minniti S, Vassanelli A and
Pozzi-Mucelli R: Comparison of CT features of Aspergillus
and bacterial pneumonia in severely neutropenic patients. J Thorac
Imaging. 22:160–165. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Escuissato DL, Gasparetto EL, Marchiori E,
Rocha GM, Inoue C, Pasquini R and Müller NL: Pulmonary infections
after bone marrow transplantation: high-resolution CT findings in
111 patients. AJR Am J Roentgenol. 185:608–615. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hope WW, Walsh TJ and Denning DW:
Laboratory diagnosis of invasive aspergillosis. Lancet Infect Dis.
5:609–622. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yeo SF and Wong B: Current status of
nonculture methods for diagnosis of invasive fungal infections.
Clin Microbiol Rev. 15:465–484. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ma SH, Xu K, Xiao ZW, Wu M, Sun ZY, Wang
ZX, Hu ZG, Dai X, Han MJ and Li YG: Peripheral lung cancer:
Relationship between multi-slice spiral CT perfusion imaging and
tumor angiogenesis and cyclin D1 expression. Clin Imaging.
31:165–177. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Caillot D, Couaillier JF, Bernard A,
Casasnovas O, Denning DW, Mannone L, Lopez J, Couillault G, Piard
F, Vagner O, et al: Increasing volume and changing characteristics
of invasive pulmonary aspergillosis on sequential thoracic computed
tomography scans in patients with neutropenia. J Clin Oncol.
19:253–259. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fuchs T, Kachelriess M and Kalender WA:
Technical advances in multi-slice spiral CT. Eur J Radiol.
36:69–73. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yang WL, Cao J, Chen BY, Xie W, Dong LX,
Wu YQ, Li JN and Hu ZD: A preliminary study on the measurement of
(1,3)-β-D-glucan in bronchoalveolar lavage for the diagnosis of
pulmonary fungal infections. Zhonghua Jie He He Hu Xi Za Zhi.
35:897–900. 2012.(In Chinese). PubMed/NCBI
|
|
17
|
Lin SJ, Schranz J and Teutsch SM:
Aspergillosis case - fatality rate: Systematic review of the
literature. Clin Infect Dis. 32:358–366. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Segal BH and Walsh TJ: Current approaches
to diagnosis and treatment of invasive aspergillosis. Am J Respir
Crit Care Med. 173:707–717. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Patterson TF: Advances and challenges in
management of invasive mycoses. Lancet. 366:1013–1025. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Prasad A, Agarwal K, Deepak D and Atwal
SS: Pulmonary Aspergillosis: What CT can offer before it is too
late! J Clin Diagn Res. 10:TE01–TE05. 2016.PubMed/NCBI
|
|
21
|
Christe A, Lin MC, Yen AC, Hallett RL,
Roychoudhury K, Schmitzberger F, Fleischmann D, Leung AN, Rubin GD,
Vock P, et al: CT patterns of fungal pulmonary infections of the
lung: Comparison of standard-dose and simulated low-dose CT. Eur J
Radiol. 81:2860–2866. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Park SY, Kim SH, Choi SH, Sung H, Kim MN,
Woo JH, Kim YS, Park SK, Lee JH, Lee KH, et al: Clinical and
radiological features of invasive pulmonary aspergillosis in
transplant recipients and neutropenic patients. Transpl Infect Dis.
12:309–315. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Franquet T, Müller NL, Giménez A, Guembe
P, de La Torre J and Bagué S: Spectrum of pulmonary aspergillosis:
Histologic, clinical, and radiologic findings. Radiographics.
21:825–837. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Paulussen C, Hallsworth JE, Álvarez-Pérez
S, Nierman WC, Hamill PG, Blain D, Rediers H and Lievens B: Ecology
of aspergillosis: Insights into the pathogenic potency of
Aspergillus fumigatus and some other Aspergillus
species. Microb Biotechnol. 10:296–322. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Demirkazik FB, Akin A, Uzun O, Akpinar MG
and Ariyürek MO: CT findings in immunocompromised patients with
pulmonary infections. Diagn Interv Radiol. 14:75–82.
2008.PubMed/NCBI
|
|
26
|
De Pauw B, Walsh TJ, Donnelly JP, Stevens
DA, Edwards JE, Calandra T, Pappas PG, Maertens J, Lortholary O,
Kauffman CA, et al: European Organization for Research and
Treatment of Cancer/Invasive Fungal Infections Cooperative Group;
National Institute of Allergy and Infectious Diseases Mycoses Study
Group (EORTC/MSG) Consensus Group: Revised definitions of invasive
fungal disease from the European Organization for Research and
Treatment of Cancer/Invasive Fungal Infections Cooperative Group
and the National Institute of Allergy and Infectious Diseases
Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis.
46:1813–1821. 2008. View
Article : Google Scholar : PubMed/NCBI
|